
Telemedicine Technologies Selection for the Posthospital Patient Care Process after Total Hip Arthroplasty

 , , , ,
, , , ,  ,
,  and
and
Abstract
:Abstract
Protocol Registration
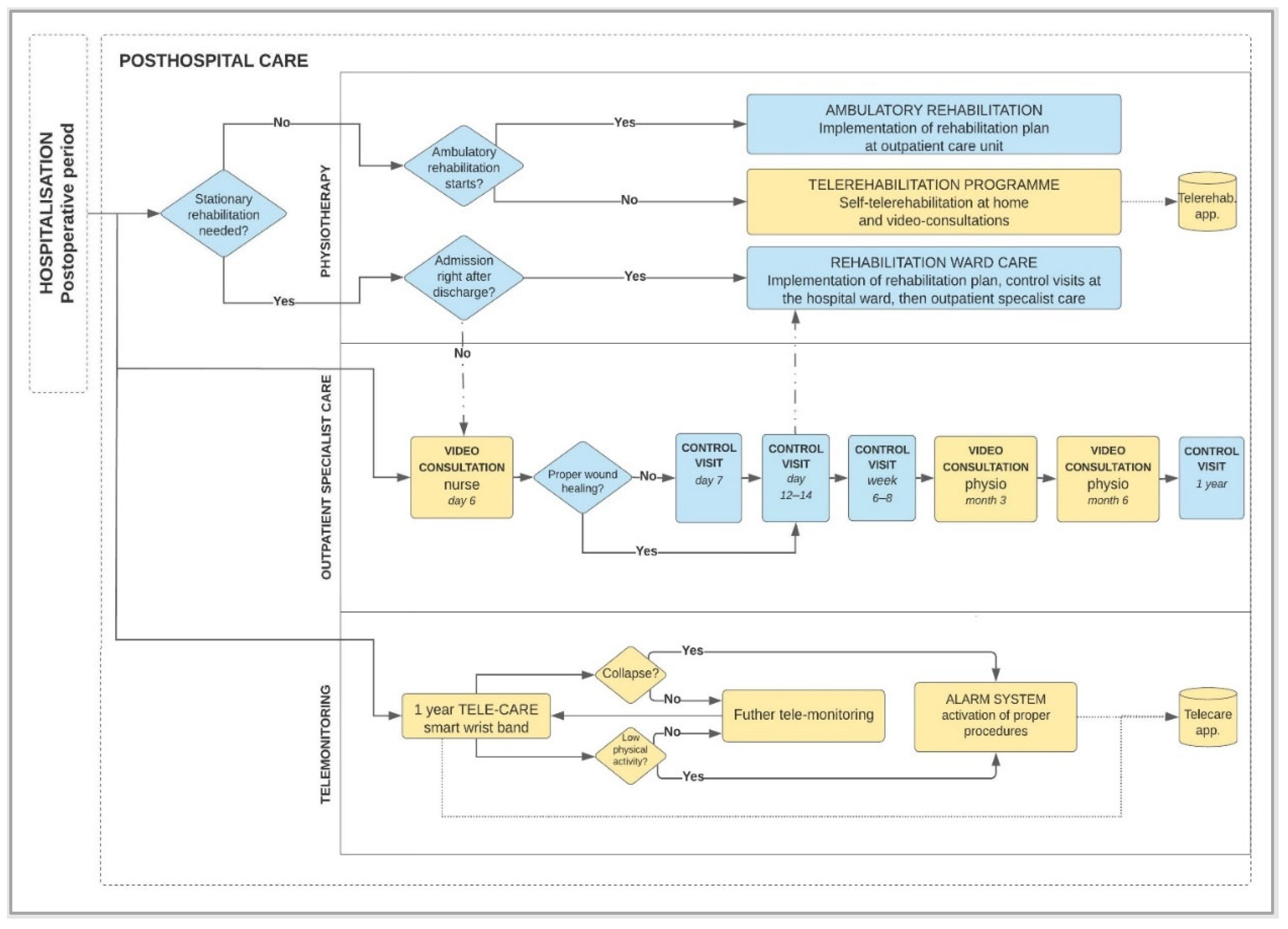
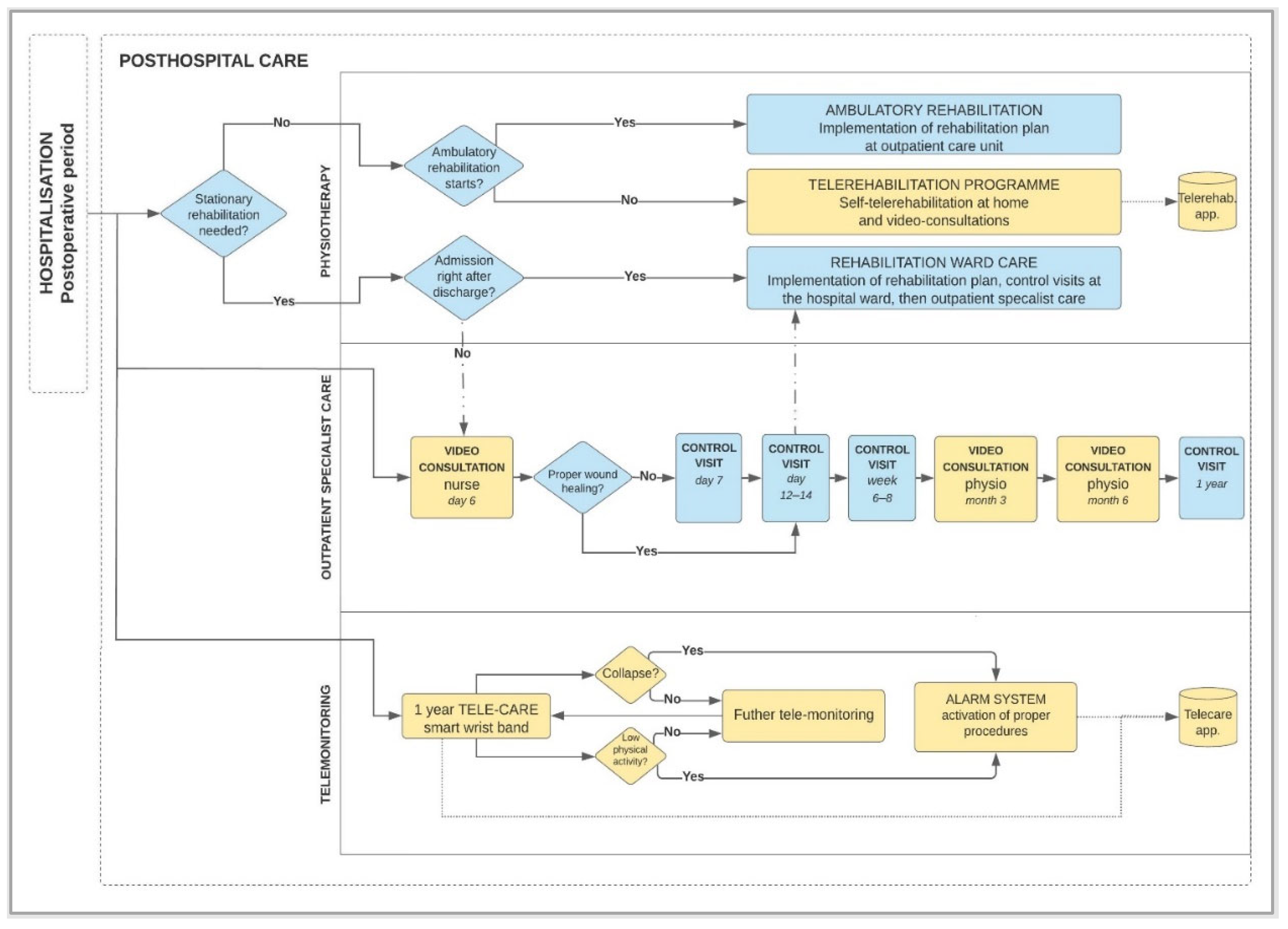
1. Introduction
- Teleconsultation,
- Telerehabilitation,
- Telemonitoring.
