

The Development and Acceptability of a Wilderness Programme to Support the Health and Well-Being of Adolescent and Young Adult Cancer Survivors: The WAYA Programme



Abstract
1. Introduction
“The smaller we come to feel ourselves compared to the mountain, the nearer we come to participating in its greatness”.Arne Næss
- To systematically develop a Wilderness programme for AYA cancer survivors (WAYA programme) in the Scandinavian countries, including theory, concept, and content building.
- To investigate the acceptability of the wilderness programme among facilitators and AYA cancer survivors.
2. Material and Methods
2.1. Study Subjects
2.1.1. Facilitators
2.1.2. Participants
2.2. Programme Development
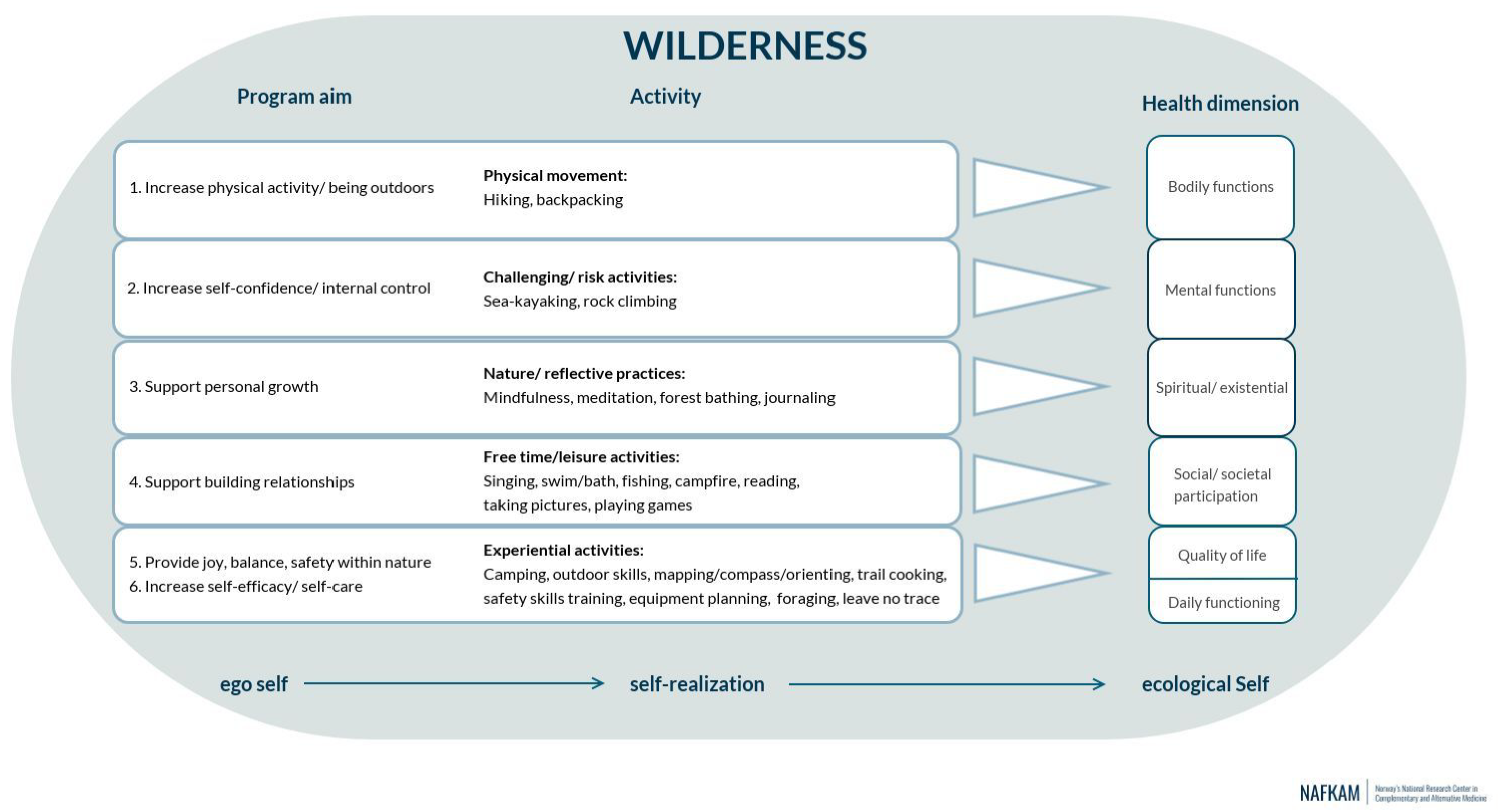
2.2.1. Theoretical Foundation, Concept Building and Aims of the Programme
- To increase physical activity in the context of the natural environment
- To increase self-confidence and provide an increased perception of internal control
- To support personal growth
- To foster togetherness, a sense of community, and support the building of meaningful relationships
- To provide joy, balance, and safety within the grandness of nature
- To increase self-efficacy and self-care in the context of personal health and well-being.
