
Prevalence and Correlates of Underweight among Women of Reproductive Age in Nepal: A Cross-Sectional Study

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Data Sources
2.2. Sampling Design
2.3. Data Collection
2.4. Sample Size
2.5. Outcome Variable
2.6. Explanatory Variables
2.6.1. Sociodemographic Factors
2.6.2. Household Environmental Factors
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
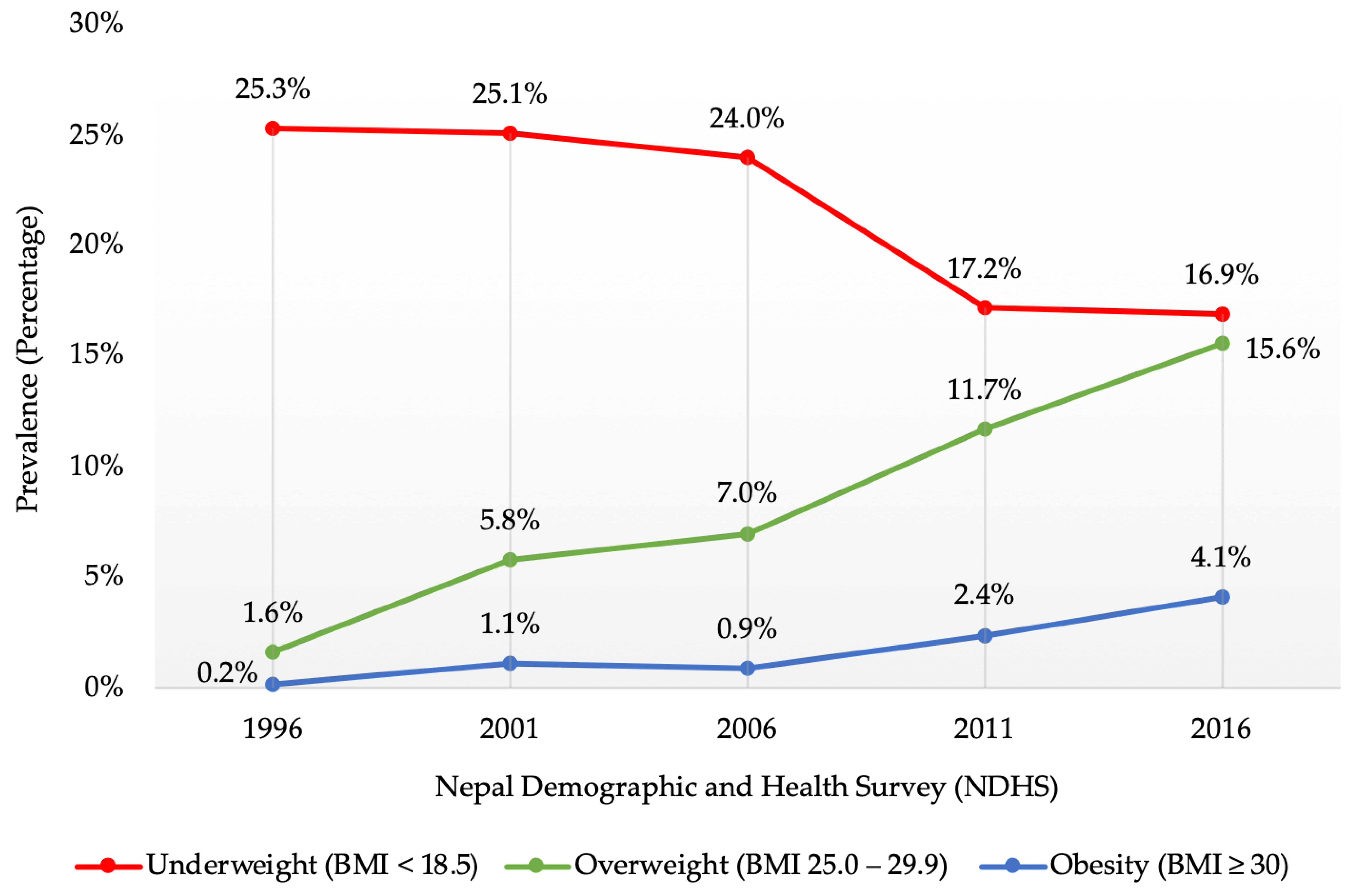
3.1. Time Trends of the Prevalence of Underweight from 1996 to 2016
3.2. Characteristics of NDHS 2016 Study Participants
3.3. Association of Sociodemographic and Household Environmental Factors with Underweight
4. Discussion
4.1. Summary of Key Findings
4.2. Time Trends of the Prevalence of Underweight
4.3. Sociodemographic Factors Associated with Underweight
4.4. Household Environmental Factors Associated with Underweight
4.5. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund (UNICEF); World Health Organization; International Bank for Reconstruction and Development/The World Bank. Levels and Trends in Child Malnutrition: Key Findings of the 2021 Edition of the Joint Child Malnutrition Estimates; World Health Organization: Geneva, Switzerland, 2021.