2. Materials and Methods
2.1. Research Questions
- Who uses telemedicine technologies in the posthospital patient care process after THA?
- What data are collected from telemedicine technologies used in the posthospital patient care process after THA?
- What are the needs of stakeholders in the posthospital patient care process after THA?
- What technologies are more common in the postoperative patient care process after total hip arthroplasty?
- Will it be possible to define groups of the most important technologies used in the studied process?
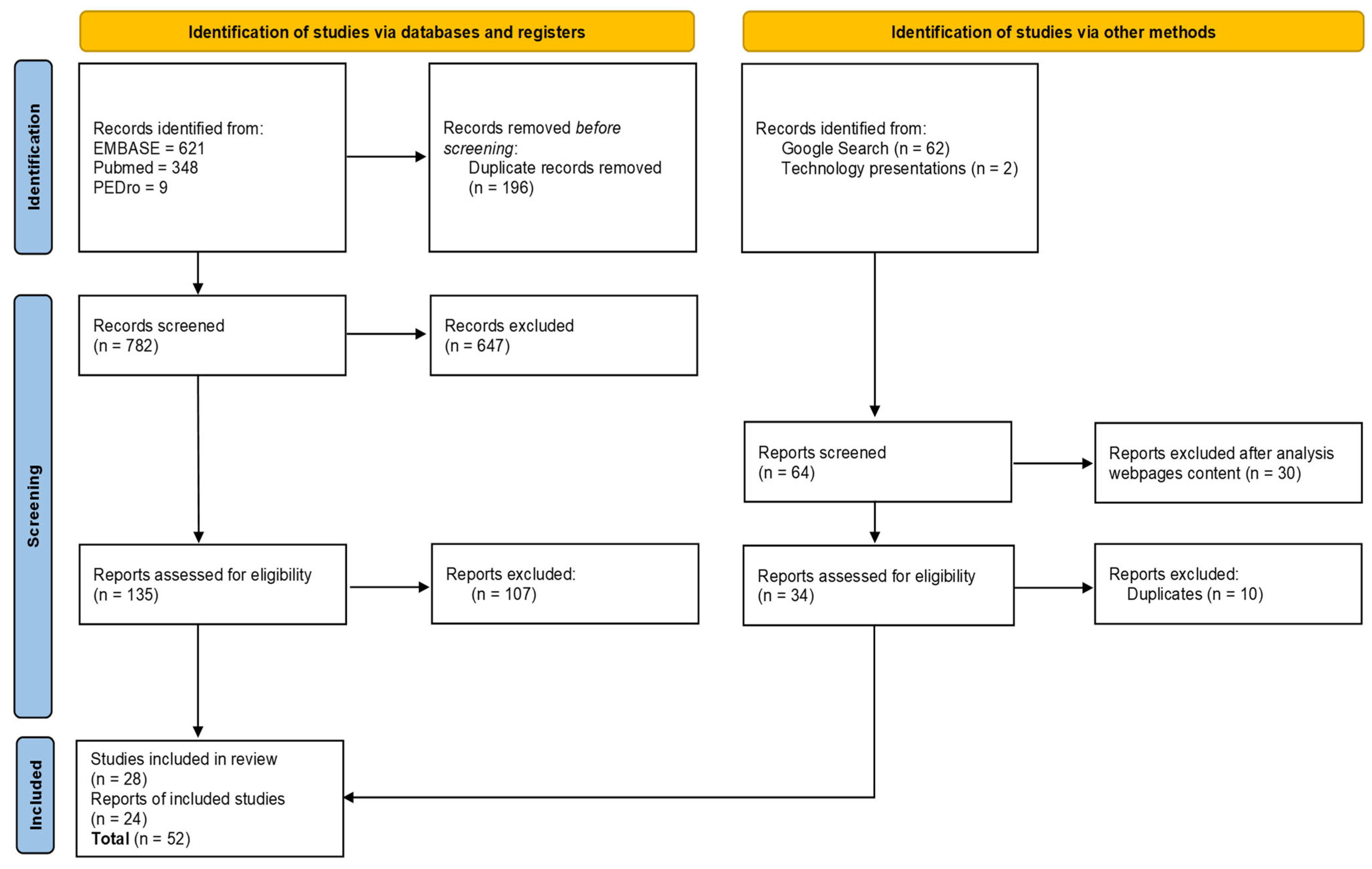
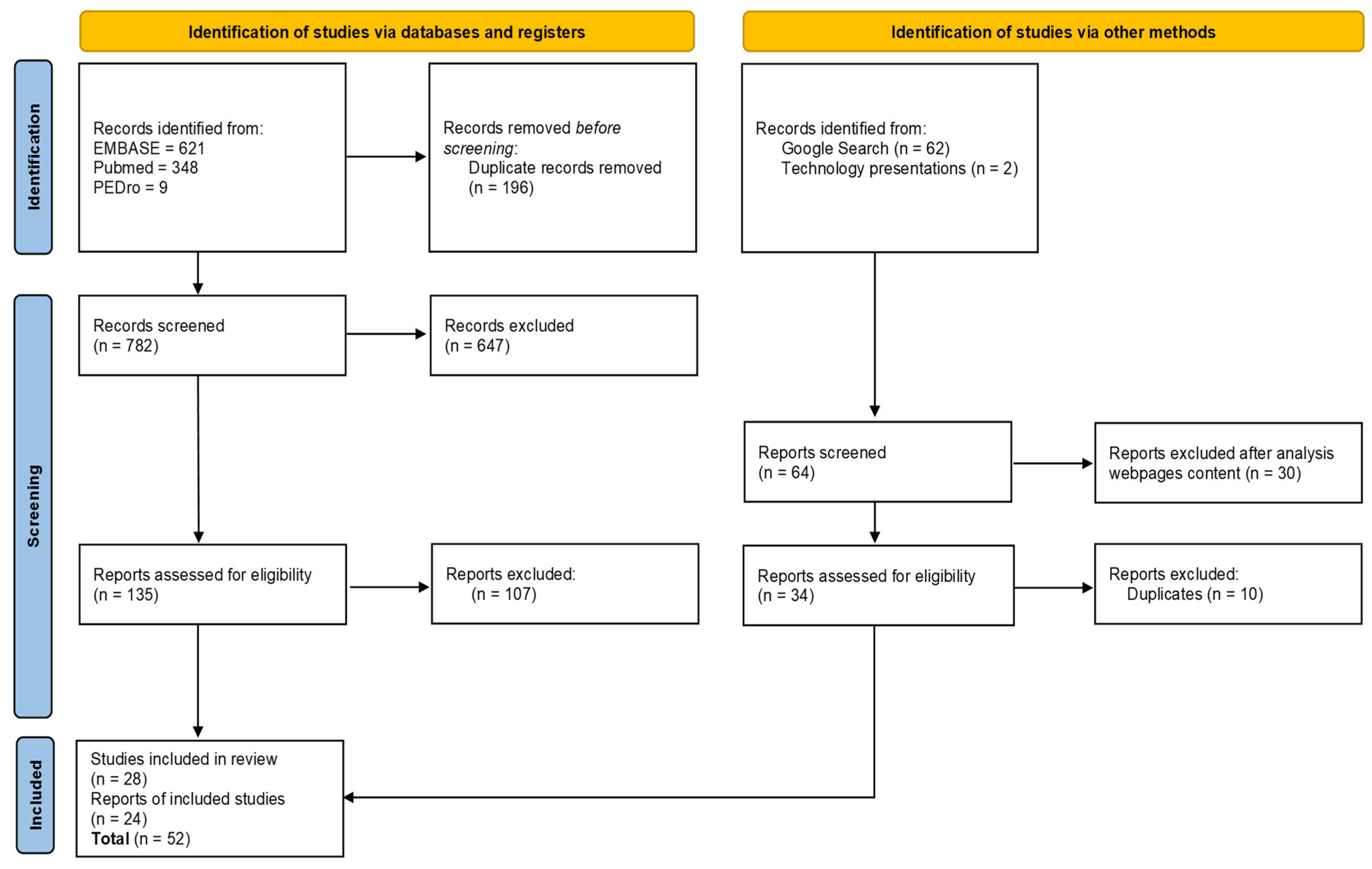
2.2. Literature Search
2.3. Technology Market Analysis
2.3.1. Market Analysis Methods
2.3.2. Google Search
- Technology is used in the healthcare sector, in specialistic medical programs, clinical trials, or EU co-financed grants,
- Technology meets the professional criteria, approvals, or recommendations recognized for telemedicine technologies by global organizations such as government institutions, the Food and Drug Administration (FDA), World Health Organization (WHO), American Telemedicine Association ATA), or medical device regulations (EU Medical Device Regulation MDR 2017/745) [9,10,11,12],
- Technology is mentioned in scientific publications over technology application,
- Technology or its direct supplier is certified in management or security systems or other specialist certifications specific to the health sector.
2.3.3. Practical Experience and Technology Knowledge
3. Results
3.1. Study Identification
3.2. Users of Telemedicine Technologies in Posthospital Patient Care Process after THA
3.3. Data Collected from Telemedicine Technologies Used in Posthospital Patient Care Process after THA
3.4. Telemedicine Technology’s Needs in the Posthospital Patient Care Process after Total Hip Arthroplasty
3.5. Analysis of Visual Telemedicine Technologies in the Posthospital Patient Care Process after THA
- Telerehabilitation application using smartphone camera [77],
- Technology-based home exercise program using iPad application [29],
- eHealth education program with web-based access to resources and communication log with hospital professionals [27],
- Tablet-based technology for daily biophysical measurements, photographs of operation wounds, and virtual interaction with a nurse [13],
