
Global Cross-Border Malaria Control Collaborative Initiatives: A Scoping Review


Abstract
1. Background
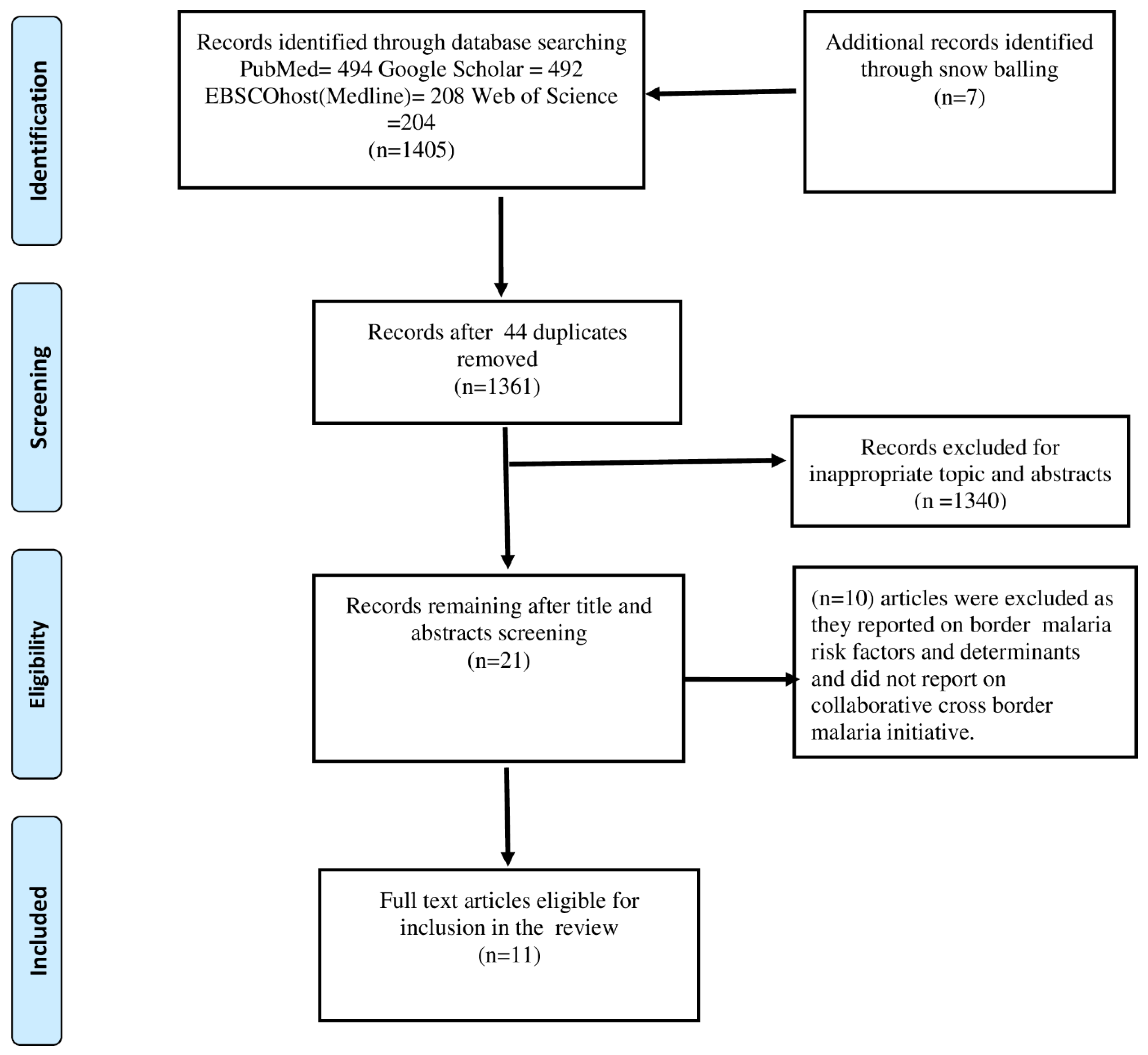
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Extraction
3. Results
3.1. Bi-National Initiatives
3.2. Tri-National Initiatives
3.3. Regional Block Initiatives
3.4. Continental Initiative
3.5. Initiatives without Peer Reviewed Publications
4. Key Collaboration Initiatives Activities
4.1. Information Sharing
4.2. Joint Malaria Prevention and Control Programs
4.3. Resource Sharing
4.4. Funding Mobilisation
4.5. Political Leadership Lobbying
4.6. Infrastructure Development
4.7. Capacity Building
4.8. Outcomes and Challenges
5. Discussion
6. Limitation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. World Malaria Report 2021. 2022. Available online: https://wwwwhoint/publications/i/item/9789240040496 (accessed on 22 February 2022).
