
An International Systematic Review of Prevalence, Risk, and Protective Factors Associated with Young People’s E-Cigarette Use


Abstract
1. Introduction
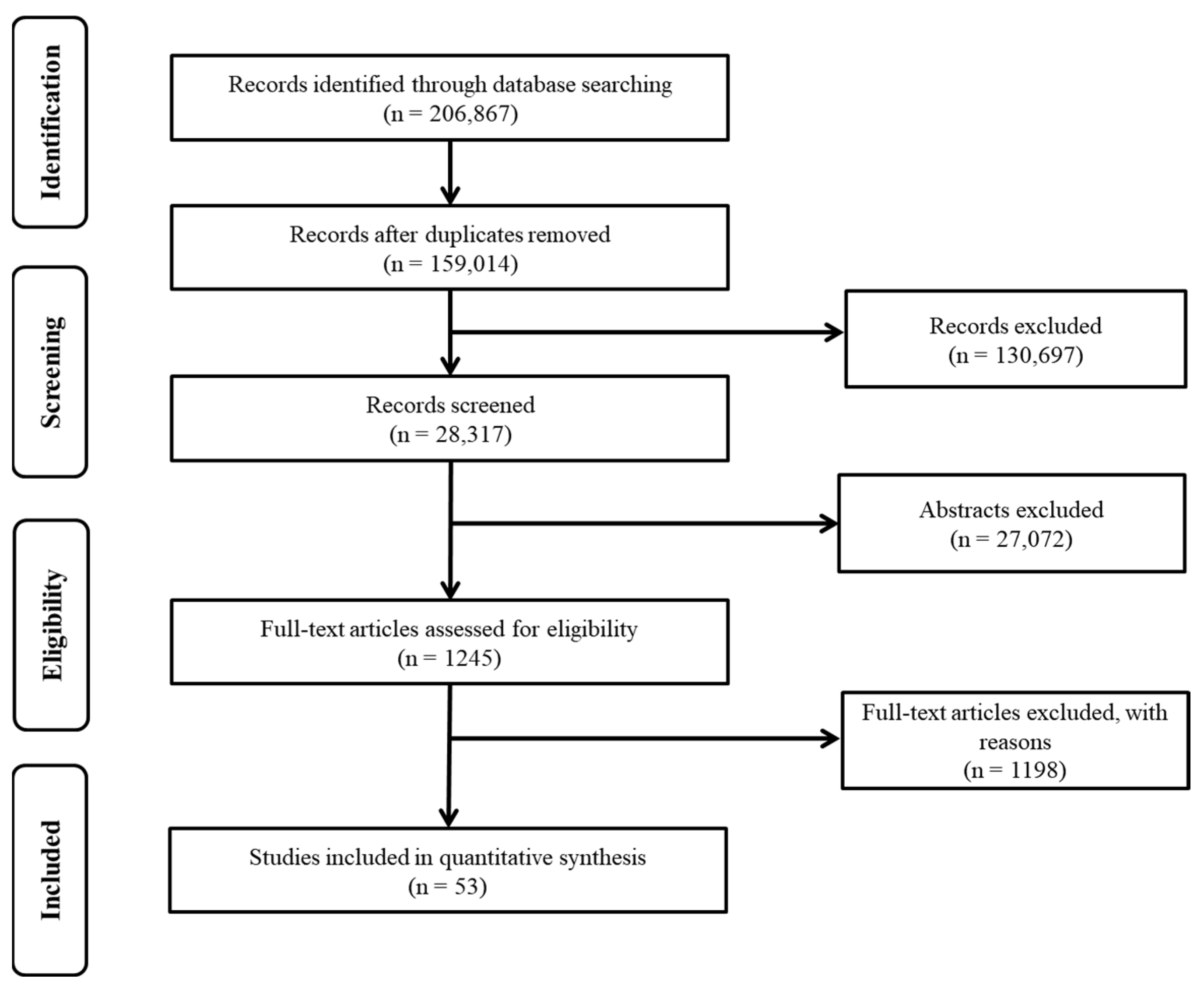
2. Methods
2.1. Study Identification
2.2. Selection Procedure
2.3. Coding and Analysis
3. Results
3.1. General Characteristics
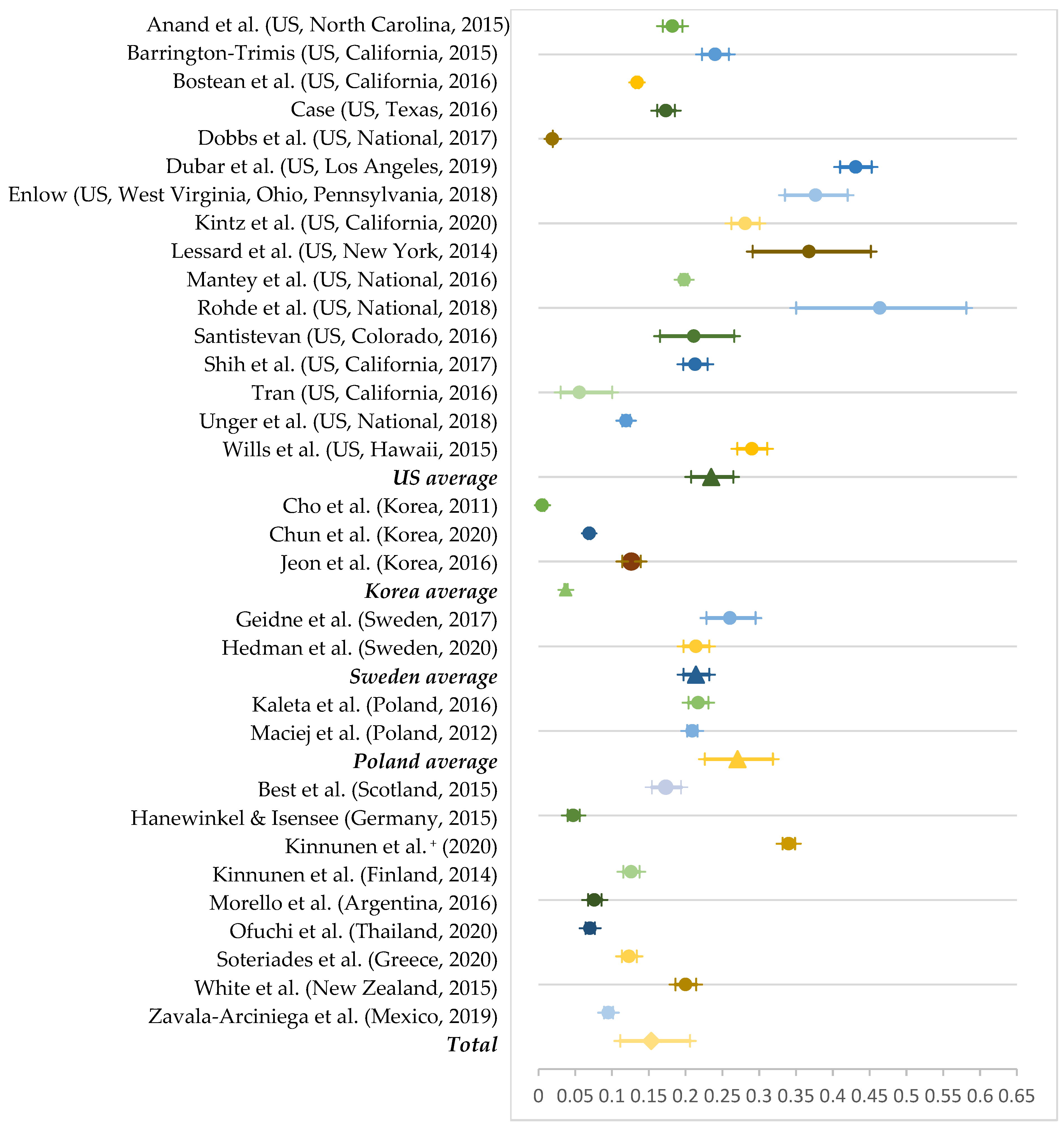
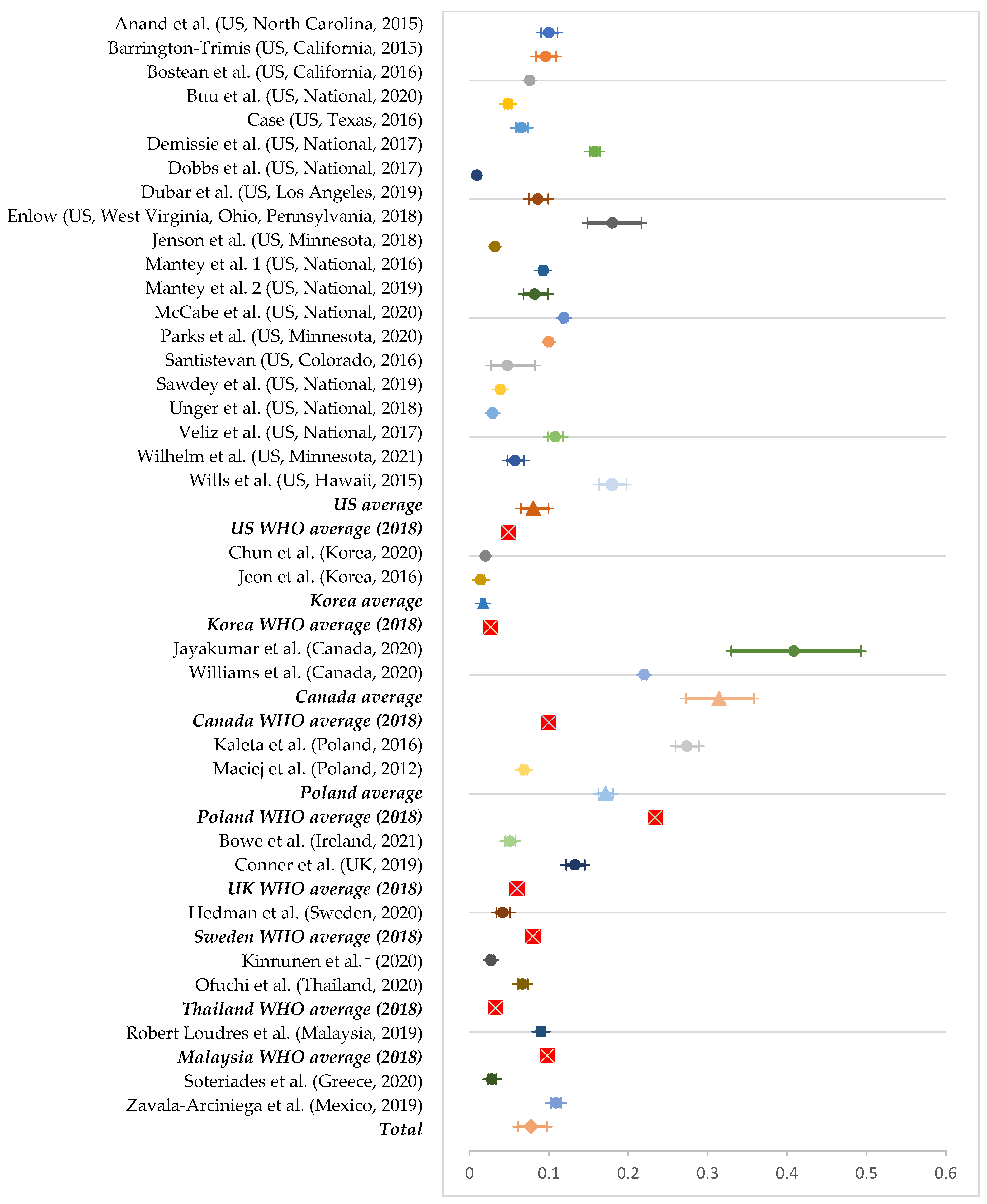
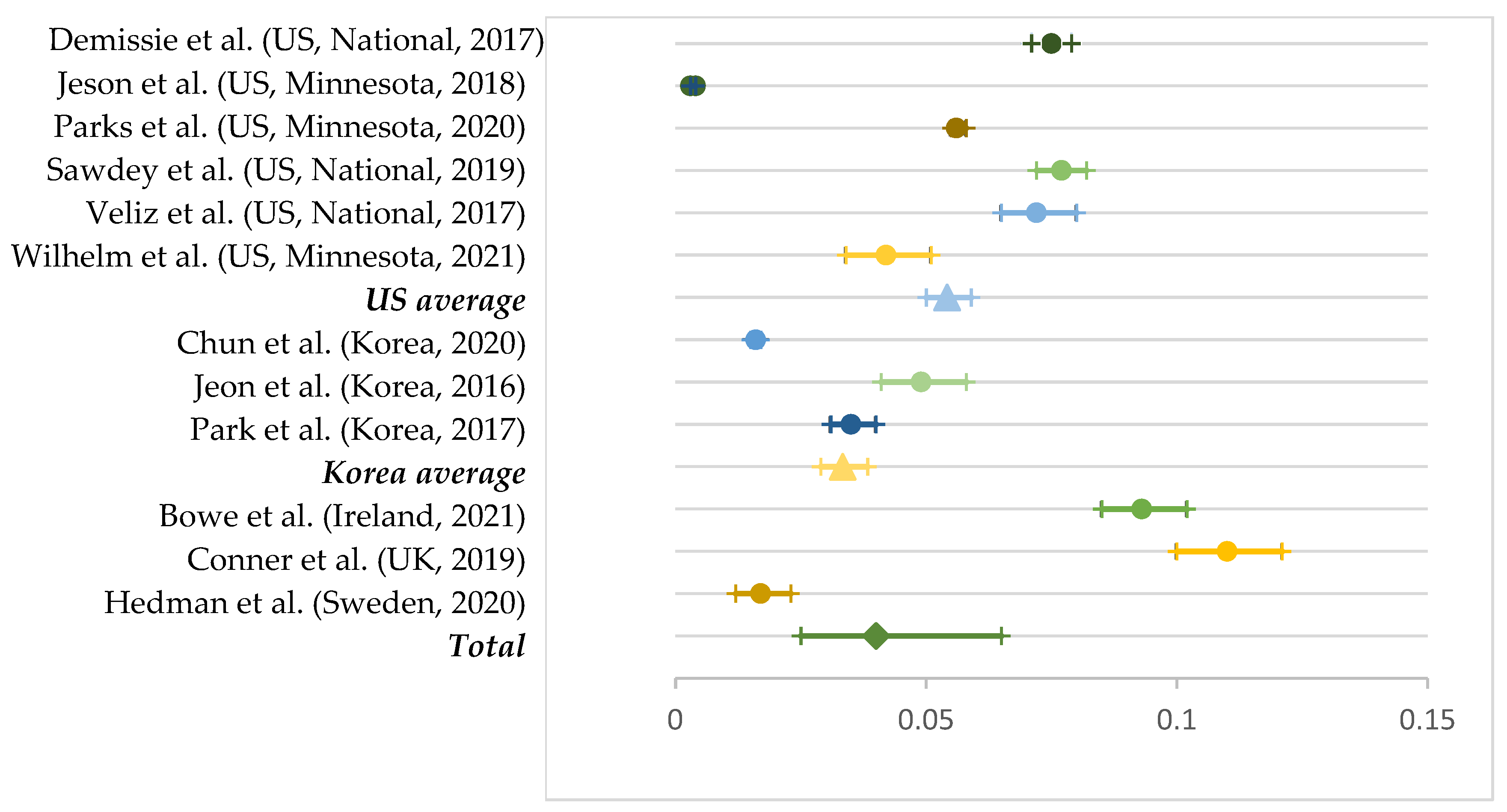
3.2. Prevalence



3.3. Sample Characteristics
3.4. Gender Differences
3.5. Protective Factors
3.6. Risk Factors

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Country) | Prevalence | Sample Size (Age) | Gender Difference | Protective Factors (β/OR) | Risk Factors (β/OR) |
|---|---|---|---|---|---|
| Anand et al. (2015) [40] (US) | Lifetime, 18.2%; Current, 10% | 3298 (9–12th grades) | Significant difference | Being female (0.59), plan to graduate high school (0.17), mother living in the household (0.55), mother never smoked tobacco (0.50), father never smoked tobacco (0.57), not knowing anyone who uses e-cigarettes (0.25) | Father’s use of snuff (3.82), mother’s use of e-cigarettes (2.60), cigarette use (8.79), smokeless tobacco use (3.75) |
| Barrington-Trimis et al. (2015) [41] (US) | Lifetime, 24%; Current, 9.6% | 2084 (11–12th grades) | Different but not statistically significant | N/A | Anyone living at home using e-cigarettes (6.80) and cigarettes (2.79), number of friends who use e-cigarettes (18.7) and cigarettes (7.46), best friends’ positive reactions to e-cigarette use (18.6), perception of the harm of e-cigarettes and cigarettes (6.02) |
| Best et al. (2015) [42] (Scotland) | Lifetime, 17.3% | 1404 (Pupils in secondary 2 and 4) | N/A | Having never smoked (0.10) | Recognizing more cigarette brands (1.20), having a best friend who smoked (3.17) |
| Bostean et al. (2016) [43] (US) | Lifetime, 13.4%; Current, 7.6% | 67,701 (7, 9, 11th grades) | Significant difference | Being female (0.84) | Parents’ education levels (1.44), having ever used tobacco (6.84), having ever used alcohol (5.83), having ever used marijuana (8.15), race (Hispanic; 1.54), presence of a retailer near schools (1.70), attending schools with a high percentage of students eligible for free and reduced lunch program (2.94) |
| Bowe et al. (2021) [27] (Ireland) | Current, 5.1%; Dual, 9.3% | 4490 (15–16 years old) | Significant difference | Parental supervision (0.71), valuing conventional social norms (0.68) | Parent smokes (1.71), feeling the need to smoke to fit in with peers (2.13), few friends who smoke (2.15), most/almost all friends who smoke (5.19), self-reported academic achievement average (1.43) and below average (2.53), parental reaction to cigarette use (do not care) (4.65) |
| Buu et al. (2020) [44] (US) | Current, 4.86% | 9258 (12–17 years old) | Significant difference | Being non-Hispanic and Black (0.38) | Higher levels of internalizing (1.29) and externalizing problems (1.42), receiving more money per week (1.12), being older (1.72) |
| Carey et al. (2019) [45] (US) | N/A | 3907 (6, 8, 10th grades) | N/A | Positive affect (0.61), belief that e-cigarettes are harmful to health (0.69) | E-cigarette use among family members (4.72), alcohol and marijuana use (3.92), poor school performance (12.98), sensation seeking (1.45), social norm (okay to use, common to use) (6.69) |
| Case (2016) [46] (US) | Lifetime, 17.3%; Current, 6.55% | 3769 (6, 8, 10th grades) | No difference | N/A | Sensation seeking (1.32) |
| Case et al. (2020) [47] (US) | N/A | 2272 (14–18 years old) | N/A | N/A | Higher recall ENDS marketing (1.64), peer tobacco use (3.06), alcohol use (2.67), having ever used marijuana with JUUL (10.08) and with other ENDS (12.07) |
| Cho et al. (2011) [9] (Korea) | Lifetime, 0.5% | 4341 (Middle and high school students) | Significant difference | N/A | Propensity to be easily affected by friends (3.9), having ever smoked a cigarette (11.2) |
| Chun et al. (2020) [48] (Korea) | Lifetime, 6.9%; Current, 2%; Dual, 1.6% | 62,276 (13–18 years old) | Significant difference | Being a vocational school student (0.66) | Tobacco accessibility (1.3), secondhand smoke exposure at home (1.09), sexual intercourse (1.25), being a middle school student (2.13) |