3.6. Analysis of Wearable Telemedicine Technologies in the Posthospital Patient Care Process after THA
- Fall sensor,
- GPS location,
- Activity sensor,
- Notification to take an exercise,
- Device insertion sensor,
- Defining the boundaries of the movement area (virtual fences),
- Communication by e-mail or phone to the patient’s guardian,
- 24-h monitoring center service,
- Pulse,
- Reminder for medications or fluid intake.
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Topol, E.J. Telemedicine 2020 and the next decade. Lancet 2020, 395, 859. [Google Scholar] [CrossRef]
- Gogia, S. Rationale, history, and basics of telehealth. In Fundamentals of Telemedicine and Telehealth; Gogia, S., Masucci, S., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 11–34. [Google Scholar]
- de Araújo Novaes, M. Chapter 10—Telecare within Different Specialties in Fundamentals of Telemedicine and Telehealth; Gogia, S., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 185–254. Available online: https://www.sciencedirect.com/science/article/pii/B9780128143094000100 (accessed on 1 January 2020).
- Glinkowski, W.M. Orthopedic Telemedicine Outpatient Practice Diagnoses Set during the First COVID-19 Pandemic Lockdown—Individual Observation. Int. J. Environ. Res. Public Health 2022, 19, 5418. [Google Scholar] [CrossRef] [PubMed]
- Eze, N.D.; Mateus, C.; Cravo Oliveira Hashiguchi, T. Telemedicine in the OECD: An umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLoS ONE 2020, 15, e0237585. [Google Scholar] [CrossRef] [PubMed]
- Furlepa, K.; Tenderenda, A.; Kozłowski, R.; Marczak, M.; Wierzba, W.; Śliwczyński, A. Recommendations for the Development of Telemedicine in Poland Based on the Analysis of Barriers and Selected Telemedicine Solutions. Int. J. Environ. Res. Public Health 2022, 19, 1221. [Google Scholar] [CrossRef]
- Kamecka, K.; Rybarczyk-Szwajkowska, A.; Staszewska, A.; Engelseth, P.; Kozlowski, R. Process of Posthospital Care Involving Telemedicine Solutions for Patients after Total Hip Arthroplasty. Int. J. Environ. Res. Public Health 2021, 18, 10135. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration Federal Agency. Digital Center of Excellence. Available online: https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health (accessed on 5 May 2022).
