
Work-Related Injuries among Insured Construction Workers Presenting to a Swiss Adult Emergency Department: A Retrospective Study (2016–2020)

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Design
2.2. Database Search Criteria
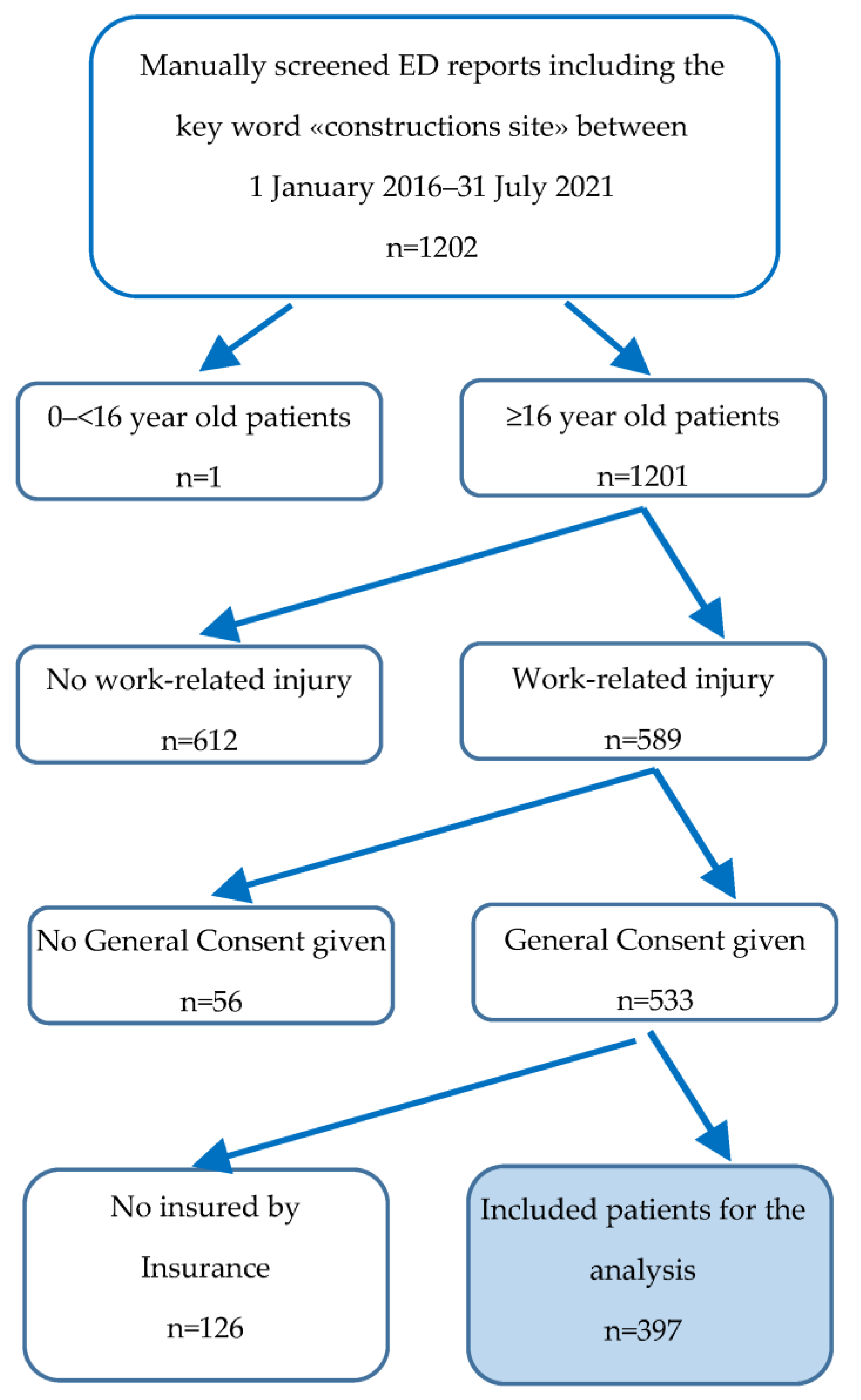
2.3. Recruitment of Patients
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Demographic and Clinical Data
- 1.
- General patient data:
- Gender
- Age
- 2.
- Admission and discharge data:
- Route of admission
- Date of admission: weekday, month, season
- Time of admission (morning/afternoon/evening/night and whether immediately after the accident to X number of days after the accident)
- Triage levels
- Treatment area in the ER and whether trauma room treatment took place
- Route of discharge
- 3.
- Admission department and hospitalization duration if hospitalized
- Anamnestic data:
- Occupation/activity performed
- Accident mechanism
- Fall (height, object causing the fall, landing area)
- machine handling/driving a transport vehicle
- Working with manual instruments
- transport by hand (lift weight)
- Moving (walking, running, climbing, tripping)
- Contaminating substances/explosion, burn, electrical contact
- Being hit by a car, being run over
- Entrapment/impact against object
- Cut on an object
- Objects causing accident:
- Terrain
- Material extraction
- Electricity
- Machines/manual instruments
- Conveyor system
- Means of transportation (driving vehicle, trailer)
- Harmful, flammable or explosive substances/gases and dust
- Foreign body splinters
- Humans and animals
- Location of accident:
- Building construction site
- Road construction site
- Excavation pit
- 4.
- Clinical and preclinical data:
- Injury type (simple injury, combined injury, polytrauma)
- Type of injury:
- Wound laceration, incl. internal organs, pneumothorax
- Cerebral commotio, cerebral hemorrhage
- Distortion, contusion, crush trauma
- Closed or open fracture, dislocation, amputation
- Burn, frostbite
- Chemical burns, electric shock, chemical substances, etc.
- Infection, poisoning, irritation of mucous membranes
- Foreign body penetration, foreign body irritation
- Treatment method: Conservative, surgical, minimally invasive, death in emergency room
- Injured body site: Head, neck, spine, thorax (and thoracic organs), back, abdomen (and abdominal organs), pelvis, shoulder, upper arm, elbow, forearm, wrist, hand, hip joint, thigh, knee joint, lower leg, foot
2.5. Statistical Analysis
2.6. Ethical Approval
2.7. Definitions
- Urgency level 1 (acute emergency, immediate treatment): Health disorder or imminent birth that may result in the death of the patient or the loss of a limb, organ, or fetus if not treated immediately.
- Urgency level 2 (emergency, treatment within 20 min): Health disorder that is not life-threatening but could worsen within a short time.
- Urgency level 3 (moderately urgent emergency, treatment within 120 min): Health disorder for which time is not a critical factor. The patient’s condition is judged to be stable at the time of arrival.
- Urgency level 4 (non-urgent situation): Health condition judged stable that does not actually require emergency medical therapy.Location of accident: Different construction sites pose different hazards for workers.
- Building construction site: In order to avoid potentially fatal accidents, Suva recommends different rules: e.g., securing floor openings and fall edges from a fall height of 2 m immediately, daily scaffolding checks, operating cranes in accordance with regulations, and attaching loads safely [32].