| Conner et al. (2019) [30] (UK) | Current, 13.3%; Dual, 11% | 3210 (13–14 years old) | Significant difference | N/A | Higher impulsivity (1.26), friends and family smoking (1.48), being male (1.64) |
| Demissie et al. (2017) [49] (US) | Current, 15.8%; Dual, 7.5% | 15,624 (9–12th grades) | Significant difference | Engaging in daily physical activity (0.91) | Engaging in a physical fight (1.72), lifetime suicide attempt (1.86), texting or emailing while driving (1.39), drinking alcohol (2.62), using marijuana (3.70), using other illicit drugs (2.73), using nonmedical drugs (2.30), having multiple sexual partners (2.35), being sexually active (1.86), drinking more soda (1.35) |
| Dobbs et al. (2017) [50] (US) | Lifetime, 19.4%; Current, 9.2% | 27,294 (9–19 years old) | N/A | N/A | Perceived e-cigarette as less harm (2.40), perceived less addictiveness of e-cigarettes (2.11), smoking history (7.84), living with a smoker (1.44), being older (1.85), being Hispanic (1.33) |
| Dubar et al. (2019) [51] (US) | Lifetime, 43.11%; Current, 8.62% | 2039 (16–20 years old) | N/A | N/A | Cigarette use (0.17), marijuana use (0.03) |
| Enlow (2018) [52] (US) | Lifetime, 37.7%; Current, 18% | 494 (13–18 years old) | N/A | Perceived costs of vaping (0.52), greater self-efficacy (0.22) | Cigarette use (2.86), alcohol use (2.67), marijuana use (2.23), more modeling of smoking in their social network (1.34), higher extraversion (2.20) |
| Etim et al. (2020) [53] (US) | N/A | 1060 (15–20 years old) | N/A | N/A | Peer e-cigarette use (2.01), exposure to e-cigarette commercials (1.27), household smoking (4.70) |
| Geidne et al. (2017) [5] (Sweden) | Lifetime, 26% | 665 (15–16 years old) | No difference | N/A | Smoking conventional cigarettes (5.6), snus use (2.2), alcohol use (4.4), water pipe use (3.2) |
| Hanewinkel & Isensee (2015) [4] (Germany) | Lifetime, 4.7% | 2693 (5–10th grades) | No difference | N/A | Higher sensation seeking (2.24), having friends (2.06) and parents (1.89) who smoke cigarettes |
| Hedman et al. (2020) [54] (Sweden) | Lifetime, 21.4%; Current, 4.2%; Dual, 1.7% | 2185 (14–15 years old, 19 years old) | Significant difference | Eating a healthy diet (0.74) | Daily smoking (6.27), participation in an arts vocational program (2.22) |
| Jayakumar et al. (2020) [55] (Canada) | Current, 41% | 137 (16–25 years old) | No difference | Perceiving moderate or great risk of regularly vaping without nicotine (0.34) | Current alcohol use (2.66), current cannabis use (13.78), having friends who used cannabis (3.80), using e-cigarettes (2.34), having friends who smoke (2.23), seeing anyone use an e-cigarette in the past seven days (5.97), currently not using cannabis (3.80) |
| Jeon et al. (2016) [56] (Korea) | Lifetime, 12.6%; Current, 1.4%; Dual, 4.9% | 2744 (13–18 years old) | Significant difference | N/A | Close friends smoking (8.58), sibling smoking (3.25), teacher smoking (1.38) |
| Jenson et al. (2018) [23] (US) | Current, 6.4%; Dual, 3.2% | 126,868 (8, 9, 11th grades) | No difference | N/A | Ethnicity (American Indian students) (3.57), sexual identity (bisexual students) (4.40), economic status (students receiving free/reduced lunch) (1.92), alcohol use (9.79), decreasing academic performance (2.47) |
| Kaleta et al. (2016) [57] (Poland) | Lifetime, 21.7%; Current, 27.4% | 3552 (13–19 years old) | Significant difference | Higher mother’s education level (0.50), higher father’s education level (0.60), perceiving e-cigarettes as more harmful (0.30) | Father’s education level - medium (1.5), alcohol use (4.3–5.3), ever having smoked tobacco (6.7–7.5), being a current tobacco smoker (9.8–32.5), parental smoking (1.4), some friends smoking (1.4–1.5) and most friends smoking (2.3), a perception that tobacco smoking is harmful to health (1.9–3.2), perceiving e-cigarettes as less harmful (1.8–2.1) |
| Kinnunen et al. (2014) [58] (Finland) | Lifetime, 12.6% | 3535 (12–18 years old) | Different but not statistically significant | N/A | Cigarette experimenter (8.09) and daily smoker (41.35), ever having used snus (2.96), ever having used waterpipe (2.21), vocational upper secondary school students (2.06), school performance slightly or much poorer (1.92) |
