

Social Infrastructure and Street Networks as Critical Infrastructure for Aging Friendly Community Design: Mediating the Effect of Physical Activity



Abstract
1. Introduction
- (1)
- explore the community characteristics that affect older adults’ functional capability by influencing the three different intensities of PA.
- (2)
- understand the environmental factors affecting older adults’ satisfaction levels with their community environment.
2. Materials and Methods
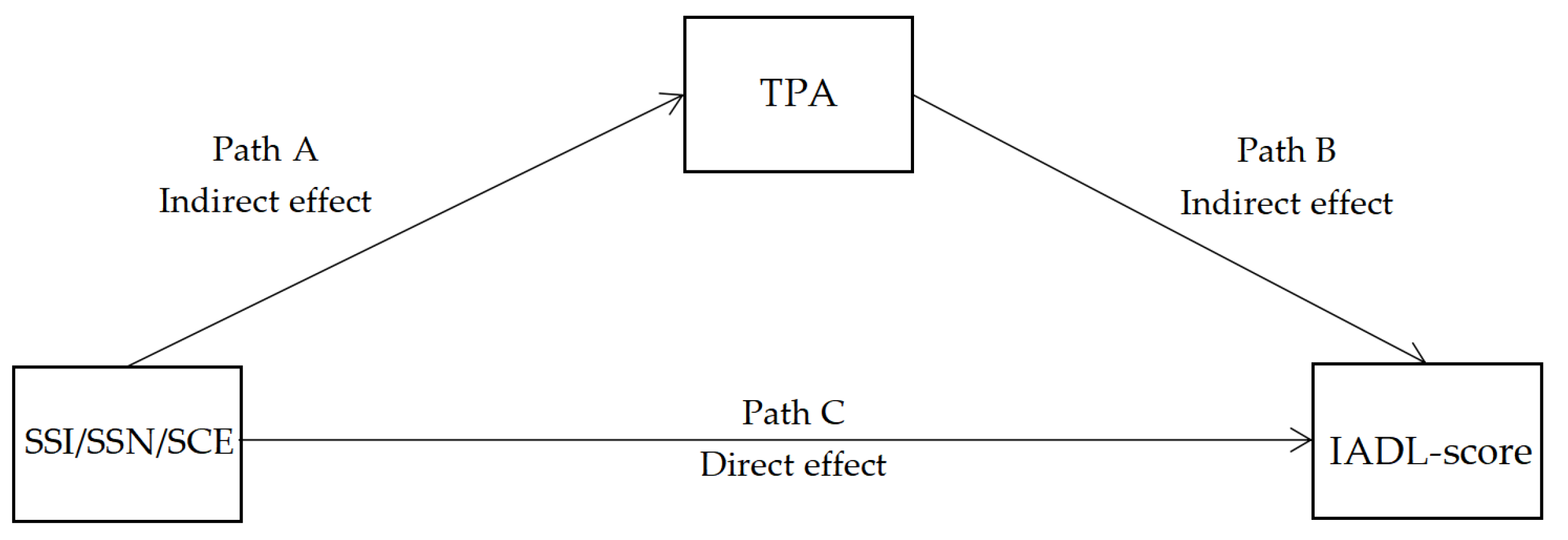
2.1. Conceptual Framework
