
Impact of the COVID-19 Pandemic on Paediatric Dental Treatment: A Retrospective Study in Banja Luka, Bosnia and Herzegovina
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
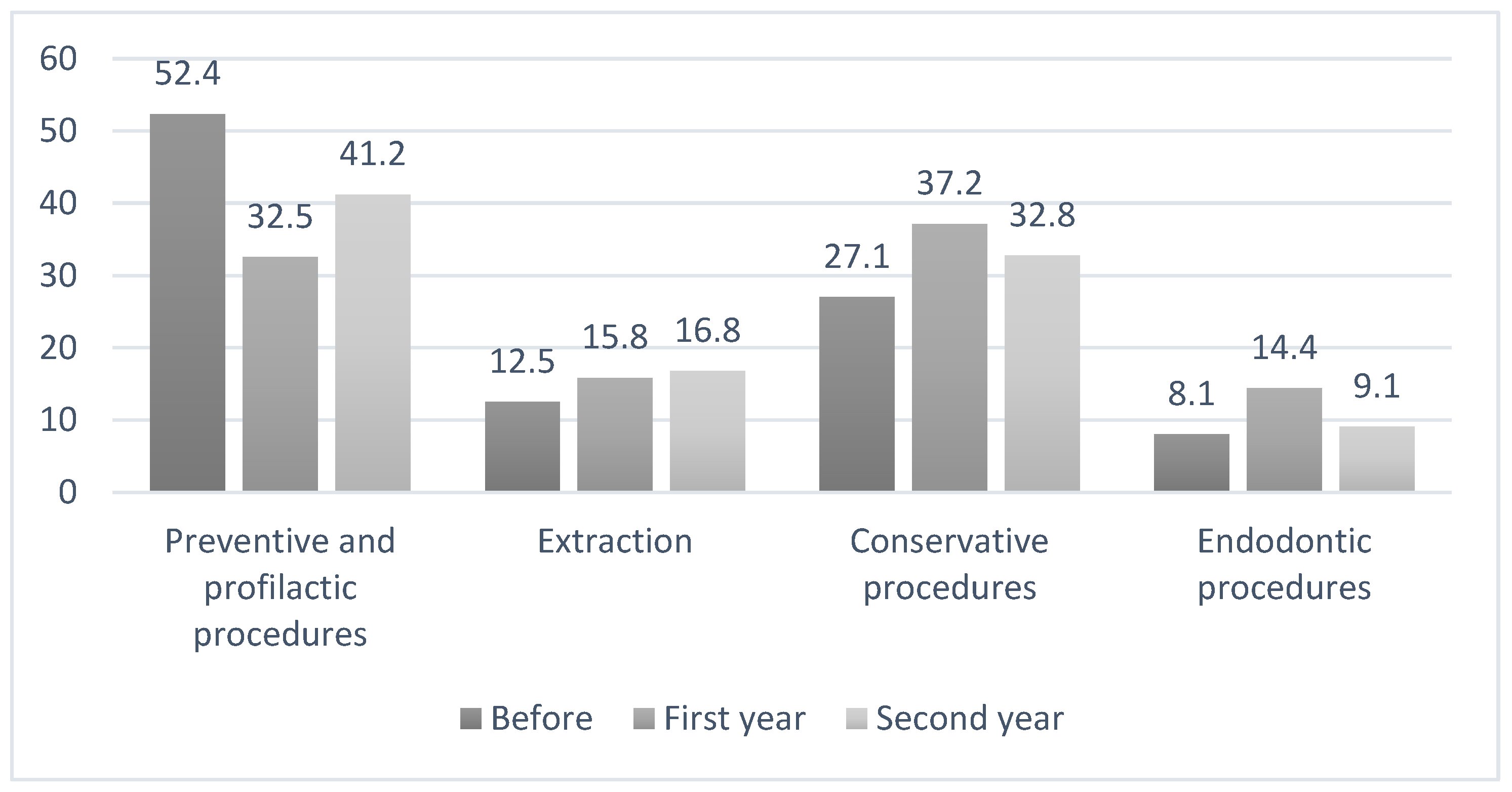
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| COVID-19 | Coronavirus disease 19 |
| WHO | World Health Organization |
| ART | Atraumatic Restorative Treatment |
References
- Tonkaboni, A.; Amirzade Iranaq, M.H.; Ziaei, H.; Ather, A. Impact of COVID-19 on dentistry. Adv. Exp. Med. Biol. 2021, 1318, 623–636. [Google Scholar] [PubMed]
- Mallineni, S.K.; Innes, N.P.; Raggio, D.P.; Araujo, M.P.; Robertson, M.D.; Jayaraman, J. Coronavirus disease (COVID-19): Characteristics in children and considerations for dentists providing their care. Int. J. Paediatr. Dent. 2020, 30, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzano, G.F.; Ingenito, A.; Cantile, T. COVID-19 disease in children: What dentists should know and do to prevent viral spread. The Italian point of view. Int. J. Environ. Res. Public Health 2020, 17, 3642. [Google Scholar] [CrossRef]
- World Health Organization. Considerations for the Provision of Essential Oral Health Services in the Context of COVID-19: Interim Guidance, 3 August 2020. Available online: https://www.who.int/publications/i/item/who-2019-nCoV-oral-health-2020.1 (accessed on 28 July 2022).