- World Health Organization. Implementing Telemedicine Services during COVID-19: Guiding Principles and Considerations for a Stepwise Approach; Interim Guidance; Republished without Changes on 7 May 2021, WPR/DSE/2020/032; WHO Regional Office for the Western Pacific: Manila, Philippines, 2021. [Google Scholar]
- Guidelines of American Telemedicine Association for Telemedicine at Home. Available online: https://www.americantelemed.org/?s=telemedicine+at+home (accessed on 5 May 2022).
- EU Medical Device Regulation. Available online: https://www.medical-device-regulation.eu/download-mdr/ (accessed on 5 May 2022).
- McGillion, M.H.; Parlow, J.; Borges, F.K.; Marcucci, M.; Jacka, M.; Adili, A.; Lalu, M.M.; Ouellette, C.; Bird, M.; Ofori, S.; et al. PVC-RAM-1 Investigators. Post-discharge after surgery Virtual Care with Remote Automated Monitoring-1 (PVC-RAM-1) technology versus standard care: Randomised controlled trial. BMJ 2021, 374, n2209. [Google Scholar] [CrossRef]
- Farias, F.A.C.; Dagostini, C.M.; Bicca, Y.A.; Falavigna, V.F.; Falavigna, A. Remote Patient Monitoring: A Systematic Review. Telemed. J. e-Health 2020, 26, 576–583. [Google Scholar] [CrossRef]
- Doiron-Cadrin, P.; Kairy, D.; Vendittoli, P.A.; Lowry, V.; Poitras, S.; Desmeules, F. Feasibility and preliminary effects of a tele-prehabilitation program and an in-person prehabilitation program compared to usual care for total hip or knee arthroplasty candidates: A pilot randomized controlled trial. Disabil. Rehabil. 2020, 42, 989–998. [Google Scholar] [CrossRef]
- Kloek, C.J.J.; van Dongen, J.M.; de Bakker, D.H.; Bossen, D.; Dekker, J.; Veenhof, C. Cost-effectiveness of a blended physiotherapy intervention compared to usual physiotherapy in patients with hip and/or knee osteoarthritis: A cluster randomized controlled trial. BMC Public Health 2018, 18, 1082. [Google Scholar] [CrossRef]
- Marsh, J.; Bryant, D.; MacDonald, S.J.; Naudie, D.; Remtulla, A.; McCalden, R.; Howard, J.; Bourne, R.; McAuley, J. Are patients satisfied with a web-based followup after total joint arthroplasty? Clin. Orthop. Relat. Res. 2014, 472, 1972–1981. [Google Scholar] [CrossRef] [PubMed]
- Kummerow Broman, K.; Roumie, C.L.; Stewart, M.K.; Castellanos, J.A.; Tarpley, J.L.; Dittus, R.S.; Pierce, R.A. Implementation of a Telephone Postoperative Clinic in an Integrated Health System. J. Am. Coll. Surg. 2016, 223, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Seron, P.; Oliveros, M.J.; Gutierrez-Arias, R.; Fuentes-Aspe, R.; Torres-Castro, R.C.; Merino-Osorio, C.; Nahuelhual, P.; Inostroza, J.; Jalil, Y.; Solano, R.; et al. Effectiveness of Telerehabilitation in Physical Therapy: A Rapid Overview. Phys. Ther. 2021, 101, pzab053. [Google Scholar] [CrossRef] [PubMed]
- Colomina, J.; Drudis, R.; Torra, M.; Pallisó, F.; Massip, M.; Vargiu, E.; Nadal, N.; Fuentes, A.; Ortega, M.; Miralles, F.; et al. Implementing mHealth-Enabled Integrated Care for Complex Chronic Patients With Osteoarthritis Undergoing Primary Hip or Knee Arthroplasty: Prospective, Two-Arm, Parallel Trial. J. Med. Internet Res. 2021, 23, e28320. [Google Scholar] [CrossRef]
- Gilboa, Y.; Maeir, T.; Karni, S.; Eisenberg, M.E.; Liebergall, M.; Schwartz, I.; Kaufman, Y. Effectiveness of a tele-rehabilitation intervention to improve performance and reduce morbidity for people post hip fracture—Study protocol for a randomized controlled trial. BMC Geriatr. 2019, 19, 135. [Google Scholar] [CrossRef]
- Hosseiniravandi, M.; Kahlaee, A.H.; Karim, H.; Ghamkhar, L.; Safdari, R. Home-based telerehabilitation software systems for remote supervising: A systematic review. Int. J. Technol. Assess Health Care 2020, 36, 113–125. [Google Scholar] [CrossRef]
- Busso, C.; Castorina, G.; Di Monaco, M.; Rodriguez, D.; Mahdavi, H.; Balocco, S.; Trucco, M.; Conti, M.; Castagna, A.; Minetto, M.A. Effectiveness of a home-based telerehabilitation system in patients after total hip arthroplasty: Study protocol of a randomized controlled trial. Trials 2020, 21, 852. [Google Scholar] [CrossRef]
- Sadiq, S.; Ahmad, A.; Ahmed, A.; Khan, I.; Asim, H.M.; Aziz, A. Role of tele-rehabilitation in patients following total hip replacement: Systematic review of clinical trials. J. Pak. Med. Assoc. 2022, 72, 101–107. [Google Scholar]
- Mark-Christensen, T.; Thorborg, K.; Kallemose, T.; Bandholm, T. Physical rehabilitation versus no physical rehabilitation after total hip and knee arthroplasties: Protocol for a pragmatic, randomized, controlled, superiority trial (The DRAW1 trial). F1000Res 2021, 10, 146. [Google Scholar] [CrossRef]
- Vesterby, M.S.; Pedersen, P.U.; Laursen, M.; Mikkelsen, S.; Larsen, J.; Søballe, K.; Jørgensen, L.B. Telemedicine support shortens length of stay after fast-track hip replacement. Acta Orthop. 2017, 88, 41–47. [Google Scholar] [CrossRef]
- Saunders, R.; Seaman, K.; Emery, L.; Bulsara, M.; Ashford, C.; McDowall, J.; Gullick, K.; Ewens, B.; Sullivan, T.; Foskett, C.; et al. Comparing an eHealth Program (My Hip Journey) With Standard Care for Total Hip Arthroplasty: Randomized Controlled Trial. JMIR Rehabil. Assist. Technol. 2021, 8, e22944. [Google Scholar] [CrossRef] [PubMed]
- Eichler, S.; ReMove-It Study Group; Rabe, S.; Salzwedel, A.; Müller, S.; Stoll, J.; Tilgner, N.; John, M.; Wegscheider, K.; Mayer, F.; et al. Effectiveness of an interactive telerehabilitation system with home-based exercise training in patients after total hip or knee replacement: Study protocol for a multicenter, superiority, no-blinded randomized controlled trial. Trials 2017, 18, 438. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.; Bourke, M.; Crossley, K.; Russell, T. Telerehabilitation is non-inferior to usual care following total hip replacement. Physiotherapy 2020, 107, 19–27. [Google Scholar] [CrossRef]