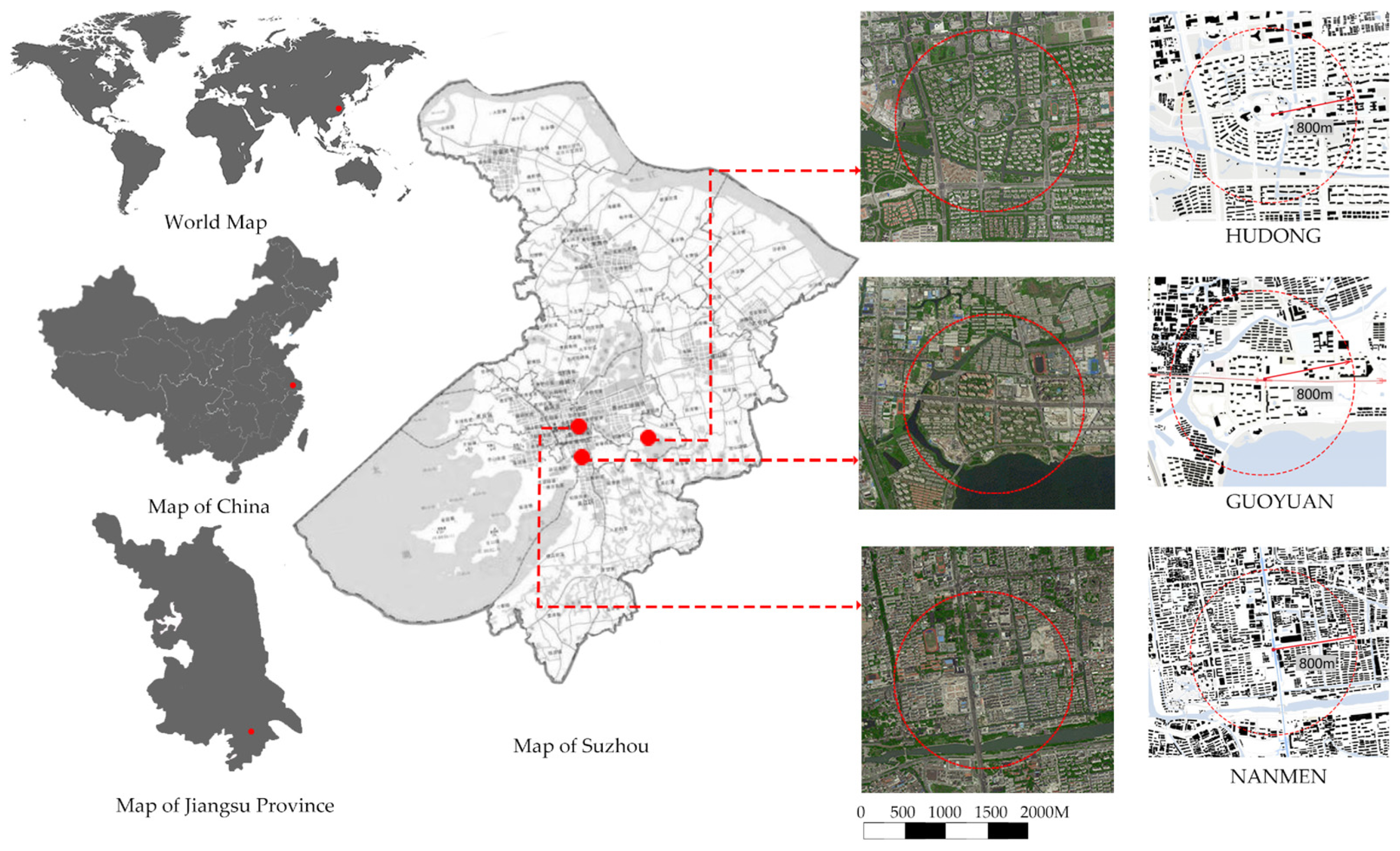
2.2. Study Samples
2.3. Data Collection
2.3.1. Physical Activity (Mediating Variable)
2.3.2. Physical Functional Capability among Older Adults
2.3.3. Dimensions of Built Environment Characteristics
2.3.4. Socioeconomic Attributes (Covariant)
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
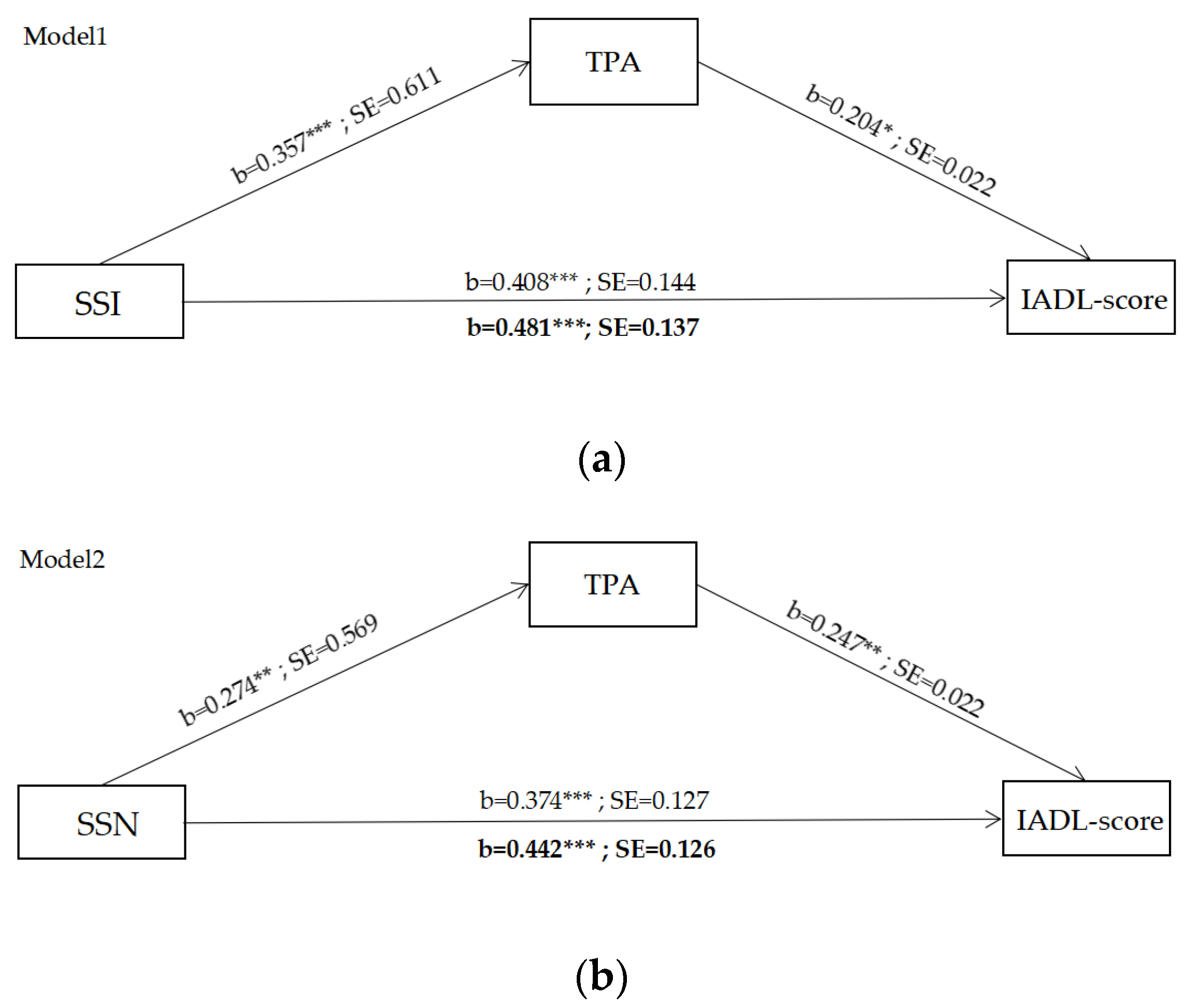
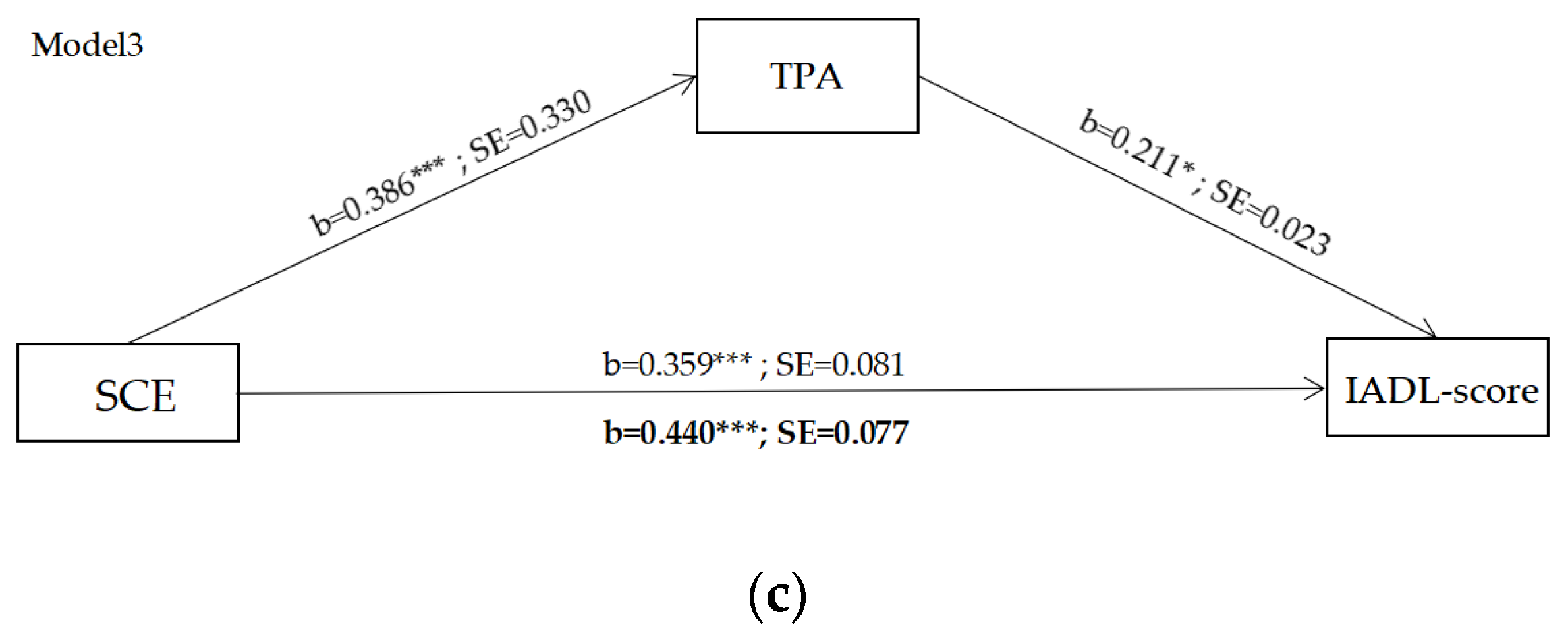
3.2. Results of Mediating Effect Model
3.3. Results of the Multilevel Regression Model
3.3.1. Influences of Community Facilities on Older Adults’ SSI
3.3.2. Influences of Street Network Quality on Older Adults’ SSN
4. Discussion
4.1. The Effects of SSI, SSN, and SCE on Physical Functions Mediated by PA
4.2. The Effect of Environmental Factors on Older Adults’ Satisfaction Levels
4.3. Planning Implications
- Pay more attention to the impact of community streets on vigorous-intensity physical activity (VPA) of older adults. Provide supportive social relationships through age-friendly street networks and, specifically, focus on street green space quality and street safety.
