
Cost-Effectiveness of Positive Memory Training (PoMeT) for the Treatment of Depression in Schizophrenia

 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Outcome Assessment
2.3. Resource Use and Cost Assessment
2.4. Cost-Effectiveness Analysis
2.5. Sensitivity Analyses
2.6. Statistical Analyses
3. Results
3.1. Participants
3.2. Outcome Results
3.3. Resource Use and Cost Results
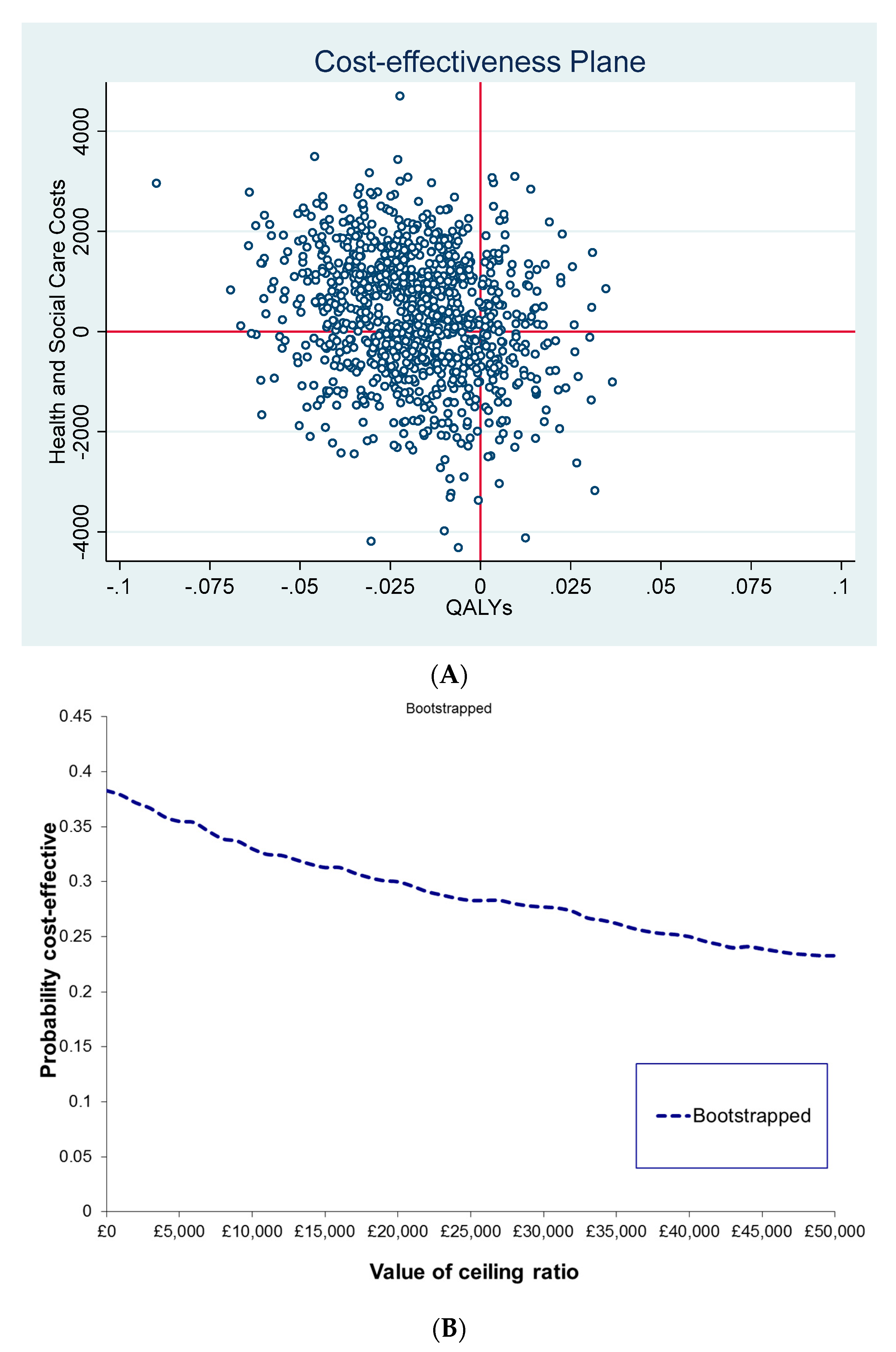
3.4. Cost-Effectiveness Analysis Results
3.5. Sensitivity Analyses Results
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mangalore, R.; Knapp, M. Cost of schizophrenia in England. J. Ment. Health Policy Econ. 2007, 10, 23–41. [Google Scholar]
- Knapp, M.; Mangalore, R.; Simon, J. The Global Costs of Schizophrenia. Schizophr. Bull. 2004, 30, 279–293. [Google Scholar] [CrossRef]
- Braga, R.J.; Reynolds, G.P.; Siris, S.G. Anxiety comorbidity in schizophrenia. Psychiatry Res. 2013, 210, 1–7. [Google Scholar] [CrossRef]
- NICE. Psychosis and Schizophrenia in Adults. Treatment and Management; National Institute for Health and Clinical Excellence (NICE): London, UK, 2014. [Google Scholar]
- van der Gaag, M.; Van Oosterhout, B.; Daalman, K.; Sommer, I.E.; Korrelboom, K. Initial evaluation of the effects of competitive memory training (COMET) on depression in schizophrenia-spectrum patients with persistent auditory verbal hallucinations: A randomized controlled trial. Br. J. Clin. Psychol. 2012, 51, 158–171. [Google Scholar] [CrossRef]
- Steel, C.; Korrelboom, K.; Baksh, M.F.; Kingdon, D.; Simon, J.; Wykes, T.; Phiri, P.; van der Gaag, M. Positive memory training for the treatment of depression in schizophrenia: A randomised controlled trial. Behav. Res. Ther. 2020, 135, 103734. [Google Scholar] [CrossRef]
- Steel, C.; Van Der Gaag, M.; Korrelboom, K.; Simon, J.; Phiri, P.; Baksh, M.F.; Wykes, T.; Rose, D.; Rose, S.; Hardcastle, M.; et al. A randomised controlled trial of positive memory training for the treatment of depression within schizophrenia. BMC Psychiatry 2015, 15, 85. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- NICE. Guide to the Methods of Technology Appraisal; National Institute for Health and Clinical Excellence (NICE): London, UK, 2013. [Google Scholar]
- NICE. Position Statement on Use of the EQ-5D-5L Valuation Set; National Institute for Health and Clinical Excellence (NICE): London, UK, 2017. [Google Scholar]
- Brazier, J.; Connell, J.; Papaioannou, D.; Mukuria, C.; Mulhern, B.; Peasgood, T.; Jones, M.L.; Paisley, S.; O’Cathain, A.; Barkham, M.; et al. A systematic review, psychometric analysis and qualitative assessment of generic preference-based measures of health in mental health populations and the estimation of mapping functions from widely used specific measures. Health Technol. Assess. 2014, 18. [Google Scholar] [CrossRef] [PubMed]