2.2.2. Content Building
2.2.3. The Role of Nature in the WAYA Programme
2.2.4. Structure of the Programme
2.2.5. Setting
2.3. Risk and Safety Plan
2.4. Programme Evaluation
2.4.1. By Facilitators
2.4.2. By Participants
2.5. Ethical Considerations
3. Results
3.1. Type of Wilderness Programme
“…first and foremost, it was that we were a group hiking together, it’s a lot easier when you are a team… one day we hiked about ten kilometres or similar, it was far and took a whole day but since we were a team supporting and encouraging each other and having fun, we could really have hiked 40 kilometres.”(Participant 10)
“I understand that I am not on a spiritual camp, but on a camp to hike along with other people touched by cancer. So in case I would want more relaxation, it would have been more appropriate with a retreat for ten days or so…”(Participant 18)
“I believe that one of the advantages to the expedition is kind of getting through the challenges of it together, so that participants have an opportunity to help one another and, build their relationships…. therefore, when they get to base-camp follow up, they can….—I love the idea that there was both actually -…. kind of solidify the relationships started with the expedition …. and have the space to talk and hang out.”(Facilitator 8)
3.2. Activities in the Programme
“Since I don’t have any distance vision it affects me in a way that I need a guide, and I need to fully concentrate. On our first hike we hiked on a narrow inclining path with lots of tree roots and stones, then I needed double concentration which was exhausting. At the same time, the rest of the group moved ahead, and I was left behind with the guide which was a bit sad, since I felt outside the group… and the second hike was too long, it was ten kilometres, so I could not make it, it would take too long.”(Participant 11)
“I also think that it is one of the beauties that people have so different needs and learn from each other and learn to take care of each other, so I think it was a good mix, because if you only had chosen the most fit participants, we would have lost a good teaching opportunity for the whole group.”(Facilitator 4)
“but if you have an expedition, and you have a goal to reach the top of, whatever you want to reach, in my experience there’s not much free time. Free time is when you are there, and if you are there earlier, well you have more free time, and then your free time is cooking and chatting, and maybe checking your environment and then going to bed.”(Facilitator 1)
“she came up to me and said: “I just want to take a stroll, going towards the waterfall”, and I was thinking…. what I have always been taught… like OK, is that safe? Is it safe for her to wander off? I do not know her.”(Facilitator 10)
“there was a time when I went off for meditation on my own, I let them know before I left as I knew I should do so …., but then I stayed a bit longer than I had said and one of the facilitators checked on me to see whether I was ok… I understand it was out of concern for me, and I know that I am in general terrible at keeping time, and then especially while being in nature without a clock!”(Participant 16)
“(camping) went really well but was something out of the ordinary. Still you learned what was a good place to be and what was a less good place to be. I mean in what way the ground was. A couple of times I started out high up in tent when going to sleep and woke up in the foot end. During the night I slid down (smiling).”(Participant 5)
“We became a group very fast. People opened up and talked about, well it was also very emotional, and at the same time when you come there and meet people who have been ill and talk about their illness there are lots of emotions, and you are allowed to just be yourself instead of trying to be someone else. That was nice… and emotional.”(Participant 10)
“it was hard for me to sit in the ring and share after the mindfulness exercises, even though what is shared is true, it is hard. People got deeper and deeper and were more and more affected. Finally, I said that if this is how it is going to be, I am not going to join in on the sharing unless it becomes sharing of something that is more positive.”(Participant 12)
3.3. Safety of the Programme
“I think, having facilitators with medical backgrounds or nurses is wonderful, and that you cannot be in the back wilderness, and be in the ocean, and be on the mountain and not have some challenges, that’s part of the… risk that they all agree to take on. So I felt, even though I tried to always write down the near misses, I felt it to be very safe.”(Facilitator 8)
“I had never kayaked before, and it was really frightening in the beginning. I also capsized (unintentionally) and that was scary, but directly as soon as I came up from under the water, they (facilitator 3 and 7) were there. You feel safe when someone is there to support you.”(Participant 10)
3.4. Facilitators in the Programme
3.5. Equipment in the Programme
“there was just some really cold night, so sleeping… and I do not know if they were, but I did trade sleeping bags with several people, and they were mentioning that they were warmer, so… I think that would be the only thing, I think everyone was getting a little wet and stuff.”(Facilitator 8)
“I learned, because I did not know that the cold comes from the ground, so I had some extra insulation under my sleeping mat, and additionally I learned that it is good to run a bit to get warm before you go to bed in the sleeping bag.”(Participant 16)
4. Discussion
5. Strenghts and Limitations
6. Recommendation for Practice and Further Research
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naess, A. Ecology, Community and Lifestyle; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Kesebir, S.; Kesebir, P. A Growing disconnection from nature is evident in cultural products. Perspect. Psychol. Sci. 2017, 12, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Kellert, S.; Case, D. The Nature of Americans. 2017. Available online: https://natureofamericans.org/sites/default/files/reports/Nature-of-Americans_National_Report_1.3_4-26-17.pdf (accessed on 15 August 2022).