- Road construction site: Traffic route and civil engineering site workers are exposed to different dangers such as passing vehicles and heavy machines and loads. Sufficient visibility and safe accesses are crucial [33].
- Excavation pit: During trenching and excavation work, it is essential to adhere to certain safety precautions. Otherwise, life danger can quickly arise. In particular, construction workers can be buried if an embankment is created too steeply or if the ground is additionally loaded by vehicles, for example [34].
3. Results
3.1. Patient Analysis
3.1.1. Age and Sex Distribution
3.1.2. Annual and Seasonal Distribution
3.1.3. Time and Day of Consultation
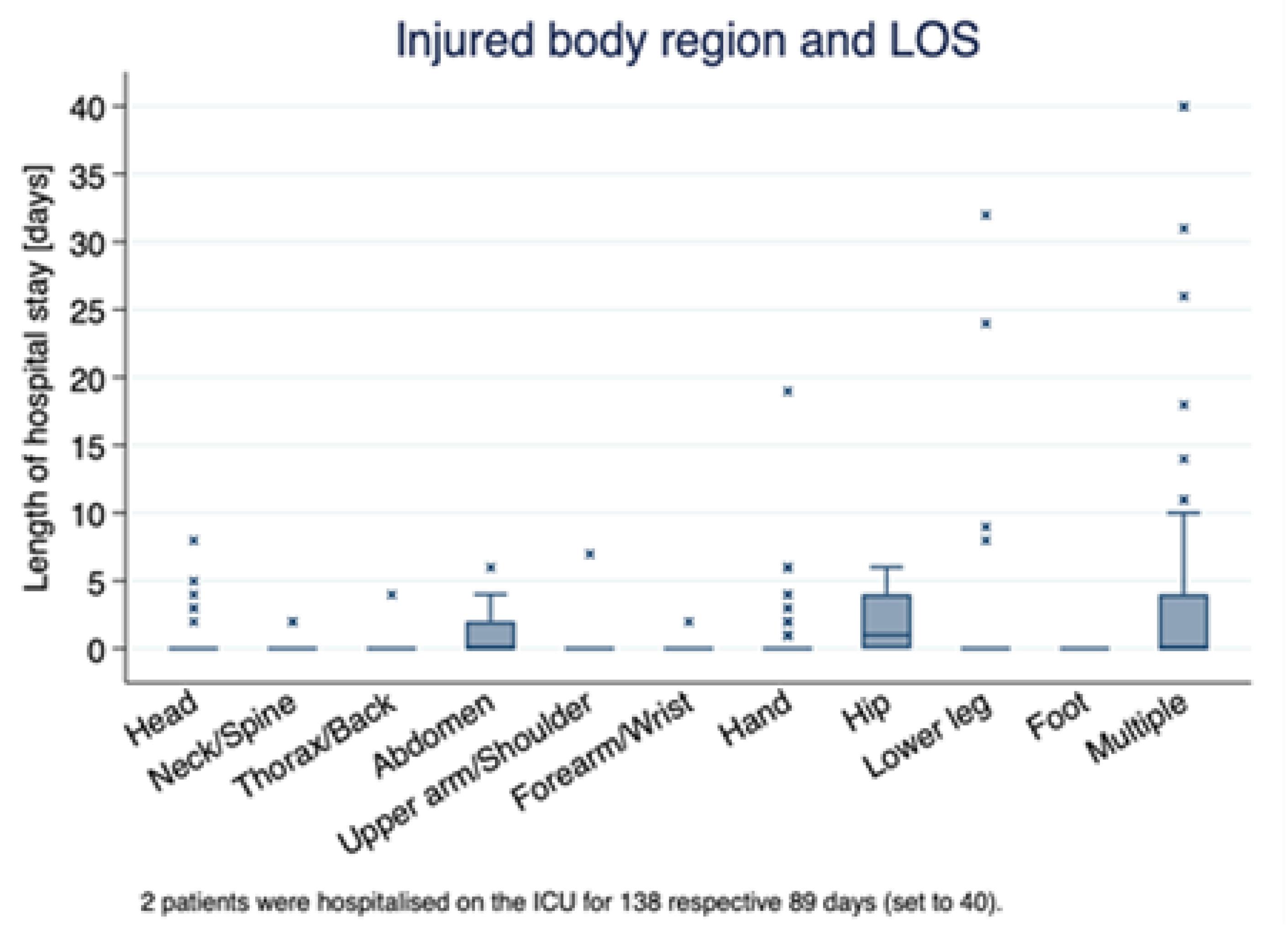
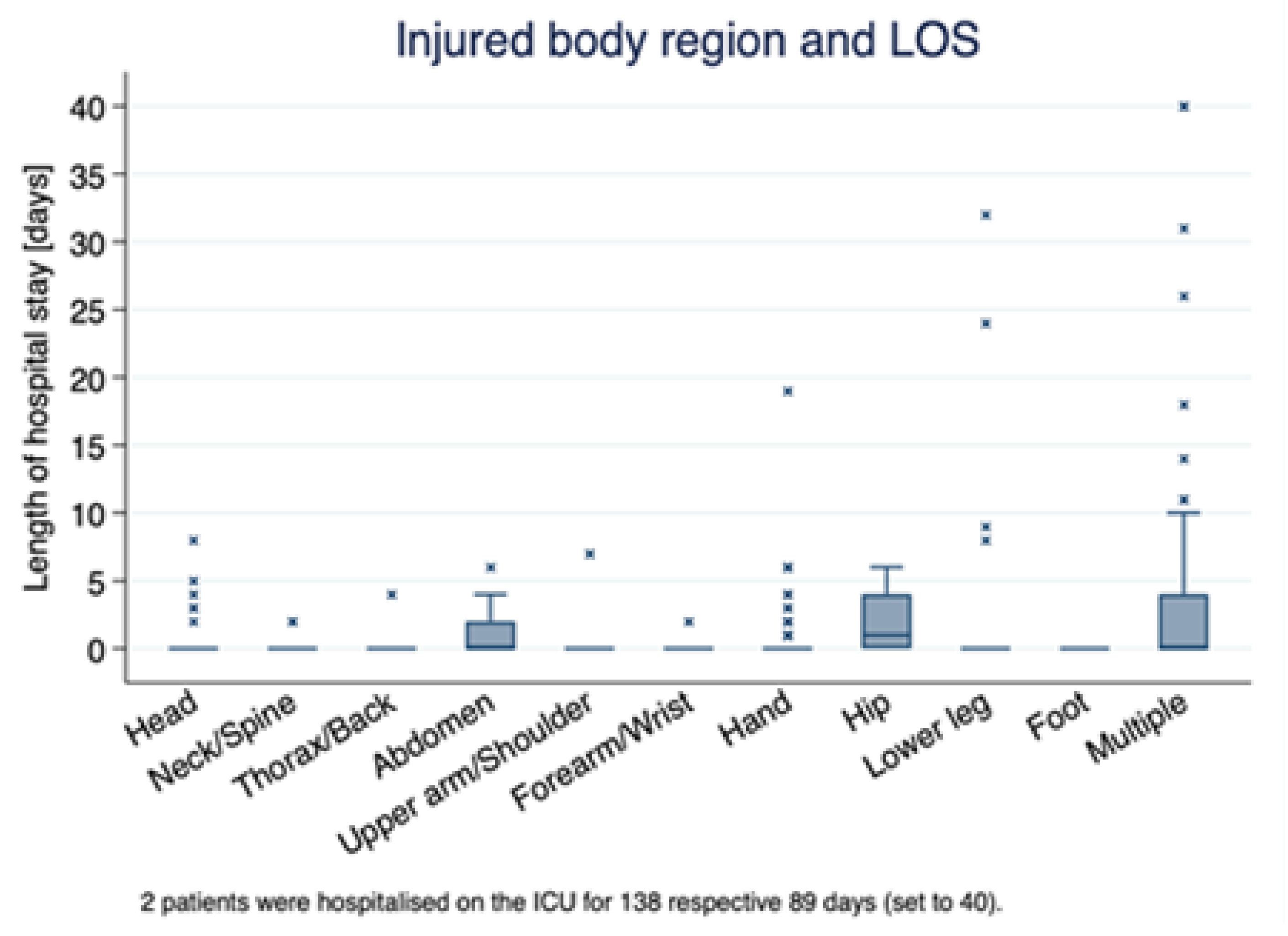
3.1.4. Location and Type of Injury
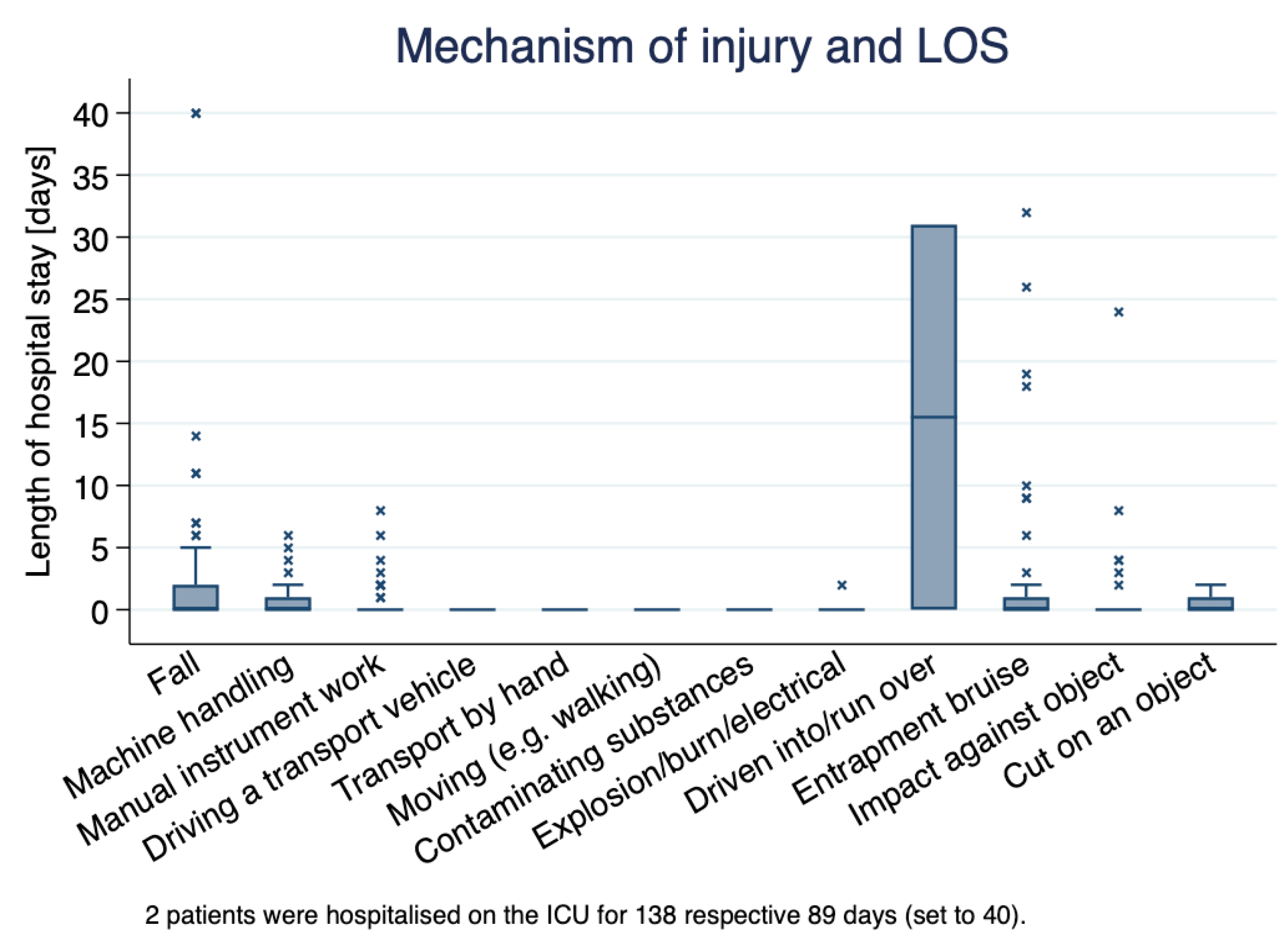
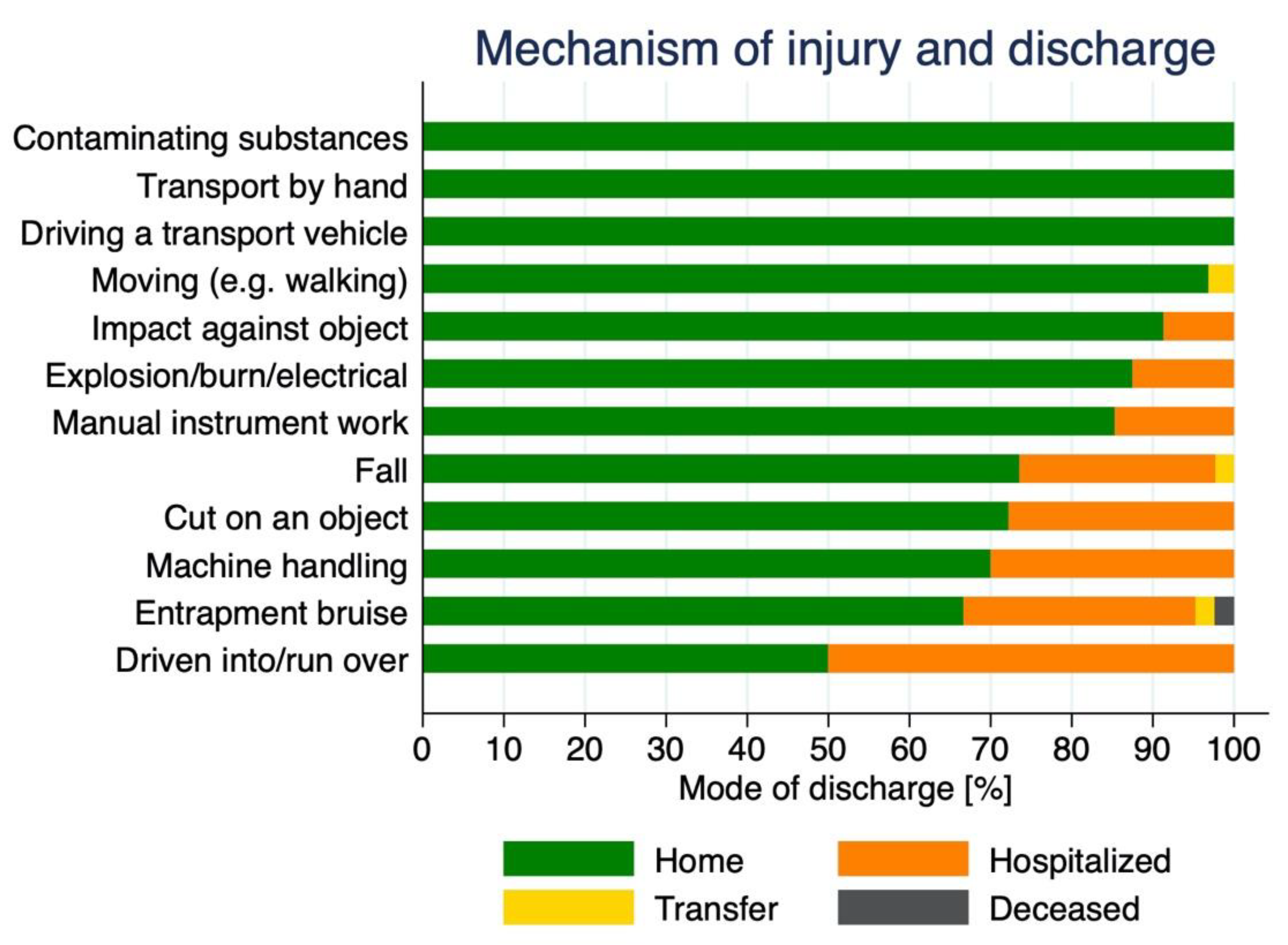
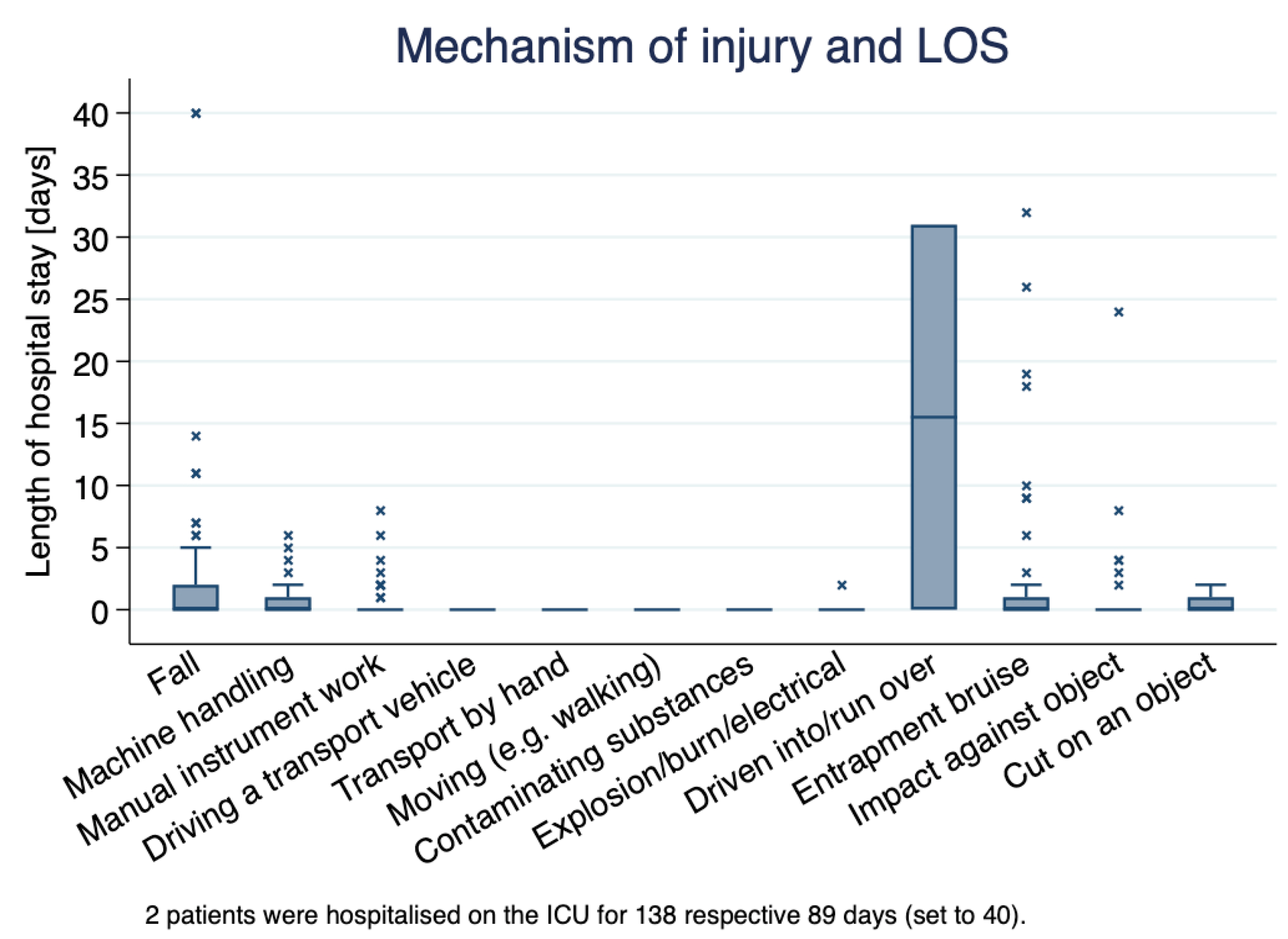
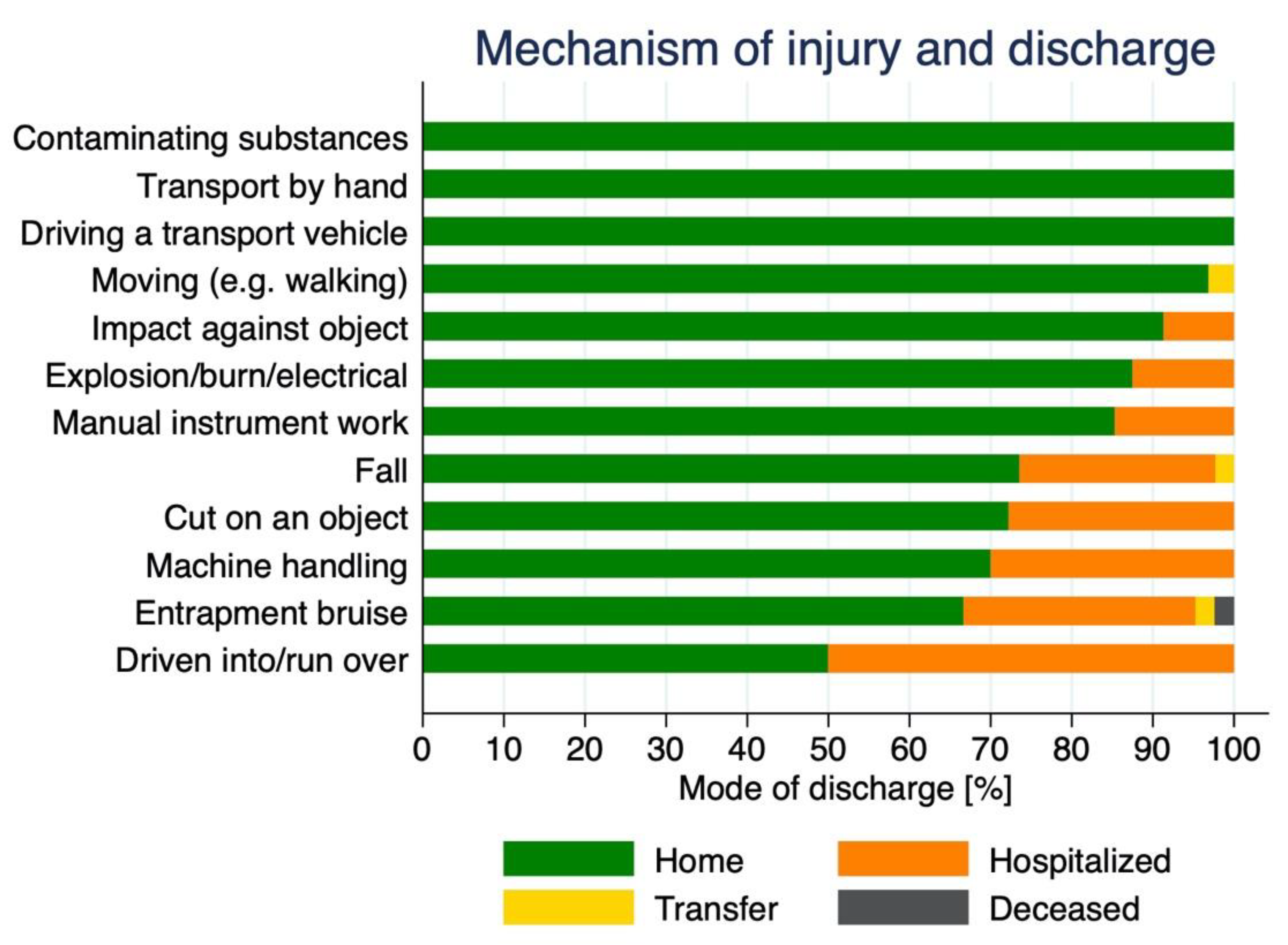
3.1.5. Mechanisms of Injury
3.1.6. Treatment
3.1.7. Admission and Discharge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gochfeld, M. Chronologic history of occupational medicine. J. Occup. Environ. Med. 2005, 47, 96–114. [Google Scholar] [CrossRef] [PubMed]
- Varacallo, M.; Knoblauch, D.K. Occupational Injuries and Workers’ Compensation Management Strategies; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- International Labour Office. Statistics of Occupational Injuries. Report III. In Proceedings of the Sixteenth International Conference of Labour Statisticians, Geneva, Switzerland, 6–15 October 1998. [Google Scholar]
- Tadros, A.; Sharon, M.; Chill, N.; Dragan, S.; Rowell, J.; Hoffman, S. Emergency department visits for work-related injuries. Am. J. Emerg. Med. 2018, 36, 1455–1458. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.S.; Wellman, H.M.; Sorock, G.S.; Warner, M.; Courtney, T.K.; Pransky, G.S.; Fingerhut, L.A. Injuries at work in the US adult population: Contributions to the total injury burden. Am. J. Public Health 2005, 95, 1213–1219. [Google Scholar] [CrossRef]
- International Labour Organization. Safety and Health at the Heart of the Future of Work Building on 100 Years of Experience; International Labour Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Leigh, J.P.; Waehrer, G.; Miller, T.R.; Keenan, C. Costs of occupational injury and illness across industries. Scand. J. Work Environ. Health 2004, 30, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Dhanabal, S.; Karuppiah, K.; Mani, K.K.; Rasdi, I.; Sambasivam, S. A Need for New Accident Theories in Malaysia. J. Public Health Med. 2016, 2, 1–4. [Google Scholar]
- Zakaria, N.H.; Malaysia, M.; Mansor, N.; Campus, D.; Abdullah, Z. Workplace Accident in Malaysia: Most Common Causes and Solutions. Bus. Manag. Rev. 2012, 2, 75–88. [Google Scholar]