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed 2020, 91, 157–160. [Google Scholar] [PubMed]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection control in dental practice during the COVID 19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef] [PubMed]
- AlHayyan, W.A.; AlShammari, K.; AlAjmi, F.; Pani, S.C. The Impact of COVID-19 on Dental Treatment in Kuwait—A Retrospective Analysis from the Nation’s Largest Hospital. Int. J. Environ. Res. Public Health 2022, 19, 9275. [Google Scholar] [CrossRef]
- Jayaraman, J.; Dhar, V.; Moorani, Z.; Donly, K.; Tinanoff, N.; Mitchell, S.; Wright, T. Impact of COVID-19 on pediatric dental practice in the United States. Pediatr. Dent. 2020, 42, 180–183. [Google Scholar]
- Ahmadi, H.; Ebrahimi, A.; Ghorbani, F. The impact of COVID-19 pandemic on dental practice in Iran: A questionnaire-based report. BMC Oral Health 2020, 20, 354. [Google Scholar] [CrossRef]
- Yang, J.; Yang, G.; Jin, R.; Song, G.; Yuan, G. Changes in paediatric dental clinic after reopening during COVID-19 pandemic in Wuhan: A retrospective study. BMJ Open 2022, 12, e048430. [Google Scholar]
- Alamoudi, R.A.; Basudan, S.; Mahboub, M.; Baghlaf, K. Impact of COVID-19 Pandemic on Dental Treatment in Children: A Retrospective Cross-Sectional Analysis in Jeddah City. Clin. Cosmet. Investig. Dent. 2022, 14, 95–102. [Google Scholar] [CrossRef]
- Cagetti, M.G.; Balian, A.; Camoni, N.; Campus, G. Influence of the COVID-19 pandemic on dental emergency admissions in an urgent dental care service in North Italy. Int. J. Environ. Res. Public Health 2021, 18, 1812. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Cieślik, K.; Łaganowski, K.; Gruszczyński, D.; Surdacka, A. The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures. Int. J. Environ. Res. Public Health 2021, 18, 3421. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Costa, D.; Ramírez, J.M.; García Guerrero, I.; Giovannini, G.; Rojo, R.; Gómez-de Diego, R. A retrospective study on the effect of the COVID-19 pandemic on dental treatments in adults. BMC Oral Health 2022, 22, 122. [Google Scholar] [CrossRef] [PubMed]
- Live COVID-19 Vaccination Tracker. Available online: https://covidvax.live/location/bih (accessed on 16 September 2022).
- Casamassimo, P.S.; Townsend, J.A.; Litch, C.S. Pediatric dentistry during and after COVID-19. Pediatr. Dent. 2020, 42, 87–90. [Google Scholar] [PubMed]
- Ilyas, N.; Agel, M.; Mitchell, J.; Sood, S. COVID-19 pandemic: The first wave—An audit and guidance for paediatric dentistry. Br. Dent. J. 2020, 228, 927–931. [Google Scholar]
- Paglia, L. COVID-19 and paediatric dentistry after the lockdown. Eur. J. Paediatr. Dent. 2020, 21, 89. [Google Scholar]
- Vuković, A.; Mandić-Rajčević, S.; Sava-Rosianu, R.; Betancourt, D.M.; Xhajanka, E.; Hysenaj, N.; Campus, G. Pediatric Dentists’ Service Provisions in South-East Europe during the First Wave of COVID-19 Epidemic: Lessons Learned about Preventive Measures and Personal Protective Equipment Use. Int. J. Environ. Res. Public Health 2021, 18, 11795. [Google Scholar] [CrossRef]
- Dolic, O.; Vojinovic, J.; Djukanovic, D.; Cupic, S.; Sukara, S.; Obradovic, M.; Kojic, Z.; Trtic, N. Caries prevalence in the primary and permanent dentition of rural and urban children in the municipality of Banja Luka, Bosnia and Herzegovina. Oral Health Dent. Manag. 2010, 9, 39–47. [Google Scholar]
- Obradović, M.; Dolić, O.; Sukara, S.; Knežević, N.; Kojić, Ž. Identifying risk factors of severe early childhood caries in infants from Bosnia and Herzegovina. Cent. Eur. J. Public Health 2020, 28, 279–285. [Google Scholar] [CrossRef]
- Eggmann, F.; Haschemi, A.A.; Doukoudis, D.; Filippi, A.; Verna, C.; Walter, C.; Weiger, R.; Zitzmann, N.U.; Bornstein, M.M. Impact of the COVID-19 pandemic on urgent dental care delivery in a Swiss university center for dental medicine. Clin. Oral Investig. 2021, 25, 5711–5721. [Google Scholar] [CrossRef]
- OECD iLibrary. Impact of COVID-19 in Bosnia and Herzegovina. Available online: https://www.oecd-ilibrary.org/sites/f0011603-en/index.html?itemId=/content/component/f0011603-en (accessed on 17 August 2022).
