
Evaluation of the Psychometric Properties of the Arab Compulsive Internet Use Scale (CIUS) by Item Response Theory Modeling (IRT)
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Procedure
2.2. Instrument: Compulsive Internet Use Scale (CIUS)
2.3. Statistical Analysis
- -
- represents the discrimination of item
- -
- is the th cutpoint for item
- -
- and is the latent trait of person j.
2.4. Model Assumptions and Fit
2.4.1. Unidimensionality
2.4.2. Local Independence
2.4.3. Monotonicity
2.4.4. Missing Values
2.4.5. Sample Size Requirement
2.4.6. Statistical Software
3. Results
3.1. Unidimensionality
3.2. Local Independence
3.3. Monotonicity
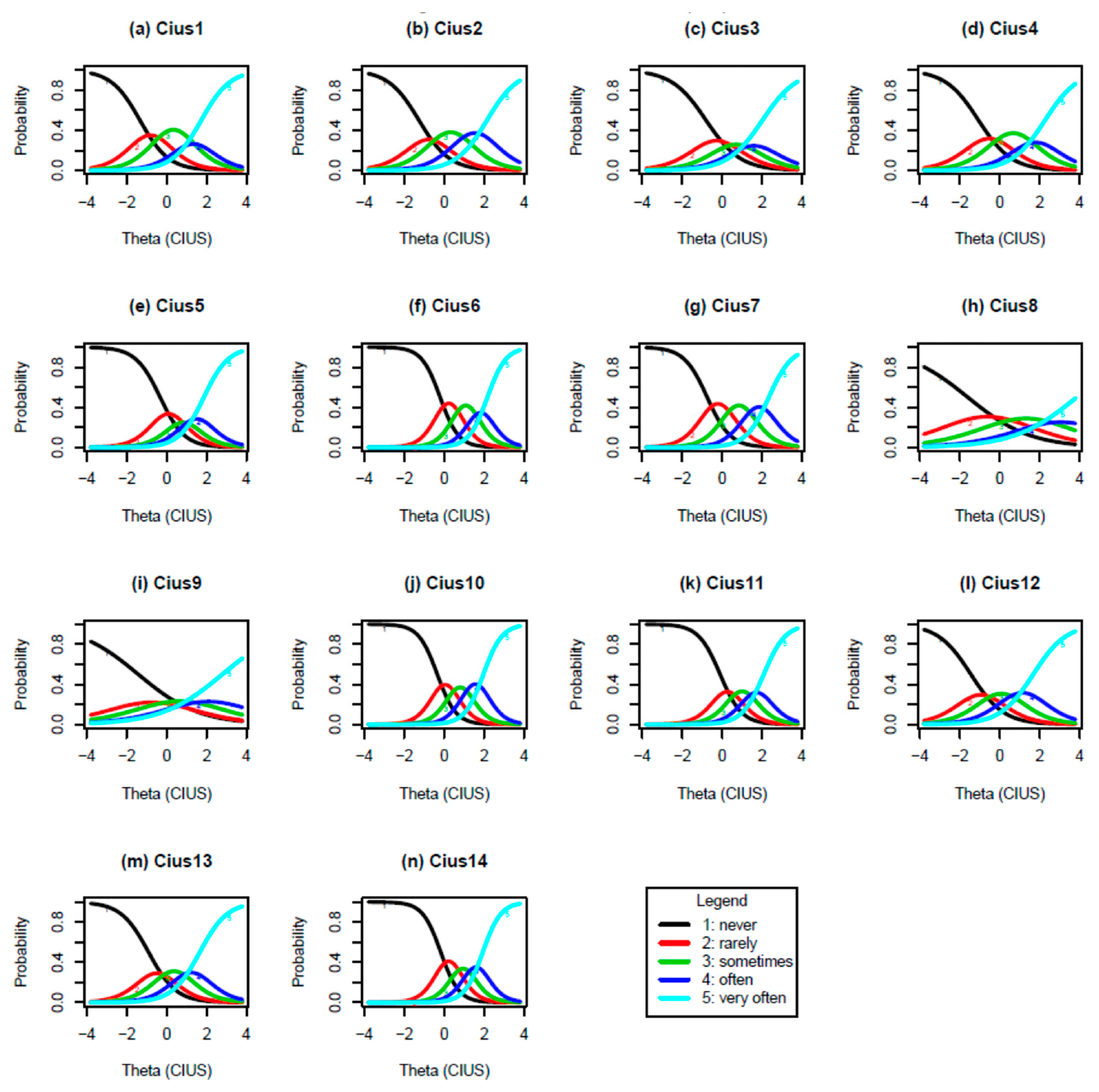
3.3.1. IRT Graded Parameter Estimates
3.3.2. Differential Item Functioning Parameter Estimates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, J.K.; Farrer, L.M.; Gulliver, A.; Bennett, K.; Griffiths, K.M. University Students’ Views on the Perceived Benefits and Drawbacks of Seeking Help for Mental Health Problems on the Internet: A Qualitative Study. JMIR Hum. Factors 2016, 3, e3. [Google Scholar] [CrossRef] [PubMed]
- Zermatten, A.; Khazaal, Y.; Coquard, O.; Chatton, A.; Bondolfi, G. Quality of Web-based information on depression. Depress. Anxiety 2010, 27, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Khazaal, Y.; Chatton, A.; Cochand, S.; Jermann, F.; Osiek, C.; Bondolfi, G.; Zullino, D. Quality of web-based information on pathological gambling. J. Gambl. Stud. 2008, 24, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Greiner, C.; Chatton, A.; Khazaal, Y. Online self-help forums on cannabis: A content assessment. Patient Educ. Couns. 2017, 100, 1943–1950. [Google Scholar] [CrossRef]
- Lecomte, T.; Potvin, S.; Corbiere, M.; Guay, S.; Samson, C.; Cloutier, B.; Francoeur, A.; Pennou, A.; Khazaal, Y. Mobile Apps for Mental Health Issues: Meta-Review of Meta-Analyses. JMIR mHealth uHealth 2020, 8, e17458. [Google Scholar] [CrossRef]
- Riper, H.; Hoogendoorn, A.; Cuijpers, P.; Karyotaki, E.; Boumparis, N.; Mira, A.; Andersson, G.; Berman, A.H.; Bertholet, N.; Bischof, G.; et al. Effectiveness and treatment moderators of internet interventions for adult problem drinking: An individual patient data meta-analysis of 19 randomised controlled trials. PLoS Med. 2018, 15, e1002714. [Google Scholar] [CrossRef]
- Pennou, A.; Lecomte, T.; Potvin, S.; Khazaal, Y. Mobile Intervention for Individuals With Psychosis, Dual Disorders, and Their Common Comorbidities: A Literature Review. Front. Psychiatry 2019, 10, 302. [Google Scholar] [CrossRef]
- Monney, G.; Penzenstadler, L.; Dupraz, O.; Etter, J.F.; Khazaal, Y. mHealth App for Cannabis Users: Satisfaction and Perceived Usefulness. Front. Psychiatry 2015, 6, 120. [Google Scholar] [CrossRef]
- Penzenstadler, L.; Chatton, A.; Van Singer, M.; Khazaal, Y. Quality of Smartphone Apps Related to Alcohol Use Disorder. Eur. Addict. Res. 2016, 22, 329–338. [Google Scholar] [CrossRef]
- Etter, J.F.; Khazaal, Y. The Stop-tabac smartphone application for smoking cessation: A randomized controlled trial. Addiction 2022, 117, 1406–1415. [Google Scholar] [CrossRef]
- Pregowska, A.; Masztalerz, K.; Garlińska, M.; Osial, M. A worldwide journey through distance education—From the post office to virtual, augmented and mixed realities, and education during the COVID-19 pandemic. Educ. Sci. 2021, 11, 118. [Google Scholar] [CrossRef]
- Rapanta, C.; Botturi, L.; Goodyear, P.; Guàrdia, L.; Koole, M. Teaching During and After the Covid-19 Crisis: Refocusing Teacher Presence and Learning Activity. Postdigit. Sci. Educ. 2020, 2, 923–945. [Google Scholar] [CrossRef]