- Rommel, A.; Varnaccia, G.; Lahmann, N.; Kottner, J.; Kroll, L.E. Occupational Injuries in Germany: Population-Wide National Survey Data Emphasize the Importance of Work-Related Factors. PLoS ONE 2016, 11, e0148798. [Google Scholar] [CrossRef]
- Jannadi, O.A.; Bu-Khamsin, M.S. Safety factors considered by industrial contractors in Saudi Arabia. Build. Environ. 2002, 37, 539–547. [Google Scholar] [CrossRef]
- Fabiano, B.; Currò, F.; Reverberi, A.P.; Pastorino, R. A statistical study on temporary work and occupational accidents: Specific risk factors and risk management strategies. Saf. Sci. 2008, 46, 535–544. [Google Scholar] [CrossRef]
- Unsar, S.; Sut, N. General assessment of the occupational accidents that occurred in Turkey between the years 2000 and 2005. Saf. Sci. 2009, 47, 614–619. [Google Scholar] [CrossRef]
- Perotti, S.; Russo, M.C. Work-related fatal injuries in Brescia County (Northern Italy), 1982 to 2015: A forensic analysis. J. Forensic Leg. Med. 2018, 58, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Errico, S.; Drommi, M.; Calamano, V.; Barranco, R.; Molinari, G.; Ventura, F. Fatal work-related injuries in the Genoa district (North-Western Italy): Forensic analysis of the 10-year period between 2011 and 2020. J. Forensic Leg. Med. 2022, 85, 102294. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kim, T.; Ahn, S. Loss assessment for sustainable industrial infrastructure: Focusing on bridge construction and financial losses. Sustainability 2020, 12, 5316. [Google Scholar] [CrossRef]
- Kim, J.M.; Ha, K.C.; Ahn, S.; Son, S.; Son, K. Quantifying the third-party loss in building construction sites utilizing claims payouts: A case study in South Korea. Sustainability 2020, 12, 10153. [Google Scholar] [CrossRef]
- Rivera, M.L.; Mora-Serrano, J.; Valero, I.; Oñate, E. Methodological—Technological Framework for Construction 4.0. Arch. Comput. Methods Eng. 2021, 28, 689–711. [Google Scholar] [CrossRef]
- Muñoz-La Rivera, F.; Vielma, J.C.; Herrera, R.F.; Gallardo, E. Waste Identification in the Operation of Structural Engineering Companies (SEC) According to Lean Management. Sustainability 2021, 13, 4249. [Google Scholar] [CrossRef]
- Sterud, T.; Tynes, T.; Mehlum, I.S.; Veiersted, K.B.; Bergbom, B.; Airila, A.; Johansson, B.; Brendler-Lindqvist, M.; Hviid, K.; Flyvholm, M.A. A systematic review of working conditions and occupational health among immigrants in Europe and Canada. BMC Public Health 2018, 18, 770. [Google Scholar] [CrossRef]
- Martinez-Rojas, M.; Gacto, M.J.; Vitiello, A.; Acampora, G.; Soto-Hidalgo, J.M. An Internet of Things and Fuzzy Markup Language Based Approach to Prevent the Risk of Falling Object Accidents in the Execution Phase of Construction Projects. Sensors 2021, 21, 6461. [Google Scholar] [CrossRef]
- Ahmed, S. Causes and effects of accident at construction site: A study for the construction industry in Bangladesh. Int. J. Sustain. Constr. Eng. Technol. 2019, 10, 18–40. [Google Scholar]