- Ibrahim, M.S.; Alibrahim, H.; Al Madani, A.; Alamri, A.; Bamashmous, M.; Tounsi, A. Fear factor in seeking dental care among Saudis during COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10589. [Google Scholar] [CrossRef] [PubMed]
- Elalouf, A.; Moran, R.; Yaron, B.; Oman, M. Pediatric Dental Emergency Visits and Treatment during Lockdown in the COVID-19 Pandemic: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 3774. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.R.; Mathew, M.G.; Suresh, S.G.; Varma, S.R.; Elsubeihi, E.S.; Arshad, F.; Elkareimi, Y.; Elsahn, N.A.; Khalil, E. Pediatric dental emergency management and parental treatment preferences during COVID-19 pandemic as compared to 2019. Saudi J. Biol. Sci. 2021, 28, 2591–2597. [Google Scholar] [CrossRef] [PubMed]
- Abramovitz, I.; Palmon, A.; Levy, D.; Karabucak, B.; Kot-Limon, N.; Shay, B.; Kolokythas, A.; Almoznino, G. Dental care during the coronavirus disease 2019 (COVID-19) outbreak: Operatory considerations and clinical aspects. Quintessence Int. 2020, 51, 418–429. [Google Scholar]
- Cirillo, N. COVID-19 outbreak: Succinct advice for dentists and oral healthcare professionals. Clin. Oral Investig. 2020, 24, 2529–2535. [Google Scholar] [CrossRef]


{kind=link}
| Before Pandemic n | First Year n | Second Year n | p-Value (χ2) | |
|---|---|---|---|---|
| New registered patients | 242 | 181 | 337 | <0.01 * (73.1) |
| Dental treatments | 2757 | 1652 | 2585 | 0.7 (196.3) |
| Dental Treatment Procedures | Before Pandemic n (% **) | First Year n (% **) | χ2 | p-Value |
|---|---|---|---|---|
| Oral hygiene training and patient motivation | 327 (11.9%) | 186 (11.3%) | 0.2 | 0.6 |
| Fluoride varnish | 580 (21.1%) | 190 (11.5%) | 468.1 | <0.01 * |
| Fissure sealant | 186 (6.7%) | 93 (5.6%) | 19.2 | 0.2 |
| Dental plaque removal | 351 (12.7%) | 69 (4.1%) | 74.0 | <0.01 * |
| Deciduous tooth extraction | 346 (12.5%) | 262 (15.8%) | 71.6 | <0.01 * |
| Glass ionomer filling | 396 (14.4%) | 354 (21.4%) | 255.4 | <0.01 * |
| Composite filling on anterior teeth | 92 (3.3%) | 46 (2.8%) | 0.9 | 0.3 |
| Composite filling on posterior teeth | 257 (9.3%) | 214 (12.9%) | 11.4 | <0.01 * |
| Temporary filling | 100 (3.6%) | 99 (6.0%) | 121.8 | <0.01 * |
| Temporary endodontic procedures | 81 (2.9%) | 130 (7.9%) | 495.3 | <0.01 * |
| Root canal filling | 41 (1.5%) | 9 (0.5%) | 8.0 | <0.01 * |
| Pearson’s Correlation | r2 = 0.6; p = 0.03 * | |||
| Dental Treatment Procedures | Before Pandemic n (% **) | Second Year n (% **) | χ2 | p-Value |
|---|---|---|---|---|
| Oral hygiene training and patient motivation | 327 (11.8%) | 362 (14.0%) | 4.2 | 0.04 * |
| Fluoride varnish | 580 (21.1%) | 403 (15.6%) | 182.1 | <0.01 * |
| Fissure sealant | 186 (6.7%) | 186 (7.2%) | 0.4 | 0.5 |
| Dental plaque removal | 351 (12.7%) | 115 (4.1%) | 968.7 | <0.01 * |
| Deciduous tooth extraction | 346 (12.5%) | 435 (16.8%) | 145.6 | <0.01 * |