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Development Initiatives. 2020 Global Nutrition Report: Action on Equity to End Malnutrition; Development Initiatives: Bristol, UK, 2020. [Google Scholar]
- Müller, O.; Krawinkel, M. Malnutrition and health in developing countries. CMAJ 2005, 173, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Levinson, F.J.; Bassett, L. Malnutrition Is Still a Major Contributor to Child Deaths; Population Reference Bureau: Washington, DC, USA, 2007. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Ford, N.D.; Patel, S.A.; Narayan, K.M. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef]
- Ferdausi, F.; Al-Zubayer, M.A.; Keramat, S.A.; Ahammed, B. Prevalence and associated factors of underweight and overweight/obesity among reproductive-aged women: A pooled analysis of data from South Asian countries (Bangladesh, Maldives, Nepal and Pakistan). Diabetes Metab. Syndr. 2022, 16, 102428. [Google Scholar] [CrossRef]
- Rai, A.; Gurung, S.; Thapa, S.; Saville, N.M. Correlates and inequality of underweight and overweight among women of reproductive age: Evidence from the 2016 Nepal demographic health survey. PLoS ONE 2019, 14, e0216644. [Google Scholar] [CrossRef]
- Nubé, M.; Van Den Boom, G.J. Gender and adult undernutrition in developing countries. Ann. Hum. Biol. 2003, 30, 520–537. [Google Scholar] [CrossRef]
- Seferidi, P.; Hone, T.; Duran, A.C.; Bernabe-Ortiz, A.; Millett, C. Global inequalities in the double burden of malnutrition and associations with globalisation: A multilevel analysis of Demographic and Health Surveys from 55 low-income and middle-income countries, 1992–2018. Lancet Glob. Health 2022, 10, e482–e490. [Google Scholar] [CrossRef]
- Biswas, T.; Townsend, N.; Magalhaes, R.; Hasan, M.M.; Mamun, A.A. Geographical and socioeconomic inequalities in the double burden of malnutrition among women in Southeast Asia: A population-based study. Lancet Reg. Health Southeast Asia 2022, 1, 100007. [Google Scholar] [CrossRef]
- Morakinyo, O.M.; Adebowale, A.S.; Obembe, T.A.; Oloruntoba, E.O. Association between household environmental conditions and nutritional status of women of childbearing age in Nigeria. PLoS ONE 2020, 15, e0243356. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Mtumwa, A.H.; Paul, E.; Vuai, S.A.H. Determinants of undernutrition among women of reproductive age in Tanzania mainland. South Afr. J. Clin. Nutr. 2016, 29, 75–81. [Google Scholar] [CrossRef]
- Han, Z.; Mulla, S.; Beyene, J.; Liao, G.; McDonald, S.D. Maternal underweight and the risk of preterm birth and low birth weight: A systematic review and meta-analyses. Int. J. Epidemiol. 2011, 40, 65–101. [Google Scholar] [CrossRef] [PubMed]
- Al Kibria, G.M. Prevalence and factors affecting underweight, overweight and obesity using Asian and World Health Organization cutoffs among adults in Nepal: Analysis of the demographic and health survey 2016. Obes. Res. Clin. Pract. 2019, 13, 129–136. [Google Scholar] [CrossRef]
- Biswas, T.; Townsend, N.; Magalhaes, R.J.S.; Islam, M.S.; Hasan, M.M.; Mamun, A. Current progress and future directions in the double burden of malnutrition among women in South and Southeast Asian countries. Curr. Dev. Nutr. 2019, 3, nzz026. [Google Scholar] [CrossRef]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015.
- Ministry of Health Nepal; New ERA; ICF. Nepal Demographic and Health Survey 2016; MOH Nepal; New ERA; ICF: Kathmandu, Nepal, 2017.