- World Health Organization. World Malaria Report 2020: 20 Years of Global Progress and Challenges; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Bhatt, S.; Weiss, D.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.E.; Moyes, C.L.; Henry, A.; Eckhoff, P.A.; et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Nájera, J.A.; González-Silva, M.; Alonso, P.L. Some lessons for the future from the Global Malaria Eradication Programme (1955–1969). PLoS Med. 2011, 8, e1000412. [Google Scholar] [CrossRef] [PubMed]
- Nabarro, D.N.; Tayler, E.M. The “Roll Back Malaria” Campaign; American Association for the Advancement of Science: Washington, DC, USA, 1998. [Google Scholar]
- The Global Fund. 2021. Available online: https://wwwtheglobalfundorg/en/ (accessed on 22 February 2022).
- Poore, P.; Nantulya, V.; Møgedal, S.; Okuonzi, S. The Global Fund to fight AIDS, tuberculosis and malaria (GFATM). Health Policy Plan. 2004, 19, 52–53. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The E-2020 Initiative of 21 Malaria-Eliminating Countries: 2019 Progress Report; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Global Technical Strategy for Malaria 2016–2030; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Feachem, R.G.; Phillips, A.A.; Targett, G.A.; Snow, R.W. Call to action: Priorities for malaria elimination. Lancet 2010, 376, 1517–1521. [Google Scholar] [CrossRef]
- Wangdi, K.; Gatton, M.L.; Kelly, G.C.; Clements, A.C.A. Cross-border malaria: A major obstacle for malaria elimination. Adv. Parasitol. 2015, 89, 79–107. [Google Scholar]
- Arisco, N.J.; Peterka, C.; Castro, M.C. Cross-border malaria in Northern Brazil. Malar. J. 2021, 20, 135. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cross Border Malaria. 2018. Available online: https://wwwwhoint/malaria/mpac/mpac-october2018-session6-border-malariapdf (accessed on 24 February 2022).