- Welch, L.S.; Hunting, K.L.; Murawski, J.A. Occupational injuries among construction workers treated in a major metropolitan emergency department in the United States. Scand. J. Work Environ. Health 2005, 31 (Suppl. S2), 11–21. [Google Scholar]
- Kartam, N.A.; Bouz, R.G. Fatalities and injuries in the Kuwaiti construction industry. Accid. Anal. Prev. 1998, 30, 805–814. [Google Scholar] [CrossRef]
- Cawley, J.C.; Homce, G.T. Occupational electrical injuries in the United States, 1992–1998, and recommendations for safety research. J. Safety Res. 2003, 34, 241–248. [Google Scholar] [CrossRef]
- Tappin, D.; Ashly, L.; Moore, D. Slip, trip and falls in residential construction. J. Cent. Hum. Factors Ergon. 2004, 5, 1174–1234. [Google Scholar]
- Ricco, M.; Vezzosi, L.; Balzarini, F.; Odone, A.; Signorelli, C. Air temperatures and occupational injuries in the construction industries: A report from Northern Italy (2000–2013). Ind. Health 2020, 58, 182–192. [Google Scholar] [CrossRef]
- Allison, R.W.; Hon, C.K.; Xia, B. Construction accidents in Australia: Evaluating the true costs. Saf. Sci. 2019, 120, 886–896. [Google Scholar] [CrossRef]
- Global Construction Perspectives and Oxford Economics. A Global Forecast for the Construction Industry to 2030; Global Construction Perspectives and Oxford Economics: London, UK, 2015. [Google Scholar]
- Munoz-La Rivera, F.; Mora-Serrano, J.; Onate, E. Factors Influencing Safety on Construction Projects (fSCPs): Types and Categories. Int. J. Environ. Res. Public Health 2021, 18, 884. [Google Scholar] [CrossRef]
- Triage. Schweizerische Gesellschaft für Notfall- und Rettungsmedizin (SGNOR). Available online: https://www.sgnor.ch/weitere-downloads (accessed on 24 May 2022).
- Acht Lebenswichtige Regeln für den Hochbau. Available online: https://www.suva.ch/de-CH/material/Lern-Lehrmittel/acht-lebenswichtige-regeln-fuer-den-hochbau-instruktionshilfe-88811d3497834978#sch-from-search#mark=hochbau (accessed on 16 May 2022).
- Neun Lebenswichtige Regeln für den Verkehrsweg- und Tiefbau. Available online: https://www.suva.ch/de-CH/material/Lern-Lehrmittel/neun-lebenswichtige-regeln-fuer-den-verkehrsweg-und-tiefbau-instruktionshilfe-88820d3909739097 (accessed on 26 May 2022).
- Gräben und Baugruben. Available online: https://www.suva.ch/de-CH/material/Checkliste/graeben-und-baugruben-67148d2833928339 (accessed on 26 May 2022).
- Kehlet, H.; Wilmore, D.W. Evidence-based surgical care and the evolution of fast-track surgery. Ann. Surg. 2008, 248, 189–198. [Google Scholar] [CrossRef]
- Sasse, N.; Ziaka, M.; Brockhus, L.; Muller, M.; Exadaktylos, A.K.; Klukowska-Rotzler, J. Trampolining Accidents in an Adult Emergency Department: Analysis of Trampolining Evolution Regarding Severity and Occurrence of Injuries. Int. J. Environ. Res. Public Health 2022, 19, 1212. [Google Scholar] [CrossRef]