- Provide supportive social relationships through age-friendly infrastructures, especially public communication spaces and the diversity of rest facilities.
- Provide full coverage and high-quality community facilities, primarily cultural, artistic, and commercial services.
4.4. Limitations of the Study
5. Conclusions
- Three variables of community-level satisfaction (the overall community environment, street networks, and social infrastructures) affected older adults’ physical functions by influencing older adults’ TPA.
- Two variables of community-level satisfaction (SSI and SSN) affected older adults’ physical functions by affecting the total duration of MPA and VPA, especially VPA.
- GS and ACI positively correlated with SSN, PCS, and DRF, while SPV positively correlated with SSI, and EDU positively correlated with SSN passively.
- Street safety and quality of street green space promote older adults’ physical health by promoting VPA, and quality of GS and ACI promotes older adults’ physical health by promoting MPA and VPA.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Health and Aging; World Health Organisation: Geneva, Switzerland, 2011.
- Sun, Y.; Li, J.; Jin, X.; Xiao, H.; He, Z.; Su, S.; Weng, M. Intra-urban excessive alcohol drinking: Geographic disparities, associated neighborhood characteristics and implications for healthy city planning. Sustain. Cities Soc. 2019, 46, 101414. [Google Scholar] [CrossRef]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E. The meaning of “aging in place” to older people. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Nagel, C.L.; Carlson, N.E.; Bosworth, M.; Michael, Y.L. The relation between neighborhood-built environment and walking activity among older adults. Am. J. Epidemiol. 2008, 168, 461–468. [Google Scholar] [CrossRef]
- Barnett, D.W.; Barnett, A.; Nathan, A. Van Cauwenberg, J.; Cerin, E. Built environmental correlates of older adults’ total PA and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Green space is associated with walking and moderate-to-vigorous physical activity (MVPA) in middle-to-older-aged adults: Findings from 203 883 Australians in the 45 and Up Study. Br. J. Sports Med. 2014, 48, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Division of Ageing and Seniors. Physical Activity and Older Adults from Canada; Statistics Canada: Ottawa, ON, Canada, 2011.
- Moran, M.; Van Cauwenberg, J.; Hercky-Linnewiel, R.; Cerin, E.; Deforche, B.; Plaut, P. Understanding the relationships between the physical environment and physical activity in older adults: A systematic review of qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Medicine 2009, 41, 1510–1530. [Google Scholar]
- Grinde, B.; Patil, G.G. Biophilia: Does visual contact with nature impact on health and well-being? Int. J. Environ. Res. Public Health 2009, 6, 2332–2343. [Google Scholar] [CrossRef]
- Takano, T.; Nakamura, K.; Watanabe, M. Urban residential environments and senior citizens longevity in megacity areas: The importance of walkable green spaces. J. Epidemiol. Community Health 2002, 56, 913–918. [Google Scholar] [CrossRef]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organisation: Geneva, Switzerland, 2021.