- Maller, C.; Townsend, M.; Pryor, A.; Brown, P.; St Leger, L. Healthy nature healthy people: ‘Contact with nature’ as an upstream health promotion intervention for populations. Health Promot. Int. 2006, 21, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Coventry, P.A.; Brown, J.V.E.; Pervin, J.; Brabyn, S.; Pateman, R.; Breedvelt, J.; Gilbody, S.; Stancliffe, R.; McEachan, R.; White, P.C.L. Nature-based outdoor activities for mental and physical health: Systematic review and meta-analysis. SSM—Popul. Health 2021, 16, 100934. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, M.P.; DeVille, N.V.; Elliott, E.G.; Schiff, J.E.; Wilt, G.E.; Hart, J.E.; James, P. Associations between nature exposure and health: A review of the evidence. Int. J. Environ. Res. Public Health 2021, 18, 4790. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef]
- Kuo, M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 2015, 6, 1093. [Google Scholar] [CrossRef]
- de Vries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural environments—Healthy environments? An exploratory analysis of the relationship between greenspace and health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef]
- Sarkar, C.; Webster, C.; Gallacher, J. Residential greenness and prevalence of major depressive disorders: A cross-sectional, observational, associational study of 94 879 adult UK Biobank participants. Lancet Planet. Health 2018, 2, e162–e173. [Google Scholar] [CrossRef]
- Jenkins, M.; Lee, C.; Houge Mackenzie, S.; Hargreaves, E.A.; Hodge, K.; Calverley, J. Nature-based physical activity and hedonic and eudaimonic wellbeing: The mediating roles of motivational quality and nature relatedness. Front. Psychol. 2022, 13, 783840. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Khreis, H.; Triguero-Mas, M.; Gascon, M.; Dadvand, P. Fifty shades of green: Pathway to healthy urban living. Epidemiology 2017, 28, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Kühn, S.; Mascherek, A.; Filevich, E.; Lisofsky, N.; Becker, M.; Butler, O.; Lochstet, M.; Mårtensson, J.; Wenger, E.; Lindenberger, U.; et al. Spend time outdoors for your brain—An in-depth longitudinal MRI study. World J. Biol. Psychiatry 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sobko, T.; Liang, S.; Cheng, W.H.G.; Tun, H.M. Impact of outdoor nature-related activities on gut microbiota, fecal serotonin, and perceived stress in preschool children: The Play&Grow randomized controlled trial. Sci. Rep. 2020, 10, 21993. [Google Scholar]
- Tischer, C.; Kirjavainen, P.; Matterne, U.; Tempes, J.; Willeke, K.; Keil, T.; Apfelbacher, C.; Täubel, M. Interplay between natural environment, human microbiota and immune system: A scoping review of interventions and future perspectives towards allergy prevention. Sci. Total Environ. 2022, 821, 153422. [Google Scholar] [CrossRef]
- Blaschke, S. The role of nature in cancer patients’ lives: A systematic review and qualitative meta-synthesis. BMC Cancer 2017, 17, 370. [Google Scholar] [CrossRef]
- National Cancer Institute. Adolescents and Young Adults with Cancer. Available online: https://www.cancer.gov/types/aya (accessed on 14 December 2021).