- Wu, C.Y.; Lee, M.B.; Liao, S.C.; Ko, C.H. A nationwide survey of the prevalence and psychosocial correlates of internet addictive disorders in Taiwan. J. Formos. Med. Assoc. 2019, 118, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Durkee, T.; Kaess, M.; Carli, V.; Parzer, P.; Wasserman, C.; Floderus, B.; Apter, A.; Balazs, J.; Barzilay, S.; Bobes, J.; et al. Prevalence of pathological internet use among adolescents in Europe: Demographic and social factors. Addiction 2012, 107, 2210–2222. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Blasco, R.; Robres, A.Q.; Sánchez, A.S. Internet addiction in young adults: A meta-analysis and systematic review. Comput. Hum. Behav. 2022, 130, 107201. [Google Scholar] [CrossRef]
- Lozano-Blasco, R.; Latorre-Martínez, M.; Cortés-Pascual, A. Screen addicts: A meta-analysis of internet addiction adolescence. Child. Youth Serv. Rev. 2022, 135, 106373. [Google Scholar] [CrossRef]
- Colder Carras, M.; Porter, A.M.; Van Rooij, A.J.; King, D.; Lange, A.; Carras, M.; Labrique, A. Gamers’ insights into the phenomenology of normal gaming and game "addiction": A mixed methods study. Comput. Human Behav. 2018, 79, 238–246. [Google Scholar] [CrossRef]
- Saruhanjan, K.; Zarski, A.C.; Schaub, M.P.; Ebert, D.D. Design of a Guided Internet- and Mobile-Based Intervention for Internet Use Disorder-Study Protocol for a Two-Armed Randomized Controlled Trial. Front. Psychiatry 2020, 11, 190. [Google Scholar] [CrossRef]
- Zanetta Dauriat, F.; Zermatten, A.; Billieux, J.; Thorens, G.; Bondolfi, G.; Zullino, D.; Khazaal, Y. Motivations to play specifically predict excessive involvement in massively multiplayer online role-playing games: Evidence from an online survey. Eur. Addict. Res. 2011, 17, 185–189. [Google Scholar] [CrossRef]
- Laier, C.; Wegmann, E.; Brand, M. Personality and Cognition in Gamers: Avoidance Expectancies Mediate the Relationship Between Maladaptive Personality Traits and Symptoms of Internet-Gaming Disorder. Front. Psychiatry 2018, 9, 304. [Google Scholar] [CrossRef] [Green Version]
- Brand, M.; Rumpf, H.J.; Demetrovics, Z.; A, M.U.; Stark, R.; King, D.L.; Goudriaan, A.E.; Mann, K.; Trotzke, P.; Fineberg, N.A.; et al. Which conditions should be considered as disorders in the International Classification of Diseases (ICD-11) designation of “other specified disorders due to addictive behaviors”? J. Behav. Addict. 2020, 11, 150–159. [Google Scholar] [CrossRef]
- Rothen, S.; Briefer, J.F.; Deleuze, J.; Karila, L.; Andreassen, C.S.; Achab, S.; Thorens, G.; Khazaal, Y.; Zullino, D.; Billieux, J. Disentangling the role of users’ preferences and impulsivity traits in problematic Facebook use. PLoS ONE 2018, 13, e0201971. [Google Scholar] [CrossRef]
- Rochat, L.; Bianchi-Demicheli, F.; Aboujaoude, E.; Khazaal, Y. The psychology of “swiping”: A cluster analysis of the mobile dating app Tinder. J. Behav. Addict. 2019, 8, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Lăzăroiu, G.; Kovacova, M.; Siekelova, A.; Vrbka, J. Addictive Behavior of Problematic Smartphone Users: The Relationship between Depression, Anxiety, and Stress. Rev. Contemp. Philos. 2020, 19, 50–56. [Google Scholar]
- Kliestik, T.; Scott, J.; Musa, H.; Suler, P. Addictive Smartphone Behavior, Anxiety Symptom Severity, and Depressive Stress. Anal. Metaphys. 2020, 19, 45–51. [Google Scholar]
- Adams, C.; Grecu, I.; Grecu, G.; Balica, R. Technology-related Behaviors and Attitudes: Compulsive Smartphone Usage, Stress, and Social Anxiety. Rev. Contemp. Philos. 2020, 19, 71–77. [Google Scholar]
- Green, M.; Kovacova, M.; Valaskova, K. Smartphone Addiction Risk, Depression Psychopathology, and Social Anxiety. Anal. Metaphys. 2020, 19, 52–56. [Google Scholar]