| Kinnunen et al. (2020) [59] (Belgium, Finland, Germany, Ireland, Italy, The Netherlands, Portugal) | Lifetime, 34%; Current, 2.7% | 12,167 (14–17 years old) | Significant difference | Being older (0.77) | Parental smoking (1.28), low academic achievement (1.79), some peers smoking (2.33), most or all peers smoking (4.62) |
| Kintz et al. (2020) [60] (US) | Lifetime, 28.1% | 2097 (11–12th grades) | No difference | N/A | Cigarette (3.46), hookah (5.85), and cigar (4.25) use |
| Kwon et al. (2018) [1] (US) | N/A | 9853 (12–17 years old) | No difference | Perceptions of e-cigarettes as addictive (0.62) and harmful (0.40) | Internalizing problems (2.53), externalizing problems (3.47), being a rule breaker (8.43), liking frightening things (3.44), preferring unpredictable friends (4.72), having ever used alcohol (3.03) or marijuana (3.42) or other substances (1.98), household secondhand smoke exposure (1.48) |
| Lessard et al. (2014) [61] (US) | Lifetime, 36.9% | 136 (Middle to late adolescence) | No difference | Parental monitoring (0.85) | Current cigarette use (3.88), current marijuana use (4.07), current alcohol use (7.72), peer substance use (1.34) |
| Maciej et al. (2012) [11] (Poland) | Lifetime, 20.9%; Current,6.9% | 13.787 (15–24 years old) | Significant difference | N/A | Being male (9.0), being older (5.9), living in urban areas (8.5), ever smoked a cigarette (9.7), current cigarette smoking (15.3), parents smoking (10.0), partner smoking (15.6) |
| Mantey et al. (2016) [62] (US) | Lifetime, 19.8%; Current, 9.3% | 22,007 (Middle and high school students) | Significant difference | Being female (0.81) | Exposure to pro e-cigarette marketing sources (1.22), being older (2.37), other tobacco use (15.66) |
| Mantey et al. (2019) [63] (US) | Current, 8.24% | 1217 (9–12th grade) | Significant difference | N/A | Retail access to e-cigarettes (2.11–5.81) |
| McCabe et al. (2020) [28] (US) | Current, 11.9% | 38,926 (8, 10, 12th grades) | Significant difference | N/A | Being male (1.59), average grades (1.44), binge drinking (2.46), cigarette use (4.83), marijuana use (3.08), nonmedical drug use (1.63), attending schools with a higher prevalence of smoking (1.35) |
| Morello et al. (2016) [64] (Argentina) | Lifetime, 7.6% | 3172 (Secondary school students) | No difference | Attending a public school (0.40) | Higher sensation seeking (1.49), being a current smoker (2.58), having friends who smoke cigarettes (1.93), exposure to ads for tobacco products online (1.87) |
| Ofuchi et al. (2020) [65] (Thailand) | Current, 6.7%;Lifetime, 7% | 6167 (13–18 years old) | Different but not statistically | N/A | Emotional abuse (1.4), physical abuse (1.4), sexual abuse (1.5), parental separation or divorce (1.36), child violence (1.8), ever having had an incarcerated household member (1.98), history of adverse childhood experience (1.5) |
| Park et al. (2017) [8] (Korea) | Dual, 3.5% | 6307 (7–12th grades) | Significant difference | N/A | Being male (2.11), earning higher grades (3.10), higher weekly allowance (1.56), residence in urban areas (1.20), friend’s smoking (2.50), daily smoking (2.11), number of cigarettes (1.52), quitting attempts (1.52), risky drinking (1.14), lifetime drug use (1.45), lifetime sexual intercourse (1.12) |
| Parks et al. (2020) [66] (US) | Current, 9.99%; Dual, 5.63% | 111,091 (5, 8, 9, 11th grades) | N/A | Internal assets (0.63), strong anti-smoking norms (0.88), positive teacher engagement (0.76) | Parental incarceration (0.43) |
| Robert Loudres et al. (2019) [29] (Malaysia) | Current, 9% | 13,162 (10–19 years old) | Significant difference | N/A | Being male (4.08), age (2.64), ethnicity (2.25), cigarette smoking (13.16) |
| Rohde et al. (2018) [19] (US) | Lifetime, 47% | 69 (14–18 years old) | Different but not statistically | Mother’s education level (0.24), addiction risk beliefs about e-cigarettes (0.46) | Combustible cigarette use (4.90) |
