
Palliative Care e-Learning for Physicians Caring for Critically Ill and Dying Patients during the COVID-19 Pandemic: An Outcome Evaluation with Self-Assessed Knowledge and Attitude

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Global Evaluation—Feasibility
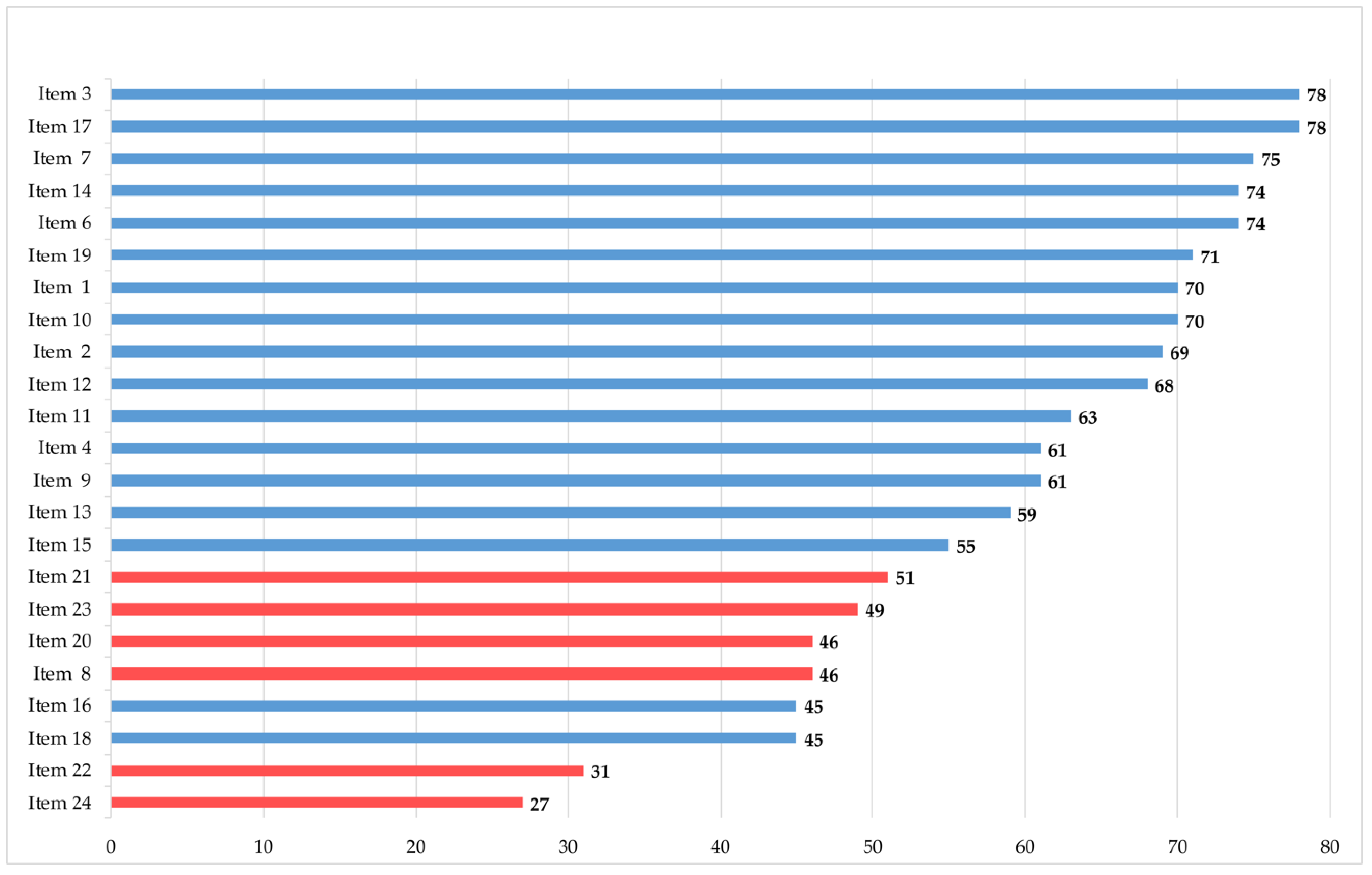
3.3. Outcome-Based Evaluation—Effect on Knowledge and Attitude
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morawa, E.; Schug, C.; Geiser, F.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Hiebel, N.; Borho, A.; Erim, Y. Psychosocial Burden and Working Conditions during the COVID-19 Pandemic in Germany: The VOICE Survey among 3678 Health Care Workers in Hospitals. J. Psychosom. Res. 2021, 144, 110415. [Google Scholar] [CrossRef] [PubMed]
- Münch, U.; Müller, H.; Deffner, T.; von Schmude, A.; Kern, M.; Kiepke-Ziemes, S.; Radbruch, L. Empfehlungen Zur Unterstützung von Belasteten, Schwerstkranken, Sterbenden Und Trauernden Menschen in Der Corona-Pandemie Aus Palliativmedizinischer Perspektive. Der Schmerz 2020, 34, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Tielker, J.M.; Weber, J.P.; Simon, S.T.; Bausewein, C.; Stiel, S.; Schneider, N. Experiences, Challenges and Perspectives for Ensuring End-of-Life Patient Care: A National Online Survey with General Practitioners in Germany. PLoS ONE 2021, 16, e0254056. [Google Scholar] [CrossRef] [PubMed]
- Bausewein, C.; Hodiamont, F.; Berges, N.; Ullrich, A.; Gerlach, C.; Oechsle, K.; Pauli, B.; Weber, J.; Stiel, S.; Schneider, N.; et al. National Strategy for Palliative Care of Severely Ill and Dying People and Their Relatives in Pandemics (PallPan) in Germany—Study Protocol of a Mixed-Methods Project. BMC Palliat. Care 2022, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schallenburger, M.; Reuters, M.C.; Schwartz, J.; Fischer, M.; Roch, C.; Werner, L.; Bausewein, C.; Simon, S.T.; van Oorschot, B.; Neukirchen, M. Inpatient Generalist Palliative Care during the SARS-CoV-2 Pandemic—Experiences, Challenges and Potential Solutions from the Perspective of Health Care Workers. BMC Palliat. Care 2022, 21, 1–11. [Google Scholar] [CrossRef]
- Palliativversorgung in Pandemiezeiten—Überblick. Available online: https://pallpan.de/elearning/#/ (accessed on 14 April 2022).
- Schwartz, J.; Schallenburger, M.; Thyson, T.; Meier, S.; Neukirchen, M. Psychische Belastung Des Intensivpersonals: Kommunikationsseminare Helfen. Available online: https://www.aerzteblatt.de/pdf.asp?id=222589 (accessed on 9 March 2022).