- Mellblom, A.V.; Kiserud, C.E.; Rueegg, C.S.; Ruud, E.; Loge, J.H.; Fosså, S.D.; Lie, H.C. Self-reported late effects and long-term follow-up care among 1889 long-term Norwegian Childhood, Adolescent, and Young Adult Cancer Survivors (the NOR-CAYACS study). Support. Care Cancer 2021, 29, 2947–2957. [Google Scholar] [CrossRef]
- Janssen, S.H.M.; van der Graaf, W.T.A.; van der Meer, D.J.; Manten-Horst, E.; Husson, O. Adolescent and Young Adult (AYA) cancer survivorship practices: An overview. Cancers 2021, 13, 4847. [Google Scholar] [CrossRef]
- Chan, Y.T.; Lau, H.Y.; Chan, W.Y.; Cheung, C.W.; Lui, W.; Chane-Thu, Y.S.J.; Dai, W.L.; To, K.C.; Cheng, H.L. Adventure therapy for child, adolescent, and young adult cancer patients: A systematic review. Support. Care Cancer 2021, 29, 35–48. [Google Scholar] [CrossRef]
- Neville, A.R.; Moothathamby, N.; Naganathan, M.; Huynh, E.; Moola, F.J. “A place to call our own”: The impact of camp experiences on the psychosocial wellbeing of children and youth affected by cancer—A narrative review. Complement. Ther. Clin. Pract. 2019, 36, 18–28. [Google Scholar] [CrossRef]
- Jong, M.; Lown, E.A.; Schats, W.; Mills, M.L.; Otto, H.R.; Gabrielsen, L.E.; Jong, M.C. A scoping review to map the concept, content, and outcome of wilderness programs for childhood cancer survivors. PLoS ONE 2021, 16, e0243908. [Google Scholar] [CrossRef] [PubMed]
- Harper, N.J.; Fernee, C.R.; Gabrielsen, L.E. Nature’s Role in Outdoor Therapies: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 5117. [Google Scholar] [CrossRef] [PubMed]
- Naess, A. The shallow and the Deep Ecology movement. Anker, Peder. Deep Ecology in Bucharest. Trumpeter 2008, 24, 56–67. [Google Scholar]
- Naess, A. Self-realization: An ecological approach to being in the world. Trumpeter 1987, 4, 35–42. [Google Scholar]
- Ryff, C.D. Self realization and meaning making in the face of adversity: A eudaimonic approach to human resilience. J. Psychol. Afr. 2014, 24, 1–12. [Google Scholar] [CrossRef]
- Jong, M.C.; Mulder, E.; Kristoffersen, A.E.; Stub, T.; Dahlqvist, H.; Viitasara, E.; Lown, E.A.; Schats, W.; Jong, M. Protocol of a mixed-method randomised controlled pilot study evaluating a wilderness programme for adolescent and young adult cancer survivors: The WAYA study. BMJ Open 2022, 12, e061502. [Google Scholar] [CrossRef]
- Huber, M.; van Vliet, M.; Giezenberg, M.; Winkens, B.; Heerkens, Y.; Dagnelie, P.C.; Knottnerus, J.A. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 2016, 6, e010091. [Google Scholar] [CrossRef]
- van Wietmarschen, H.A.; Staps, S.; Meijer, J.; Flinterman, J.F.; Jong, M.C. The Use of the Bolk Model for Positive Health and Living Environment in the Development of an Integrated Health Promotion Approach: A Case Study in a Socioeconomically Deprived Neighborhood in The Netherlands. Int. J. Environ. Res. Public Health 2022, 19, 2478. [Google Scholar] [CrossRef]
- Huber, M.; Knottnerus, J.A.; Green, L.; Horst, H.v.d.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; Meer, J.W.; et al. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef]
- Haverkamp, B.; Bovenkerk, B.; Verweij, M.F. A practice-oriented review of health concepts. J. Med. Philos. 2018, 43, 381–401. [Google Scholar] [CrossRef]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Chiu, C.P.K.; Wang, R.; Oei, T.P.S.; Leung, F.Y.K. The effect of loving-kindness meditation on positive emotions: A meta-analytic review. Front. Psychol. 2015, 6, 1693. [Google Scholar] [CrossRef] [PubMed]
- Svenska Fjällklubben. Riskanalys med Riskmatris. Available online: https://fjallklubben.se/images/SFK/Sakerhetsplanen/SFK_Sakerhetsplan_1.3_Bilaga_2_Riskanalys.pdf (accessed on 29 April 2022).