- Schwinger, C.; Chandyo, R.K.; Ulak, M.; Hysing, M.; Shrestha, M.; Ranjitkar, S.; Strand, T.A. Prevalence of underweight, overweight, and obesity in adults in Bhaktapur, Nepal in 2015–2017. Front. Nutr. 2020, 7, 567164. [Google Scholar] [CrossRef]
- Rawal, L.B.; Kanda, K.; Mahumud, R.A.; Joshi, D.; Mehata, S.; Shrestha, N.; Poudel, P.; Karki, S.; Renzaho, A. Prevalence of underweight, overweight and obesity and their associated risk factors in Nepalese adults: Data from a nationwide survey, 2016. PLoS ONE 2018, 13, e0205912. [Google Scholar] [CrossRef]
- Haddad, L.; Cameron, L.; Barnett, I. The double burden of malnutrition in SE Asia and the Pacific: Priorities, policies and politics. Health Policy Plan 2015, 30, 1193–1206. [Google Scholar] [CrossRef]
- Rana, K.; Ghimire, P.; Chimoriya, R.; Chimoriya, R. Trends in the Prevalence of overweight and obesity and associated socioeconomic and household environmental factors among women in Nepal: Findings from the Nepal demographic and health surveys. Obesities 2021, 1, 113–135. [Google Scholar] [CrossRef]
- Jones-Smith, J.C.; Gordon-Larsen, P.; Siddiqi, A.; Popkin, B.M. Is the burden of overweight shifting to the poor across the globe? Time trends among women in 39 low- and middle-income countries (1991–2008). Int. J. Obes. 2012, 36, 1114–1120. [Google Scholar] [CrossRef] [Green Version]
- Rana, K.; Shrestha, V.; Chimoriya, R. The effect of housing on health and challenges of demographic changes. Glob. J. Sci. Front. Res. 2020, 20, 75–82. [Google Scholar]
- Shrestha, N.; Mishra, S.R.; Ghimire, S.; Gyawali, B.; Pradhan, P.M.S.; Schwarz, D. Application of single-level and multi-level modeling approach to examine geographic and socioeconomic variation in underweight, overweight and obesity in Nepal: Findings from NDHS 2016. Sci. Rep. 2020, 10, 2406. [Google Scholar] [CrossRef] [PubMed]
- Das Gupta, R.; Haider, S.S.; Hashan, M.R.; Hasan, M.; Sutradhar, I.; Sajal, I.H.; Joshi, H.; Haider, M.R.; Sarker, M. Association between the frequency of television watching and overweight and obesity among women of reproductive age in Nepal: Analysis of data from the Nepal Demographic and Health Survey 2016. PLoS One 2020, 15, e0228862. [Google Scholar] [CrossRef] [PubMed]
- DHS Program. The Demographic and Health Surveys (DHS) Program. Available online: https://dhsprogram.com/data/available-datasets.cfm (accessed on 17 June 2022).
- DHS Program. Demographic and Health Survey (DHS). Available online: https://dhsprogram.com/Methodology/Survey-Types/DHS.cfm (accessed on 10 June 2022).
- DHS Program. Team and Partners. Available online: https://dhsprogram.com/Who-We-Are/About-Us.cfm (accessed on 11 June 2022).
- Ministry of Health and Population Nepal; New ERA; ICF International. Nepal Demographic and Health Survey 2011; MOHP Nepal; New ERA; ICF International: Kathmandu, Nepal, 2012.
- Ministry of Health and Population Nepal; New ERA; Macro International. Nepal Demographic and Health Survey 2006; MOHP Nepal; New ERA; Macro International: Kathmandu, Nepal, 2007.
- Ministry of Health Nepal; New ERA; ORC Macro. Nepal Demographic and Health Survey 2001; MOH Nepal; New ERA; ORC Macro: Calverton, MD, USA, 2002.
- Pradhan, A.; Aryal, R.H.; Regmi, G.; Ban, B.; Govindasamy, P. Nepal Family Health Survey 1996; MOH Nepal; New ERA; Macro International: Kathmandu, Nepal, 1997.