- Moonen, B.; Barrett, S.; Tulloch, J.; Jamison, D. Shrinking the Malaria Map: A Prospectus on Malaria Elimination; Global Health Sciences, University of California: San Francisco, CA, USA, 2009. [Google Scholar]
- Gueye, C.S.; Teng, A.; Kinyua, K.; Wafula, F.; Gosling, R.; McCoy, D. Parasites and vectors carry no passport: How to fund cross-border and regional efforts to achieve malaria elimination. Malar. J. 2012, 11, 334. [Google Scholar] [CrossRef]
- Pindolia, D.K.; Garcia, A.J.; Wesolowski, A.; Smith, D.L.; Buckee, C.O.; Noor, A.M.; Snow, R.W.; Tatem, A.J. Human movement data for malaria control and elimination strategic planning. Malar. J. 2012, 11, 205. [Google Scholar] [CrossRef]
- Martens, P.; Hall, L. Malaria on the move: Human population movement and malaria transmission. Emerg. Infect. Dis. 2000, 6, 103. [Google Scholar] [CrossRef]
- Koita, K.; Novotny, J.; Kunene, S.; Zulu, Z.; Ntshalintshali, N.; Gandhi, M.; Gosling, R. Targeting imported malaria through social networks: A potential strategy for malaria elimination in Swaziland. Malar. J. 2013, 12, 219. [Google Scholar] [CrossRef]
- Raman, J.; Gast, L.; Balawanth, R.; Tessema, S.; Brooke, B.; Maharaj, R.; Munhenga, G.; Tshikae, P.; Lakan, V.; Mwamba, T.; et al. High levels of imported asymptomatic malaria but limited local transmission in KwaZulu-Natal, a South African malaria-endemic province nearing malaria elimination. Malar. J. 2020, 19, 152. [Google Scholar] [CrossRef] [PubMed]
- Lover, A.A.; Harvard, K.E.; Lindawson, A.E.; Smith Gueye, C.; Shretta, R.; Gosling, R.; Feachem, R. Regional initiatives for malaria elimination: Building and maintaining partnerships. PLoS Med. 2017, 14, e1002401. [Google Scholar] [CrossRef] [PubMed]
- Njau, J.; Silal, S.P.; Kollipara, A.; Fox, K.; Balawanth, R.; Yuen, A.; White, L.J.; Moya, M.; Pillay, Y.; Moonasar, D. Investment case for malaria elimination in South Africa: A financing model for resource mobilization to accelerate regional malaria elimination. Malar. J. 2021, 20, 344. [Google Scholar] [CrossRef] [PubMed]
- Ren, M. Greater political commitment needed to eliminate malaria. Infec. Dis. Poverty 2019, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Newby, G.; Bennett, A.; Larson, E.; Cotter, C.; Shretta, R.; Phillips, A.A.; Feachem, R.G.A. The path to eradication: A progress report on the malaria-eliminating countries. Lancet 2016, 387, 1775–1784. [Google Scholar] [CrossRef]
- Mendis, K.; Rietveld, A.; Warsame, M.; Bosman, A.; Greenwood, B.; Wernsdorfer, W.H. From malaria control to eradication: The WHO perspective. Trop. Med. Int. Health 2009, 14, 802–809. [Google Scholar] [CrossRef]
- Moonen, B.; Cohen, J.M.; Tatem, A.J.; Cohen, J.; Hay, S.I.; Sabot, O.; Smith, D. A framework for assessing the feasibility of malaria elimination. Malar. J. 2010, 9, 322. [Google Scholar] [CrossRef]
- Nasir, S.I.; Amarasekara, S.; Wickremasinghe, R.; Fernando, D.; Udagama, P. Prevention of re-establishment of malaria: Historical perspective and future prospects. Malar. J. 2020, 19, 452. [Google Scholar] [CrossRef]
- Tatem, A.J.; Rogers, D.J.; Hay, S.I. Estimating the malaria risk of African mosquito movement by air travel. Malar. J. 2006, 5, 57. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Tatem, A.J. Global malaria connectivity through air travel. Malar. J. 2013, 12, 269. [Google Scholar] [CrossRef]