- Al-Janabi, H.; Peters, T.J.; Brazier, J.; Bryan, S.; Flynn, T.N.; Clemens, S.; Moody, A.; Coast, J. An investigation of the construct validity of the ICECAP-A capability measure. Qual. Life Res. 2013, 22, 1831–1840. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.; Anand, P.; Gray, A.; Rugkåsa, J.; Yeeles, K.; Burns, T. Operationalising the capability approach for outcome measurement in mental health research. Soc. Sci. Med. 2013, 98, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.M.; Al-Janabi, H.; Byford, S.; Kuyken, W.; Richardson, J.; Iezzi, A.; Coast, J. Assessing the validity of the ICECAP-A capability measure for adults with depression. BMC Psychiatry 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vergunst, F.; Jenkinson, C.; Burns, T.; Anand, P.; Gray, A.; Rugkåsa, J.; Simon, J. Psychometric validation of a multi-dimensional capability instrument for outcome measurement in mental health research (OxCAP-MH). Health Qual. Life Outcomes 2017, 15, 1–11. [Google Scholar] [CrossRef]
- Simon, J.; Mayer, S.; Łaszewska, A.; Rugkåsa, J.; Yeeles, K.; Burns, T.; Gray, A. Cost and quality-of-life impacts of community treatment orders (CTOs) for patients with psychosis: Economic evaluation of the OCTET trial. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 85–95. [Google Scholar] [CrossRef]
- Kingslake, J.; Dias, R.; Dawson, G.R.; Simon, J.; Goodwin, G.M.; Harmer, C.J.; Morriss, R.; Brown, S.; Guo, B.; Dourish, C.T.; et al. The effects of using the PReDicT Test to guide the antidepressant treatment of depressed patients: Study protocol for a randomised controlled trial. Trials 2017, 18, 558. [Google Scholar] [CrossRef]
- Beecham, J.; Knapp, M. Costing psychiatric interventions. Meas. Ment. Health Needs 2001, 2, 200–224. [Google Scholar]
- Curtis, L.; Burns, A. Unit Costs of Health and Social Care 2016; Personal Social Services Research Unit, University of Kent: Canterbury, UK, 2016. [Google Scholar]
- Department of Health. NHS Reference Costs 2015–2016; Department of Health: London, UK, 2016. [Google Scholar]
- ISD Scotland. Scottish National Tariff 2015–2016; ISD Scotland: Edinburgh, UK, 2016. [Google Scholar]
- Joint Formulary Committee. British National Formulary (BNF) 72 (September 2016–March 2017); Pharmaceutical Press: London, UK, 2016. [Google Scholar]
- Office for National Statistics (ONS). Annual Survey of Hours and Earnings: 2016 Provisional Results; ONS: Newport, UK, 2016. [Google Scholar]