- Varfi, N.; Rothen, S.; Jasiowka, K.; Lepers, T.; Bianchi-Demicheli, F.; Khazaal, Y. Sexual Desire, Mood, Attachment Style, Impulsivity, and Self-Esteem as Predictive Factors for Addictive Cybersex. JMIR Ment. Health 2019, 6, e9978. [Google Scholar] [CrossRef]
- Francesco, E.; Khazaal, Y.; Jasiowka, K.; Lepers, T.; Bianchi-Demicheli, F.; Rothen, S. Factor structure of the Cybersex Motives Questionnaire. J. Behav. Addict. 2018, 7, 601–609. [Google Scholar]
- Weinstein, A.M.; Zolek, R.; Babkin, A.; Cohen, K.; Lejoyeux, M. Factors Predicting Cybersex Use and Difficulties in Forming Intimate Relationships among Male and Female Users of Cybersex. Front. Psychiatry 2015, 6, 54. [Google Scholar] [CrossRef]
- Khazaal, Y.; Chatton, A.; Achab, S.; Monney, G.; Thorens, G.; Dufour, M.; Zullino, D.; Rothen, S. Internet Gamblers Differ on Social Variables: A Latent Class Analysis. J. Gambl. Stud. 2017, 33, 881–897. [Google Scholar] [CrossRef] [PubMed]
- Khazaal, Y.; Chatton, A.; Rochat, L.; Hede, V.; Viswasam, K.; Penzenstadler, L.; Berle, D.; Starcevic, V. Compulsive Health-Related Internet Use and Cyberchondria. Eur. Addict. Res. 2021, 27, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Starcevic, V.; Khazaal, Y. Relationships between Behavioural Addictions and Psychiatric Disorders: What Is Known and What Is Yet to Be Learned? Front. Psychiatry 2017, 8, 53. [Google Scholar] [CrossRef]
- Starcevic, V.; Khazaal, Y. Editorial: Problematic Gaming, Personality, and Psychiatric Disorders. Front. Psychiatry 2019, 10, 1004. [Google Scholar] [CrossRef]
- Marmet, S.; Studer, J.; Wicki, M.; Bertholet, N.; Khazaal, Y.; Gmel, G. Unique versus shared associations between self-reported behavioral addictions and substance use disorders and mental health problems: A commonality analysis in a large sample of young Swiss men. J. Behav. Addict. 2019, 8, 664–677. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Jeon, H.J.; Bae, J.N.; Seong, S.J.; Hong, J.P. Prevalence and Psychiatric Comorbidities of Internet Addiction in a Nationwide Sample of Korean Adults. Psychiatry Investig. 2017, 14, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Young, K.S.; Brand, M. Merging Theoretical Models and Therapy Approaches in the Context of Internet Gaming Disorder: A Personal Perspective. Front. Psychol. 2017, 8, 1853. [Google Scholar] [CrossRef] [PubMed]
- Kuss, D.J.; Griffiths, M.D.; Pontes, H.M. Chaos and confusion in DSM-5 diagnosis of Internet Gaming Disorder: Issues, concerns, and recommendations for clarity in the field. J. Behav. Addict. 2016, 6, 103–109. [Google Scholar] [CrossRef]
- Wichstrom, L.; Stenseng, F.; Belsky, J.; von Soest, T.; Hygen, B.W. Symptoms of Internet Gaming Disorder in Youth: Predictors and Comorbidity. J. Abnorm. Child Psychol. 2019, 47, 71–83. [Google Scholar] [CrossRef]
- Petry, N.M.; O’Brien, C.P. Internet gaming disorder and the DSM-5. Addiction 2013, 108, 1186–1187. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Petry, N.M.; Rash, C.J.; Alessi, S.M. A randomized controlled trial of brief interventions for problem gambling in substance abuse treatment patients. J. Consult. Clin. Psychol. 2016, 84, 874–886. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B. Substance use and addictive disorders in DSM-5 and ICD 10 and the draft ICD 11. Curr. Opin. Psychiatry 2017, 30, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Kardefelt-Winther, D. A critical account of DSM-5 criteria for internet gaming disorder. Addict. Res. Theory 2015, 23, 93–98. [Google Scholar] [CrossRef]