- Dondorp, A.M.; Nosten, F.; Yi, P.; Das, D.; Phyo, A.P.; Tarning, J.; Lwin, K.M.; Ariey, F.; Hanpithakpong, W.; Lee, S.J.; et al. Artemisinin resistance in Plasmodium falciparum malaria. N. Engl. J. Med. 2009, 361, 455–467. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Maharaj, R.; Moonasar, D.; Baltazar, C.; Kunene, S.; Morris, N. Sustaining control: Lessons from the Lubombo spatial development initiative in southern Africa. Malar. J. 2016, 15, 409. [Google Scholar] [CrossRef]
- Sharp, B.L.; Kleinschmidt, I.; Streat, E.; Maharaj, R.; Barnes, K.I.; Durrheim, D.N.; Ridl, F.C.; Morris, N.; Seocharan, I.; Kunene, S.; et al. Seven years of regional malaria control collaboration—Mozambique, South Africa, and Swaziland. Am. J. Trop. Med. Hyg. 2007, 76, 42–47. [Google Scholar] [CrossRef]
- Xia, Z.-G.; Wang, R.-B.; Wang, D.-Q.; Feng, J.; Zheng, Q.; Deng, C.-S.; Abdulla, S.; Guan, Y.-Y.; Ding, W.; Yao, J.-W.; et al. China–Africa cooperation initiatives in malaria control and elimination. Adv. Parasitol. 2014, 86, 319–337. [Google Scholar]
- Moonasar, D.; Maharaj, R.; Kunene, S.; Candrinho, B.; Saute, F.; Ntshalintshali, N.; Morris, N. Towards malaria elimination in the MOSASWA (Mozambique, South Africa and Swaziland) region. Malar. J. 2016, 15, 419. [Google Scholar] [CrossRef]
- Gosling, R.D.; Whittaker, M.; Gueye, C.S.; Fullman, N.; Baquilod, M.; Kusriastuti, R.; Feachem, R.G. Malaria elimination gaining ground in the Asia Pacific. Malar. J. 2012, 11, 346. [Google Scholar] [CrossRef]
- Raman, J.; Fakudze, P.; Sikaala, C.H.; Chimumbwa, J.; Moonasar, D. Eliminating malaria from the margins of transmission in Southern Africa through the Elimination 8 Initiative. Trans. R. Soc. S. Afr. 2021, 76, 137–145. [Google Scholar] [CrossRef]
- Khadka, A.; Perales, N.A.; Wei, D.J.; Gage, A.D.; Haber, N.; Verguet, S.; Patenaude, B.; Fink, G. Malaria control across borders: Quasi-experimental evidence from the Trans-Kunene malaria initiative (TKMI). Malar. J. 2018, 17, 224. [Google Scholar] [CrossRef]
- Kooma, E. Ministry of Health, Zambia and the Ministry of Health and Social Services, Namibia. JOJ Nurs. Health Care 2017, 5, 138–149. [Google Scholar]
- Krisher, L.K.; Krisher, J.; Ambuludi, M.; Arichabala, A.; Beltrán-Ayala, E.; Navarrete, P.; Ordoñez, T.; Polhemus, M.E.; Quintana, F.; Rochford, R.; et al. Successful malaria elimination in the Ecuador-Peru border region: Epidemiology and lessons learned. Malar. J. 2016, 15, 573. [Google Scholar] [CrossRef]
- Sambo, L.G.; Ki-Zerbo, G.; Kirigia, J.M. Malaria control in the African Region: Perceptions and viewspoints on proceedings of the Africa Leaders Malaria Alliance (ALMA). BMC Proc. 2011, 5, 1–8. [Google Scholar] [CrossRef]
- Saldanha, R.; Mosnier, E.; Barcellos, C.; Carbunar, A.; Charron, C.; Desconnets, J.C.; Guarmit, B.; Gomes, M.D.; Mandon, T.; Mendes, A.M.; et al. Contributing to elimination of cross-border malaria through a standardized solution for case surveillance, data sharing, and data interpretation: Development of a cross-border monitoring system. JMIR Public Health Surveill. 2020, 6, e15409. [Google Scholar] [CrossRef]
- Amazon Malaria Initiative. 2021. Available online: https://wwwresearchgatenet/publication/277555373_Mid-term_performance_evaluation_of_Amazon_Malaria_Initiative_AMI (accessed on 24 February 2022).
- Mekong Basin Disease Surveillance Network. 2021. Available online: https://www.nti.org/about/projects/mekong-basin-disease-surveillance-network/ (accessed on 22 February 2022).
- Elimination 8. 2018. Available online: https://malariaelimination8.org/about-us/ (accessed on 20 April 2020).
- MESA Alliannce. 2021. Available online: https://mesamalaria.org/mesa-track/sahel-malaria-elimination-initiative-same-initiative (accessed on 22 February 2022).
