
Comparison of Treatment Outcomes among Sibling Oocytes Using Different Culture Systems—Conventional IVF versus INVOcell Device—And Evaluation of INVOcell User Satisfaction: The INVOcIVF Study


Abstract
:1. Introduction
2. Materials and Methods
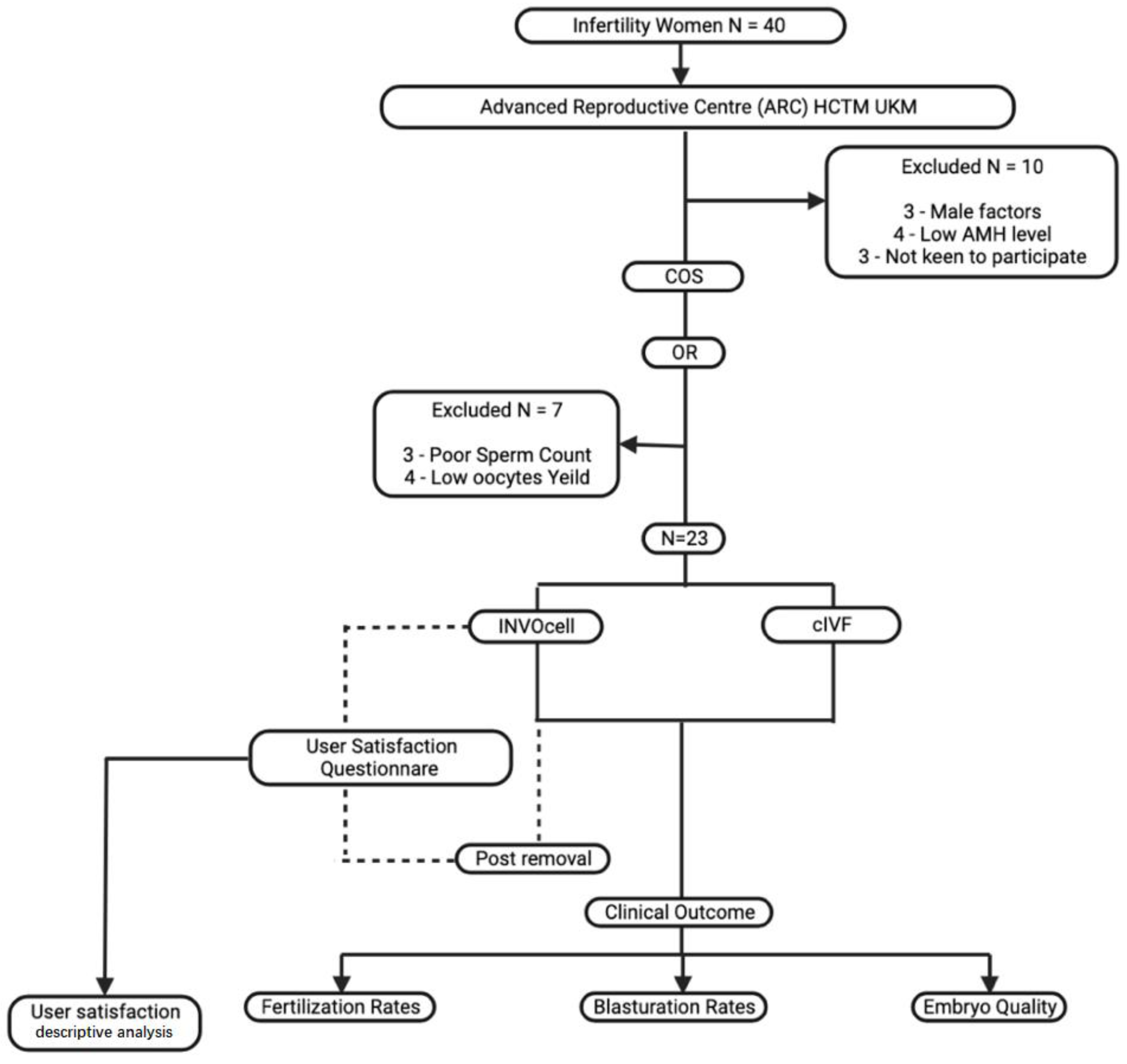
2.1. Study Design
2.2. Study Protocol
2.3. Evaluation of INVOcell Device
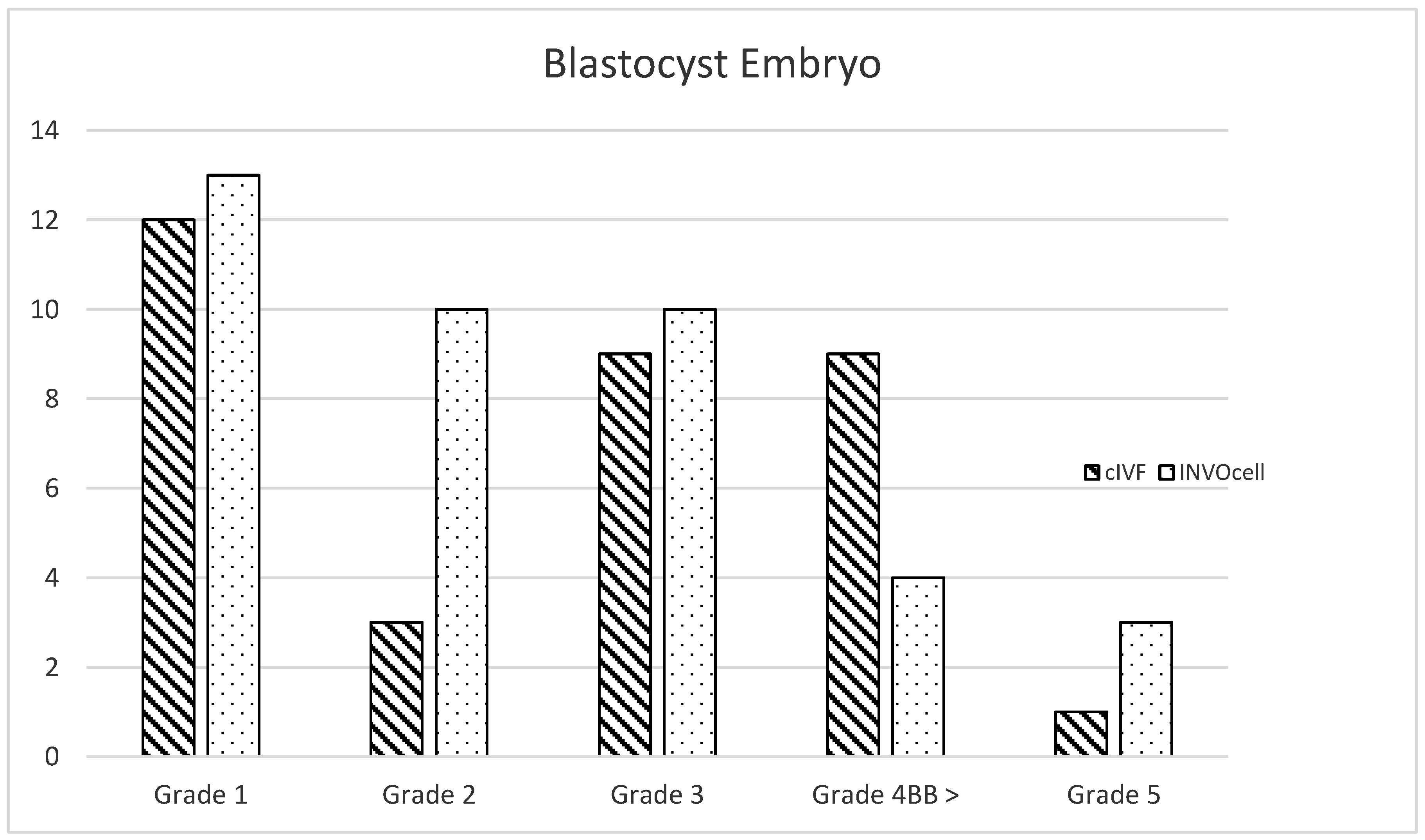
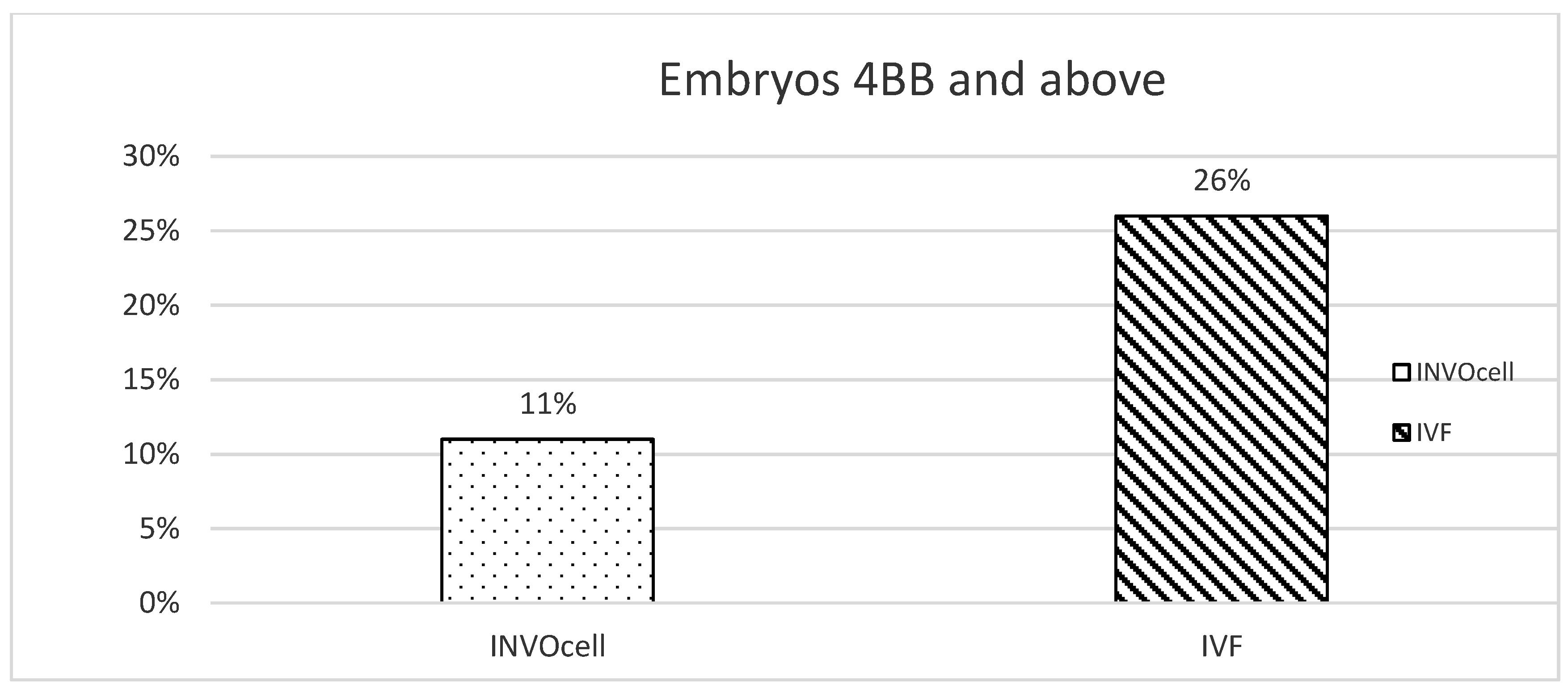
2.4. Fertilization, Blastulation, and Embryo Quality Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ranoux, C.; Aubriot, F.X.; Dubuisson, J.B.; Cardone, V.; Foulot, H.; Poirot, C.; Chevallier, O. A new in vitro fertilization technique: Intravaginal culture. Fertil. Steril. 1988, 49, 654–657. [Google Scholar] [CrossRef]