- Callinan, J. Barriers and Facilitators to E-Learning in Palliative Care. Int. J. Palliat. Nurs. 2020, 26, 394–402. [Google Scholar] [CrossRef]
- Sinclair, P.; Kable, A.; Levett-Jones, T. The Effectiveness of Internet-Based e-Learning on Clinician Behavior and Patient Outcomes: A Systematic Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 52–64. [Google Scholar] [CrossRef]
- Gamondi, C.; Larkin, C.; Payne, S. Core Competencies in Palliative Care: An EAPC White Paper on Palliative Care Education—Part 1. Eur. J. Palliat. Care 2013, 20, 86–91. [Google Scholar]
- Gibbins, J.; Williams, J.; Cooke, J.; Alder, D.; Forbes, K. Can E-Learning Help Surface or Change Medical Students’ Attitudes towards Palliative Care, Death and Dying? BMJ Support. Palliat. Care 2012, 2, A32. [Google Scholar] [CrossRef]
- Schiekirka, S.; Anders, S.; Raupach, T. Assessment of Two Different Types of Bias Affecting the Results of Outcome-Based Evaluation in Undergraduate Medical Education. BMC Med. Educ. 2014, 14, 149. [Google Scholar] [CrossRef]
- Schulz-Quach, C.; Wenzel-Meyburg, U.; Fetz, K. Can Elearning Be Used to Teach Palliative Care?—Medical Students’ Acceptance, Knowledge, and Self-Estimation of Competence in Palliative Care after Elearning. BMC Med. Educ. 2018, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Thyson, T.; Schallenburger, M.; Scherg, A.; Leister, A.; Schwartz, J.; Neukirchen, M. Communication in the Face of Death and Dying—How Does the Encounter with Death Influence the Patient Management Competence of Medical Students? An Outcome-Evaluation. BMC Med. Educ. 2022, 22, 25. [Google Scholar] [CrossRef] [PubMed]
- Ben-Arye, E.; Keshet, Y.; Schiff, A.; Zollman, C.; Portalupi, E.; Nave, R.; Shaham, D.; Samuels, N.; Schiff, E. From COVID-19 Adversity Comes Opportunity: Teaching an Online Integrative Medicine Course. BMJ Support. Palliat. Care 2021. [Google Scholar] [CrossRef] [PubMed]
- Mastoras, G.; Farooki, N.; Willinsky, J.; Dharamsi, A.; Somers, A.; Gray, A.; Yaphe, J.; Dalseg, T.; O’Connor, E. Rapid Deployment of a Virtual Simulation Curriculum to Prepare for Critical Care Triage during the COVID-19 Pandemic. Can. J. Emerg. Med. 2022, 24, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Schallenburger, M. Outcome Evaluation of a Case-Based Blended Learning Format in Palliative Care Teaching. WAT der DG Palliativmedizin, 10 March 2018 in Göttingen, Germany. Available online: https://www.dgpalliativmedizin.de/neuigkeiten/vortraege-wat-2018.html (accessed on 20 September 2022).