- Bengtsson, M. How to plan and perform a qualitative study using content analysis. NursingPlus Open 2016, 2, 8–14. [Google Scholar] [CrossRef]
- Hilgendorf, I.; Bergelt, C.; Bokemeyer, C.; Kaatsch, P.; Seifart, U.; Stein, A.; Langer, T. Long-term follow-up of children, adolescents, and young adult cancer survivors. Oncol. Res. Treat. 2021, 44, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Chronic health conditions in adult survivors of childhood cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef]
- Bowen, D.J.; Neill, J.T. A meta-analysis of adventure therapy outcomes and moderators. Open Psychol. J. 2013, 6, 28–53. [Google Scholar] [CrossRef]
- Dobud, W.W.; Harper, N.J. Of Dodo birds and common factors: A scoping review of direct comparison trials in adventure therapy. Complement. Ther. Clin. Pract. 2018, 31, 16–24. [Google Scholar] [CrossRef]
- Stea, T.H.; Jong, M.C.; Fegran, L.; Sejersted, E.; Jong, M.; Wahlgren, S.L.H.; Fernee, C.R. Mapping the concept, content, and outcome of family-based outdoor therapy for children and adolescents with mental health problems: A scoping review. Int. J. Environ. Res. Public Health 2022, 19, 5825. [Google Scholar] [CrossRef]
- Paquette, L.; Fortin, J.; Crete, A.; Maltais, D.; Brassard, A. Effect of and outdoor developmental adventure program on the psychosocial adjustment of adolescents journeying with cancer. In Proceedings of the 2017 Symposium on Experiential Education Research—45th Annual International AEE Conference, Ontario, ON, Canada, 7 November 2017. [Google Scholar]
- Stevens, B.; Kagan, S.; Yamada, J.; Epstein, I.; Beamer, M.; Bilodeau, M.; Baruchel, S. Adventure therapy for adolescents with cancer. Pediatr. Blood Cancer 2004, 43, 278–284. [Google Scholar] [CrossRef]
- Wynn, B.; Frost, A.; Pawson, P. Adventure therapy proves successful for adolescent survivors of childhood cancers. Nurs. N. Z. 2012, 18, 28–30. [Google Scholar]
- Carlson, K.P.; Cook, M. Challenge by choice: Adventure-based counseling for seriously ill adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2007, 16, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Gill, E.; Goldenberg, M.; Starnes, H.; Phelan, S. Outdoor adventure therapy to increase physical activity in young adult cancer survivors. J. Psychosoc. Oncol. 2016, 34, 184–199. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J. A wilderness program for adolescents with cancer. J. Assoc. Pediatr. Oncol. Nurses 1989, 6, 24–25. [Google Scholar] [CrossRef] [PubMed]
- Slavin, M. Climbing Out: Exploring the Psychosocial Impacts of an Adventure Programme for Young Adult Survivors of Cancer; University of Glasgow: Glasgow, UK, 2015. [Google Scholar]
- Victorson, D.; Doninger, G.; Victorson, S.; Victorson, G.; Hall, L.; Maletich, C.; Corr, B.R.; Scortino, K.; Burns, Z.; Allen, L.; et al. Psychosocial and biological outcomes of immersive, mindfulness-based treks in nature for groups of young adults and caregivers affected by cancer: Results from a Single Arm Program Evaluation from 2016–2021. Int. J. Environ. Res. Public Health 2021, 18, 12622. [Google Scholar]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Ngamkham, S.; Holden, J.E.; Smith, E.L. A systematic review: Mindfulness intervention for cancer-related pain. Asia Pac. J. Oncol. Nurs. 2019, 6, 161–169. [Google Scholar] [CrossRef]
- Oberoi, S.; Yang, J.; Woodgate, R.L.; Niraula, S.; Banerji, S.; Israels, S.J.; Altman, G.; Beattie, S.; Rabbani, R.; Askin, N.; et al. Association of mindfulness-based interventions with anxiety severity in adults with cancer: A systematic review and meta-analysis. JAMA Netw. Open 2020, 3, e2012598. [Google Scholar] [CrossRef]