- EndMalaria. 2019. Available online: https://endmalaria.org/sites/default/files/u221/3_Michael%20Katende.pdf (accessed on 26 May 2022).
- Malaria Consortium. 2022. Available online: https://malariaconsortium.org/news/136.htm (accessed on 22 February 2022).
- Asia Pacific Malaria Elimination on Network. 2021. Available online: https://wwwapmenorg/about (accessed on 23 February 2022).
- Teklehaimanot, A.; Mejia, P. Malaria and poverty. Ann. N. Y. Acad. Sci. 2008, 1136, 32–37. [Google Scholar] [CrossRef]
- Cohen, J.M.; Smith, D.L.; Cotter, C.; Ward, A.; Yamey, G.; Sabot, O.J.; Moonen, B. Malaria resurgence: A systematic review and assessment of its causes. Malar. J. 2012, 11, 122. [Google Scholar] [CrossRef]
- Leach-Kemon, K.; Chou, D.P.; Schneider, M.T.; Tardif, A.; Dieleman, J.L.; Brooks, B.P.; Hanlon, M.; Murray, C.J. The global financial crisis has led to a slowdown in growth of funding to improve health in many developing countries. Health Aff. 2012, 31, 228–235. [Google Scholar] [CrossRef]
- ALMA. Cross-Border Collaborations Set to Defeat Malaria in Africa. 2021. Available online: https://alma2030org/news/cross-border-collaborations-set-to-defeat-malaria-in-africa/ (accessed on 22 February 2022).
- Ope, M.; Sonoiya, S.; Kariuki, J.; Mboera, L.E.; Gandham, R.N.; Schneidman, M.; Kimura, M. Regional initiatives in support of surveillance in East Africa: The East Africa integrated disease surveillance network (EAIDSNet) experience. Emerg. Health Threat. J. 2013, 6, 19948. [Google Scholar] [CrossRef]
- Liverani, M.; Teng, S.; Le, M.S.; Coker, R. Sharing public health data and information across borders: Lessons from Southeast Asia. Glob. Health 2018, 14, 94. [Google Scholar] [CrossRef]
- Van Panhuis, W.G.; Paul, P.; Emerson, C.; Grefenstette, J.; Wilder, R.; Herbst, A.J.; Heymann, D.; Burke, D.S. A systematic review of barriers to data sharing in public health. BMC Public Health 2014, 14, 1144. [Google Scholar] [CrossRef]
- Phommasack, B.; Jiraphongsa, C.; Ko Oo, M.; Bond, K.C.; Phaholyothin, N.; Suphanchaimat, R.; Ungchusak, K.; Macfarlane, S.B. Mekong Basin Disease Surveillance (MBDS): A trust-based network. Emerg. Health Threat. J. 2013, 6, 19944. [Google Scholar] [CrossRef]
- Gordon, A.; Vander Meulen, R.J.; Maglior, A. The 2019 Isdell: Flowers Cross Border Malaria Initiative Round Table: Community engagement in the context of malaria elimination. Malar. J. 2019, 18, 432. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Name of Collaborative Initiative | Region/ Countries | Type of Collaboration | Operational Years | Aims/Objective(s) | Summary of Collaboration Key Activities | Outcomes | Challenges |
|---|---|---|---|---|---|---|---|---|
| Maharaj et al. (2016) [31] | Lubombo Spatial Development Initiative (LSDI) | Mozambique, South Africa, Swaziland | Tri-national | 1999–2011 | To accelerate socio-economic development in the region | The three countries shared technical expertise along the border regions of Kwa Zulu Natal, Eastern Swaziland and Southern Mozambique. A joint Indoor Residual Spraying (IRS) and case management program was implemented along the three nations common border region. | The initiative led to a significant overall reduction in malaria burden in the border regions. South Africa recorded a 99% decrease in malaria cases whilst Swaziland recorded a 98% reduction in malaria cases In Swaziland, malaria incidence declined from 28/100,000 pop in 2000 to <3/100,000 pop by 2001 In Mozambique, malaria prevalence declined from an average of 70% to less than 10% in (Zone 1–Zone 3). Manhica and Matola regions. | The financial burden for operating the initiative was huge. Financial commitment by member states did not materialise leading to closure of the initiative. |