- Unipark. Available online: https://www.unipark.com/ (accessed on 14 July 2022).
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES-A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist 2000, 5, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Raupach, T.; Münscher, C.; Beißbarth, T.; Burckhardt, G.; Pukrop, T. Towards Outcome-Based Programme Evaluation: Using Student Comparative Self-Assessments to Determine Teaching Effectiveness. Med. Teach. 2011, 33, e446–e453. [Google Scholar] [CrossRef]
- Jansen, G.; Latka, E.; Behrens, F.; Zeiser, S.; Scholz, S.; Janus, S.; Kinzel, K.; Thaemel, D.; Kottkamp, H.W.; Rehberg, S.; et al. Kliniksanitäter. Ein Interprofessionelles Blended-Learning-Konzept Zur Weiterqualifikation von Rettungsdienst-Und Medizinischem Personal Zum Einsatz Auf Intensivstationen Und in Notaufnahmen Während Der COVID-19-Pandemie. Anaesthesist 2021, 70, 13. [Google Scholar] [CrossRef]
- Curran, V.; Lockyer, J.; Sargeant, J.; Fleet, L. Evaluation of Learning Outcomes in Web-Based Continuing Medical Education. Acad. Med. 2006, 81, S30–S34. [Google Scholar] [CrossRef]
- Kirkpatrick, D.L. Evaluating Training Programs; Berret-Koehler Publishers, Inc.: San Francisco, CA, USA, 1994. [Google Scholar]
- Cotogni, P.; Saini, A.; de Luca, A. In-Hospital Palliative Care: Should We Need to Reconsider What Role Hospitals Should Have in Patients with End-Stage Disease or Advanced Cancer? J. Clin. Med. 2018, 7, 18. [Google Scholar] [CrossRef]
- Nehls, W.; Delis, S.; Haberland, B.; Maier, B.O.; Sänger, K.; Tessmer, G.; Radbruch, L.; Bausewein, C. Management of Patients with COVID-19—Recommendations from a Palliative Care Perspective. Pneumologie 2020, 74, 652–659. [Google Scholar] [CrossRef]
- Arenella, C.; Yox, S.; Eckstein, D.S.; Ousley, A. Expanding the Reach of a Cancer Palliative Care Curriculum through Web-Based Dissemination: A Public-Private Collaboration. J. Cancer Educ. 2010, 25, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Taroco, A.L.C.; de Oliveira Valente, T.C.; Carbogim, C.S. Distance Learning for Updating Health Professionals in Palliative Care: A Systematic Review. BMJ Support. Palliat. Care 2017, 7, 205–211. [Google Scholar] [CrossRef] [PubMed]
- DeNofrio, J.C.; Verma, M.; Kosinski, A.S.; Navarro, V.; Taddei, T.H.; Volk, M.L.; Bakitas, M.; Ramchandran, K. Palliative Care Always: Hepatology—Virtual Primary Palliative Care Training for Hepatologists. Hepatol. Commun. 2022, 6, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Pelayo, M.; Cebrián, D.; Areosa, A.; Agra, Y.; Izquierdo, J.V.; Buendía, F. Effects of Online Palliative Care Training on Knowledge, Attitude and Satisfaction of Primary Care Physicians. BMC Fam. Pract. 2011, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Kneebone, R.L.; Scott, W.; Darzi, A.; Horrocks, M. Simulation and clinical practice: Strengthening the relationship. Med. Educ. 2004, 38, 1095–1102. [Google Scholar] [CrossRef]
- Moon, H.; Hyun, H.S. Nursing students’ knowledge, attitude, self-efficacy in blended learning of cardiopulmonary resuscitation: A randomized controlled trial. BMC Med. Educ. 2019, 19, 414. [Google Scholar] [CrossRef]


{kind=link}
| No. | Statement | Competency |
|---|---|---|
| 1 | I am familiar with the four dimensions of palliative care. | Knowledge |
| 2 | I am able to explain different models of palliative care delivery. | Knowledge |