- Kardefelt-Winther, D.; Heeren, A.; Schimmenti, A.; van Rooij, A.; Maurage, P.; Carras, M.; Edman, J.; Blaszczynski, A.; Khazaal, Y.; Billieux, J. How can we conceptualize behavioural addiction without pathologizing common behaviours? Addiction 2017, 112, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Rumpf, H.J.; Achab, S.; Billieux, J.; Bowden-Jones, H.; Carragher, N.; Demetrovics, Z.; Higuchi, S.; King, D.L.; Mann, K.; Potenza, M.; et al. Including gaming disorder in the ICD-11: The need to do so from a clinical and public health perspective. J. Behav. Addict. 2018, 7, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Billieux, J.; Schimmenti, A.; Khazaal, Y.; Maurage, P.; Heeren, A. Are we overpathologizing everyday life? A tenable blueprint for behavioral addiction research. J. Behav. Addict. 2015, 4, 119–123. [Google Scholar] [CrossRef]
- Starcevic, V. Tolerance and withdrawal symptoms may not be helpful to enhance understanding of behavioural addictions. Addiction 2016, 111, 1307–1308. [Google Scholar] [CrossRef]
- Starcevic, V.; Aboujaoude, E. Internet addiction: Reappraisal of an increasingly inadequate concept. CNS Spectr. 2017, 22, 7–13. [Google Scholar] [CrossRef]
- Khazaal, Y.; Breivik, K.; Billieux, J.; Zullino, D.; Thorens, G.; Achab, S.; Gmel, G.; Chatton, A. Game Addiction Scale Assessment Through a Nationally Representative Sample of Young Adult Men: Item Response Theory Graded-Response Modeling. J. Med. Internet Res. 2018, 20, e10058. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H. Defining tolerance in Internet Gaming disorder: Isn’t it time? Addiction 2016, 111, 2064–2065. [Google Scholar] [CrossRef]
- Lemmens, J.S.; Valkenburg, P.M.; Gentile, D.A. The Internet Gaming Disorder Scale. Psychol. Assess. 2015, 27, 567–582. [Google Scholar] [CrossRef]
- Aarseth, E.; Bean, A.M.; Boonen, H.; Colder Carras, M.; Coulson, M.; Das, D.; Deleuze, J.; Dunkels, E.; Edman, J.; Ferguson, C.J.; et al. Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. J. Behav. Addict. 2017, 6, 267–270. [Google Scholar] [CrossRef] [PubMed]
- King, D.L.; Chamberlain, S.R.; Carragher, N.; Billieux, J.; Stein, D.; Mueller, K.; Potenza, M.N.; Rumpf, H.J.; Saunders, J.; Starcevic, V.; et al. Screening and assessment tools for gaming disorder: A comprehensive systematic review. Clin. Psychol. Rev. 2020, 77, 101831. [Google Scholar] [CrossRef] [PubMed]
- van Rooij, A.J.; Schoenmakers, T.M.; van de Mheen, D. Clinical validation of the C-VAT 2.0 assessment tool for gaming disorder: A sensitivity analysis of the proposed DSM-5 criteria and the clinical characteristics of young patients with ‘video game addiction’. Addict. Behav. 2017, 64, 269–274. [Google Scholar] [CrossRef]
- Khazaal, Y.; Achab, S.; Billieux, J.; Thorens, G.; Zullino, D.; Dufour, M.; Rothen, S. Factor Structure of the Internet Addiction Test in Online Gamers and Poker Players. JMIR Mental Health 2015, 2, e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meerkerk, G.J.; Van Den Eijnden, R.J.; Vermulst, A.A.; Garretsen, H.F. The Compulsive Internet Use Scale (CIUS): Some psychometric properties. Cyberpsychol. Behav. 2009, 12, 1–6. [Google Scholar] [CrossRef]
- Downing, M.J., Jr.; Antebi, N.; Schrimshaw, E.W. Compulsive use of Internet-based sexually explicit media: Adaptation and validation of the Compulsive Internet Use Scale (CIUS). Addict. Behav. 2014, 39, 1126–1130. [Google Scholar] [CrossRef]
- Review, W.P. Arabic Speaking Countries 2020. Available online: https://worldpopulationreview.com/country-rankings/arab-countries (accessed on 1 September 2022).
- Stats, I.W. Arabic Speaking Internet Users Statistics. Available online: https://www.internetworldstats.com/stats19.htm (accessed on 1 September 2022).