| Sharp et al. (2007) [32] | Lubombo Spatial Development Initiative (LSDI) | Mozambique, Swaziland and South Africa | Tri-national | 1999–2011 | To accelerate socio-economic development within the three countries common border regions | The initiative instituted an Indoor Residual Spraying (IRS) program along the three country border regions. Entomological surveillance activities were conducted along the three countries’ common border regions. The initiative instituted routine monitoring of malaria cases along the border regions. | A significant reduction in Plasmodium falciparum prevalence was recorded from 60% in 1999 to 33% by 2005 within the Lubombo region i.e., in Mozambique project implementation zones (Zone 1–3), malaria prevalence declined in Zone 1 from 65% in 1999 to 4% by 2005. In Zone 3, prevalence declined from 70% in year 2000 to 33% in 2005. In Zone 2, prevalence declined from 69% in 2000 to 20% in 2005. Swaziland recorded a significant decline in malaria cases from 1395 in year 2000 to 200 cases by 2005. In South Africa, KwaZulu Natal district, malaria cases declined from 41077 in 1999 to 1771 by 2005, whilst in Mpumalanga province, malaria cases declined from 13656 in 1999 to 3099 by 2005 A significant reduction in vector abundancy and density was recorded in Mozambique attributable to the an effective IRS program i.e., Anopheles. gambiae s.l. catches declined from 5077 mosquitoes (pre-IRS) to 969 mosquitoes (post-IRS) An. funestus s.l. catches declined from 8830 (pre IRS) to 2107 (post IRS) Vector density declined from 14.9 (pre IRS to 0.2 (post IRS) for An. arabiensis ss Density for An. funestus s.s. declined from 26.3 (pre IRS) to 0.9 (post IRS) Sporozite index for An. arabiensis s.s. declined from 7.1 (pre-IRS) to 0.8 (post-IRS) An. funestus s.s. sporozite index declined from 1.2 (pre-IRS) to 0.02 (post-IRS) | Not indicated |
| Xia et al. (2014) [33] | China-Africa Initiative | China and Africa | Continental | 1950s-present | To foster closer socio-economic China and Africa ties | China supports Africa medical services through training and supply of equipment. China provides academic exchanges and training programs for health workers and academics China deploys medical personnel to African countries China donates anti-malaria medicines to various African countries China has piloted malaria elimination programs in African countries. China supports the registration of pharmaceutical products. | China supports construction of thirty malaria research centres across thirty (30) across African countries China piloted malaria elimination programs in African countries | Not indicated |
| Moonasar et al. (2016) [34] | MOSASWA (Mozambique, South Africa and Swaziland) | Mozambique, South Africa and Swaziland | Tri-national | 2015-Current | To accelerate transition from control to pre- elimination in Southern Mozambique and accelerate the transition from pre elimination to elimination in Eswatini and South Africa. | The initiative implements a joint support and expanded coverage IRS program. The partnership has scaled up drug based parasite clearance strategies and accelerated transition from pre-elimination to zero local transmission. The initiative mobilise resources and advocates for increased long term financing of malaria control and elimination programs The initiative has also created strategies targeted towards migrant and mobile populations | Not indicated | Not indicated |
| Gosling et al. (2012) [35] | Asia Pacific Malaria Elimination Network | Asia (Vanuatu, Solomon Islands, Bhutan, China, Democratic Republic of Korea, Indonesia, Malaysia, Philippines, Republic of Korea, Sri Lanka, | Regional | 2009-current | Strengthen regional and multi sectoral collaboration around evidence based practises to reach malaria elimination goals. | APMEN designs and implement training programs and also promotes the use of Geographic Information Systems (GIS). The alliance has developed community engagement strategies for malaria elimination. The partnership provides funding for training program in member states The alliance holds annual technical meetings and produces a series of country cases studies | Not indicated | Not indicated |