- Pelle, T.; Bevers, K.; van der Palen, J.; van den Hoogen, F.H.J.; van den Ende, C.H.M. Development and evaluation of a tailored e-self-management intervention (dr. Bart app) for knee and/or hip osteoarthritis: Study protocol. BMC Musculoskelet. Disord. 2019, 20, 398. [Google Scholar] [CrossRef]
- Pelle, T.; Bevers, K.; van der Palen, J.; van den Hoogen, F.H.J.; van den Ende, C.H.M. Effect of the dr. Bart application on healthcare use and clinical outcomes in people with osteoarthritis of the knee and/or hip in the Netherlands; a randomized controlled trial. Osteoarthr. Cartil. 2020, 28, 418–427. [Google Scholar] [CrossRef]
- Alexandre, D.J.A.; Ramalho, G.S.; Civile, V.T.; Carvas Junior, N.; Cury Fernandes, M.B.; Cacione, D.G.; Trevisani, V.F.M. Telerehabilitation versus conventional face-to-face land-based exercises following hip or knee arthroplasty. Cochrane Database Syst. Rev. 2021, 11, CD014931. [Google Scholar]
- Patel, B.; Thind, A. Usability of Mobile Health Apps for Postoperative Care: Systematic Review. JMIR Perioper. Med. 2020, 3, e19099. [Google Scholar] [CrossRef]
- Nelson, M.; Russell, T.; Crossley, K.; Bourke, M.; McPhail, S. Cost-effectiveness of telerehabilitation versus traditional care after total hip replacement: A trial-based economic evaluation. J. Telemed. Telecare 2021, 27, 359–366. [Google Scholar] [CrossRef]
- Asiri, A.; AlBishi, S.; AlMadani, W.; ElMetwally, A.; Househ, M. The Use of Telemedicine in Surgical Care: A Systematic Review. Acta Inform. Med. 2018, 26, 201–206. [Google Scholar] [CrossRef]
- Wang, X.; Hunter, D.J.; Vesentini, G.; Pozzobon, D.; Ferreira, M.L. Technology-assisted rehabilitation following total knee or hip replacement for people with osteoarthritis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 506. [Google Scholar] [CrossRef]
- Byra, J.; Czernicki, K. The Effectiveness of Virtual Reality Rehabilitation in Patients with Knee and Hip Osteoarthritis. J. Clin. Med. 2020, 9, 2639. [Google Scholar] [CrossRef]
- Dawes, A.J.; Lin, A.Y.; Varghese, C.; Russell, M.M.; Lin, A.Y. Mobile health technology for remote home monitoring after surgery: A meta-analysis. Br. J. Surg. 2021, 108, 1304–1314. [Google Scholar] [CrossRef]
- Negrini, S.; Kiekens, C.; Bernetti, A.; Capecci, M.; Ceravolo, M.G.; Lavezzi, S.; Zampolini, M.; Boldrini, P. Telemedicine from research to practice during the pandemic. “Instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur. J. Phys. Rehabil. Med. 2020, 56, 327–330. [Google Scholar] [CrossRef]
- Dangi, R.; Lalwani, P.; Choudhary, G.; You, I.; Pau, G. Study and Investigation on 5G Technology: A Systematic Review. Sensors 2021, 22, 26. [Google Scholar] [CrossRef]
- Shamsabadi, A.; Pashaei, Z.; Karimi, A.; Mirzapour, P.; Qaderi, K.; Marhamati, M.; Barzegary, A.; Fakhfouri, A.; Mehraeen, E.; SeyedAlinaghi, S.; et al. Internet of things in the management of chronic diseases during the COVID-19 pandemic: A systematic review. Health Sci. Rep. 2022, 5, e557. [Google Scholar] [CrossRef]
- Fatoum, H.; Hanna, S.; Halamka, J.D.; Sicker, D.C.; Spangenberg, P.; Hashmi, S.K. Blockchain Integration with Digital Technology and the Future of Health Care Ecosystems: Systematic Review. J. Med. Internet Res. 2021, 23, e19846. [Google Scholar] [CrossRef]
- Gunter, R.L.; Chouinard, S.; Fernandes-Taylor, S.; Wiseman, J.T.; Clarkson, S.; Bennett, K.; Greenberg, C.C.; Kent, K.C. Current Use of Telemedicine for Post-Discharge Surgical Care: A Systematic Review. J. Am. Coll. Surg. 2016, 222, 915–927. [Google Scholar] [CrossRef]
- Docpulse Telemedicine System. Available online: https://docpulse.com/products/telemedicine/ (accessed on 4 May 2022).
- EngageConsult Software. Available online: https://www.engagehealth.uk/engage-consult/ (accessed on 4 May 2022).
- Webcamconsult Teleconsultation System. Available online: https://webcamconsult.com/en/ (accessed on 4 May 2022).
- Comarch Medcall Software. Available online: https://www.comarch.com/healthcare/med-hub/comarch-medcall-new-system-for-videoconsultation-and-teleconsultation/ (accessed on 4 May 2022).
- Ringcentral Software. Available online: https://www.ringcentral.com/video.html (accessed on 4 May 2022).
- Teledochealth Software. Available online: https://www.teladochealth.com/ (accessed on 4 May 2022).
- Doxy Software. Available online: https://doxy.me/en/ (accessed on 4 May 2022).
- eClinic by Healthcare Communications Software. Available online: https://healthcare-communications.com/solutions/appointment-management/eclinic-video-consultations/ (accessed on 4 May 2022).
- Cliniko Software. Available online: https://www.cliniko.com/features/appointments/telehealth/ (accessed on 4 May 2022).
- Medfile Software. Available online: https://www.medfile.pl (accessed on 4 May 2022).
- Telemedi Teleconsultation System. Available online: https://telemedi.com (accessed on 4 May 2022).
- Aurero Software. Available online: https://aurero.com (accessed on 4 May 2022).
- Proassist Software. Available online: https://proassist.pl/telemedycyna/ (accessed on 4 May 2022).
- Mira Software Platform. Available online: https://www.mirarehab.com/product/ (accessed on 4 May 2022).
- Kinex Connect Rehabilitation System. Available online: https://kinexmedical.com/ (accessed on 4 May 2022).
- iSalus Othopaedic EHR. Available online: https://isalushealthcare.com/products/orthopaedic-ehr/ (accessed on 4 May 2022).
- WizeCare Connect System. Available online: https://wizecare.com/ (accessed on 4 May 2022).
- VERA Animated Avatar Rehabilitation System. Available online: https://orthofeed.com/2019/05/09/the-1-advantage-for-tha-or-tka-tele-rehabilitation/ (accessed on 4 May 2022).