- Neumann, P.J.; Sanders, G.D.; Russell, L.B.; Siegel, J.E.; Ganiats, T.G. Cost-Effectiveness in Health and Medicine; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Manca, A.; Hawkins, N.; Sculpher, M.J. Estimating mean QALYs in trial-based cost-effectiveness analysis: The importance of controlling for baseline utility. Health Econ. 2005, 14, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; Chapman & Hall: New York, NY, USA, 1993. [Google Scholar]
- Fenwick, E.; Byford, S. A guide to cost-effectiveness acceptability curves. Br. J. Psychiatry 2005, 187, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Stinnett, A.; Mullahy, J. Net Health Benefits: A New Framework for the Analysis of Uncertainty in Cost-Effectiveness Analysis. Med. Decis. Mak. 1998, 18 (Suppl. 2), S68–S80. [Google Scholar] [CrossRef] [PubMed]
- Van Hout, B.; Janssen, M.F.; Feng, Y.S.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Coretti, S.; Ruggeri, M.; McNamee, P. The minimum clinically important difference for EQ-5D index: A critical review. Expert Rev. Pharmacoeconomics Outcomes Res. 2014, 14, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Payakachat, N.; Ali, M.M.; Tilford, J.M. Can The EQ-5D Detect Meaningful Change? A Systematic Review. PharmacoEconomics 2015, 33, 1137–1154. [Google Scholar] [CrossRef] [PubMed]
- Helter, T.M.; Coast, J.; Łaszewska, A.; Stamm, T.; Simon, J. Comparison of capability and health-related quality of life instruments in capturing aspects of mental well-being in people with schizophrenia and depression. BJPsych Open 2022, 8, E117. [Google Scholar] [CrossRef]
- Craig, T.K.; Calafell, M.D.M.R.; Ward, T.; Leff, J.P.; Huckvale, M.; Howarth, E.; Emsley, R.; Garety, P. AVATAR therapy for auditory verbal hallucinations in people with psychosis: A single-blind, randomised controlled trial. Lancet Psychiatry 2018, 5, 31–40. [Google Scholar] [CrossRef]
- Opoka, S.M.; Lincoln, T.M. The effect of cognitive behavioral interventions on depression and anxiety symptoms in patients with schizophrenia spectrum disorders: A systematic review. Psychiatr. Clin. 2017, 40, 641–659. [Google Scholar] [CrossRef]


{kind=link}
| Health Economic Analysis Cohort | p-Value | ||||
|---|---|---|---|---|---|
| PoMeT (n = 48) | TAU (n = 46) | ||||
| n | % or Mean (SD) | n | % or Mean (SD) | ||
| Age | 48 | 42.92 (9.65) | 46 | 43.57 (11.22) | 0.765 |
| Gender | 0.194 | ||||
| Male | 33 | 68.75 | 37 | 80.43 | |
| Female | 15 | 31.25 | 9 | 19.57 | |
| Ethnicity | 0.198 | ||||
| White | 44 | 91.67 | 41 | 89.13 | |
| Asian | 0 | 0 | 3 | 6.52 | |
| Black | 2 | 4.17 | 2 | 4.35 | |
| Other | 2 | 4.17 | 0 | 0 | |