| Raman et al. (2021) [36] | Elimination 8 (E8) | Mozambique, Zimbabwe, Malawi, Namibia, South Africa, Eswatini, Lesotho, Angola Botswana | Regional | 2010-present | To strengthen regional collaboration in Southern Africa toward malaria elimination goals. To facilitate policy harmonisation, reduction of cross border transmission and mobilise additional resources | The initiative was created by Ministers’ of Health of SADC member states to enhance cross border malaria control initiatives and deployment of malaria health units at strategic points along the borders. | E8 funded the construction of thirty three (33) health posts in eight (8) SADC countries border regions. The health posts have been credited with a 30% reduction in malaria incidence and 40% reduction in malaria mortality. Through the efforts of the alliance malaria trends have been on a decline in certain Southern African countries. i.e. In South Africa, malaria cases declined from 30 000 in 2017 to 12 000 in 2019 In Namibia, malaria cases declined from 60 000 in 2017 to <3000 in 2019. The initiative has created malaria situation rooms The group keeps the malaria issue on the agenda at SADC summits. The initiative plays a pivotal role in strengthening political commitment for malaria E8 lobbied for increased domestic funding among member states | Member states lack internal domestic financing capacity to independently support malaria control programs. The initiative is totally funded by donors. There is ministerial and technical team policy misalignment Countries reportedly reluctant to share malaria epidemiological data on regional E8 platform despite signing protocols Countries within the alliance are reluctant to adopt new technologies and techniques brought through the initiative An existing overburdened health systems with endemic bottlenecks within the region |
| Khadka et al. (2018) [37] | Trans-Kunene Malaria Initiative | Angola and Namibia | Bi-national | 2012-current | To enhance bilateral collaboration, joint malaria control between Angola and Namibia along the northern Namibia and Southern Angola border region | Is an arrangement between government of Namibia and Angola The initiative was formed to enhance cross border malaria control in the two countries border regions of Cunene-Cuando Cabango. The partnership facilitate sharing of technical scientific information between the two countries | A quasi-experimental intervention conducted by the partnership over two years utilising treated bed nets; led to a significant reduction of odds of malaria fever among children by 54% (aOR 0.46 95% CI: 0.29–0.73). Among children under two (2) years, the odds of fever were reduced by 71% (aOR 0.39 95% CI: 0.23–0.65). Among children over two (2) years, the odds of fever were reduced by 47% (aOR 0.53 95% CI: 0.30–0.65). | Not indicated |
| Kooma et al. (2017) [38] | Trans-Zambezi Malaria Initiative | Angola, Namibia, Botswana, Zambia, and Zimbabwe | Regional | 2006-current | The collaboration aims to accelerate the reduction of malaria transmission among the border communities through implementation of coordinated cost effective malaria control activities | The initiative promotes cross border malaria collaboration as well as support SADC and E8 malaria elimination goals | Not indicated | Not indicated |
| Krisher et al. (2016) [39] | Ecuador–Peru Collaboration (Unofficial) | El Oro Region (Ecuador) and Tumbes Region (Peru) | Bi-national | 1995-current | Collaborative was created unofficially by the two countries health officials to share epidemiological information | Local health officers created an unofficial cross border collaboration initiative for malaria control which resulted in sharing of epidemiological data, resources and conducting operational research | The initiative led to a significant reduction in malaria incidence in El Oro (Ecuador) region from 230 malaria cases per 10,000 pop. in 1999 to <10 cases per 10 000 pop. by year 2012 In Tumbes region (Peru) malaria cases declined from 1800 cases per 10,000 pop. in 1999 to <10 cases per 10,000 pop. by the year 2012 The collaboration between the two nation’s health officials led to the identification of Chloroquine resistance leading to its cessation as a drug of choice. | Not stated |