- Fukuda, M.; Fukuda, K.; Ranoux, C. Unexpected low oxygen tension of intravaginal culture. Hum. Reprod. 1996, 11, 1293–1295. [Google Scholar] [CrossRef] [PubMed]
- Frydman, R.; Ranoux, C. INVO: A simple, low cost effective assisted reproductive technology. Hum. Reprod. 2008, 2008, 85–89. [Google Scholar] [CrossRef]
- Ombelet, W. Global access to infertility care in developing countries: A case of human rights, equity and social justice. Facts Views Vis. Obgyn. 2011, 3, 257–266. [Google Scholar]
- Ombelet, W.; Cooke, I.; Dyer, S.; Serour, G.; Devroey, P. Infertility and the provision of infertility medical services in developing countries. Hum. Reprod. Update 2008, 14, 605–621. [Google Scholar] [CrossRef]
- Gameiro, S.; Boivin, J.; Peronace, L.; Verhaak, C.M. Why do patients discontinue fertility treatment? A systematic review of reasons and predictors of discontinuation in fertility treatment. Hum. Reprod. Update 2012, 18, 652–669. [Google Scholar] [CrossRef]
- Edition, B.A. INVOcell Launched in Malaysia by Advanced Reproductive Centre, Hospital Canselor Tuanku Muhriz. 25 August 2022. Available online: https://www.prnewswire.com/news-releases/invocell-launched-in-malaysia-by-advanced-reproductive-centre-hospital-canselor-tuanku-muhriz-301612139.html (accessed on 20 August 2022).