| Primary Diagnosis | 0.571 | ||||
| Schizophrenia | 33 | 68.75 | 32 | 69.57 | |
| Schizoaffective or psychosis NOS | 15 | 31.25 | 14 | 30.43 | |
| Age of first psychosis issue | 46 | 23.09 (9.38) | 44 | 22.05 (9.26) | 0.598 |
| Age of first MH contact | 46 | 25.17 (8.38) | 43 | 25.49(9.36) | 0.868 |
| Age of first psychosis services | 46 | 26.87(8.27) | 43 | 26.81 (9.53) | 0.977 |
| Depression Severity | 0.802 | ||||
| Mild/moderate | 20 | 41.67 | 18 | 39.13 | |
| Severe | 28 | 58.33 | 28 | 60.87 | |
| Accommodation | 0.249 | ||||
| Own accommodation | 7 | 14.58 | 8 | 17.39 | |
| Housing association/local authority accommodation | 28 | 58.33 | 24 | 52.17 | |
| In a relative’s/friend’s home | 9 | 18.75 | 8 | 17.39 | |
| Residential facilities | 4 | 8.33 | 6 | 13.04 | |
| Living Situation | 0.772 | ||||
| Living alone | 26 | 54.17 | 25 | 54.35 | |
| Living with others | 22 | 45.83 | 21 | 45.65 | |
| Higher Education | 0.216 | ||||
| Yes | 21 | 43.75 | 26 | 56.52 | |
| No | 27 | 56.25 | 20 | 43.48 | |
| Age left formal education | 47 | 16.40 (1.30) | 45 | 16.40 (1.54) | 0.989 |
| Employment | 0.554 | ||||
| Employed or self-employed | 6 | 12.50 | 5 | 10.87 | |
| Unemployed | 41 | 85.42 | 40 | 86.96 | |
| Retired | 1 | 2.08 | 1 | 2.17 | |
| Baseline EQ-5D-5L | 48 | 0.657 (0.286) | 45 | 0.597 (0.254) | 0.301 |
| Baseline EQ VAS | 48 | 52 (22.70) | 45 | 48 (18.52) | 0.373 |
| M0 Mean (SD) | M3 Mean (SD) | M6 Mean (SD) | M9 Mean (SD) | |
|---|---|---|---|---|
| EQ-5D-5L | ||||
| PoMeT (n = 48) | 0.657 (0.286) | 0.693 (0.210) | 0.677 (0.256) | 0.648 (0.264) |
| TAU (n = 46) | 0.600 (0.270) | 0.659 * (0.250) | 0.671 * (0.247) | 0.677 * (0.256) |
| EQ VAS | ||||
| PoMeT (n = 48) | 52 (22.70) | 60 * (19.36) | 58 (22.98) | 53 (24.10) |
| TAU (n = 46) | 48 (18.35) | 53 (25.33) | 51 (23.32) | 56 * (22.43) |
| Before Trial Costs (Extrapolated) | During Trial Costs | Before Trial vs. During Trial Costs | ||||||
|---|---|---|---|---|---|---|---|---|
| PoMeT (n = 48) | TAU (n = 46) | PoMET vs. TAU | PoMeT (n = 48) | TAU (n = 46) | PoMeT vs. TAU | PoMeT (n = 48) | TAU (n = 46) | |
| Cost category | Mean (SD) | Mean (SD) | Diff (95% CI) | Mean (SD) | Mean (SD) | Diff (95% CI) | Diff (95% CI) | Diff (95% CI) |
| (A) Mental Health (MH) Community, Outpatient and Inpatient Care | 2015 (3414) | 2274 (6093) | −259 (−2303 to 1785) | 1636 (2304) | 1370 (1798) | 265 (−580 to 1110) | 379 (−705 to 1464) | 904 (−878 to 2685) |
| MH Community Care | 1253 (2191) | 1070 (1530) | 183 (−589 to 955) | 891 (996) | 1111 (1743) | −220 (−807 to 367) | 363 (−109 to 835) | −41 (−637 to 556) |