| Santistevan (2016) [67] (US) | Lifetime, 21%; Current, 4.8% | 251 (13–19 years old) | N/A | N/A | Awareness of e-cigarettes through social media (15.68), shared information with peers (52.10) |
| Sawdey et al. (2019) [68] (US) | Current, 3.9%; Dual, 7.7% | 12,460 (12–17 years old) | N/A | N/A | Low academic achievement (1.3), other tobacco use (3.7), marijuana and alcohol use (2.6), high internalizing problems (1.5), high externalizing problems (2.0), high sensation seeking (1.9), household tobacco use (1.4) |
| Shih et al. (2017) [69] (US) | Past year, 21.3% | 2359 (High school students and college freshmen) | N/A | Neighborhood cohesion (0.83) | Neighborhood problems with alcohol and drugs (1.25), neighborhood disorganization (1.59) |
| Soteriades et al. (2020) [70] (Greece) | Lifetime, 12.3%; Current, 2.8% | 4096 (13–15 years old) | Significant difference | N/A | Use of any combustible tobacco products (7.85), e-cigarette use by other family members (5.72), being older (2.87) |
| Tran (2016) [71] (US) | Lifetime, 5.6% | 180 (6–9th grades) | N/A | N/A | Previous cigarette smoking experience (0.054), perception of benefits of cigarette smoking (1.14) |
| Trucco et al. (2021) [72] (US) | N/A | 176 (14–17 years old) | N/A | N/A | Perceptions of e-cigarettes as being cool (0.28) |
| Unger et al. (2018) [73] (US) | Lifetime, 11.9%; Current, 2.9% | 13,651 (12–17 years old) | N/A | N/A | Exposure to tobacco websites (3.0-3.2) |
| Veliz et al. (2017) [74] (US) | Current, 10.8%; Dual, 7.2% | 4450 (12th grade) | N/A | Participation in at least one competitive sport (6.2), or three or more sports (6.4), participation in soccer (0.37) | Participation in wrestling (2.14), participation in baseball/softball (1.36) |
| Vogel et al. (2018) [75] (US) | N/A | 173 (13–18 years old) | N/A | N/A | Percentage of friends who use e-cigarettes (0.22), past month cigarette use (0.19) |
| White et al. (2015) [76] (New Zealand) | Lifetime, 20% | 3127 (14–15 years old) | Significant difference | N/A | Higher weekly income/allowances (2.03), current smoking (4.56), having close friends who smoke cigarettes (2.11), having used other tobacco products (2.71), having ever used marijuana (2.24), having ever engaged in binge drinking (1.87) |
| Wilhelm et al. (2021) [77] (US) | Current, 5.7%; Dual, 4.2% | 2009 (8, 9, 11th grades) | Significant difference | Strong parental anti-smoking norms (0.19), college aspirations (0.41), internal developmental assets (0.54), parental connectedness (0.64) | Regular religious participation (2.69) |
| Williams et al. (2020) [78] (Canada) | Current, 22% | 60,601 (14–18 years old) | Significant difference | Intramural participation among female students (0.87) | Varsity participation (1.37) for females and males (1.57), participation in both intramural and varsity sports for females (1.34) and males (1.46) |
| Wills et al. * (2015) [79] (US) | Lifetime, 29%; Current 18.0% | 1941 (9–10th grades) | No difference | Parental support (23.3), parental monitoring (20.0), academic involvement (16.6), behavioral self-control (61.2), emotional self-control (40.4) | Parent–adolescent conflict (8.7), sensation seeking (15.8), rebelliousness (8.4), smoker prototypes (9.4), smoking expectancies (10.1), behavioral dysregulation (43.6), emotional dysregulation (24.7), peer smoking (1.5), perceiving e-cigarette as healthy (1.8), alcohol use (1.5), marijuana use (0.6), heavy drinking (0.3) |
| Zavala-Arciniega et al. (2019) [80] (Mexico) | Lifetime, 9.5%; Current, 10.9% | 8718 (Middle school- aged students) | N/A | N/A | Being male (2.46), higher family affluence (1.13), being a regular smoker (1.81), drug use in the last year (1.89), higher technophilia (1.84), higher sensation seeking (1.31), family members using both e-cigarettes and cigarettes (1.51), being an occasional smoker (0.59) |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kwon, E.; Seo, D.; Lin, H.; Chen, Z. Predictors of youth e-cigarette use susceptibility in a US nationally representative sample. Addict. Behav. 2018, 82, 79–85. [Google Scholar] [CrossRef] [PubMed]
- JUULPod. Available online: https://www.juul.com/about-juul (accessed on 23 May 2021).