- Khazaal, Y.; Chatton, A.; Atwi, K.; Zullino, D.; Khan, R.; Billieux, J. Arabic validation of the Compulsive Internet Use Scale (CIUS). Subst. Abus. Treat. Prev. Policy 2011, 6, 32. [Google Scholar] [CrossRef]
- Hawi, N.S. Arabic validation of the Internet addiction test. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 200–204. [Google Scholar] [CrossRef]
- Vally, Z. Symptoms of Internet Gaming Disorder, Inattention, and Impulsivity: A Cross-Sectional Study Conducted in the United Arab Emirates. Psychiatr. Q. 2020, 92, 301–310. [Google Scholar] [CrossRef]
- Samaha, A.A.; Fawaz, M.; El Yahfoufi, N.; Gebbawi, M.; Abdallah, H.; Baydoun, S.A.; Ghaddar, A.; Eid, A.H. Assessing the Psychometric Properties of the Internet Addiction Test (IAT) Among Lebanese College Students. Front. Public Health 2018, 6, 365. [Google Scholar] [CrossRef]
- Narayanan, A. A review of eight software packages for structural equation modelling. Am. Stat. 2012, 66, 129–138. [Google Scholar] [CrossRef]
- El-Sheikh, A.; Abonazel, M.; Gamil, N. A review of software packages for structural equation modeling: A comparative study. Appl. Math. Phys. 2017, 5, 85–94. [Google Scholar]
- Yilmaz, F. Comparison of different estimation methods used in confirmatory factor analyses in non-normal data: A Monte Carlo study. Int. Online J. Educ. Sci. 2019, 11, 131–140. [Google Scholar] [CrossRef]
- Bean, G.J.; Bowen, N.K. Item response theory and confirmatory factor analysis: Complementary approaches for scale development. J. Evid. Based Soc. Work. 2021, 18, 597–618. [Google Scholar]
- Rizopoulos, D. An R package for latent variable modelling and item response theory analyses. J. Stat. Softw. 2006, 17, 1–25. [Google Scholar] [CrossRef]
- De Ayala, R.J. The Theory and Practice of Item Response Theory; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Samejima, F. Estimation of latent ability using a response pattern of graded scores. Psychometrika 1969, 34, 100. [Google Scholar] [CrossRef]
- Baker, B. The Basics of Item Response Theory; Boston, C., Rudner, L., Eds.; Office of Educational Research and Improvement: Washington, DC, USA, 2001. [Google Scholar]
- Rodriguez, A.; Reise, S.P.; Haviland, M.G. Evaluating bifactor models: Calculating and interpreting statistical indices. Psychol. Methods 2016, 21, 137–150. [Google Scholar] [CrossRef]
- DeMars, C. Item Response Theory; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Raju, N.S.; Laffitte, L.J.; Byrne, B.M. Measurement equivalence: A comparison of methods based on confirmatory factor analysis and item response theory. J. Appl. Psychol. 2002, 87, 517–529. [Google Scholar] [CrossRef]
- Hays, R.D.; Morales, L.S.; Reise, S.P. Item response theory and health outcomes measurement in the 21st century. Med. Care 2000, 38, II28–II42. [Google Scholar] [CrossRef]
- Bteich, G.; Berbiche, D.; Khazaal, Y. Validation of the short Arabic UPPS-P Impulsive Behavior Scale. BMC Psychiatry 2017, 17, 244. [Google Scholar] [CrossRef]
- An, X.; Yung, Y. Item Response Theory: What It Is and How You Can Use the IRT Procedure to Apply It; Paper SAS364-2014; SAS Institute: Cary, NC, USA, 2014. [Google Scholar]
- Lipscomb, J.; Gotay, C.; Snyder, C. Outcomes Assessment in Cancer: Measures, Methods and Applications; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Mielenz, T.J.; Callahan, L.F.; Edwards, M.C. Item response theory analysis of Centers for Disease Control and Prevention Health-Related Quality of Life (CDC HRQOL) items in adults with arthritis. Health Qual. Life Outcomes 2016, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Prisciandaro, J.J.; Tolliver, B.K. An item response theory evaluation of the young mania rating scale and the montgomery-asberg depression rating scale in the systematic treatment enhancement program for bipolar disorder (STEP-BD). J. Affect. Disord. 2016, 205, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T. Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modeling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Stochl, J.; Jones, P.B.; Croudace, T.J. Mokken scale analysis of mental health and well-being questionnaire item responses: A non-parametric IRT method in empirical research for applied health researchers. BMC Med. Res. Methodol. 2012, 12, 74. [Google Scholar] [CrossRef] [PubMed]
- McDonald, R.P. The dimensionality of tests and items. Br. J. Math. Stat. Psychol. 1981, 34, 100–117. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Kline, R. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA; London, UK, 2011. [Google Scholar]
- Reeve, B.B.; Hays, R.D.; Bjorner, J.B.; Cook, K.F.; Crane, P.K.; Teresi, J.A.; Thissen, D.; Revicki, D.A.; Weiss, D.J.; Hambleton, R.K.; et al. Psychometric evaluation and calibration of health-related quality of life item banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care 2007, 45, S22–S31. [Google Scholar] [CrossRef]