| Drop-in Center | 425 (1339) | 208 (632) | 217 (−212 to 645) | 205 (509) | 203 (532) | 2 (−211 to 216) | 220 (−99 to 539) | 6 (−142 to 154) |
| Community Psychiatrist | 0 | 0 | 0 | 5 (23) | 5 (14) | −0.2 (−8 to 8) | −5 (−11 to 2) | −5 (−9 to −1) |
| Community Psychologist | 48 (334) | 0 | 48 (−49 to 145) | 3 (19) | 56 (291) | −53 (−140 to 33) | 46 (−52 to 143) | −56 (−142 to 31) |
| CPN | 373 (343) | 437 (652) | −63 (279 to 152) | 414 (411) | 438 (443) | −25 (−200 to 151) | −41 (−181 to 101) | −2 (−193 to 190) |
| Self Help Group | 332 (844) | 396 (992) | −64 (−442 to 314) | 222 (496) | 404 (1442) | −182 (−631 to 268) | 110 (−56 to 277) | −8 (−504 to 489) |
| Drug Alcohol Support | 75 (398) | 29 (139) | 46 (−76 to 168) | 43 (234) | 6 (33) | 37 (−31 to 106) | 32 (−16 to 80) | 24 (−10 to 58) |
| MH Outpatient Care | 393 (948) | 353 (399) | 40 (−257 to 338) | 263 (266) | 259 (209) | 3 (−94 to 101) | 131 (−160 to 421) | 94 (−30 to 218) |
| Outpatient Psychiatrist | 269 (251) | 314 (392) | −45 (−181 to 91) | 225 (199) | 227 (149) | −2 (−74 to 70) | 44 (−35 to 122) | 87 (−22 to 196) |
| Outpatient Psychologist | 124 (862) | 39 (149) | 85 (−168 to 339) | 37 (177) | 32 (151) | 5 (−62 to 72) | 87 (−170 to 344) | 7 (−58 to 71) |
| MH Inpatient Care | 368 (2550) | 850 (5581) | −482 (−2284 to 1319) | 482 (164) | 0 | 482 (−146 to 1110) | −113 (−1031 to 803) | −850 (−807 to 2508) |
| (B) Psychiatric Medication | 1006 (1011) | 839 (890) | 167 (−223 to 556) | 1359 (1338) | 1197 (779) | 162 (−401 to 726) | −353 (−566 to −141) * | −358 (−688 to −28) * |
| (C) Intervention (PoMeT) | 0 | 0 | 0 | 823 (354) | 0 | 823 (721 to 927) * | −823 (−927 to −721) * | 0 |
| MH Care: A + B + C | 3021 (3795) | 3113 (6272) | −92 (−2234 to 2049) | 3818 (2803) | 2567 (2370) | 1251 (185 to 2316) * | −798 (−1966 to 371) | 546 (−1291 to 2382) |
| (D) Non-Mental Health Care | 888 (1729) | 1112 (2058) | −224 (−1005 to 556) | 758 (1180) | 2247 (1014) | −1489 (−3557 to 578) | 130 (−305 to 565) | −1135 (−3284 to 914) |
| Primary Care | 182 (220) | 212 (254) | −30 (−127 to 67) | 175 (175) | 162 (166) | 13 (−56 to 83) | 7 (−32to 45) | 50 (−22 to 123) |
| General Practitioner (GP) | 163 (210) | 196 (245) | −33 (−127 to 60) | 150 (170) | 143 (159) | 7 (−60 to 75) | 12 (−21 to 46) | 53 (−17 to 122) |
| GP Practice Nurse | 19 (35) | 16 (32) | 3 (−11 to 17) | 25 (38) | 18 (30) | 6 (−8 to 20) | −6 (−16 to 5) | −2 (−15 to 10) |
| NMH Community Care | 279 (423) | 244 (379) | −35 (−129 to 199) | 218 (268) | 367 (720) | −148 (−375 to 78) | 61 (−58 to 181) | −123 (−362 to 117) |
| Community District Nurse | 11 (62) | 7 (50) | 4 (−19 to 27) | 25 (119) | 13 (57) | 11 (−26 to 49) | −14 (−33 to 5) | −6 (−29 to 17) |