- World Health Organization. Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied logistic regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Dewan, M. Malnutrition in women. Stud. Home Comm. Sci. 2008, 2, 7–10. [Google Scholar] [CrossRef]
- Biswas, T.; Magalhaes, R.J.S.; Townsend, N.; Das, S.K.; Mamun, A. Double burden of underweight and overweight among women in South and Southeast Asia: A systematic review and meta-analysis. Adv. Nutr. 2020, 11, 128–143. [Google Scholar] [CrossRef]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2022; FAO: Rome, Italy, 2022. [Google Scholar]
- Bhandari, S.; Sayami, J.T.; Thapa, P.; Sayami, M.; Kandel, B.P.; Banjara, M.R. Dietary intake patterns and nutritional status of women of reproductive age in Nepal: Findings from a health survey. Arch. Public Health 2016, 74, 2. [Google Scholar] [CrossRef]
- Kamal, S.M.; Hassan, C.H.; Alam, G.M. Dual burden of underweight and overweight among women in Bangladesh: Patterns, prevalence, and sociodemographic correlates. J. Health Popul. Nutr. 2015, 33, 92–105. [Google Scholar]
- Kominiarek, M.A.; Peaceman, A.M. Gestational weight gain. Am. J. Obstet. Gynecol. 2017, 217, 642–651. [Google Scholar] [CrossRef]
- Marston, C.; Arjyal, A.; Maskey, S.; Regmi, S.; Baral, S. Using qualitative evaluation components to help understand context: Case study of a family planning intervention with female community health volunteers (FCHVs) in Nepal. BMC Health Serv. Res. 2020, 20, 685. [Google Scholar] [CrossRef]
- Khanam, M.; Osuagwu, U.L.; Sanin, K.I.; Haque, M.A.; Rita, R.S.; Agho, K.E.; Ahmed, T. Underweight, overweight and obesity among reproductive bangladeshi women: A nationwide survey. Nutrients 2021, 13, 4408. [Google Scholar] [CrossRef] [PubMed]
- Tanwi, T.S.; Chakrabarty, S.; Hasanuzzaman, S.; Saltmarsh, S.; Winn, S. Socioeconomic correlates of overweight and obesity among ever-married urban women in Bangladesh. BMC Public Health 2019, 19, 842. [Google Scholar] [CrossRef] [PubMed]
- Bharmal, N.H.; McCarthy, W.J.; Gadgil, M.D.; Kandula, N.R.; Kanaya, A.M. The association of religious affiliation with overweight/obesity among South Asians: The mediators of atherosclerosis in South Asians living in America (MASALA) study. J. Relig. Health 2018, 57, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.M.; Chan, C.K.; Reidpath, D.D. Religiosity and spirituality and the intake of fruit, vegetable, and fat: A systematic review. Evid. Based Complement Alternat. Med. 2013, 2013, 146214. [Google Scholar] [CrossRef] [PubMed]
- Van Minh, H.; Nguyen-Viet, H. Economic aspects of sanitation in developing countries. Environ. Health Insights 2011, 5, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Thapa, R.; Bam, K.; Tiwari, P.; Sinha, T.K.; Dahal, S. Implementing federalism in the health system of Nepal: Opportunities and challenges. Int. J. Health Policy Manag. 2019, 8, 195–198. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Total Sample (n = 6165) | Underweight (BMI < 18.5) | ||
|---|---|---|---|---|
| n (%) or Mean ± SD | COR | 95%CI | p-Value | |
| Weight (kg) | 50.7 ± 9.6 | |||
| Height (cm) | 151.7 ± 5.6 | |||
| BMI (kg/m2) | 22.0 ± 3.9 | |||
| Sociodemographic factors | ||||
| Individual-level factors | ||||
| Age (years) | ||||
| 15–24 | 2331 (37.8%) | ref | ||