- Campo, G.; Cegolon, L.; De Merich, D.; Fedeli, U.; Pellicci, M.; Heymann, W.C.; Pavanello, S.; Guglielmi, A.; Mastrangelo, G. The Italian National Surveillance System for Occupational Injuries: Conceptual Framework and Fatal Outcomes, 2002–2016. Int. J. Environ. Res. Public Health 2020, 17, 7631. [Google Scholar] [CrossRef]
- Al-Hajj, S.; Chahrour, M.A.; Nasrallah, A.A.; Hamed, L.; Pike, I. Physical trauma and injury: A multi-center study comparing local residents and refugees in Lebanon. J. Glob. Health 2021, 11, 17001. [Google Scholar] [CrossRef]
- Win, K.N.; Trivedi, A.; Lai, A.; Hasylin, H.; Abdul-Mumin, K. Non-fatal occupational accidents in Brunei Darussalam. Ind. Health 2021, 59, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Benavides, F.G.; Benach, J.; Muntaner, C.; Delclos, G.L.; Catot, N.; Amable, M. Associations between temporary employment and occupational injury: What are the mechanisms? Occup. Environ. Med. 2006, 63, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Nakata, A.; Ikeda, T.; Takahashi, M.; Haratani, T.; Hojou, M.; Swanson, N.G.; Fujioka, Y.; Araki, S. The prevalence and correlates of occupational injuries in small-scale manufacturing enterprises. J. Occup. Health 2006, 48, 366–376. [Google Scholar] [CrossRef]
- Binazzi, A.; Levi, M.; Bonafede, M.; Bugani, M.; Messeri, A.; Morabito, M.; Marinaccio, A.; Baldasseroni, A. Evaluation of the impact of heat stress on the occurrence of occupational injuries: Meta-analysis of observational studies. Am. J. Ind. Med. 2019, 62, 233–243. [Google Scholar] [CrossRef]
- Ricco, M. Air temperature exposure and agricultural occupational injuries in the Autonomous Province of Trento (2000–2013, North-Eastern Italy). Int. J. Occup. Med. Environ. Health 2018, 31, 317–331. [Google Scholar] [CrossRef] [Green Version]
- Ricco, M.; Garbarino, S.; Bragazzi, N.L. Migrant Workers from the Eastern-Mediterranean Region and Occupational Injuries: A Retrospective Database-Based Analysis from North-Eastern Italy. Int. J. Environ. Res. Public Health 2019, 16, 673. [Google Scholar] [CrossRef]
- Moore, J.T.; Cigularov, K.P.; Sampson, J.M.; Rosecrance, J.C.; Chen, P.Y. Construction workers’ reasons for not reporting work-related injuries: An exploratory study. Int. J. Occup. Saf. Ergon. 2013, 19, 97–105. [Google Scholar] [CrossRef]
- Dutta, P.; Rajiva, A.; Andhare, D.; Azhar, G.S.; Tiwari, A.; Sheffield, P.; Ahmedabad, H.; Climate Study, G. Perceived heat stress and health effects on construction workers. Indian J. Occup. Environ. Med. 2015, 19, 151–158. [Google Scholar] [CrossRef]
- Varghese, B.M.; Hansen, A.; Bi, P.; Pisaniello, D. Are workers at risk of occupational injuries due to heat exposure? A comprehensive literature review. Saf. Sci. 2018, 110, 380–392. [Google Scholar] [CrossRef]
- Varghese, B.M.; Barnett, A.G.; Hansen, A.L.; Bi, P.; Hanson-Easey, S.; Heyworth, J.S.; Sim, M.R.; Pisaniello, D.L. The effects of ambient temperatures on the risk of work-related injuries and illnesses: Evidence from Adelaide, Australia 2003–2013. Environ. Res. 2019, 170, 101–109. [Google Scholar] [CrossRef]