| Occupational Therapy | 6 (44) | 28 (190) | −22 (−79 to 36) | 4 (15) | 98 (553) | 50 (−29 to 129) | 2 (−12 to 16) | −70 (−244 to 104) |
| Physiotherapy | 0 | 10 (65) | −10 (−29 to 10) | 9 (45) | 22 (77) | −14 (−40 to 13) | −9 (−22 to 5) | −13 (−35 to 10) |
| Emergency Services | 59 (246) | 24 (112) | 35 (−43 to 114) | 20 (79) | 77 (185) | −57 (−116 to 2) | 39 (−24 to 103) | −53 (−120 to 13) |
| Alternative Care | 25 (171) | 0 | 25 (−25 to 74) | 0 | 9 (58) | −9 (−26 to 9) | 25 (−25 to 74) | −9 (−26 to 9) |
| Other Health Care | 178 (302) | 176 (234) | 3 (−108 to 113) | 161 (189) | 148 (186) | 12 (−64 to 89) | 18 (−67 to 103) | 28 (−53 to 108) |
| NMH Out- and Daypatient Care | 221 (592) | 446 (1294) | −226 (−643 to 192) | 164 (328) | 286 (759) | −122 (−365 to 121) | 57 (−98 to 213) | 161 (−267 to 589) |
| Accident and Emergency | 28 (108) | 48 (167) | −20 (−78 to 38) | 41 (114) | 48 (112) | −7 (−53 to 40) | −14 (−61 to 34) | 0 (−62 to 62) |
| NMH Outpatient | 130 (319) | 399 (1267) | −269 (−655 to 117) | 102 (245) | 175 (408) | −73 (−212 to 66) | 28 (−84 to 139) | 224 (−142 to 589) |
| Daypatient | 64 (441) | 0 | 64 (−64 to 192) | 21 (123) | 63 (367) | −42 (−156 to 72) | 43 (−50 to 136) | −63 (−172 to 46) |
| NMH Inpatient Care | 206 (1151) | 209 (992) | −3 (−443 to 436) | 201 (839) | 1433 (6379) | −1232 (−3141 to 676) | 5 (−372 to 383) | −1224 (−3155 to 708) |
| Health Care: A + B + C + D | 3909 (3887) | 4225 (6893) | −317 (−2631 to 1998) | 4576 (2894) | 4814 (7238) | −239 (−2532 to 2055) | −668 (−1876 to 541) | −589 (−3483 to 2304) |
| (E) Social Care | 784 (1836) | 1520 (4282) | −736 (−2016 to 633) | 1118 (2438) | 745 (2397) | 373 (−618 to 1363) | −335 (−931 to 261) | 775 (−504 to 2054) |
| Social Worker | 180 (546) | 793 (3686) | −613 (−1718 to 492) | 254 (522) | 208 (473) | 46 (−157 to 250) | −74 (−261 to 112) | 585 (−440 to 1610) |
| Home Helper | 103 (698) | 78 (519) | 25 (−226 to 277) | 29 (181) | 172 (1058) | −143 (−461 to 175) | 74 (−136 to 285) | −94 (−255 to 67) |
| Housing Worker | 4 (22) | 35 (110) | −32 (−65 to 1) | 31 (178) | 21 (97) | 10 (−48 to 69) | −28 (−79 to 24) | 15 (−13 to 42) |
| Community Support Worker | 478 (1544) | 561 (1963) | −83 (−809 to 643) | 789 (2180) | 334 (1110) | 454 (−253 to 1162) | −311 (−1024 to 403) | 227 (−385 to 838) |
| Volunteer Helper | 19 (93) | 53 (215) | −34 (−103 to 35) | 15 (56) | 11 (53) | 4 (−18 to 27) | 4 (−27 to 35) | 43 (−17 to 103) |
| Health and Social Care: A + B + C + D + E | 4692 (4324) | 5746 (7721) | −1054 (−3643 to 1535) | 5694 (3997) | 5560 (7588) | 134 (−2378 to 2646) | −1002 (−2661 to 257) | 186 (−2857 to 3229) |