- Van der Ark, L.A. Mokken scale analysis in R. J. Stat. Softw. 2007, 20, 1–19. [Google Scholar] [CrossRef]
- Choi, S.W.; Gibbons, L.E.; Crane, P.K. Lordif: An R Package for Detecting Differential Item Functioning Using Iterative Hybrid Ordinal Logistic Regression/Item Response Theory and Monte Carlo Simulations. J. Stat. Softw. 2011, 39, 1–30. [Google Scholar] [CrossRef]
- Jiang, S.; Wang, C.; Weiss, D.J. Sample Size Requirements for Estimation of Item Parameters in the Multidimensional Graded Response Model. Front. Psychol. 2016, 7, 109. [Google Scholar] [CrossRef] [PubMed]
- Reeve, B.R.; Fayers, P. Applying item response theory modelling for evaluating questionnaire item and scale properties In Assessing Quality of Life in Clinical Trials: Methods and Practice, 2nd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Dhir, A.; Chen, S.; Nieminen, M. Psychometric Validation of the Chinese Compulsive Internet Use Scale (CIUS) with Taiwanese High School Adolescents. Psychiatr. Q. 2015, 86, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Yong, R.K.F.; Inoue, A.; Kawakami, N. The validity and psychometric properties of the Japanese version of the Compulsive Internet Use Scale (CIUS). BMC Psychiatry 2017, 17, 201. [Google Scholar] [CrossRef] [PubMed]
- Alavi, S.; Jannatifard, F.; Eslami, M.; Rezapour, H. Validity, reliability and factor analysis of compulsive internet use scale in students of Isfahan’s universities. Health Inf. Manag. 2011, 7, 715–724. [Google Scholar]
- Gmel, G.; Khazaal, Y.; Studer, J.; Baggio, S.; Marmet, S. Development of a short form of the compulsive internet use scale in Switzerland. Int. J. Methods Psychiatr. Res. 2019, 28, e1765. [Google Scholar] [CrossRef]
- Cartierre, N.; Coulon, N.; Demerval, R. Validation d’une version courte en langue française pour adolescents de la Compulsive Internet Use Scale. Neuropsychiatr. Enfance Adolesc. 2011, 59, 415–419. [Google Scholar] [CrossRef]
- Besser, B.; Rumpf, H.J.; Bischof, A.; Meerkerk, G.J.; Higuchi, S.; Bischof, G. Internet-Related Disorders: Development of the Short Compulsive Internet Use Scale. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Fernandez, O.; Griffiths, M.D.; Kuss, D.J.; Dawes, C.; Pontes, H.M.; Justice, L.; Rumpf, H.J.; Bischof, A.; Gassler, A.K.; Suryani, E.; et al. Cross-Cultural Validation of the Compulsive Internet Use Scale in Four Forms and Eight Languages. Cyberpsychology Behav. Soc. Netw. 2019, 22, 451–464. [Google Scholar] [CrossRef]
- Rehbein, F.; Kliem, S.; Baier, D.; Mossle, T.; Petry, N.M. Prevalence of Internet gaming disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction 2015, 110, 842–851. [Google Scholar] [CrossRef]
- Kiraly, O.; Sleczka, P.; Pontes, H.M.; Urban, R.; Griffiths, M.D.; Demetrovics, Z. Validation of the Ten-Item Internet Gaming Disorder Test (IGDT-10) and evaluation of the nine DSM-5 Internet Gaming Disorder criteria. Addict. Behav. 2017, 64, 253–260. [Google Scholar] [CrossRef]
- Deleuze, J.; Nuyens, F.; Rochat, L.; Rothen, S.; Maurage, P.; Billieux, J. Established risk factors for addiction fail to discriminate between healthy gamers and gamers endorsing DSM-5 Internet gaming disorder. J. Behav. Addict. 2017, 1–9. [Google Scholar] [CrossRef]
- Pontes, H.M.; Kiraly, O.; Demetrovics, Z.; Griffiths, M.D. The conceptualisation and measurement of DSM-5 Internet Gaming Disorder: The development of the IGD-20 Test. PLoS ONE 2014, 9, e110137. [Google Scholar] [CrossRef]
- Ko, C.H.; Yen, J.Y.; Chen, S.H.; Wang, P.W.; Chen, C.S.; Yen, C.F. Evaluation of the diagnostic criteria of Internet gaming disorder in the DSM-5 among young adults in Taiwan. J. Psychiatr. Res. 2014, 53, 103–110. [Google Scholar] [CrossRef]
- Mak, K.K.; Young, K.S. Development and Differential Item Functioning of the Internet Addiction Test-Revised (IAT-R): An Item Response Theory Approach. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 312–328. [Google Scholar] [CrossRef]
- Kaptsis, D.; King, D.L.; Delfabbro, P.H.; Gradisar, M. Withdrawal symptoms in internet gaming disorder: A systematic review. Clin. Psychol. Rev. 2016, 43, 58–66. [Google Scholar] [CrossRef]
- Baggio, S.; Starcevic, V.; Studer, J.; Simon, O.; Gainsbury, S.M.; Gmel, G.; Billieux, J. Technology-mediated addictive behaviors constitute a spectrum of related yet distinct conditions: A network perspective. Psychol. Addict. Behav. 2018, 32, 564–572. [Google Scholar] [CrossRef]
- Khazaal, Y.; van Singer, M.; Chatton, A.; Achab, S.; Zullino, D.; Rothen, S.; Khan, R.; Billieux, J.; Thorens, G. Does self-selection affect samples’ representativeness in online surveys? An investigation in online video game research. J. Med. Internet Res. 2014, 16, e164. [Google Scholar] [CrossRef]