- Van der Gucht, K.; Takano, K.; Labarque, V.; Vandenabeele, K.; Nolf, N.; Kuylen, S.; Cosyns, V.; Van Broeck, N.; Kuppens, P.; Raes, F. A Mindfulness-based intervention for adolescents and young adults after cancer treatment: Effects on quality of life, emotional distress, and cognitive vulnerability. J. Adolesc. Young Adult Oncol. 2017, 6, 307–317. [Google Scholar] [CrossRef]
- Djernis, D.; Lerstrup, I.; Poulsen, D.; Stigsdotter, U.; Dahlgaard, J.; O’Toole, M. A systematic review and meta-analysis of nature-based mindfulness: Effects of moving mindfulness training into an outdoor natural setting. Int. J. Environ. Res. Public Health 2019, 16, 3202. [Google Scholar] [CrossRef]
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef]
- Novak, B.K.; Gebhardt, A.; Pallerla, H.; McDonald, S.B.; Haramati, A.; Cotton, S. Impact of a university-wide interdisciplinary mind-body skills program on student mental and emotional well-being. Glob. Adv. Health Med. 2020, 9, 2164956120973983. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Value |
|---|---|
| Age, mean ± SD | 46.3 ± 8.4 |
| Gender, n/% | |
| Male | 7/46.7 |
| Female | 8/53.3 |
| Nationality, n/% | |
| Sweden | 7/46.7 |
| Netherlands | 3/20.0 |
| USA | 3/20.0 |
| Finland | 1/6.7 |
| Norway | 1/6.7 |
| Competence/skills, n/% | |
| Outdoor/nature guide | 8/47.1 |
| Research data collection/physical measurements | 5/33.3 |
| Counselling/supervision (youth) groups | 5/33.3 |
| Survival training/instructor | 4/26.7 |
| Mindfulness-based practices | 3/20.0 |
| Kayak instructor | 2/13.3 |
| Nursing | 2/13.3 |
| Climbing instructor | 1/13.3 |
| Characteristics | Value |
|---|---|
| Age, mean ± SD | 29.1 ± 3.8 |
| Gender, n/% | |
| Male | 6/35.3 |
| Female | 11/64.7 |
| Ethnicity, n/% | |
| One or both parents from Sweden | 16/94.1 |
| Both parents from outside Sweden | 1/5.9 |
| Marital status, n/% | |
| Married-partner | 8/47.1 |
| Single | 9/52.9 |
| Family situation, n/% | |
| No children | 16/94.1 |
| Children | 1/5.9 |
| Education, n/% | |
| Comprehensive | 1/5.9 |
| High school | 5/29.4 |
| College/university | 9/52.9 |
| Other | 2/11.8 |
| Employment status, n/% | |
| Full time work | 7/41.2 |
| Part time work | 4/23.5 |
| Full time education | 2/11.8 |
| Unable to work | 4/23.5 |
| Economic situation, n/% | |
| (how often do you have good finances to be able to do the same things as your friends) | |
| Always | 7/41.2 |
| Often | 8/47.1 |
| Sometimes | 1/5.9 |
| Seldom | 1/5.9 |
| Primary cancer type, n/% | |
| Haematological | 6/35.3 |
| Brain | 5/29.4 |
| Testicular | 2/11.8 |
| Thyroid | 2/11.8 |
| Osteosarcoma | 1/5.9 |
| Breast | 1/5.9 |
| Age at cancer diagnosis, mean ± SD (min-max) | 18.9 ± 8.5 (1.5–29) |
| Time since last treatment, n/% | |
| <3 months | 4/23.5 |
| 4–11 months | 1/5.9 |
| 1–5 years | 4/23.5 |
| >5 years | 7/41.2 |
| On active treatment | 1/5.9 |
| Health Issue | n/% |
|---|---|
| Pain (all pain) | 12/70.6 |
| Mental health problems (all combined) | 10/58.8 |
| Allergies/asthma | 6/35.3 |
| Cognitive dysfunction | 6/35.3 |
| Depression | 5/29.4 |
| Gastro-intestinal problems | 4/23.5 |
| Anxiety | 4/23.5 |
| Visual impairment | 2/11.8 |
| Hearing compromised | 2/11.8 |
| Sleeping problems | 2/11.8 |
| Balance problems | 2/11.8 |
| Hormonal dysfunction | 2/11.8 |
| Tiredness (general) | 1/5.9 |
| Concentration problems | 1/5.9 |
| Memory problems | 1/5.9 |
| Skin sensitivity | 1/5.9 |
| Restricted joint movement | 1/5.9 |
| Paresis (partial) | 1/5.9 |
| Gout | 1/5.9 |
| Osteoporosis | 1/5.9 |
| Anaemia | 1/5.9 |
| Characteristics | Programme Model | ||
|---|---|---|---|
| Expedition | Online Coaching | Base-Camp | |
| Duration (days) | 8 | 90 | 4 |
| Group size | 10 | NA ** | 10 |
| Group structure | closed | NA | closed |