| (F) Total Indirect Costs | 1617 (3070) | 4920 (13782) | −3303 (−7482 to 876) | 2300 (4607) | 2762 (5894) | −462 (−2638 to 1713) | −683 (−1924 to 558) | 2158 (−1367 to 5683) |
| Lost Productivity (days) | 49 (301) | 298 (1502) | −250 (−704 to 204) | 176 (1027) | 95 (457) | 81 (−244 to 406) | −127 (−338 to 84) | 203 (−236 to 643) |
| Informal Care | 1568 (3081) | 4521 (13750) | −3053 (−7224 to 1117) | 2124 (4489) | 2667 (5908) | −543 (−2702 to 1616) | −556 (−1765 to 653) | 1954 (−1547 to 5456) |
| Societal: A + B + C + D + E + F | 6309 (5344) | 10666 (15826) | −4357 (−9283 to 569) | 7994 (6623) | 8322 (9843) | −328 (−3836 to 3081) | −1685 (−3444 to 73) | 2344 (−2474 to 7161) |
| Perspective | Cost Difference (95% CI) PoMeT vs. TAU | QALY Difference (95% CI) PoMeT vs. TAU | ICER (95% CI) PoMeT vs. TAU | Interpretation of ICER |
|---|---|---|---|---|
| Health and social care | £270 (−£2191 to £2731) | −0.0177 (−0.0538 to 0.0186) | −£15,254/QALY (−£347,765/QALY to £645,414/QALY) | PoMeT on average is more expensive and less effective |
| Societal | −£458 (−£3783 to £2868) | −0.0175 (−0.0537 to 0.0186) | £26,171/QALY (−£666,926/QALY to £788,883/QALY) | PoMeT on average is less expensive but less effective |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon, J.; Kiss, N.; Korrelboom, K.; Kingdon, D.; Wykes, T.; Phiri, P.; van der Gaag, M.; Baksh, M.F.; Steel, C. Cost-Effectiveness of Positive Memory Training (PoMeT) for the Treatment of Depression in Schizophrenia. Int. J. Environ. Res. Public Health 2022, 19, 11985. https://doi.org/10.3390/ijerph191911985
Simon J, Kiss N, Korrelboom K, Kingdon D, Wykes T, Phiri P, van der Gaag M, Baksh MF, Steel C. Cost-Effectiveness of Positive Memory Training (PoMeT) for the Treatment of Depression in Schizophrenia. International Journal of Environmental Research and Public Health. 2022; 19(19):11985. https://doi.org/10.3390/ijerph191911985
Chicago/Turabian StyleSimon, Judit, Noemi Kiss, Kees Korrelboom, David Kingdon, Til Wykes, Peter Phiri, Mark van der Gaag, M. Fazil Baksh, and Craig Steel. 2022. "Cost-Effectiveness of Positive Memory Training (PoMeT) for the Treatment of Depression in Schizophrenia" International Journal of Environmental Research and Public Health 19, no. 19: 11985. https://doi.org/10.3390/ijerph191911985
APA StyleSimon, J., Kiss, N., Korrelboom, K., Kingdon, D., Wykes, T., Phiri, P., van der Gaag, M., Baksh, M. F., & Steel, C. (2022). Cost-Effectiveness of Positive Memory Training (PoMeT) for the Treatment of Depression in Schizophrenia. International Journal of Environmental Research and Public Health, 19(19), 11985. https://doi.org/10.3390/ijerph191911985