- Brand, M.; Young, K.S.; Laier, C.; Wolfling, K.; Potenza, M.N. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neurosci. Biobehav. Rev. 2016, 71, 252–266. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Algeria n = 592 | Lebanon, Sample 1 n = 155 | Lebanon, Sample 2 n = 568 | Total n = 1315 | |
|---|---|---|---|---|
| Age | ||||
| up to 30 | 99.9 | 100 | 72.7 | 88.1 |
| 31–40 | 0 | 0 | 17.1 | 7.4 |
| over 40 | 0 | 0 | 4.0 | 1.7 |
| missing | 2.0 | 0 | 6.2 | 2.7 |
| Gender, female | 55.1 | 50.0 | 73.6 | 62.4 |
| CIUS total score | 33.6 (12.9) | 35.9 (8.6) | 35.1 (9.0) | 34.5 (10.9) |
| Algeria (592) | Lebanon, Sample 1 (155) | Lebanon, Sample 2 (568) | All (1315) | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CIUS | Item Label | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | p * | |
| Scoring | |||||||||||||||||||||||
| 1 | Do you find it difficult to stop using the Internet when you are online? | 25.5 | 22.1 | 20.3 | 17.4 | 14.7 | 18.7 | 20.6 | 34.8 | 20.0 | 5.8 | 14.3 | 23.6 | 38.7 | 7.9 | 15.5 | 19.8 | 22.6 | 30.0 | 13.6 | 14.0 | <0.005 | |
| 2 | Do you continue to use the Internet despite your intention to stop? | 34.3 | 18.2 | 14.9 | 23.1 | 9.5 | 13.5 | 31.6 | 32.9 | 13.5 | 8.4 | 10.9 | 19.9 | 43.3 | 15.1 | 10.7 | 21.7 | 20.5 | 29.3 | 18.6 | 9.9 | <0.005 | |
| 3 | Do others (e.g., partner, children, parents) say you should use the Internet less? | 39.4 | 19.8 | 12.3 | 15.5 | 13.0 | 29.0 | 20.0 | 21.3 | 18.7 | 11.0 | 25.2 | 27.6 | 25.2 | 8.5 | 13.6 | 32.0 | 23.2 | 18.9 | 12.9 | 13.0 | <0.005 | |
| 4 | Do you prefer to use the Internet instead of spending time with others (e.g., partner, children, parents)? | 36.8 | 18.8 | 17.9 | 14.0 | 12.5 | 11.6 | 23.9 | 31.0 | 23.2 | 10.3 | 19.5 | 28l7 | 36.6 | 8.1 | 7.0 | 26.4 | 23.7 | 27.5 | 12.5 | 9.9 | <0.005 | |
| 5 | Are you short of sleep because of the Internet? | 37.0 | 18.1 | 12.3 | 17.6 | 15.0 | 52.9 | 20.6 | 11.0 | 11,6 | 3.9 | 41.5 | 29.2 | 17.3 | 4.9 | 7.0 | 40.8 | 23.2 | 14.3 | 11.4 | 10.3 | <0.005 | |
| 6 | Do you think about the Internet, even when not online? | 56.1 | 17.2 | 12.8 | 8.4 | 5.4 | 23.2 | 35.5 | 26.5 | 11.6 | 3.2 | 35.2 | 35.2 | 20.2 | 4.6 | 4.8 | 43.2 | 27.1 | 17.6 | 7.1 | 4.9 | <0.005 | |
| 7 | Do you look forward to your next Internet session? | 41.7 | 29.4 | 15.2 | 10.5 | 3.2 | 12.3 | 27.1 | 36.1 | 20.0 | 4.5 | 21.1 | 31.0 | 30.6 | 10.2 | 7.0 | 29.4 | 29.8 | 24.3 | 11.5 | 5.0 | <0.005 | |
| 8 | Do you think you should use the Internet less often? | 32.3 | 25.5 | 18.2 | 14.4 | 9.5 | 34.2 | 29.7 | 21.3 | 8.4 | 6.5 | 21.5 | 28.5 | 30.1 | 10.7 | 9.2 | 27.8 | 27.3 | 23.7 | 12. | 9.0 | <0.005 | |
| 9 | Have you unsuccessfully tried to spend less time on the Internet? | 49.8 | 19.1 | 13.0 | 11.5 | 6.6 | 12.3 | 15.5 | 21.3 | 25.8 | 25.2 | 11.4 | 18.7 | 29.4 | 17.4 | 23.1 | 28.8 | 18.5 | 21.1 | 15.7 | 15.9 | <0.005 | |
| 10 | Do you rush through your (home) work in order to go on the Internet? | 46.1 | 17.7 | 13.5 | 14.9 | 7.8 | 29.7 | 26.5 | 20.6 | 17.4 | 5.8 | 32.7 | 30.1 | 24.1 | 7.6 | 5.5 | 38.4 | 21.1 | 18.9 | 12.0 | 6.5 | <0.005 | |
| 11 | Do you neglect your daily obligations (work, school, or family life) because you prefer to go on the Internet? | 52.4 | 17.2 | 12.2 | 12.0 | 6.3 | 49.0 | 20.0 | 14.2 | 8.4 | 8.4 | 40.5 | 25.5 | 21.5 | 6.3 | 6.2 | 46.8 | 21.1 | 16.4 | 9.1 | 6.5 | <0.005 | |
| 12 | Do you go on the Internet when you are feeling down? | 16.4 | 16.9 | 17.1 | 25.2 | 24.5 | 16.8 | 21.3 | 31.6 | 21.9 | 8.4 | 23.9 | 21.3 | 29.9 | 14.1 | 10.7 | 19.7 | 19.3 | 24.3 | 20.0 | 16.7 | <0.005 | |
| 13 | Do you use the Internet to escape from your sorrows or get relief from negative feelings? | 31.6 | 17.2 | 16.0 | 16.6 | 18.6 | 21.9 | 20.6 | 29.7 | 19.4 | 8.4 | 24.6 | 23.1 | 27.3 | 13.7 | 11.3 | 27.5 | 20.2 | 22.5 | 15.7 | 14.2 | <0.005 | |
| 14 | Do you feel restless, frustrated, or irritated when you cannot use the Internet? | 45.9 | 22.5 | 9.8 | 12.5 | 9.3 | 40.0 | 22.6 | 23.9 | 8.4 | 5.2 | 42.8 | 28.2 | 18.5 | 6.2 | 4.4 | 43.9 | 24.9 | 15.2 | 9.3 | 6.7 | <0.005 | |
| Discrimination | Threshold | ||||
|---|---|---|---|---|---|
| Item | αi | β1 | β2 | β3 | β4 |
| 1 | 1.39 | −1.33 | −0.28 | 0.96 | 1.74 |
| 2 | 1.31 | −1.27 | −0.29 | 0.93 | 2.14 |
| 3 | 1.16 | −0.80 | 0.25 | 1.16 | 2.03 |
| 4 | 1.21 | −1.06 | 0.03 | 1.32 | 2.27 |
| 5 | 1.64 | −0.32 | 0.53 | 1.15 | 1.87 |
| 6 | 2.16 | −0.21 | 0.67 | 1.49 | 2.16 |
| 7 | 1.74 | −0.74 | 0.33 | 1.36 | 2.35 |
| 8 | 0.64 | −1.60 | 0.39 | 2.24 | 3.86 |
| 9 | 0.66 | −1.42 | −0.05 | 1.38 | 2.80 |
| 10 | 2.14 | −0.35 | 0.44 | 1.16 | 1.96 |
| 11 | 1.85 | −0.09 | 0.64 | 1.38 | 2.09 |
| 12 | 1.21 | −1.44 | −0.44 | 0.60 | 1.68 |
| 13 | 1.45 | −0.90 | −0.07 | 0.82 | 1.66 |
| 14 | 2.20 | −0.17 | 0.62 | 1.26 | 1.93 |
| CIUS | Item Label | CIUS-9 [97] | CIUS-8 [96] | CIUS-5 [98] | CIUS-Arab Items with High or Very High Discriminative Power |