- Gurcanli, G.E.; Mungen, U. Analysis of construction accidents in Turkey and responsible parties. Ind. Health 2013, 51, 581–595. [Google Scholar] [CrossRef]
- Irumba, R. Spatial analysis of construction accidents in Kampala, Uganda. Safety Sci. 2014, 64, 109–120. [Google Scholar] [CrossRef]
- Abbas, R.A.; Zalat, M.M.; Ghareeb, N.S.E. Non-fatal occupational injuries and safety climate: A cross-sectional study of construction building Workers in Mit-Ghamr City, Dakahlia governorate, Egypt. Open J. Safety Sci. Technol. 2013, 3, 69–79. [Google Scholar] [CrossRef]
- Dong, X.S.; Wang, X.; Daw, C. Fatal falls among older construction workers. Hum Factors 2012, 54, 303–315. [Google Scholar] [CrossRef]
- Hu, K.; Rahmandad, H.; Smith-Jackson, T.; Winchester, W. Factors influencing the risk of falls in the construction industry: A review of the evidence. Constr. Manag. Econ. 2011, 29, 397–416. [Google Scholar] [CrossRef]
- Lingard, H.; Holmes, N. Understandings of occupational health and safety risk control in small business construction firms: Barriers to implementing technological controls. Constr. Manag. Econ. 2001, 19, 217–226. [Google Scholar] [CrossRef]
- Herrero, S.G.; Saldana, M.A.; Rodriguez, J.G.; Ritzel, D.O. Influence of task demands on occupational stress: Gender differences. J. Safety Res. 2012, 43, 365–374. [Google Scholar] [CrossRef]
- Hasebe, T.; Sakai, T. Are elderly workers more likely to die in occupational accidents? Evidence from both industry-aggregated data and administrative individual-level data in Japan. Jpn. World Econ. 2018, 48, 79–89. [Google Scholar] [CrossRef]
- Alazab, R.M. Work-Related Diseases and Occupational Injuries among Workers in the Construction Industry in Egypt. Afr. Newsl. Occup. Health Saf. 2004, 14, 37–42. [Google Scholar]
- Welch, L.S.; Hunting, K.L.; Murawski, J.A. Occupational Injuries among Construction Workers Treated at the George Washington University Emergency Department. 1990-97. CPWR. 2004. Available online: http://www.cpwr.com (accessed on 24 August 2022).
- Kiconco, A.; Ruhinda, N.; Halage, A.A.; Watya, S.; Bazeyo, W.; Ssempebwa, J.C.; Byonanebye, J. Determinants of occupational injuries among building construction workers in Kampala City, Uganda. BMC Public Health 2019, 19, 1444. [Google Scholar] [CrossRef]
- Toccalino, D.; Colantonio, A.; Chan, V. Update on the epidemiology of work-related traumatic brain injury: A systematic review and meta-analysis. Occup. Environ. Med. 2021, 78, 769–776. [Google Scholar] [CrossRef]
- Sahraravand, A.; Haavisto, A.K.; Holopainen, J.M.; Leivo, T. Ocular traumas in working age adults in Finland—Helsinki Ocular Trauma Study. Acta Ophthalmol. 2017, 95, 288–294. [Google Scholar] [CrossRef]
- Cai, M.; Zhang, J. Epidemiological Characteristics of Work-Related Ocular Trauma in Southwest Region of China. Int. J. Environ. Res. Public Health 2015, 12, 9864–9875. [Google Scholar] [CrossRef]