- Handy, S.L.; Boarnet, M.G.; Ewing, R.; Killingsworth, R.E. How the built environment affects physical activity: Views from urban planning. Am. J. Prev. Med. 2002, 23, 64–73. [Google Scholar] [CrossRef]
- Marshall, W.E.; Garrick, N.; Piatkowski, D.P.; Newton, D. Chapter seventeen-community design, street networks, and public health. In Advances in Transportation and Health; Mark, J., Nieuwenhuijsen, M., Khreis, H., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 371–388. [Google Scholar]
- Van Holle, V.; Deforche, B.; Van Cauwenberg, J.; Goubert, L.; Maes, L.; Van de Weghe, N.; De Bourdeaudhuij, I. Relationship between the physical environment and different domains of physical activity in European adults: A systematic review. BMC Public Health 2012, 12, 807. [Google Scholar] [CrossRef] [PubMed]
- Pearsall, H.; Heck, S.; Tablas, M.; Pierce, J.; Hinrichs, C.; Roman, L.A.; Shabazz, J. Building knowledge infrastructure for diverse stakeholders to scale up co-production equitably. Curr. Opin. Environ. Sustain. 2022, 54, 101156. [Google Scholar] [CrossRef]
- Depietri, Y. Planning for urban green infrastructure: Addressing tradeoffs and synergies. Curr. Opin. Environ. Sustain. 2022, 54, 101148. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef]
- Wu, Y.T.; Prina, M.; Matthews, F. The availability of local primary care services, satisfaction with health services and self-rated health in older English adults: A population-based study. Prev. Med. Rep. 2022, 27, 101786. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, Y.; Lu, S.; Chan, O.F.; Chui, C.; Lum, T. Objective and perceived built environment, sense of community, and mental wellbeing in older adults in Hong Kong: A multilevel structural equation study. Landsc. Urban Plan. 2021, 209, 104058. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. The Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Lawton, M.P. Environment and other determinants of weil-being in older people. Gerontologist 1983, 23, 349–357. [Google Scholar] [CrossRef]
- Lawton, M.P.; Nahemow, L. Ecology and the aging process. In The Psychology of Adult Development and Aging; Eisdorfer, C., Lawton, M.P., Eds.; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Kerr, J.; Carlson, J.; Rosenberg, D.; Withers, A. Identifying and promoting safe walking routes in older adults. Health 2012, 4, 720–724. [Google Scholar] [CrossRef]
- Cerin, E.; Conway, T.; Saelens, B.; Frank, L.; Sallis, J. Cross-validation of the factorial structure of the Neighborhood Environment Walkability Scale (NEWS) and its abbreviated form (NEWS-A). Int. J. Behav. Nutr. Phys. Act. 2009, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Clemente, O.; Ewing, R. Identifying and Measuring Urban Design Qualities Related to Walkability. J. Phys. Act. Health 2006, 3, S223–S240. [Google Scholar]
- Clemente, O.; Ewing, R. Measuring Urban Design Qualities: An Illustrated Field Manual; University of Maryland: College Park, MD, USA, 2005. [Google Scholar]
- World Health Organization (WHO). The World Health Organization Quality of Life (WHOQOL)-BREF; World Health Organisation: Geneva, Switzerland, 2012.
- Lee, R.E.; Booth, K.M.; Reese-Smith, J.Y. The Physical Activity Resource Assessment (PARA) instrument: Evaluating features, amenities and incivilities of physical activity resources in urban neighborhoods. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 1–9. [Google Scholar] [CrossRef] [PubMed]
- SIP 4-99 Research Group. Environmental Supports for Physical Activity Questionnaire; Prevention Research Center, Norman J. Arnold School of Public Health, University of South Carolina: Columbia, SC, USA, 2002. [Google Scholar]
- Saint-Louis Environment and Physical Activity Instrument. Available online: https://bel.uqtr.ca/id/eprint/3228/1/Saint-Louis%20Environment%20and%20Physical%20Activity%20Instrument.pdf (accessed on 25 January 2006).