| Amount of time in group activities * (h) | 4–8 | NA | 4–6 |
| Amount of time in structured activities * (h) | 6–8 | NA | 4–6 |
| Amount of free time * (h) | 3 | NA | 6 |
| Facilitator-participant ratio | 1:2 | 1:1 | 1:3 |
| Programme Activity | Disability of Participant (n) | Adaptation/Alternative |
|---|---|---|
| Hiking trails | Peripheral neuropathy (n = 1) | Kayaking, shorter hiking trails, extra breaks, warm water bottles for pain relief |
| Restricted joint movement (n = 1) | Shorter hiking trails, hiking with Nordic hiking poles, extra breaks, canoeing | |
| Visual impairments (n = 2) | Assistance by facilitators, boat transport, canoeing, swimming to shore with guidance of facilitator | |
| Obsessive-compulsive disorder symptoms (n = 1) | Guidance by facilitator to assure that nothing is left behind on the trail | |
| Cognitive dysfunction (n = 1) | Shorter hiking trails, canoeing | |
| Paresis (n = 1) Balance problems (n = 2) | Hiking with Nordic hiking poles | |
| Backpacking | Peripheral neuropathy (n = 1) Restricted joint movement (n = 1) Visual impairments (n = 2) | Backpack carried by facilitators |
| Balance problems (n = 4) Pain (n = 4) Skin sensitivity (n = 1) | Bigger items such as tent carried by facilitators | |
| Setting up/breaking down camp | Visual impairments (n = 1) | Long rope from the tent to trees in forest for guidance relating to going to the “bathroom” in the woods |
| Cognitive dysfunction (n = 6) Concentration problems (n = 1) | Allowing extra time to sleep in the morning and for breaking down camp and packing up, full-time assistance by facilitator throughout all camping activities | |
| Obsessive-compulsive disorder symptoms (n = 1) | Allowing extra time for breaking down camp and packing up. Check by facilitators that all outdoor equipment is in order and in place in the tent | |
| Anxiety/depression (n = 9) | Supportive talks, individually guided meditation exercises, allowing extra time by themselves to process and recover, journaling | |
| Kayaking | Visual impairments (n = 2) | Double kayak with facilitator |
| Rock climbing | Visual impairments (n = 2) Peripheral neuropathy (n = 1) | Alternative activities such as learning bushcraft skills |
| Eating/Cooking | Allergies/intolerance (n = 6) | Home-made freeze-dried food |
| Gastro-intestinal problems (n = 4) | Medication |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jong, M.C.; Stub, T.; Mulder, E.; Jong, M. The Development and Acceptability of a Wilderness Programme to Support the Health and Well-Being of Adolescent and Young Adult Cancer Survivors: The WAYA Programme. Int. J. Environ. Res. Public Health 2022, 19, 12012. https://doi.org/10.3390/ijerph191912012
Jong MC, Stub T, Mulder E, Jong M. The Development and Acceptability of a Wilderness Programme to Support the Health and Well-Being of Adolescent and Young Adult Cancer Survivors: The WAYA Programme. International Journal of Environmental Research and Public Health. 2022; 19(19):12012. https://doi.org/10.3390/ijerph191912012
Chicago/Turabian StyleJong, Miek C., Trine Stub, Eric Mulder, and Mats Jong. 2022. "The Development and Acceptability of a Wilderness Programme to Support the Health and Well-Being of Adolescent and Young Adult Cancer Survivors: The WAYA Programme" International Journal of Environmental Research and Public Health 19, no. 19: 12012. https://doi.org/10.3390/ijerph191912012
APA StyleJong, M. C., Stub, T., Mulder, E., & Jong, M. (2022). The Development and Acceptability of a Wilderness Programme to Support the Health and Well-Being of Adolescent and Young Adult Cancer Survivors: The WAYA Programme. International Journal of Environmental Research and Public Health, 19(19), 12012. https://doi.org/10.3390/ijerph191912012