- Forrest, K.Y.; Cali, J.M. Epidemiology of lifetime work-related eye injuries in the U.S. population associated with one or more lost days of work. Ophthalmic Epidemiol. 2009, 16, 156–162. [Google Scholar] [CrossRef]
- Gobba, F.; Dall’Olio, E.; Modenese, A.; De Maria, M.; Campi, L.; Cavallini, G.M. Work-Related Eye Injuries: A Relevant Health Problem. Main Epidemiological Data from a Highly-Industrialized Area of Northern Italy. Int. J. Environ. Res. Public Health 2017, 14, 604. [Google Scholar] [CrossRef]
- Zawilla, N.; Badr, H.; Al Shatti, A. Non-Fatal Occupational Injuries and Disability in Construction Workers in Kuwait 2003–2005. Egypt. J. Occup. Med. 2008, 32, 43–61. [Google Scholar]
- Salminen, S. Shift Work and Extended Working Hours as Risk Factors for Occupational Injury. Ergon. Open J. 2010, 3, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Powell, R.; Copping, A. Sleep deprivation and its consequences in construction workers. J. Constr. Eng. Manag. 2010, 136, 1086–1092. [Google Scholar] [CrossRef]
- Al-Bouwarthan, M.; Quinn, M.M.; Kriebel, D.; Wegman, D.H. Risk of Kidney Injury among Construction Workers Exposed to Heat Stress: A Longitudinal Study from Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 3775. [Google Scholar] [CrossRef]
- Chung, J.W.Y.; So, H.C.F.; Yan, V.C.M.; Kwok, P.S.T.; Wong, B.Y.M.; Yang, J.Y.; Chan, A.P.C. A Survey of Work-Related Pain Prevalence Among Construction Workers in Hong Kong: A Case-Control Study. Int. J. Environ. Res. Public Health 2019, 16, 1404. [Google Scholar] [CrossRef]
- Kao, K.Y.; Spitzmueller, C.; Cigularov, K.; Wu, H. Linking insomnia to workplace injuries: A moderated mediation model of supervisor safety priority and safety behavior. J. Occup. Health Psychol. 2016, 21, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Brossoit, R.M.; Crain, T.L.; Leslie, J.J.; Hammer, L.B.; Truxillo, D.M.; Bodner, T.E. The effects of sleep on workplace cognitive failure and safety. J. Occup. Health Psychol. 2019, 24, 411–422. [Google Scholar] [CrossRef]
- Kecklund, G.; Ekstedt, M.; Akerstedt, T.; Dahlgren, A.; Samuelson, B. The effects of double-shifts (15.5 hours) on sleep, fatigue and health. J. Hum. Ergol. 2001, 30, 53–58. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 397) | Age Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Injured body part | n | (%) | 16–25 (n = 80) | (%) | 26–35 (n = 107) | (%) | 36–45 (n = 98) | (%) | 46–55 (n = 74) | (%) | 56–65 (n = 38) | (%) | p-value |
| Head | 136 | (34.3) | 33 | (41.2) | 33 | (30.8) | 33 | (33.7) | 20 | (27.0) | 17 | (44.7) | 0.209 |
| Head (single injury) | 108 | (27.2) | 27 | (33.8) | 28 | (26.2) | 26 | (26.5) | 16 | (21.6) | 11 | (28.9) | 0.552 |
| Neck, spine | 36 | (9.1) | 6 | (7.5) | 8 | (7.5) | 10 | (10.2) | 7 | (9.5) | 5 | (13.2) | 0.826 |
| Neck, spine (single injury) | 13 | (3.3) | 2 | (2.5) | 4 | (3.7) | 2 | (2.0) | 3 | (4.1) | 2 | (5.3) | 13 |