| 3 | I am capable of naming reasons for incorporating specialized palliative care into standard care. | Knowledge |
| 4 | I am aware of symptoms such as dyspnea/cough, restlessness/anxiety, and death rattle and can name interventions to relieve them. | Knowledge |
| 5 | I know to use opioids to treat dyspnea (substance, dose, interval, administration). | Knowledge |
| 6 | I am familiar with palliative sedation and am able to explain its meaning. | Knowledge |
| 7 | I understand the importance of relatives and their care. | Knowledge |
| 8 | I can critically reflect on my own strengths and weaknesses in conducting conversations. | Attitude |
| 9 | I know the SPIKES [19] model and can use it in conversations. | Knowledge |
| 10 | I know how to conduct digital conversations with relatives. | Knowledge |
| 11 | I know different methods of digital communication, can implement them, and can name best practice examples. | Knowledge |
| 12 | I know how to replace facial expressions with other communication methods when wearing a face shield. | Knowledge |
| 13 | I know how to talk to patients about changing and adjusting treatment goals. | Knowledge |
| 14 | I know that treatment decisions require a medical indication as well as the patient’s or the authorized representative’s consent. | Knowledge |
| 15 | I know how to talk to patients about the triage process. | Knowledge |
| 16 | I can recognize to what extent patient goals are appropriate and achievable. | Knowledge |
| 17 | I know the importance of interprofessional and interdisciplinary collaboration. | Knowledge |
| 18 | I am able to support relatives and patients in saying goodbye. | Knowledge |
| 19 | I am familiar with how tasks are performed in a palliative care ward. | Knowledge |
| 20 | I can interact with severely ill patients without fear. | Attitude |
| 21 | I can interact with people at the end of their life knowing that I cannot fully understand their specific situation. | Attitude |
| 22 | I am able to reflect on my own attitude toward death and dying. | Attitude |
| 23 | Interacting with dying patients and their relatives forces me to confront my own mortality. | Attitude |
| 24 | I am able to deal with my own mortality. | Attitude |
| Factor | Answers, n (%) | |||||
|---|---|---|---|---|---|---|
| Age | <25 y | 25–34 y | 35–44 y | 45–54 y | 55–64 y | >64 y |
| 1 (4) | 8 (33) | 9 (37) | 5 (20) | 1 (4) | 0 (0) | |
| Gender | Male | Female | Other | |||
| 14 (58) | 10 (42) | 0 (0) | ||||
| Work experience | <5 y | 5–9 y | >10 y | |||
| 5 (22) | 7 (30) | 11 (48) | ||||
| Experience in intensive care medicine | yes | no | ||||
| 17 (71) | 7 (29) | |||||
| No. | Statement | Factor | Agreement |
|---|---|---|---|
| 1 | The e-learning tool was user-friendly. | Structure | 96% |
| 2 | The amount of time needed to complete the e-learning program was reasonable. | Efficiency | 83% |
| 3 | The e-learning tool is suitable for deepening/consolidating knowledge about caring for seriously ill and dying patients in a pandemic. | Comprehension | 96% |
| 4 | The content of the e-learning tool is clearly presented. | Structure | 96% |
| 5 | The e-learning tool is visually appealing. | Structure | 96% |
| 6 | The e-learning tool is relevant to my work. | Effectiveness | 92% |
| 7 | The e-learning tool is useful for my work. | Effectiveness | 100% |