- Qiao, W.; Sheng, Y.; Fang, B.; Wang, Y. Land use change information mining in highly urbanized area based on transfer matrix:A case study of Suzhou. Geogr. Reserrch 2013, 8, 1497–1507. [Google Scholar]
- Gillen, G. Chapter 1-overview of cognitive and perceptual rehabilitation. In Cognitive and Perceptual Rehabilitation; Mosby Elsevier: Maryland Heights, MO, USA, 2009; pp. 1–31. [Google Scholar]
- Australia, I. An assessment of Australia’s future infrastructure needs. Aust. Infrastruct. Audit. 2019, 6, 158–208. [Google Scholar]
- Mehta, V. The Street: A Quint Essential Social Public Space; Routledge: Abingdon, UK; New York, NY, USA,, 2013; pp. 1–237. [Google Scholar]
- Xu, L.; Shi, J. Walking activity quality and built environment: Take three commercial streets in Shanghai as examples. Shanghai Urban Plan. Rev. 2017, 1, 17–24. [Google Scholar]
- Harvey, C.; Aultman-Hall, L.; Hurley, S.E.; Troy, A. Effects of skeletal streetscape design on perceived safety. Landsc. Urban Plan. 2015, 142, 18–28. [Google Scholar] [CrossRef]
- Ewing, R.; Clemente, O. Measuring Urban Design: Metrics for Livable Places; Island Press: Washington, DC, USA, 2013. [Google Scholar]
- Chan, E.T.H.; Schwanen, T.; Banister, D. The role of perceived environment, neighbourhood characteristics, and attitudes in walking behaviour: Evidence from a rapidly developing city in China. Transportation 2021, 48, 431–454. [Google Scholar] [CrossRef]
- Moniruzzaman, M.; Páez, A. A model-based approach to select case sites for walkability audits. Health Place 2012, 18, 1323–1334. [Google Scholar] [CrossRef]
- Li, X.; Li, Z.; Jia, T.; Yan, P.; Wang, D.; Liu, G. The sense of community revisited in Hankow, China: Combining the impacts of perceptual factors and built environment attributes. Cities 2021, 111, 103108. [Google Scholar] [CrossRef]
- Kim, Y.S.; Moon, J.H. Factors affecting perception of marriage needs including health related variables: In 20–30s unmarried workers. J. Digit. Converg. 2019, 17, 225–233. [Google Scholar]
- Song, S.; Yap, W.; Hou, Y.; Yuen, B. Neighbourhood built environment, physical activity, and physical health among older adults in Singapore: A simultaneous equations approach. J. Transp. Health 2020, 18, 100881. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium Commun. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed]
- Maasakkers, C.M.; Melis, R.; Kessels, R.; Gardiner, P.A.; Olde Rikkert, M.; Thijssen, D.; Claassen, J. The short-term effects of sedentary behaviour on cerebral hemodynamics and cognitive performance in older adults: A cross-over design on the potential impact of mental and/or physical activity. Alzheimer’s Res. Ther. 2020, 12, 76. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Helbich, M.; Yao, Y.; Zhang, J.; Liu, P.; Yuan, Y.; Liu, Y. Urban greenery and mental wellbeing in adults: Cross-sectional mediation analyses on multiple pathways across different greenery measures. Environ. Res. 2019, 176, 108535. [Google Scholar] [CrossRef]
- Tuckett, A.G.; Banchoff, A.W.; Winter, S.J.; King, A.C. The built environment and older adults: A literature review and an applied approach to engaging older adults in built environment improvements for health. Int. J. Older People Nurs. 2018, 13, 12171. [Google Scholar] [CrossRef]
- Zhong, S.; Lee, C.; Lee, H. The role of community environments in older adults’ intergenerational and peer social interactions. Cities 2022, 10, 1016. [Google Scholar] [CrossRef]
- Newton, R.; Ormerod, M.; Burton, E.; Mitchell, L.; Ward-Thompson, C. Increasing independence for older people through good street design. Int. J. Integr. Care 2010, 18, 24–29. [Google Scholar] [CrossRef]
- Canning, K.L.; Brown, R.E.; Jamnik, V.K.; Salmon, A.; Ardern, C.I.; Kuk, J.L. Individuals underestimate moderate and vigorous intensity physical activity. PLoS ONE 2014, 9, e97927. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Miao, J.; Lu, Y.; Song, Y.; Chen, L.; Liu, Y. Urban greenery mitigates the negative effect of urban density on older adults’ life satisfaction: Evidence from Shanghai, China. Cities 2022, 124, 103607. [Google Scholar] [CrossRef]
- Wu, H.; Kumar, P.; Cao, S. Implementation of green infrastructure for improving the building environment of elderly care centres. J. Build. Eng. 2022, 54, 104682. [Google Scholar] [CrossRef]
- Jessica, K.B.; Bu, F.; Fluharty, M.E.; Paul, E.; Sonke, J.K.; Fancourt, D. Engagement in leisure activities and depression in older adults in the United States: Longitudinal evidence from the Health and Retirement Study. Soc. Sci. Med. 2022, 294, 114703. [Google Scholar]