- Fadus, M.C.; Smith, T.T.; Squeglia, L.M. The rise of e-cigarettes, pod mod devices, and JUUL among youth: Factors influencing use, health implications, and downstream effects. Drug Alcohol Depend. 2019, 201, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Hanewinkel, R.; Isensee, B. Risk factors for e-cigarette, conventional cigarette, and dual use in German adolescents: A cohort study. Prev. Med. 2015, 74, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Geidne, S.; Beckman, L.; Edvardsson, I.; Hulldin, J. Prevalence and risk factors of electronic cigarette use among adolescents: Data from four Swedish municipalities. Nordic Stud. Alcohol Drugs 2017, 33, 225–240. [Google Scholar] [CrossRef]
- Cullen, K.A.; Ambrose, B.K.; Gentzke, A.S.; Apelberg, B.J.; Jamal, A.; King, B.A. Notes from the field: Use of electronic cigarettes and any tobacco product among middle and high school students-United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1276–1277. [Google Scholar] [CrossRef]
- Chapman, S.L.C.; Wu, L. E-cigarette prevalence and correlates of use among adolescents versus adults: A review and comparison. J. Psychiatr. Res. 2014, 54, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, H.; Min, S. Factors associated with electronic cigarette use among current cigarette-smoking adolescents in the Republic of Korea. Addict. Behav 2017, 69, 22–26. [Google Scholar] [CrossRef]
- Cho, J.H.; Shin, E.; Moon, S. Electronic-cigarette smoking experience among adolescents. J. Adolesc Health 2011, 49, 542–546. [Google Scholar] [CrossRef]
- Gao, W.; Sanna, M.; Chuluunbaatar, E.; Tsai, M.; Levy, D.T.; Wen, C.P. Are e-cigarettes reviving the popularity of conventional smoking among Taiwanese male adolescents? A time-trend population-based analysis for 2004–2017. Tob. Control 2021, 30, 132–136. [Google Scholar] [CrossRef]
- Goniewicz, M.L.; Zielinska-Danch, W. Electronic cigarette use among teenagers and young adults in Poland. Pediatrics 2012, 130, e879–e885. [Google Scholar] [CrossRef]
- Cerrai, S.; Benedetti, E.; Colasante, E.; Scalese, M.; Gorini, G.; Gallus, S.; Molinaro, S. E-cigarette use and conventional cigarette smoking among European students: Findings from the 2019 ESPAD survey. Addiction 2022. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.; Brown, R.; Page, N.; Hallingberg, B.; Marynard, O.; McKell, J.; Gray, L.; Blackwell, A.; Lowthian, E.; Munafò, M.; et al. Young people’s use of e-cigarettes in Wales, England and Scotland before and after introduction of EU Tobacco Products Directive regulations: A mixed-method natural experimental evaluation. Int. J. Drug Policy 2020, 85, 102795. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C. European tobacco products directive (TPD): Current impact and future steps. Tob. Control 2022, 31, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Xi, B.; Ma, C.; Zhao, M.; Bovet, P. Prevalence of e-cigarette use and its associated factors among youths aged 12 to 16 years in 68 countries and territories: Global youth tobacco survey, 2012-2019. Am. J. Public Health 2022, 112, 650–661. [Google Scholar] [CrossRef]
- WHO. Most Recent Nationally Representative Survey Reporting Prevalence of Smokeless Tobacco Use or E-Cigarette Use among Adolescents (Tobacco Control: Monitor). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/gho-tobacco-control-monitor-survey-reporting-prevalence-of-smokeless-tobacco-use-or-e-cigarette-use-among-adolescents (accessed on 22 August 2021).
- Yoong, S.L.; Stockings, E.; Chai, L.K.; Tzelepis, F.; Wiggers, J.; Oldmeadow, C.; Paul, C.; Peruga, A.; Kingsland, M.; Attia, J.; et al. Prevalence of electronic nicotine delivery systems (ENDS) use among youth globally: A systematic review and meta-analysis of country level data. Aust. N. Z. J. Public Health 2018, 42, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Her, W. Factors influencing type of cigarette smoked among adolescents: Focusing on the differences between conventional cigarette and electronic cigarette (in Korean). Health Soc. Welf. Rev. 2020, 40, 489–519. [Google Scholar] [CrossRef]
- Rohde, J.A.; Noar, S.M.; Horvitz, C.; Lazard, A.J.; Ross, J.C.; Sutfin, E.L. The role of knowledge and risk beliefs in adolescent e-cigarette use: A pilot study. Int. J. Environ. Res. Public Health 2018, 15, 830. [Google Scholar] [CrossRef]
- Marques, P.; Piqueras, L.; Sanz, M. An updated overview of e-cigarette impact on human health. Respir. Res. 2021, 22, 151. [Google Scholar] [CrossRef]
- Hua, M.; Talbot, P. Potential health effects of electronic cigarettes: A systematic review of case reports. Prev. Med. Rep. 2016, 4, 169–178. [Google Scholar] [CrossRef]
- Pisinger, C.; Døssing, M. A systematic review of health effects of electronic cigarettes. Prev. Med. 2014, 69, 248–260. [Google Scholar] [CrossRef]
- Jenson, T.E. Psychosocial and behavioral risk profiles of cigarette smokers and e-cigarette users among adolescents in Minnesota: The 2016 Minnesota student survey. Prev. Chronic Dis. 2018, 15, 180222. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.B.; Olgin, J.E.; Nah, G.; Vittinghoff, E.; Ctaldo, J.K.; Pletcher, M.J.; Marcus, G.M. Cigarette and e-cigarette dual use and risk of cardiopulmonary symptoms in the health eHeart study. PLoS ONE 2018, 13, e0198681. [Google Scholar] [CrossRef] [PubMed]
- Varnier, S.; Ronziere, T.; Ferre, J.C.; Lassalle, V.; Verin, M. Reversible cerebral vasoconstriction syndrome triggered by an electronic cigarette: Case report. Eur. J. Neurol. 2015, 22, e64–e65. [Google Scholar] [CrossRef]
- Pepper, J.K.; Brewer, N.T. Electronic nicotine delivery system (electronic cigarette) awareness, use, reactions and beliefs: A systematic review. Tob. Control 2015, 23, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Bowe, A.K.; Doyle, F.; Stanistreet, D.; O’Connell, E.; Durcan, M.; Major, E.; O’Donovan, D.; Kavanagh, P. E-cigarette-only and dual use among adolescents in Ireland: Emerging behaviours with different risk profiles. Int. J. Environ. Res. Public Health 2021, 18, 332. [Google Scholar] [CrossRef]
- McCabe, S.E.; Boyd, C.J.; Evans-Polce, R.J.; McCabe, V.V.; Veliz, P.T. School-level prevalence and predictors of e-cigarette use in 8th, 10th, and 12th grade US youth: Results from a national survey (2015–2016). J. Adolesc. Health 2020, 67, 531–541. [Google Scholar] [CrossRef]
- Robert Lourdes, T.G.; Abd Hamid, H.A.; Mohd Yusoff, M.F.; Hasani, W.S.R.; Rifin, H.M.; Saminathan, T.A.; Majid, N.L.A.; Ling, J.M.Y.; Ismail, H.; Aris, T. Factors associated with e-cigarette usage and the reasons for initiation among Malaysian adolescents. Asia Pac. J. Public Health 2019, 31 (Suppl. S7), 44S–52S. [Google Scholar] [CrossRef]
- Conner, M.; Grogan, S.; Simms-Ellis, R.; Scholtens, K.; Sykes-Muskett, B.; Cowap, L.; Lawton, R.; Armitage, C.J.; Meads, D.; Schmitt, L.; et al. Patterns and predictors of e-cigarette, cigarette and dual use uptake in UK adolescents: Evidence from a 24-month prospective study. Addiction 2019, 114, 2048–2055. [Google Scholar] [CrossRef]
- Gusenbauer, M. Google scholar to overshadow them all? Comparing the sizes of 12 academic search engines and bibliographic databases. Scientometrics 2018, 118, 177–214. [Google Scholar] [CrossRef]
- Shunli, L. Comprehensive Evaluation of EBSCO Database: Comparing with ProQuest Database. Available online: http://en.cnki.com.cn/Article_en/CJFDTotal-TSGJ200808017.htm (accessed on 22 August 2021).