- Lucena, E.; Saa, A.M.; Navarro, D.E.; Pulido, C.; Lombana, O.; Moran, A. INVO procedure: Minimally invasive IVF as an alternative treatment option for infertile couples. Sci. World J. 2012, 2012, 571596. [Google Scholar] [CrossRef] [PubMed]
- Post, T.A. Declining fertility rates in ASEAN. Asian Post, 1 September 2020. [Google Scholar]
- Craig, J. Replacement level fertility and future population growth. Popul. Trends 1994, 20–22. [Google Scholar]
- Katz, P.; Showstack, J.; Smith, J.F.; Nachtigall, R.D.; Millstein, S.G.; Wing, H.; Eisenberg, M.L.; Pasch, L.A.; Croughan, M.S.; Adler, N. Costs of infertility treatment: Results from an 18-month prospective cohort study. Fertil. Steril. 2011, 95, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Dow, K. Looking into the Test Tube: The Birth of IVF on British Television. Med. Hist. 2019, 63, 189–208. [Google Scholar] [CrossRef]
- Morishita, N.; Ochi, M.; Horiuchi, T. History and prospects of intracytoplasmic sperm injection (ICSI) and the development of golden hamster ICSI embryos. Reprod. Med. Biol. 2021, 20, 410–418. [Google Scholar] [CrossRef]
- Glenn, T.L.; Kotlyar, A.M.; Seifer, D.B. The Impact of Intracytoplasmic Sperm Injection in Non-Male Factor Infertility-A Critical Review. J. Clin. Med. 2021, 10, 2616. [Google Scholar] [CrossRef]
- Butts, S.F.; Owen, C.; Mainigi, M.; Senapati, S.; Seifer, D.B.; Dokras, A. Assisted hatching and intracytoplasmic sperm injection are not associated with improved outcomes in assisted reproduction cycles for diminished ovarian reserve: An analysis of cycles in the United States from 2004 to 2011. Fertil. Steril. 2014, 102, 1041–1047.e1. [Google Scholar] [CrossRef]
- The Practice Committees of the American Society for Reproductive Medicine; The Society for Assisted Reproductive Technology. Intracytoplasmic sperm injection (ICSI) for non-male factor indications: A committee opinion. Fertil. Steril. 2020, 114, 239–245. [Google Scholar] [CrossRef]
- McPherson, N.O.; Vincent, A.D.; Pacella-Ince, L.; Tremellen, K. Comparison of in vitro fertilisation/intracytoplasmic sperm injection on live birth rates in couples with non-male factor infertility and advanced maternal age. J. Assist. Reprod. Genet. 2021, 38, 669–678. [Google Scholar] [CrossRef]
- Zagadailov, P.; Seifer, D.B.; Shan, H.; Zarek, S.M.; Hsu, A.L. Do state insurance mandates alter ICSI utilization? Reprod. Biol. Endocrinol. 2020, 18, 33. [Google Scholar] [CrossRef]
- Swain, J.E. Optimizing the culture environment in the IVF laboratory: Impact of pH and buffer capacity on gamete and embryo quality. Reprod. Biomed. Online 2010, 21, 6–16. [Google Scholar] [CrossRef]
- Zhang, J.Q.; Li, X.L.; Peng, Y.; Guo, X.; Heng, B.C.; Tong, G.Q. Reduction in exposure of human embryos outside the incubator enhances embryo quality and blastulation rate. Reprod. Biomed. Online 2010, 20, 510–515. [Google Scholar] [CrossRef]