| 8 | The “checklist telephone call” is a helpful tool that I will use in the future. | Effectiveness | 88% |
| 9 | The recommendation “180 s/6 items” is a helpful tool that I will use in the future. | Effectiveness | 88% |
| 10 | The videos help me transfer my knowledge to daily tasks. | Structure | 83% |
| 11 | The important issues in dealing with severely ill or dying patients are addressed completely. | Comprehension | 92% |
| 12 | The layout is useful for targeting specific topics. | Structure | 96% |
| 13 | I will use the e-learning tool for specific questions in the future. | Satisfaction | 84% |
| 14 | Overall, I am satisfied with the e-learning tool. | Overall Satisfaction | 96% |
| Factor | n | 95% CI | SE (%) |
|---|---|---|---|
| 1 | 18 | 0.37–0.74 | 0.087 |
| 2 | 20 | 0.22–0.62 | 0.095 |
| 3 | 20 | 0.30–0.77 | 0.112 |
| 4 | 20 | 0.20–0.57 | 0.089 |
| 5 | 20 | 0.22–0.62 | 0.095 |
| 6 | 20 | 0.34–0.73 | 0.092 |
| 7 | 20 | 0.32–0.78 | 0.108 |
| 8 | 20 | 0.18–0.55 | 0.088 |
| 9 | 20 | 0.25–0.64 | 0.093 |
| 10 | 20 | 0.48–0.74 | 0.063 |
| 11 | 20 | 0.41–0.66 | 0.058 |
| 12 | 20 | 0.36–0.72 | 0.086 |
| 13 | 20 | 0.24–0.61 | 0.088 |
| 14 | 19 | 0.08–0.52 | 0.105 |
| 15 | 19 | 0.32–0.64 | 0.077 |
| 16 | 19 | 0.18–0.54 | 0.084 |
| 17 | 19 | 0.09–0.55 | 0.110 |
| 18 | 19 | 0.16–0.49 | 0.077 |
| 19 | 19 | 0.20–0.64 | 0.103 |
| 20 | 19 | 0.10–0.42 | 0.077 |
| 21 | 19 | 0.13–0.53 | 0.095 |
| 22 | 19 | 0.01–0.29 | 0.065 |
| 23 | 19 | 0.02–0.30 | 0.067 |
| 24 | 19 | −0.04–0.20 ** | 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwartz, J.; Schallenburger, M.; Tenge, T.; Batzler, Y.-N.; Schlieper, D.; Kindgen-Milles, D.; Meier, S.; Niegisch, G.; Karger, A.; Roderburg, C.; et al. Palliative Care e-Learning for Physicians Caring for Critically Ill and Dying Patients during the COVID-19 Pandemic: An Outcome Evaluation with Self-Assessed Knowledge and Attitude. Int. J. Environ. Res. Public Health 2022, 19, 12377. https://doi.org/10.3390/ijerph191912377
Schwartz J, Schallenburger M, Tenge T, Batzler Y-N, Schlieper D, Kindgen-Milles D, Meier S, Niegisch G, Karger A, Roderburg C, et al. Palliative Care e-Learning for Physicians Caring for Critically Ill and Dying Patients during the COVID-19 Pandemic: An Outcome Evaluation with Self-Assessed Knowledge and Attitude. International Journal of Environmental Research and Public Health. 2022; 19(19):12377. https://doi.org/10.3390/ijerph191912377
Chicago/Turabian StyleSchwartz, Jacqueline, Manuela Schallenburger, Theresa Tenge, Yann-Nicolas Batzler, Daniel Schlieper, Detlef Kindgen-Milles, Stefan Meier, Günter Niegisch, André Karger, Christoph Roderburg, and et al. 2022. "Palliative Care e-Learning for Physicians Caring for Critically Ill and Dying Patients during the COVID-19 Pandemic: An Outcome Evaluation with Self-Assessed Knowledge and Attitude" International Journal of Environmental Research and Public Health 19, no. 19: 12377. https://doi.org/10.3390/ijerph191912377
APA StyleSchwartz, J., Schallenburger, M., Tenge, T., Batzler, Y.-N., Schlieper, D., Kindgen-Milles, D., Meier, S., Niegisch, G., Karger, A., Roderburg, C., & Neukirchen, M. (2022). Palliative Care e-Learning for Physicians Caring for Critically Ill and Dying Patients during the COVID-19 Pandemic: An Outcome Evaluation with Self-Assessed Knowledge and Attitude. International Journal of Environmental Research and Public Health, 19(19), 12377. https://doi.org/10.3390/ijerph191912377