- Williamson, P.O.; Minter, C.I.J. Exploring PubMed as a reliable resource for scholarly communications services. J. Med. Libr. Assoc. 2019, 107, 16–29. [Google Scholar] [CrossRef]
- National Center for Chronic Disease Prevention and Health Promotion Office on Smoking and Health. E-Cigarette Use among Youth and Young Adults: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, AT, USA, 2016.
- CDC. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/about-e-cigarettes.html (accessed on 3 June 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- WHO. Available online: https://www.who.int/southeastasia/health-topics/adolescent-health (accessed on 22 August 2021).
- Seo, D.; Huang, Y. Systematic review of social network analysis in adolescent cigarette smoking behavior. J. Sch. Health 2012, 82, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.; Gregory, D. Evaluation of qualitative research studies. Evid. Based Nurs. 2003, 6, 36–40. [Google Scholar] [CrossRef]
- Anand, V.; McGinty, K.L.; O’Brien, K.; Guenthner, G.; Hahn, E.; Martin, C.A. E-cigarette use and beliefs among urban public high school students in North Carolina. J. Adolesc. Health 2015, 57, 46–51. [Google Scholar] [CrossRef]
- Barrington-Trimis, J.L.; Berhane, K.; Unger, J.B.; Cruz, T.B.; Huh, J.; Leventhal, A.M.; Urman, R.; Wang, K.; Howland, S.; Gilreath, T.D.; et al. Psychosocial factors associated with adolescent electronic cigarette and cigarette use. Pediatrics 2015, 136, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Best, C.; van der Slujis, W.; Haseen, F.; Eadie, D.; Staed, M.; MacKintosh, A.M.; Pearce, J.; Tisch, C.; MacGregor, A.; Amos, A.; et al. Does exposure to cigarette brands increase the likelihood of adolescent e-cigarette use? A cross-sectional study. BMJ Open 2015, 6, e008734. [Google Scholar] [CrossRef]
- Bostean, G.; Crespi, C.M.; Vorapharuek, P.; McCarthy, W.J. E-cigarette use among students and e-cigarette specialty retailer presence near schools. Health Place 2016, 42, 129–136. [Google Scholar] [CrossRef]
- Buu, A.; Hu, Y.; Wong, S.; Lin, H. Internalizing and externalizing problems as risk factors for initiation and progression of e-cigarette and combustible cigarette use in the US youth population. Int. J. Ment. Health Addict. 2021, 19, 1759–1771. [Google Scholar] [CrossRef]
- Carey, F.R.; Rogers, S.M.; Cohn, E.A.; Harrell, M.B.; Wilkinson, A.V.; Perry, C.L. Understanding susceptibility to e-cigarettes: A comprehensive model of risk factors that influence the transition from non-susceptible to susceptible among e-cigarette naïve adolescents. Addict. Behav. 2019, 91, 68–74. [Google Scholar] [CrossRef]
- Case, K. Sensation Seeking and E-Cigarette Use in Texas Adolescents and Young Adults. Ph.D. Thesis, University of Texas School of Public Health, Dallas, TX, USA, 2016. [Google Scholar]
- Case, K.R.; Obinwa, U.C.; Clendennen, S.L.; Perry, C.L.; Harrell, M.B. Predictors of JUUL, other electronic nicotine delivery systems, and combustible tobacco initiation among Texas youth. Prev. Med. 2020, 138, 106097. [Google Scholar] [CrossRef]
- Chun, J.; Yu, M.; Kim, J.; Kim, A. E-cigarette, cigarette, and dual use in Korean adolescents: A test of problem behavior theory. J. Psychoact. Drugs 2020, 52, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Demissie, Z.; Jones, S.E.; Clayton, H.B.; King, B.A. Adolescent risk behaviors and use of electronic vapor products and cigarettes. Pediatrics 2017, 139, e2162921. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, P.D.; Hammig, B.; Henry, L.J. E-cigarette use among US adolescents: Perceptions of relative addiction and harm. Health Educ. J. 2017, 76, 293–301. [Google Scholar] [CrossRef]
- Dubar, M.S.; Davis, J.P.; Rodriguez, A.; Tucker, J.S.; Seelam, R.; D’Amico, E.J. Disentangling within- and between-person effects of shared risk factors on e-cigarette use and cigarette use trajectories from late adolescence to young adulthood. Nicotine Tob. Res. 2019, 21, 1414–1422. [Google Scholar] [CrossRef]
- Enlow, P.T. Characterizing Risk Factors of Adolescent Electronic Cigarette Use. Ph.D. Thesis, West Virginia University, Morgantown, WV, USA, 2018. [Google Scholar]
- Etim, N.; Pike, J.; Xie, B. Age-varying associations between e-cigarette use and peer use, household use, and exposure to e-cigarette commercials among alternative high school students in Southern California. Tob. Induc. Dis. 2020, 18, 7. [Google Scholar] [CrossRef]
- Hedman, L.; Backman, H.; Stridsman, C.; Lundbäck, M.; Andersson, M.; Rönmark, E. Predictors of electronic cigarette use among Swedish teenagers: A population-based cohort study. BMJ Open 2020, 10, e040683. [Google Scholar] [CrossRef]
- Jayakumar, N.; O’Connor, S.; Diemert, L.; Schwartz, R. Predictors of e-cigarette initiation: Findings from the youth and young adult panel study. Tob. Use Insights 2020, 13, 1–9. [Google Scholar] [CrossRef]
- Jeon, C.; Jung, K.J.; Kimm, H.; Lee, S.; Barrington-Trimis, J.L.; McConnell, R.; Samet, J.M.; Jee, S.H. E-cigarettes, conventional cigarettes, and dual use in Korean adolescents and university students: Prevalence and risk factors. Drug Alcohol Depend. 2016, 168, 99–103. [Google Scholar] [CrossRef]
- Kaleta, D.; Wojtysiak, P.; Polańska, K. Use of electronic cigarettes among secondary and high school students from a socially disadvantaged rural area in Poland. BMC Public Health 2016, 16, 703. [Google Scholar] [CrossRef]
- Kinnunen, J.M.; Ollila, H.; El-Amin, S.E.; Pere, L.A.; Lindfors, P.L.; Rimpelä, A.H. Awareness and determinants of electronic cigarette use among Finnish adolescents in 2013: A population-based study. Tob. Control 2014, 24, e264–e270. [Google Scholar] [CrossRef]
- Kinnunen, J.M.; Rimpelä, A.H.; Lindfors, P.L.; Clancy, L.; Alves, J.; Hoffmann, L.; Richter, M.; Kunst, A.E.; Lorant, V. Electronic cigarette use among 14- to 17-year-olds in Europe. Eur. J. Public Health 2021, 31, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Kintz, N.; Liu, M.; Chou, C.P.; Urman, R.; Berhane, K.; Unger, J.B.; Cruz, T.B.; McConnell, R.; Barrington-Trimis, J.L. Risk factors associated with subsequent initiation of cigarettes and e-cigarettes in adolescence: A structural equation modeling approach. Drug Alcohol Depend. 2020, 207, 107676. [Google Scholar] [CrossRef] [PubMed]
- Lessard, J.; Henrie, J.; Livingston, J.A.; Leonard, K.E.; Colder, C.R.; Eiden, R.D. Correlates of ever having used electronic cigarettes among older adolescent children of alcoholic fathers. Nicotine Tob. Res. 2014, 16, 1656–1660. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mantey, D.S.; Cooper, M.R.; Cledennen, S.L.; Pasch, K.E.; Perry, C.L. E-cigarette marketing exposure is associated with e-cigarette use among US youth. J. Adolesc. Health 2016, 58, 686–690. [Google Scholar] [CrossRef]
- Mantey, D.S.; Barroso, C.S.; Kelder, B.T.; Kelder, S.H. Retail access to e-cigarettes and frequency of e-cigarette use in high school students. Tob. Regul. Sci. 2019, 5, 280–290. [Google Scholar] [CrossRef]