- Neuroforma System. Available online: https://www.neuro-forma.com/science/ (accessed on 4 May 2022).
- Comarch Wristband. Available online: https://www.comarch.com/healthcare/products/remote-medical-care/remote-care-services/wristband/ (accessed on 4 May 2022).
- Sidly Wristband. Available online: https://sidly.eu/en/ (accessed on 4 May 2022).
- Telecare24 Wrist Band with Telecare System. Available online: https://www.telecare24.co.uk/ (accessed on 4 May 2022).
- MobiCare Telecare System. Available online: https://www.satisgps.com/aktualnosci/mobicare-system-monitorowania-i-teleopieki-dla-seniorow/ (accessed on 4 May 2022).
- NOVAMA Wristband Telecare System. Available online: https://novama.pl/samorzady?gclid=CjwKCAjwopWSBhB6EiwAjxmqDYjXKE-5W1QTUNr46zBQxmV9UBx4jYz3JDjl6W40XLbLGCW4ZOPbGxoC2gsQAvD_BwEa (accessed on 4 May 2022).
- Rahman, M.F.; Wen, Y.; Xu, H.; Tseng, T.-L.; Akundi, S. Data mining in telemedicine. In Advances in Telemedicine for Health Monitoring: Technologies, Design and Applications; IET Digital Library: London, UK, 2020; pp. 103–131. [Google Scholar] [CrossRef]
- Kalron, A.; Tawil, H.; Peleg-Shani, S.; Vatine, J.J. Effect of telerehabilitation on mobility in people after hip surgery: A pilot feasibility study. Int. J. Rehabil. Res. 2018, 41, 244–250. [Google Scholar] [CrossRef]
- Fan, Y.J.; Yin, Y.H.; Xu, L.D.; Zeng, Y.; Wu, F. IoT-Based Smart Rehabilitation System. IEEE Trans. Ind. Inform. 2014, 10, 1568–1577. [Google Scholar]
- Huis In’t Veld, R.; Peters, A.; Vollenbroek-Hutten, M.; Hermens, H.; van den Hoven, C. Patient Needs for an Ambulant Dislocation Alert System Following Total Hip Arthroplasty. Telemed. J. e-Health 2018, 24, 386–394. [Google Scholar] [CrossRef]
- Ministry of Foreign Affairs Republic of Poland Communicate on Tech Products. Available online: https://www.gov.pl/web/diplomacy/teleneuroforma-by-titanis-meden-inmed (accessed on 4 May 2022).
- Faria, C.; Silva, J.; Campilho, A. Rehab@home: A tool for home-based motor function rehabilitation. Disabil. Rehabil. Assist. Technol. 2015, 10, 67–74. [Google Scholar] [CrossRef]
- Esculier, J.F.; Vaudrin, J.; Bériault, P.; Gagnon, K.; Trem-blay, L.E. Home-based balance training programme using Wii Fit with balance board for Parkinson’s disease: A pilot study. J. Rehabil. Med. 2012, 44, 144–150. [Google Scholar]
- Yong, J.L.; Soon, Y.T.; Xu, D.; Thia, E.; Pei, F.C.; Kuah, C.W.; Kong, K.H. A feasibility study using interactive commercial off-the-shelf computer gaming in upper limb rehabilitation in patients after stroke. J. Rehabil. Med. 2010, 42, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Sugarman, H.; Weisel-Eichler, A.; Burstin, A.; Brown, R. Use of the Wii Fit system for the treatment of balance problems in the elderly: A feasibility study. In Proceedings of the IEEE Virtual Rehabilitation International Conference, Haifa, Israel, 29 June–2 July 2009; pp. 111–116. [Google Scholar]
- Physical Rehabilitation Assistant for Patients. Available online: https://rehabee.pl/ (accessed on 13 April 2021).
- NHS Digital. Advice on Using Video Consultation Systems, Assured Video Consultation Systems. 2020. Available online: https://digital.nhs.uk/services/gp-it-futures-systems/approved-econsultation-systems (accessed on 4 May 2022).
- Guide of Telemedicine Working Group Foundation. Available online: http://telemedycyna-poradnik.pl/api/file/events/rtgr/poradnik_dla_lekarzy-1.pdf (accessed on 4 May 2022).
- Raja, J.M.; Elsakr, C.; Roman, S.; Cave, B.; Pour-Ghaz, I.; Nanda, A.; Maturana, M.; Khouzam, R.N. Apple Watch, Wearables, and Heart Rhythm: Where do we stand? Ann. Transl. Med. 2019, 7, 417. [Google Scholar] [CrossRef]
- da Silva, J.M.; Derogarian, F.; Canas Ferreira, J.; Grade Tavares, V. Chapter 10—Wearable sensor networks for human gait. In Wearable Technologies and Wireless Body Sensor Networks for Healthcare; Healthcare Technologies: London, UK, 2019; pp. 321–360. [Google Scholar]
- Majumder, S.; Mondal, T.; Deen, M.J. Wearable Sensors for Remote Health Monitoring. Sensors 2017, 12, 130. [Google Scholar] [CrossRef]
- Henriksen, A.; Mikalsen, H.M.; Woldaregay, A.Z.; Muzny, M.; Hartvigsen, G.; Hopstock, L.A.; Grimsgaard, S. Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer Wrist-Worn Wearables. J. Med. Internet Res. 2018, 22, e110. [Google Scholar] [CrossRef]
- Yetisen, A.K.; Martinez-Hurtado, J.L.; Ünal, B.; Khademhosseini, A.; Butt, H. Wearables in Medicine. Adv. Mater. 2018, 11, e1706910. [Google Scholar] [CrossRef]
- Singhal, A.; Cowie, M.R. The Role of Wearables in Heart Failure. Curr. Heart Fail. Rep. 2020, 17, 125–132. [Google Scholar] [CrossRef]
- Dunn, J.; Runge, R.; Snyder, M. Wearables and the medical revolution. Per. Med. 2018, 15, 429–448. [Google Scholar] [CrossRef]
- Reeder, B.; Chung, J.; Lyden, K.; Winters, J.; Jankowski, C.M. Older women’s perceptions of wearable and smart home activity sensors. Inform. Health Soc. Care 2020, 45, 96–109. [Google Scholar] [CrossRef]
- Yen, H.Y. Smart wearable devices as a psychological intervention for healthy lifestyle and quality of life: A randomized controlled trial. Qual. Life Res. 2021, 30, 791–802. [Google Scholar] [CrossRef]
- Varga, P.; Peto, J.; Franko, A.; Balla, D.; Haja, D.; Janky, F.; Soos, G.; Ficzere, D.; Maliosz, M.; Toka, L. 5G support for Industrial IoT Applications—Challenges, Solutions, and Research gaps. Sensors 2020, 4, 828. [Google Scholar] [CrossRef]
- Attaran, M. The impact of 5G on the evolution of intelligent automation and industry digitization. J. Ambient Intell. Humaniz. Comput. 2021, 21, 1–17. [Google Scholar] [CrossRef]
- Li, D. 5G and intelligence medicine-how the next generation of wireless technology will reconstruct healthcare? Precis. Clin. Med. 2019, 2, 205–208. [Google Scholar] [CrossRef]
- Laplante, P.A.; Kassab, M.; Laplante, N.L.; Voas, J.M. Building Caring Healthcare Systems in the Internet of Things. IEEE Syst. J. 2018, 12, 3030–3037. [Google Scholar] [CrossRef]
- Kelly, J.T.; Campbell, K.L.; Gong, E.; Scuffham, P. The Internet of Things: Impact and Implications for Health Care Delivery. J. Med. Internet Res. 2020, 10, e20135. [Google Scholar] [CrossRef]
- Ahad, A.; Tahir, M.; Aman, S.M.; Ahmed, K.I.; Mughees, A.; Numani, A. Technologies Trend towards 5G Network for Smart Health-Care Using IoT: A Review. Sensors 2020, 21, 4047. [Google Scholar] [CrossRef]
- Eichler, S.; Salzwedel, A.; Rabe, S.; Mueller, S.; Mayer, F.; Wochatz, M.; Hadzic, M.; John, M.; Wegscheider, K.; Völler, H. The Effectiveness of Telerehabilitation as a Supplement to Rehabilitation in Patients After Total Knee or Hip Replacement: Randomized Controlled Trial. JMIR Rehabil. Assist. Technol. 2019, 7, e14236. [Google Scholar] [CrossRef]
- Update on Physiotherapy Rehabilitation after Total Knee or Hip Replacement: OHTAC Recommendation. Available online: http://www.hqontario.ca/Portals/0/Documents/evidence/reports/recommendation-knee-hip-replacement-140310-en.pdf (accessed on 10 April 2021).