| 25–34 | 1834 (29.7%) | 0.46 | 0.39–0.54 | <0.001 |
| 35–49 | 2000 (32.4%) | 0.44 | 0.38–0.52 | <0.001 |
| Educational status | ||||
| No formal education | 2126 (34.5%) | ref | ||
| Primary | 965 (15.7%) | 0.79 | 0.64–0.98 | 0.030 |
| Secondary | 2223 (36.1%) | 0.99 | 0.85–1.15 | 0.860 |
| Higher | 851 (13.8%) | 0.69 | 0.55–0.87 | 0.001 |
| Employment status | ||||
| Not currently employed | 2498 (40.5%) | ref | ||
| Currently employed | 3667 (59.5%) | 0.77 | 0.68–0.88 | <0.001 |
| Family-level factors | ||||
| Marital status | ||||
| Never married | 1323 (21.5%) | ref | ||
| Married/living with a partner | 4671 (75.7%) | 0.44 | 0.38–0.51 | <0.001 |
| Widowed/divorced/separated | 171 (2.8%) | 0.33 | 0.20–0.55 | <0.001 |
| Number of household members | ||||
| ≤ 5 | 3763 (61.0%) | ref | ||
| > 5 | 2402 (39.0%) | 1.38 | 1.21–1.59 | <0.001 |
| Wealth index* | ||||
| Poorest | 1310 (21.2%) | ref | ||
| Poorer | 1250 (20.3%) | 1.08 | 0.88–1.31 | 0.466 |
| Middle | 1251 (20.3%) | 1.08 | 0.88–1.31 | 0.472 |
| Richer | 1276 (20.7%) | 0.84 | 0.68–1.03 | 0.086 |
| Richest | 1078 (17.5%) | 0.43 | 0.34–0.56 | <0.001 |
| Religion | ||||
| Hindu | 5369 (87.1%) | ref | ||
| Buddhist | 296 (4.8%) | 0.45 | 0.30–0.68 | <0.001 |
| Muslim | 267 (4.3%) | 1.86 | 1.41–2.45 | <0.001 |
| Other | 233 (3.8%) | 0.51 | 0.32–0.79 | 0.003 |
| Household environmental factors | ||||
| Environmental factors | ||||
| Place of residence | ||||
| Urban | 3984 (64.6%) | ref | ||
| Rural | 2181 (35.4%) | 1.20 | 1.05–1.38 | 0.008 |
| Province of residence | ||||
| Province 1 | 878 (14.2%) | ref | ||
| Province 2 | 984 (16.0%) | 2.61 | 2.05–3.34 | <0.001 |
| Province 3 | 822 (13.3%) | 0.84 | 0.62–1.13 | 0.242 |
| Province 4 | 783 (12.7%) | 0.64 | 0.47–0.89 | 0.007 |
| Province 5 | 962 (15.6%) | 1.61 | 1.24–2.08 | <0.001 |
| Province 6 | 862 (14.0%) | 1.32 | 1.01–1.73 | 0.045 |
| Province 7 | 874 (14.2%) | 1.95 | 1.51–2.52 | <0.001 |
| Ecological zone | ||||
| Mountain | 441 (7.2%) | ref | ||
| Hill | 2823 (45.7%) | 0.90 | 0.67–1.20 | 0.458 |
| Terai | 2901 (47.1%) | 1.60 | 1.21–2.12 | 0.001 |
| Household facilities | ||||
| Source of drinking water | ||||
| Unimproved | 344 (5.6%) | ref | ||
| Improved | 5549 (90%) | 1.03 | 0.77–1.37 | 0.866 |
| Type of toilet facility | ||||
| Unimproved | 747 (12.1%) | ref | ||
| Improved | 5146 (83.5%) | 0.44 | 0.37–0.52 | <0.001 |
| Cooking fuel | ||||
| Solid fuel | 4201 (68.1%) | ref | ||
| Clean fuel | 1690 (27.4%) | 0.48 | 0.40–0.57 | <0.001 |
| Access to electricity | ||||
| No | 592 (9.6%) | ref | ||
| Yes | 5301 (86.0%) | 0.62 | 0.50–0.75 | <0.001 |
| Housing characteristics | ||||
| Main floor material | ||||
| Unimproved | 3815 (61.9%) | ref | ||
| Improved | 2078 (33.7%) | 0.53 | 0.45–0.62 | <0.001 |
| Main wall material | ||||
| Unimproved | 3255 (52.8%) | ref | ||
| Improved | 2638 (42.8%) | 0.70 | 0.61–0.80 | <0.001 |
| Main roof material | ||||
| Unimproved | 635 (10.3%) | ref | ||
| Improved | 5258 (85.3%) | 0.88 | 0.71–1.09 | 0.232 |
| Household possessions | ||||
| Refrigerator | ||||
| No | 5013 (81.3%) | ref | ||
| Yes | 880 (14.3%) | 0.47 | 0.37–0.59 | <0.001 |
| Television | ||||
| No | 2793 (45.3%) | ref | ||
| Yes | 3100 (50.3%) | 0.57 | 0.50–0.66 | <0.001 |
| Mobile phone | ||||