- Morello, P.; Pérez, A.; Peña, L.; Lozano, P.; Thrasher, J.F.; Sargent, J.D.; Mejia, R. Prevalence and predictors of e-cigarette trial among adolescents in Argentina. Tob. Prev. Cessat. 2016, 2, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ofuchi, T.; Zaw, A.M.M.; Thepthien, B. Adverse childhood experiences and prevalence of cigarette and e-cigarette use among adolescents in Bangkok, Thailand. Asia Pac. J. Public Health 2020, 32, 398–405. [Google Scholar] [CrossRef]
- Parks, M.J.; Davis, L.; Wilhelm, A.K.; McMorris, B.J.; Borowsky, I.W.; Shlafer, R.J. Parental incarceration and youth tobacco product use: Implications for prevention and the e-cigarette epidemic. Addict. Behav. 2020, 107, 106428. [Google Scholar] [CrossRef]
- Santistevan, A. Awareness of E-Cigarettes and Correlation of Use among High School Students. Ph.D. Thesis, Colorado State University, Fort Collins, CO, USA, 2016. [Google Scholar]
- Sawdey, M.D.; Day, H.R.; Coleman, B.; Gardner, L.D.; Johnson, S.E.; Limpert, J.; Hammad, H.T.; Goniewicz, M.L.; Abrams, D.B.; Stanton, C.A.; et al. Associations of risk factors of e-cigarette and cigarette use and susceptibility to use among baseline PATH study youth participants (2013–2014). Addict. Behav. 2019, 91, 51–60. [Google Scholar] [CrossRef]
- Shih, R.A.; Parast, L.; Pedersen, E.R.; Troxel, W.M.; Tucker, J.S.; Miles, J.N.V.; Kraus, L.; D’Amico, E.J. Individual, peer, and family factor modification of neighborhood-level effects on adolescent alcohol, cigarette, e-cigarette, and marijuana use. Drug Alcohol Depend. 2017, 180, 76–85. [Google Scholar] [CrossRef]
- Soteriades, S.; Barbouni, A.; Rachiotis, G.; Grevenitou, P.; Mouchtouri, V.; Pinaka, O.; Dadouli, K.; Hadjichristodoulou, C. Prevalence of electronic cigarette use and its determinants among 13-to-15 year-old students in Greece: Results from the 2013 global youth tobacco survey (GYTS). Int. J. Environ. Res. Public Health 2020, 17, 1671. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.D. Predictors of Adolescent E-Cigarette Use. Ph.D. Thesis, Loma Linda University, Loma Linda, CA, USA, 2016. [Google Scholar]
- Trucco, E.M.; Cristello, J.V.; Sutherland, M.T. Do parents still matter? The impact of parents and peers on adolescent electronic cigarette use. J. Adolesc. Health 2021, 68, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.B.; Bartsch, L. Exposure to tobacco websites: Associations with cigarette and e-cigarette use and susceptibility among adolescents. Addict. Behav. 2018, 78, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Veliz, P.; McCabe, S.E.; McCabe, V.V.; Boyd, C.J. Adolescent sports participation, e-cigarette use, and cigarette smoking. Am. J. Prev. Med. 2017, 53, e175–e183. [Google Scholar] [CrossRef]
- Vogel, E.A.; Ramo, D.E.; Rubinstein, M.L. Prevalence and correlates of adolescents’ e-cigarette use frequency and dependence. Drug Alcohol Depend. 2018, 188, 109–112. [Google Scholar] [CrossRef]
- White, J.; Li, J.; Newcombe, R.; Walton, D. Tripling use of electronic cigarettes among New Zealand adolescents between 2012 and 2014. J. Adolesc. Health 2015, 56, 522–528. [Google Scholar] [CrossRef]
- Wilhelm, A.K.; Parks, M.; Eisenberg, M.E.; Allen, M.L. Patterns of tobacco use and related protective factors among Somali youth in the United States. J. Immigr. Minor. Health 2020, 23, 103–112. [Google Scholar] [CrossRef]
- Williams, G.C.; Burns, K.E.; Battista, K.; de Groh, M.; Jiang, Y.; Leatherdale, S.T. High school sport participation and substance use: A cross-sectional analysis of students from the COMPASS study. Addict. Behav. Rep. 2020, 12, 100298. [Google Scholar] [CrossRef]
- Wills, T.A.; Knight, R.; Williams, R.J.; Pagano, I.; Sargent, J.D. Risk factors for exclusive e-cigarette use and dual e-cigarette use and tobacco use in adolescents. Pediatrics 2015, 135, e43–e51. [Google Scholar] [CrossRef]
- Zavala-Arciniega, L.; Lozano, P.; Kollath-Cattano, C.; Gutierrez-Torres, D.S.; Santillan, E.A.; Barrientos-Gutierrez, I.; Hardin, J.W.; Thrasher, J.F. E-cigarette use frequency and motivations among current users in middle school. Drug Alcohol Depend. 2019, 204, 107585. [Google Scholar] [CrossRef]
- Chun, J.; Lee, J.; Kim, J.; Lee, S. An international systematic review of cyberbullying measurements. Comput. Hum. Behav. 2020, 113, 106485. [Google Scholar] [CrossRef]
- Dowling, N.A.; Merkouris, S.S.; Greenwood, C.J.; Oldenhof, E.; Toumbourou, J.W.; Youssef, G.J. Early risk and protective factors for problem gambling: A systematic review and meta-analysis of longitudinal studies. Clin. Psychol Rev. 2017, 51, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Guydish, J.; Passalacqua, E.; Pagano, A.; Martinez, C.; Le, T.; Chun, J.; Tajima, B.; Docto, L.; Garina, D.; Delucchi, K. An international systematic review of smoking prevalence in addiction treatment. Addiction 2016, 111, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Timshel, I.; Montgomery, E.; Dalgaard, N.T. A systematic review of risk and protective factors associated with family related violence in refugee families. Child. Abuse Negl. 2017, 70, 315–330. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Riley, R.D.; Higgins, J.P.T.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef]
- American Academy of Child and Adolescent Psychiatry. Facts for Families: Adolescent Development Part I and II. Available online: https://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/FFF-Guide-Table-of-Contents.aspx#letterN (accessed on 22 August 2021).
- Chun, J. Public health threat of tobacco and substance use in Asia: An introduction to the theme issue. J. Psychoactive Drugs 2020, 52, 1–4. [Google Scholar] [CrossRef]
- Kim, J. Factors associated with Korean multicultural youths’ alcohol use: Focusing on the foreign parents’ nationalities (in Korean). J. Multi-Cultural Contents Stud. 2020, 34, 33–61. [Google Scholar] [CrossRef]
- Jin, P.; Jiang, J.Y. E-cigarettes in ten Southeast Asian countries: A comparison of national regulations. Glob. Health 2017, 1, 1–10. [Google Scholar] [CrossRef]
- Wipfli, H.; Bhuiyan, M.R.; Qin, X.; Gainullina, Y.; Palaganas, E.; Jimba, M.; Saito, J.; Ernstrom, K.; Raman, R.; Withers, M. Tobacco use and e-cigarette regulation: Perspectives of university students in the Asia-Pacific. Addict. Behav. 2020, 107, 106420. [Google Scholar] [CrossRef]
- Graham, A.L.; Jacobs, M.A.; Amato, M.S.; Cha, S.; Bottcher, M.M.; Papandonatos, G.D. Effectiveness of a quit vaping text message program in promoting abstinence among young adult e-cigarette users: Protocol for a randomized controlled trial. JMIR Res. Protoc. 2020, 9, e18327. [Google Scholar] [CrossRef]
- National Institute of Mental Health. What Is Prevalence? Available online: https://www.nimh.nih.gov/health/statistics/what-is-prevalence (accessed on 22 August 2021).