- Poppe, L.; Deforche, B.; Cauwenberg, J.V.; Brondeel, R.; Mertens, L.; Weghe, N.V.; Benoit, S.; Veitch, J.; Dyck, D.V. The association between the number of parks near home and levels of physical activity among community-dwelling older adults: A longitudinal study. Cities 2022, 130, 103931. [Google Scholar] [CrossRef]
- Lei, P.; Feng, Z. Age-friendly neighbourhoods and depression among older people in China: Evidence from China family panel studies. J. Affect. Disord. 2021, 286, 187–196. [Google Scholar] [CrossRef]
- Bellazzecca, E.; Teasdale, S.; Biosca, O.; Skelton, D.A. The health impacts of place-based creative programmes on older adults’ health: A critical realist review. Health Place 2022, 76, 102839. [Google Scholar] [CrossRef] [PubMed]
- Lian, J.W.; Yen, D.C. Online shopping drivers and barriers for older adults: Age and gender differences. Comput. Hum. Behav. 2014, 37, 133–143. [Google Scholar] [CrossRef]
- Frank, L.; Kerr, J.; Rosenberg, D.; King, A. Healthy aging and where you live: Community design relationships with physical activity and body weight in older Americans. J. Phys. Act. Health 2010, 7, 82–90. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, H.; Yang, X.; Li, G. Neighborhood streets as places of older adults’ active travel and social interaction-a study in Daokou ancient town. J. Transp. Health 2022, 24, 101309. [Google Scholar] [CrossRef]
- Benjamin, B.J.H.; Van Dyck, D.; Deforche, B.; Van de Weghe, N.; Boussauw, K.; Mertens, L. Creating safe and attractive environments for cycling: Which factors are important for older adults? A think-aloud Study in virtual reality. J. Transp. Health 2022, 25, 101430. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tools and Measures | Topics | Domains |
|---|---|---|
| Walking Route Audit Tool for Seniors (WRATS) [26] | Community street networks (the best walking routes for older adults, transportation, roads and streets, pedestrian facilities, bike facilities, traffic safety, parks and recreation, parks, recreation programs) | Community street networks |
| Neighborhood Environment Walkability Survey (NEWS) & Neighborhood Environment Walkability Survey-Abbreviated (NEWS-A) [27] | Community environment attributes relate to physical activity | Community environment |
| Measurement Instrument for Urban Design Quantities Related to Walkability [28] | Community environment (communities, architecture and building design, social and cultural environment) | Community environment |
| Measuring Urban Design Qualities—An Illustrated Field Manual [29] | Community street networks (imageability, enclosure, human scale, transparency, complexity) | Community environment |
| Instrumental activities of daily living (IADL) [22] | Instrumental activities (ability to use telephone, shopping, food preparation, housekeeping, laundry, mode of transportation, responsibility for own medications) | Daily activities (e.g., physical activities, social activities) |
| World Health Organization Quality of Life (WHOQOL)-BREF [30] | Multiple domains | Quality of life |
| Physical Activity Resource Assessment (PARA) Instrument [31] | Physical activity | Physical activity |
| Environmental Supports for Physical Activity Questionnaire [32] | Multiple domains | Multiple domains |
| Saint Louis Environment and Physical Activity Instrument [33] | Multiple domains | Multiple domains |
| Categories | Variables | Scale |
|---|---|---|
| Satisfaction of social infrastructure (SSI) | ||
| Educational infrastructure (EDU) | 1. The degree of subject satisfaction with each subtype of the infrastructure | 5—Satisfied 4—Slightly satisfied 3—Neutral 2—Slightly unsatisfied 1—Very unsatisfied |
| Health and aged care services (HCS) | ||
| Commercial services (CS) | ||
| Arts and cultural infrastructure (ACI) | ||
| Green and blue space (GBS) 1 | ||
| Recreational infrastructure (RI) | ||
| Social infrastructure (SI) | 2. The degree of subject satisfaction with the overall category of infrastructure. | |
| Satisfaction of street networks (SSN) | ||
| Public communication space (PCS) | 1. The degree of subject satisfaction with each subtype of the street networks | 5—Satisfied 4—Slightly satisfied 3—Neutral 2—Slightly unsatisfied 1—Very unsatisfied |
| Green space (GS) 2 | ||
| Street accessibility (SA) | ||
| Street walkability (SW) | ||