| No | 1747 (28.3%) | ref | ||
| Yes | 4418 (71.7%) | 0.46 | 0.41–0.53 | <0.001 |
| Bicycle | ||||
| No | 3522 (57.1%) | ref | ||
| Yes | 2371 (38.5%) | 1.45 | 1.26–1.66 | <0.001 |
| Motorised vehicle | ||||
| No | 4782 (77.6%) | ref | ||
| Yes | 1111 (18.0%) | 0.75 | 0.62–0.90 | 0.002 |
| Variable | Underweight (BMI < 18.5) | ||
|---|---|---|---|
| AOR | 95%CI | p-Value | |
| Sociodemographic factors | |||
| Individual-level factors | |||
| Age (years) | |||
| 15–24 | ref | ||
| 25–34 | 0.57 | 0.46–0.71 | <0.001 |
| 35–49 | 0.47 | 0.37–0.60 | <0.001 |
| Educational status | |||
| No formal education | ref | ||
| Primary | 0.76 | 0.60–0.97 | 0.027 |
| Secondary | 0.73 | 0.58–0.93 | 0.010 |
| Higher | 0.77 | 0.56–1.05 | 0.099 |
| Family-level factors | |||
| Marital status | |||
| Never married | ref | ||
| Married/living with a partner | 0.54 | 0.44–0.67 | <0.001 |
| Widowed/divorced/separated | 0.45 | 0.26–0.78 | 0.005 |
| Wealth index* | |||
| Poorest | ref | ||
| Poorer | 0.99 | 0.79–1.23 | 0.894 |
| Middle | 0.76 | 0.58–0.99 | 0.040 |
| Richer | 0.75 | 0.56–1.01 | 0.055 |
| Richest | 0.50 | 0.35–0.71 | <0.001 |
| Religion | |||
| Hindu | ref | ||
| Buddhist | 0.56 | 0.36–0.87 | 0.011 |
| Muslim | 1.08 | 0.78–1.48 | 0.655 |
| Other | 0.56 | 0.35–0.90 | 0.016 |
| Household environmental factors | |||
| Environmental factors | |||
| Province of residence | |||
| Province 1 | ref | ||
| Province 2 | 2.04 | 1.54–2.70 | <0.001 |
| Province 3 | 1.08 | 0.77–1.51 | 0.671 |
| Province 4 | 0.82 | 0.58–1.17 | 0.266 |
| Province 5 | 1.41 | 1.07–1.86 | 0.016 |
| Province 6 | 1.30 | 0.95–1.79 | 0.102 |
| Province 7 | 1.67 | 1.27–2.21 | <0.001 |
| Ecological zone | |||
| Mountain | ref | ||
| Hill | 1.24 | 0.91–1.69 | 0.176 |
| Terai | 1.67 | 1.18–2.36 | 0.004 |
| Household facilities | |||
| Type of toilet facility | |||
| Unimproved | ref | ||
| Improved | 0.70 | 0.56–0.86 | <0.001 |
| Household possessions | |||
| Television | |||
| No | ref | ||
| Yes | 0.81 | 0.67–0.98 | 0.030 |
| Mobile phone | |||
| No | ref | ||
| Yes | 0.63 | 0.54–0.74 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, K.; Chimoriya, R.; Haque, N.B.; Piya, M.K.; Chimoriya, R.; Ekholuenetale, M.; Arora, A. Prevalence and Correlates of Underweight among Women of Reproductive Age in Nepal: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 11737. https://doi.org/10.3390/ijerph191811737
Rana K, Chimoriya R, Haque NB, Piya MK, Chimoriya R, Ekholuenetale M, Arora A. Prevalence and Correlates of Underweight among Women of Reproductive Age in Nepal: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11737. https://doi.org/10.3390/ijerph191811737
Chicago/Turabian StyleRana, Kritika, Ritesh Chimoriya, Nabila Binte Haque, Milan K. Piya, Romila Chimoriya, Michael Ekholuenetale, and Amit Arora. 2022. "Prevalence and Correlates of Underweight among Women of Reproductive Age in Nepal: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 18: 11737. https://doi.org/10.3390/ijerph191811737
APA StyleRana, K., Chimoriya, R., Haque, N. B., Piya, M. K., Chimoriya, R., Ekholuenetale, M., & Arora, A. (2022). Prevalence and Correlates of Underweight among Women of Reproductive Age in Nepal: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(18), 11737. https://doi.org/10.3390/ijerph191811737