- Boyle, M. Guidelines for evaluating prevalence studies. Evid.-Based Ment. Health 1998, 1, 37–39. [Google Scholar] [CrossRef]
- Pineiro, B.; Correa, J.B.; Simmons, V.N.; Harrell, P.T.; Menzie, N.S.; Unrod, M.; Meltzer, L.R.; Brandon, T.H. Gender differences in use and expectancies of e-cigarettes: Online survey results. Addict. Behav. 2016, 52, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Hartwell, G.; Thomas, S.; Egan, M.; Gilmore, A.; Petticrew, M. E-cigarettes and equity: A systematic review of differences in awareness and use between sociodemographic groups. Tob. Control 2017, 26, e85–e91. [Google Scholar] [CrossRef] [PubMed]
- Abrams, L.R.; Kalousova, L.; Fleischer, N.L. Gender differences in relationships between sociodemographic factors and e-cigarette use with smoking cessation:2014–15 current population survey tobacco use supplement. J. Public Health 2019, 42, e43–e51. [Google Scholar] [CrossRef] [PubMed]
- Amrock, S.M.; Lee, L.; Weitzman, M. Perceptions of e-cigarettes and noncigarette tobacco products among US youth. Pediatrics 2016, 138, e20154306. [Google Scholar] [CrossRef]
- Rom, R.; Pecorelli, A.; Valacchi, G.; Reznick, A.Z. Are e-cigarettes a safe and good alternative to cigarette smoking? Ann. N. Y. Acad. Sci. 2014, 1340, 65–74. [Google Scholar] [CrossRef]
- Thomas, R.E.; McLellan, J.; Perera, R. School-based programmes for preventing smoking (Review). Cochrane Database Syst Rev. 2013, 8, 1616–2040. [Google Scholar] [CrossRef]
- Cambron, C.; Kosterman, R.; Catalano, R.F.; Guttmannova, K.; Hawkins, J.D. Neighborhood, family, and peer factors associated with early adolescent smoking and alcohol use. J. Youth Adolesc. 2018, 47, 369–382. [Google Scholar] [CrossRef]
- Andrews, J.O.; Bentley, G.; Crawford, S.; Pretlow, L.; Tingen, M.S. Using community-based participatory research to develop a culturally sensitive smoking cessation intervention with public housing neighborhoods. Ethn. Dis. 2007, 17, 331–337. [Google Scholar]
- Pike, J.S.; Tan, N.; Miller, S.; Cappelli, C.; Xie, B.; Stacy, A.W. The effect of e-cigarette commercials on youth smoking: A prospective study. Am. J. Health Behav. 2019, 43, 1103–1118. [Google Scholar] [CrossRef]
- Amin, S.; Dunn, A.G.; Laranjo, L. Exposure to e-cigarette information and advertising in social media and e-cigarette use in Australia: A mixed methods study. Drug Alcohol Depend. 2020, 213, 108112. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.; Glasser, A.M.; Abudayyeh, H.; Pearson, J.L.; Villanti, A.C. E-Cigarette marketing and communication: How e-cigarette companies market e-cigarettes and the public engages with e-cigarette information. Nicotine Tob. Res. 2019, 21, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Tilden, C.; Vernberg, D.K. Adolescents’ interpretations of e-cigarette advertising and their engagement with e-cigarette information: Results from five focus groups. Psychol Health 2020, 35, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Mackey, T.K.; Miner, A.; Cuomo, R.E. Exploring the e-cigarette e-commerce marketplace: Identifying Internet e-cigarette marketing characteristics and regulatory gaps. Drug Alcohol Depend. 2015, 156, 97–103. [Google Scholar] [CrossRef]
- Williams, R.S.; Derrick, J.; Ribisl, K.M. Electronic cigarette sales to minors via the internet. JAMA Pediatr. 2015, 169, e1563. [Google Scholar] [CrossRef] [PubMed]
- Institute for Global Tobacco Control. Available online: https://www.globaltobaccocontrol.org/e-cigarette_policyscan (accessed on 1 September 2022).
- Government of Canada. Available online: https://www.canada.ca/en/health-canada/services/smoking-tobacco/vaping/product-safety-regulation.html#a1 (accessed on 1 September 2022).
- Campus, B.; Fafard, P.; Pierre, J.S.; Hoffman, S.J. Comparing the regulation and incentivization of e-cigarettes across 97 countries. Soc. Sci Med. 2021, 291, 114187. [Google Scholar] [CrossRef]
- Bureau of Alcohol, Tobacco, Firearms and Explosives. Available online: https://www.atf.gov/alcohol-tobacco/prevent-all-cigarette-trafficking-pact-act (accessed on 1 September 2022).
- Library of Congress. Available online: https://www.congress.gov/bill/116thcongress/senate-bill/1253/text (accessed on 1 September 2022).
- Kim, J. Korean Adolescent’s Cigarette, E-Cigarette, and Dual Use within the Peer Network Context. Ph.D. Thesis, Ewha Womans University, Seoul, Korea, 2022. [Google Scholar]
- Public Health Law Center. Available online: https://www.publichealthlawcenter.org/resources/us-ecigarette-regulations-50-state-review/nc (accessed on 1 September 2022).
- U.S. Food & Drug Administration. Available online: http://www.fda.gov/tobacco-products/products-ingredients-components/vaporizers-e-cigarettes-and-other-electronic-nicotine-delivery-systems-ends (accessed on 1 September 2022).
- Merrill, J.K.; Alberg, A.J.; Goffin, J.R.; Ramalingam, S.S.; Simmons, V.N.; Warren, G.W. American society of clinical oncology policy brief: FDA’s regulation electronic nicotine delivery systems and tobacco products. J. Oncol. Pract. 2016, 13, 58–60. [Google Scholar] [CrossRef]
- Korean Law Information Center. Available online: https://law.go.kr/lsSc.do?menuId=1&subMenuId=15&tabMenuId=81&query=%EB%8B%B4%EB%B0%B0#undefined (accessed on 1 September 2022).
- Hod, R.; Nor, N.H.M.; Manjam, S. Systematic review on e-cigarette and its effects on weight gain and adipocytes. PLoS ONE 2022, 17, e0270818. [Google Scholar] [CrossRef]
- Glasser, A.; Abudayyeh, H.; Cantrell, J.; Niaura, R. Patterns of e-cigarette use among youth and young adults: Review of the impact of e-cigarettes on cigarette smoking. Nicotine Tob. Res. 2019, 21, 1320–1330. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Lee, S.; Chun, J. An International Systematic Review of Prevalence, Risk, and Protective Factors Associated with Young People’s E-Cigarette Use. Int. J. Environ. Res. Public Health 2022, 19, 11570. https://doi.org/10.3390/ijerph191811570
Kim J, Lee S, Chun J. An International Systematic Review of Prevalence, Risk, and Protective Factors Associated with Young People’s E-Cigarette Use. International Journal of Environmental Research and Public Health. 2022; 19(18):11570. https://doi.org/10.3390/ijerph191811570
Chicago/Turabian StyleKim, Jinyung, Serim Lee, and JongSerl Chun. 2022. "An International Systematic Review of Prevalence, Risk, and Protective Factors Associated with Young People’s E-Cigarette Use" International Journal of Environmental Research and Public Health 19, no. 18: 11570. https://doi.org/10.3390/ijerph191811570
APA StyleKim, J., Lee, S., & Chun, J. (2022). An International Systematic Review of Prevalence, Risk, and Protective Factors Associated with Young People’s E-Cigarette Use. International Journal of Environmental Research and Public Health, 19(18), 11570. https://doi.org/10.3390/ijerph191811570