| Diversity of rest facilities (DRF) | ||
| Street networks (SN) | 2. The degree of subject satisfaction with the overall category of infrastructure. | |
| Satisfaction of community environment (SCE) | ||
| Community environment (CE) | The degree of subject satisfaction with the overall category of community environment. | 5—Satisfied 4—Slightly satisfied 3—Neutral 2—Slightly unsatisfied 1—Very unsatisfied |
| Categories | Variables | Number of Participants | Percentage of Participants (%) |
|---|---|---|---|
| Community of Location | HUDONG | 35 | 32.4% |
| GUOYUAN | 34 | 31.5% | |
| NANMEN | 39 | 36.1% | |
| Gender | Male | 54 | 50 |
| Female | 54 | 50 | |
| Education | Junior high school or below | 30 | 27.8 |
| High school | 60 | 55.6 | |
| College or above | 18 | 16.6 | |
| Household income (RMB/month) | Below 3000 | 23 | 21.3 |
| 3000 to 5000 | 35 | 32.4 | |
| 5000 to 10,000 | 32 | 29.6 | |
| 10,000 and above | 18 | 16.7 | |
| Household structure | Lives alone | 28 | 25.9 |
| Lives with spouse | 80 | 74.1 | |
| Living with children | 61 | 56.5 | |
| Living without children | 47 | 43.5 |
| Model | Path | Effect | SE | 95%CI | |
|---|---|---|---|---|---|
| Lower CI | Upper CI | ||||
| SSI→IADL-score | Total indirect effect | 0.111 | 0.075 | 0.009 | 0.285 |
| SSN→IADL-score | 0.094 | 0.066 | 0.002 | 0.251 | |
| SCE→IADL-score | 0.068 | 0.046 | 0.004 | 0.175 | |
| Model | Path | Effect | SE | 95%CI | |||
|---|---|---|---|---|---|---|---|
| Lower CI | Upper CI | ||||||
| SSI→IADL-score | SSI | LPA | IADL-score | −0.069 | 0.112 | −0.296 | 0.153 |
| SSI | MPA | IADL-score | 0.111 | 0.094 | −0.056 | 0.311 | |
| SSI | VPA | IADL-score | 0.234 | 0.067 | 0.118 | 0.376 | |
| Total indirect effect | 0.276 | 0.098 | 0.098 | 0.480 | |||
| SSN→IADL-score | SSN | LPA | IADL-score | −0.136 | 0.090 | −0.325 | 0.029 |
| SSN | MPA | IADL-score | 0.146 | 0.085 | 0.014 | 0.342 | |
| SSN | VPA | IADL-score | 0.227 | 0.067 | 0.113 | 0.376 | |
| Total indirect effect | 0.237 | 0.093 | 0.074 | 0.438 | |||
| SCE→IADL-score | SCE | LPA | IADL-score | 0.192 | 0.233 | −0.2550 | 0.682 |
| SCE | MPA | IADL-score | −0.131 | 0.207 | −0.593 | 0.240 | |
| SCE | VPA | IADL-score | 0.251 | 0.117 | 0.034 | 0.492 | |
| Total indirect effect | 0.313 | 0.265 | −0.245 | 0.799 | |||
| Model | Model Summary | Variance Analysis | Unstandardized Coefficients | |||||
| R | R2 | F | Sig | B | Std. Error | t | Sig. | |
| (Constant) | 0.845 | 0.714 | 58.638 | 0.000 | 3.058 *** | 0.511 | 5.986 | 0.000 |
| ACI 2 | 0.328 *** | 0.059 | 5.585 | 0.000 | ||||
| GS 3 | 0.329 *** | 0.063 | 5.248 | 0.000 | ||||
| EDU 4 | −0.746 *** | 0.135 | −5.541 | 0.000 | ||||
| CS 5 | 0.170 * | 0.072 | 2.356 | 0.021 | ||||
| Model | Model Summary | Variance Analysis | Unstandardized Coefficients | |||||
| R | R2 | F | Sig | B | Std. Error | t | Sig. | |
| (Constant) | 0.806 | 0.650 | 43.550 | 0.000 | 0.147 | 0.203 | 0.725 | 0.470 |
| PCS 2 | 0.291 *** | 0.072 | 4.056 | 0.000 | ||||
| DRF 3 | 0.235 ** | 0.068 | 3.461 | 0.001 | ||||
| SPV 4 | 0.230 ** | 0.068 | 3.387 | 0.001 | ||||
| GS 5 | 0.177 * | 0.074 | 2.394 | 0.019 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, J.; Xia, Z.; Sun, X.; Wang, X.; Luo, S. Social Infrastructure and Street Networks as Critical Infrastructure for Aging Friendly Community Design: Mediating the Effect of Physical Activity. Int. J. Environ. Res. Public Health 2022, 19, 11842. https://doi.org/10.3390/ijerph191911842
Jiang J, Xia Z, Sun X, Wang X, Luo S. Social Infrastructure and Street Networks as Critical Infrastructure for Aging Friendly Community Design: Mediating the Effect of Physical Activity. International Journal of Environmental Research and Public Health. 2022; 19(19):11842. https://doi.org/10.3390/ijerph191911842
Chicago/Turabian StyleJiang, Jiayi, Zhengwei Xia, Xiaodi Sun, Xuanxuan Wang, and Shixian Luo. 2022. "Social Infrastructure and Street Networks as Critical Infrastructure for Aging Friendly Community Design: Mediating the Effect of Physical Activity" International Journal of Environmental Research and Public Health 19, no. 19: 11842. https://doi.org/10.3390/ijerph191911842
APA StyleJiang, J., Xia, Z., Sun, X., Wang, X., & Luo, S. (2022). Social Infrastructure and Street Networks as Critical Infrastructure for Aging Friendly Community Design: Mediating the Effect of Physical Activity. International Journal of Environmental Research and Public Health, 19(19), 11842. https://doi.org/10.3390/ijerph191911842