| Sambo et al. (2009) [40] | Africa Leaders Malaria Alliance (ALMA) | African Region | Continental | 2009-current | To enhance and sustain African leaders commitment towards malaria elimination | The alliance is composed of African heads of states. The alliance seek to strengthen African leaders commitment to malaria control and elimination. The alliance also aims to strengthen cross border malaria control programs across African states. | Not indicated | Majority of malaria endemic countries lack domestic funding capacity to independently support own malaria control programs |
| Saldanha et al. (2020) [41] | French Guiana-Brazil | French Guiana and Brazil | South America | 1996-present | Cooperative agreement created to improve health status of the two country’s common border region population | Regular sharing of epidemic data | The alliance created a harmonised cross border malaria information system (CBMIS) which improved access to data for all health officials and stakeholder The CBMIS assisted the two countries’ health authorities to timeously assess malaria epidemiologic dynamics in both space and time. | Limited health data access for health official in the two countries and different tools and terminology before adoption of CBMIS |
| Name of Initiative | Region | Initiative Type | Country Composition | Operational Years | Aims and Objective(s) |
|---|---|---|---|---|---|
| Amazon Malaria Initiative (AMI) [42] | Amazon Region | Regional | Brazil, Colombia, Ecuador, Guyana, Guyana, Peru, Suriname | 2001-present | To standardise malaria prevention and control interventions through development of standard treatment guidelines, sentinel surveillance, trials and research. |
| Mekong Malaria Elimination (MME) hub [43] | Greater Mekong Delta sub-region | Regional | Laos, Cambodia, Vietnam, China (Yunnan Province), Myanmar Thailand | 2017-present | To develop and coordinate partnerships and strengthen advocacy communication To provide leading technical support on cross country malaria projects and regional surveillance |
| Zambia Zimbabwe (ZAM-ZIM) [44] | Southern Africa | Bi-national | Zimbabwe and Zambia | 2013-present | To strengthen cross border collaboration and coordination of malaria elimination along Zimbabwe and Zambia border. |
| Sahel Malaria Elimination Initiative (SaME) [45] | Sahel sub-region | Regional | Burkina Faso, Cape Verde, Chad, Mali, Mauritania, Niger, Senegal, Gambia | 2018-present | To accelerate towards the attainment of malaria elimination goals by 2030. To scale up and sustain universal coverage of anti-malarial medicines and mobilizing financing for elimination. To fast-track the introduction of innovative technologies to combat malaria and develop a sub-regional scorecard. |
| Great Lakes Malaria Elimination Initiative (GLMEI) [46] | Central and East African region | Regional | Burundi, Democratic Republic of Congo, Kenya, Rwanda, South Sudan, Uganda, Tanzania | 2019-present | To strengthen control and elimination of malaria in the Africa Great lakes region with main focus on cross border areas. |
| Mozambique Zimbabwe South Africa (MOZIZA) [47] | Southern Africa | Tri-national | Mozambique, South Africa and Zimbabwe | 2011-Unknown | To achieve universal coverage of key malaria interventions To reduce transmission and eliminating malaria in districts which share borders in the three countries |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fambirai, T.; Chimbari, M.J.; Ndarukwa, P. Global Cross-Border Malaria Control Collaborative Initiatives: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 12216. https://doi.org/10.3390/ijerph191912216
Fambirai T, Chimbari MJ, Ndarukwa P. Global Cross-Border Malaria Control Collaborative Initiatives: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12216. https://doi.org/10.3390/ijerph191912216
Chicago/Turabian StyleFambirai, Tichaona, Moses John Chimbari, and Pisirai Ndarukwa. 2022. "Global Cross-Border Malaria Control Collaborative Initiatives: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 19: 12216. https://doi.org/10.3390/ijerph191912216
APA StyleFambirai, T., Chimbari, M. J., & Ndarukwa, P. (2022). Global Cross-Border Malaria Control Collaborative Initiatives: A Scoping Review. International Journal of Environmental Research and Public Health, 19(19), 12216. https://doi.org/10.3390/ijerph191912216