| Glass ionomer filling | 396 (14.3%) | 510 (19.7%) | 19.3 | <0.01 * |
| Composite filling on anterior teeth | 92 (3.3%) | 54 (2.1%) | 74.0 | <0.01 * |
| Composite filling on posterior teeth | 257 (9.3%) | 284 (10.9%) | 3.3 | 0.1 |
| Temporary filling | 100 (3.6%) | 76 (2.9%) | 18.5 | 0.2 |
| Temporary endodontic procedures | 81 (2.9%) | 148 (5.7%) | 231.7 | <0.01 * |
| Root canal filling | 41 (1.4%) | 12 (0.4%) | 13.9 | <0.01 * |
| Pearson’s Correlation | r2 = 0.8; p < 0.01 * | |||
| Dental Treatment Procedures | First Year n (% **) | Second Year n (% **) | χ2 | p-Value |
|---|---|---|---|---|
| Oral hygiene training and patient motivation | 186 (11.3%) | 362 (14.0%) | 5.2 | 0.02 * |
| Fluoride varnish | 190 (11.5%) | 403 (15.6%) | 10.6 | <0.01 * |
| Fissure sealant | 93 (5.6%) | 186 (7.2%) | 35.3 | 0.06 |
| Dental plaque removal | 69 (4.1%) | 115 (4.1%) | 0.2 | 0.6 |
| Deciduous tooth extraction | 262 (15.8%) | 435 (16.8%) | 0.5 | 0.4 |
| Glass ionomer filling | 354 (21.4%) | 510 (19.7%) | 1.2 | 0.2 |
| Composite filling on anterior teeth | 46 (2.8%) | 54 (2.1%) | 20.1 | 0.1 |
| Composite filling on posterior teeth | 214 (12.95%) | 284 (10.9%) | 2.9 | 0.08 |
| Temporary filling | 99 (6.0%) | 76 (2.9%) | 21.7 | <0.01 * |
| Temporary endodontic procedures | 130 (7.9%) | 148 (5.7%) | 65.9 | 0.01 * |
| Root canal filling | 9 (0.5%) | 12 (0.5%) | 0.13 | 0.7 |
| Pearson’s Correlation | R = 0.9; p < 0.01 * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolic, O.; Obradovic, M.; Kojic, Z.; Knezevic, N.; Trtic, N.; Veselinovic, V.; Sukara, S. Impact of the COVID-19 Pandemic on Paediatric Dental Treatment: A Retrospective Study in Banja Luka, Bosnia and Herzegovina. Int. J. Environ. Res. Public Health 2022, 19, 12292. https://doi.org/10.3390/ijerph191912292
Dolic O, Obradovic M, Kojic Z, Knezevic N, Trtic N, Veselinovic V, Sukara S. Impact of the COVID-19 Pandemic on Paediatric Dental Treatment: A Retrospective Study in Banja Luka, Bosnia and Herzegovina. International Journal of Environmental Research and Public Health. 2022; 19(19):12292. https://doi.org/10.3390/ijerph191912292
Chicago/Turabian StyleDolic, Olivera, Marija Obradovic, Zeljka Kojic, Natasa Knezevic, Natasa Trtic, Valentina Veselinovic, and Slava Sukara. 2022. "Impact of the COVID-19 Pandemic on Paediatric Dental Treatment: A Retrospective Study in Banja Luka, Bosnia and Herzegovina" International Journal of Environmental Research and Public Health 19, no. 19: 12292. https://doi.org/10.3390/ijerph191912292
APA StyleDolic, O., Obradovic, M., Kojic, Z., Knezevic, N., Trtic, N., Veselinovic, V., & Sukara, S. (2022). Impact of the COVID-19 Pandemic on Paediatric Dental Treatment: A Retrospective Study in Banja Luka, Bosnia and Herzegovina. International Journal of Environmental Research and Public Health, 19(19), 12292. https://doi.org/10.3390/ijerph191912292