- Dias Correia, F.; Nogueira, A.; Magalhães, I.; Guimarães, J.; Moreira, M.; Barradas, I.; Molinos, M.; Teixeira, L.; Pires, J.; Seabra, R.; et al. Digital versus conventional rehabilitation after total hip arthroplasty: A single-center, parallel-group pilot study. JMIR Rehabil. Assist. Technol. 2019, 6, e14523. [Google Scholar] [CrossRef]
- Mishra, R.; Narayanan, M.D.K.; Umana, G.E.; Montemurro, N.; Chaurasia, B.; Deora, H. Virtual Reality in Neurosurgery: Beyond Neurosurgical Planning. Int. J. Environ. Res. Public Health. 2022, 19, 1719. [Google Scholar] [CrossRef]
- Barsom, E.Z.; Graafland, M.; Schijven, M.P. Systematic review on the effectiveness of augmented reality applications in medical training. Surg. Endosc. 2016, 30, 4174–4183. [Google Scholar] [CrossRef]
- Barteit, S.; Lanfermann, L.; Bärnighausen, T.; Neuhann, F.; Beiersmann, C. Augmented, Mixed, and Virtual Reality-Based Head-Mounted Devices for Medical Education: Systematic Review. JMIR Serious Games 2021, 9, e29080. [Google Scholar] [CrossRef]
- Montemurro, N. Telemedicine: Could it represent a new problem for spine surgeons to solve? Glob. Spine J. 2022, 12, 1306–1307. [Google Scholar] [CrossRef]
- Telemedicine Working Group. Available online: http://telemedycyna-poradnik.pl/ (accessed on 4 September 2022).
- Clotman, K.; Twickler, M.B. Diabetes or endocrinopathy admitted in the COVID-19 ward. Eur. J. Clin. Investig. 2020, 50, e13262. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | ||
|---|---|---|
| Technological area | Teleconsultation | [13,14,15,16,17,18,19,20,21,22] |
| Telerehabilitation | [15,16,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37] | |
| Telemonitoring | [13,14,15,20,22,30,31,33,35,38,39,40,41,42,43] | |
| Stakeholders in the care process | Family physician | [20] |
| Health care team | [27] | |
| Hospital surgical team | [20] | |
| Nurse | [13] | |
| Occupational therapist | [21] | |
| Orthopedic surgeon | [17,18,25] | |
| Patient | [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,43] | |
| Physician | [13,24,38] | |
| Physiotherapist | [15,16,19,22,23,24,25,26,28,34,43] | |
| Policymaker | [25] | |
| Primary caregiver | [21] | |
| Rehabilitation center | [28] | |
| Social worker | [20] | |
| Surgeon’s administrative assistant | [17] |
| Google Search Phrase | Results | Language of Search |
|---|---|---|
| “Software for medical video consultation” | [44,45,46,47,48,49,50,51,52] | EN |
| [53,54,55,56] | PL | |
| “Software for orthopedic telerehabilitation’ | [57,58,59,60,61] | EN |
| [62] | PL | |
| “Telemetric wrist band with collapse function” | [63,64] | EN |
| “Telecare monitoring” | [65,66] | EN |
| [67] | PL |
| Medical Area | Innovation | Data Type and Usage | Telemedicine Technology Proposed by Our Research Team |
|---|---|---|---|
| Physiotherapy | Telerehabilitation program for remote self-rehabilitation at patient’s home | Qualitative and quantitative data. Personal data, electronic health records (EHR), files with medical tests results, measurement results from wearable devices (e.g., basic life parameters, parameters and pictures of the exercises performed, gait analysis, number of steps, percentage of physical, cognitive performance, number and time of patient fall), with the use of written data, sound, images, and movie. Data can be gathered and analyzed in real-time by medical specialists or/and can be analyzed by AI, compared with algorithms and automatic feedback given to the patient. | Telerehabilitation systems using AI technology in wearable and visual technologies collecting, processing, and presenting data from physical activities which were ordered by doctors and physiotherapists; system enabling physiotherapists to control and moderate ordered activities and monitoring the results. |