- Gardner, D.K.; Lane, M.; Calderon, I.; Leeton, J. Environment of the preimplantation human embryo in vivo: Metabolite analysis of oviduct and uterine fluids and metabolism of cumulus cells. Fertil. Steril. 1996, 65, 349–353. [Google Scholar] [CrossRef]
- Bonaventura, L.; Ahlering, P.; Morris, R.; Mouchel, J.; Scheiber, M.; Batzofin, J. P-93: The INVOcell, a new medical device for intra vaginal fertilization and culture. Fertil. Steril. 2006, 86, S164. [Google Scholar] [CrossRef]
- Ranoux, C.; Seibel, M.M. New techniques in fertilization: Intravaginal culture and microvolume straw. J. Vitr. Fert. Embryo. Transf. 1990, 7, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Sterzik, K.; Rosenbusch, B.; Sasse, V.; Wolf, A.; Beier, H.M.; Lauritzen, C. A new variation of in-vitro fertilization: Intravaginal culture of human oocytes and cleavage stages. Hum. Reprod. 1989, 4 (Suppl. 8), 83–86. [Google Scholar] [CrossRef] [PubMed]
- Taymor, M.L.; Ranoux, C.J.; Gross, G.L. Natural oocyte retrieval with intravaginal fertilization: A simplified approach to in vitro fertilization. Obs. Gynecol. 1992, 80, 888–891. [Google Scholar]
- Krasnopolskaya, K.V.; Beketova, A.N.; Sesina, N.I.; Chinchenko, N.K.; Badalyan, G.V.; Sudarikova, N.M.; Bocharova, T.V.; Zakharchenko, E.O. The effect of short-term disturbance of day 3 embryo culture on the development and implantation. Gynecol. Endocrinol. 2019, 35 (Suppl. 1), 1–4. [Google Scholar] [CrossRef]
- Kirkegaard, K.; Agerholm, I.E.; Ingerslev, H.J. Time-lapse monitoring as a tool for clinical embryo assessment. Hum. Reprod. 2012, 27, 1277–1285. [Google Scholar] [CrossRef]
- Chen, X.; Shi, S.; Mao, J.; Zou, L.; Yu, K. Developmental Potential of Abnormally Fertilized Oocytes and the Associated Clinical Outcomes. Front. Physiol. 2020, 11, 528424. [Google Scholar] [CrossRef]
- Doody, K.J.; Broome, E.J.; Doody, K.M. Comparing blastocyst quality and live birth rates of intravaginal culture using INVOcell™ to traditional in vitro incubation in a randomized open-label prospective controlled trial. J. Assist. Reprod. Genet. 2016, 33, 495–500. [Google Scholar] [CrossRef]
- Jellerette-Nolan, T.; Cooper, A.R.; Doody, K.J.; Nichols, J.E.; Park, J.K.; Poe-Zeigler, R.L.; Khair, A.F.; Stong, L.M.; Paulson, R.J.; Daftary, G.S. Real-world experience with intravaginal culture using INVOCELL: An alternative model for infertility treatment. FS Rep. 2021, 2, 9–15. [Google Scholar] [CrossRef]
- Babayev, E.; Jain, T. Intravaginal culture using INVOCELL: Is it a viable treatment option for infertility? FS Rep. 2021, 2, 7–8. [Google Scholar] [CrossRef]
- INVO Bioscience. INVO Bioscience Announces Four Individual Poster Abstracts Discussing the Benefits of INVOcell. In Proceedings of the 2021 American Society for Reproductive Medicine (ASRM) Congress & Expo, Baltimore, MD, USA, 20 October 2021. [Google Scholar]
- Evans, C.W.; Renee, H. Effect of Angle of Turning and Shaking Agitation during Incubation on Embryo Development and Hatchability. 2009. Available online: https://repository.lib.ncsu.edu/handle/1840.16/133 (accessed on 23 August 2022).