|---|---|---|---|---|---|
| 1 | Do you find it difficult to stop using the Internet when you are online? | X | X | X | X |
| 2 | Do you continue to use the Internet despite your intention to stop? | ||||
| 3 | Do others (e.g., partner, children, parents) say you should use the Internet less? | X | X | ||
| 4 | Do you prefer to use the Internet instead of spending time with others (e.g., partner, children, parents)? | X | X | ||
| 5 | Are you short of sleep because of the Internet? | X | X | X | X |
| 6 | Do you think about the Internet, even when not online? | X | |||
| 7 | Do you look forward to your next Internet session? | X | X | X | |
| 8 | Do you think you should use the Internet less often? | ||||
| 9 | Have you unsuccessfully tried to spend less time on the Internet? | X | X | ||
| 10 | Do you rush through your (home) work in order to go on the Internet? | X | |||
| 11 | Do you neglect your daily obligations (work, school, or family life) because you prefer to go on the Internet? | X | X | X | X |
| 12 | Do you go on the Internet when you are feeling down? | X | X | X | |
| 13 | Do you use the Internet to escape from your sorrows or get relief from negative feelings? | X | |||
| 14 | Do you feel restless, frustrated, or irritated when you cannot use the Internet? | X | X | X |
| CIUS | Item Label | Item Classification by CIUS’ Authors | DSM-5 Concordance * | ICD-11 Concordance * |
|---|---|---|---|---|
| 1 | Do you find it difficult to stop using the Internet when you are online? | Loss of Control | Unsuccessful attempt to stop/limit | Impaired control |
| 2 | Do you continue to use the Internet despite your intention to stop? | Loss of Control | Unsuccessful attempt to stop/limit | Impaired control |
| 3 | Do others (e.g., partner, children, parents) say you should use the Internet less? | Conflict/Negative consequences | Deception | Increasing priority |
| 4 | Do you prefer to use the Internet instead of spending time with others (e.g., partner, children, parents)? | Preoccupation regarding Internet use | Loss of interest | Increasing priority |
| 5 | Are you short of sleep because of the Internet? | Loss of control | Unsuccessful attempt to stop/limit | Impaired control |
| 6 | Do you think about the Internet, even when not online? | Preoccupation regarding Internet use | Preoccupation | Increasing priority |
| 7 | Do you look forward to your next Internet session? | Preoccupation regarding Internet use | Preoccupation | Increasing priority |
| 8 | Do you think you should use the Internet less often? | Conflict/Problems | Unsuccessful attempt to stop/limit | Impaired control |
| 9 | Have you unsuccessfully tried to spend less time on the Internet? | Loss of control | Unsuccessful attempt to stop/limit | Impaired control |
| 10 | Do you rush through your (home) work in order to go on the Internet? | Conflict/Problems | Loss of interest | Increasing priority |
| 11 | Do you neglect your daily obligations (work, school, or family life) because you prefer to go on the Internet? | Conflict/Problems | Harm/Continue use despite problems | Continued use despite harm and functional impairment |
| 12 | Do you go on the Internet when you are feeling down? | Coping/escape | Escape | - |
| 13 | Do you use the Internet to escape from your sorrows or get relief from negative feelings? | Coping/escape | Escape | - |
| 14 | Do you feel restless, frustrated, or irritated when you cannot use the Internet? | Withdrawal | Withdrawal | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khazaal, Y.; El Abiddine, F.Z.; Penzenstadler, L.; Berbiche, D.; Bteich, G.; Valizadeh-Haghi, S.; Rochat, L.; Achab, S.; Khan, R.; Chatton, A. Evaluation of the Psychometric Properties of the Arab Compulsive Internet Use Scale (CIUS) by Item Response Theory Modeling (IRT). Int. J. Environ. Res. Public Health 2022, 19, 12099. https://doi.org/10.3390/ijerph191912099
Khazaal Y, El Abiddine FZ, Penzenstadler L, Berbiche D, Bteich G, Valizadeh-Haghi S, Rochat L, Achab S, Khan R, Chatton A. Evaluation of the Psychometric Properties of the Arab Compulsive Internet Use Scale (CIUS) by Item Response Theory Modeling (IRT). International Journal of Environmental Research and Public Health. 2022; 19(19):12099. https://doi.org/10.3390/ijerph191912099
Chicago/Turabian StyleKhazaal, Yasser, Fares Zine El Abiddine, Louise Penzenstadler, Djamal Berbiche, Ghada Bteich, Saeideh Valizadeh-Haghi, Lucien Rochat, Sophia Achab, Riaz Khan, and Anne Chatton. 2022. "Evaluation of the Psychometric Properties of the Arab Compulsive Internet Use Scale (CIUS) by Item Response Theory Modeling (IRT)" International Journal of Environmental Research and Public Health 19, no. 19: 12099. https://doi.org/10.3390/ijerph191912099