| Outpatient specialist care | Remote medical consultations with specialist personnel: nurse, doctor, physiotherapist | Qualitative and quantitative data. Personal data, electronic health records (EHR), files with medical tests results, with the use of written data, sound, online or recorded movie. Data can be gathered and analyzed real-time or/and can be analyzed by AI, compared with algorithms and automatic feedback given to the patient. | Software, application for conducting remote medical patient–specialist video-consultation with keeping EHR. |
| Telemonitoring | Telecare wrist band with collapse and activity sensor | Qualitative and quantitative data. Personal data, electronic health records (EHR), measurement results from wearable devices as basic life parameters, parameters and pictures of the exercises performed, gait analysis, number of steps, percentage of physical, cognitive performance, number and time of patient fall, with the use of written data (numbers, alerts, communicates) via sound and database files send to monitoring system. Data can be gathered and analyzed real-time or/and can be analyzed by AI, compared with algorithms and automatic feedback given to the patient. | Telemetric wrist bands with connection to medical centers monitoring patient’s condition and with alarm system to patient’s guardian. |
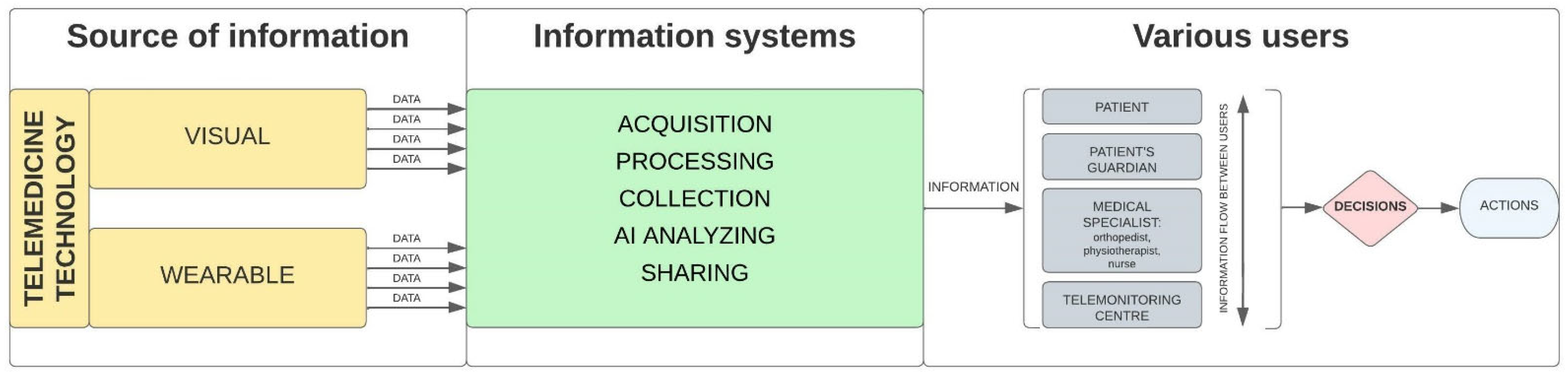
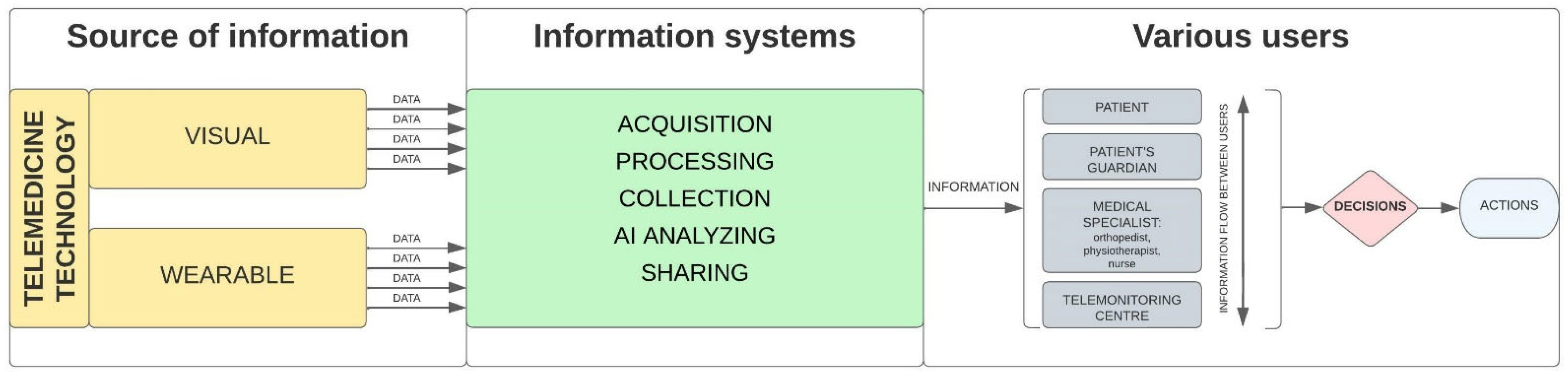
| Technology Function | Technology Example |
|---|---|
| Obtaining information | Measuring sensors, video cameras, radars, and data collecting sensors (wearable and visual). |
| Information processing | Artificial Intelligence (AI) technologies, where as a result, we obtain a statement and indication of, i.e., image recognition, critical points, good/bad results, repeated errors, and progress. Medical software, applications, databases appropriate for safe and easy electronic medical data management. |
| Presenting information | Wireless and internet communication systems and applications using, i.a., charts, summaries, alerts including light signaling in wireless and internet communication systems including sound and light signaling, individually designed to the technology recipient/user needs and perception possibilities: to patient, to patient’s guardian, to medical doctor, to physiotherapist, to nurse, telemonitoring center staff. |
| Communication | Software and applications using secure IT connection and databases for remote patient-specialist medical consultations. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamecka, K.; Foti, C.; Gawiński, Ł.; Matejun, M.; Rybarczyk-Szwajkowska, A.; Kiljański, M.; Krochmalski, M.; Kozłowski, R.; Marczak, M. Telemedicine Technologies Selection for the Posthospital Patient Care Process after Total Hip Arthroplasty. Int. J. Environ. Res. Public Health 2022, 19, 11521. https://doi.org/10.3390/ijerph191811521
Kamecka K, Foti C, Gawiński Ł, Matejun M, Rybarczyk-Szwajkowska A, Kiljański M, Krochmalski M, Kozłowski R, Marczak M. Telemedicine Technologies Selection for the Posthospital Patient Care Process after Total Hip Arthroplasty. International Journal of Environmental Research and Public Health. 2022; 19(18):11521. https://doi.org/10.3390/ijerph191811521
Chicago/Turabian StyleKamecka, Karolina, Calogero Foti, Łukasz Gawiński, Marek Matejun, Anna Rybarczyk-Szwajkowska, Marek Kiljański, Marek Krochmalski, Remigiusz Kozłowski, and Michał Marczak. 2022. "Telemedicine Technologies Selection for the Posthospital Patient Care Process after Total Hip Arthroplasty" International Journal of Environmental Research and Public Health 19, no. 18: 11521. https://doi.org/10.3390/ijerph191811521
APA StyleKamecka, K., Foti, C., Gawiński, Ł., Matejun, M., Rybarczyk-Szwajkowska, A., Kiljański, M., Krochmalski, M., Kozłowski, R., & Marczak, M. (2022). Telemedicine Technologies Selection for the Posthospital Patient Care Process after Total Hip Arthroplasty. International Journal of Environmental Research and Public Health, 19(18), 11521. https://doi.org/10.3390/ijerph191811521