- Paterek, J.A.E. Vaginal Foreign Body Evaluation and Treatment; Treasure Island StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 32.9 years old |
| BMI | 24.9 kg/m2 |
| Fertility Factors | n (%) |
| 9 (39.1) |
| 3 (13.1) |
| 5 (21.7) |
| 6 (26.1) |
| Type of Intervention | cIVF | INVOcell® |
|---|---|---|
| No. of oocytes | n (mean) 115 (4.987) | n (mean) 138 (6) |
| No. of blastocysts | n (%) 39 (33.9) | n (%) 45(32.6) |
| Fertilization Rates | |||
| INVOcell® (n = 23) Median (IQR) | cIVF (n = 23) Median (IQR) | Z statistic | p-value a |
| 1.0 (0.2–4.0) | 3.0 (1.0–4.0) | −0.973 | 0.331 |
| Blastulation Rates | |||
| INVOcell® (n = 23) Median (IQR) | cIVF (n = 23) Median (IQR) | Z statistic | p-value a |
| 1.0 (0.2–1.0) | 0.5 (0–1.0) | −2.420 | 0.016 * |
| Good-Quality Embryos | |||
| INVOcell® (n = 23) Median (IQR) | cIVF (n = 23) Median (IQR) | Z statistic | p-value a |
| 0 (0–0.33) | 0 (0–0.25) | −0.473 | 0.636 |
| Q1 | Did you have all information and advice that you needed before insertion of the device? | ||
| Answers | Frequency | Percentage (%) | |
| No | 0 | 0 | |
| Unsure | 0 | 0 | |
| Yes | 23 | 100 | |
| Q2 | Did you experience an increase in vaginal discharge? | ||
| Answers | Frequency | Percentage (%) | |
| No | 12 | 52.2 | |
| Unsure | 0 | 0 | |
| Yes | 11 | 47.8 | |
| Q3 | Did you experience per-vaginal bleeding? | ||
| Answers | Frequency | Percentage (%) | |
| No | 22 | 95.7 | |
| Unsure | 0 | 0 | |
| Yes | 1 | 4.3 | |
| Q4 | Did you have any other side effects following intravaginal culture device insertion? | ||
| Answers | Frequency | Percentage (%) | |
| No | 23 | 100 | |
| Unsure | 0 | 0 | |
| Yes | 0 | 0 | |
| Q5 | Did the intravaginal culture device affect your daily life? | ||
| Answers | Frequency | Percentage (%) | |
| No | 23 | 100 | |
| Unsure | 0 | 0 | |
| Yes | 0 | 0 | |
| Q6 | Did you have any discomfort following intravaginal culture device insertion? | ||
| Answers | Frequency | Percentage (%) | |
| No | 23 | 100 | |
| Unsure | 0 | 0 | |
| Yes | 0 | 0 | |
| Q7 | Did you think that the follow-up you received was adequate? | ||
| Answers | Frequency | Percentage (%) | |
| No | 12 | 52.2 | |
| Unsure | 0 | 0 | |
| Yes | 11 | 47.8 | |
| Q8 | Did the treatment meet your expectations? | ||
| Answers | Frequency | Percentage (%) | |
| No | 0 | 0 | |
| Unsure | 5 | 21.7 | |
| Yes | 18 | 78.3 | |
| Q9 | Was the removal of the device painful? | ||
| Answers | Frequency | Percentage (%) | |
| No | 23 | 100 | |
| Unsure | 0 | 0 | |
| Yes | 0 | 0 | |
| Q10 | In a similar situation would you chose the intravaginal culture device again or recommend it to a good friend? | ||
| Answers | Frequency | Percentage (%) | |
| No | 0 | 0 | |
| Unsure | 5 | 21.7 | |
| Yes | 18 | 78.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang Mohsin, W.S.; Abdullah Chue, N.S.; Abdul Hamid, F.; Abu, M.A.; Othman, S.; Mat Jin, N.; Woon, S.Y.; Abdul Karim, A.K.; Ahmad, M.F. Comparison of Treatment Outcomes among Sibling Oocytes Using Different Culture Systems—Conventional IVF versus INVOcell Device—And Evaluation of INVOcell User Satisfaction: The INVOcIVF Study. Int. J. Environ. Res. Public Health 2022, 19, 12391. https://doi.org/10.3390/ijerph191912391
Yang Mohsin WS, Abdullah Chue NS, Abdul Hamid F, Abu MA, Othman S, Mat Jin N, Woon SY, Abdul Karim AK, Ahmad MF. Comparison of Treatment Outcomes among Sibling Oocytes Using Different Culture Systems—Conventional IVF versus INVOcell Device—And Evaluation of INVOcell User Satisfaction: The INVOcIVF Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12391. https://doi.org/10.3390/ijerph191912391
Chicago/Turabian StyleYang Mohsin, Wan Syahirah, Nor Shaireen Abdullah Chue, Fazilah Abdul Hamid, Muhammad Azrai Abu, Sukhilmi Othman, Norazilah Mat Jin, Shu Yuan Woon, Abdul Kadir Abdul Karim, and Mohd Faizal Ahmad. 2022. "Comparison of Treatment Outcomes among Sibling Oocytes Using Different Culture Systems—Conventional IVF versus INVOcell Device—And Evaluation of INVOcell User Satisfaction: The INVOcIVF Study" International Journal of Environmental Research and Public Health 19, no. 19: 12391. https://doi.org/10.3390/ijerph191912391