| Thorax, back | 30 | (7.6) | 5 | (6.2) | 7 | (6.5) | 10 | (10.2) | 4 | (5.4) | 4 | (10.5) | 0.680 |
| Thorax, back (single injury) | 11 | (2.8) | 1 | (1.2) | 3 | (2.8) | 3 | (3.1) | 3 | (4.1) | 1 | (2.6) | 0.883 |
| Abdomen, pelvis | 23 | (5.8) | 6 | (7.5) | 6 | (5.6) | 5 | (5.1) | 3 | (4.1) | 3 | (7.9) | 0.872 |
| Abdomen, pelvis (single injury) | 8 | (2.0) | 1 | (1.2) | 3 | (2.8) | 2 | (2.0) | 1 | (1.4) | 1 | (2.6) | 0.937 |
| Shoulder, upper arm, elbow | 43 | (10.8) | 10 | (12.5) | 5 | (4.7) | 13 | (13.3) | 9 | (12.2) | 6 | (15.8) | 0.189 |
| Shoulder, upper arm, elbow (single injury) | 23 | (5.8) | 7 | (8.8) | 1 | (0.9) | 5 | (5.1) | 6 | (8.1) | 4 | (10.5) | 0.082 |
| Forearm, wrist, carpus | 27 | (6.8) | 3 | (3.8) | 8 | (7.5) | 6 | (6.1) | 9 | (12.2) | 1 | (2.6) | 0.221 |
| Forearm, wrist, carpus (single injury) | 19 | (4.8) | 1 | (1.2) | 8 | (7.5) | 5 | (5.1) | 5 | (6.8) | 0 | (0.0) | 0.167 |
| Hand | 92 | (23.2) | 20 | (25.0) | 23 | (21.5) | 20 | (20.4) | 21 | (28.4) | 8 | (21.1) | 0.743 |
| Hand (single injury) | 79 | (19.9) | 16 | (20.0) | 19 | (17.8) | 19 | (19.4) | 18 | (24.3) | 7 | (18.4) | 0.864 |
| Hip joint, femur | 11 | (2.8) | 0 | (0.0) | 3 | (2.8) | 6 | (6.1) | 2 | (2.7) | 0 | (0.0) | 0.114 |
| Hip joint, femur (single injury) | 8 | (2.0) | 0 | (0.0) | 2 | (1.9) | 5 | (5.1) | 1 | (1.4) | 0 | (0.0) | 0.119 |
| Knee joint, lower leg | 60 | (15.1) | 11 | (13.8) | 23 | (21.5) | 11 | (11.2) | 12 | (16.2) | 3 | (7.9) | 0.179 |
| Knee joint, lower leg (single injury) | 45 | (11.3) | 8 | (10.0) | 17 | (15.9) | 8 | (8.2) | 10 | (13.5) | 2 | (5.3) | 0.280 |
| Foot | 21 | (5.3) | 4 | (5.0) | 7 | (6.5) | 7 | (7.1) | 2 | (2.7) | 1 | (2.6) | 0.637 |
| Foot (single injury) | 15 | (3.8) | 3 | (3.8) | 4 | (3.7) | 6 | (6.1) | 1 | (1.4) | 1 | (2.6) | 0.589 |
| Multiple injured body parts | 58 | (14.6) | 13 | (16.2) | 13 | (12.1) | 14 | (14.3) | 10 | (13.5) | 8 | (21.1) | 0.729 |
| Total (N = 397) | Age Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type of injury | n | (%) | 16–25 (n = 80) | (%) | 26–35 (n = 107) | (%) | 36–45 (n = 98) | (%) | 46–55 (n = 74) | (%) | 56–65 (n = 38) | (%) | p-value |
| Wound laceration, incl. pneumothorax, internal organs | 190 | (47.9) | 40 | (50.0) | 54 | (50.5) | 46 | (46.9) | 31 | (41.9) | 19 | (50.0) | 0.809 |
| Traumatic brain injury | 32 | (8.1) | 6 | (7.5) | 6 | (5.6) | 14 | (14.3) | 2 | (2.7) | 4 | (10.5) | 0.056 |
| Distortion | 123 | (31.0) | 27 | (33.8) | 40 | (37.4) | 25 | (25.5) | 19 | (25.7) | 12 | (31.6) | 0.321 |
| Contusion | 84 | (21.2) | 19 | (23.8) | 17 | (15.9) | 25 | (25.5) | 18 | (24.3) | 5 | (13.2) | 0.275 |
| Crush trauma | 21 | (5.3) | 5 | (6.2) | 4 | (3.7) | 5 | (5.1) | 2 | (2.7) | 5 | (13.2) | 0.174 |
| Closed fracture | 49 | (12.3) | 6 | (7.5) | 13 | (12.1) | 12 | (12.2) | 12 | (16.2) | 6 | (15.8) | 0.528 |
| Open fracture | 24 | (6.0) | 4 | (5.0) | 5 | (4.7) | 5 | (5.1) | 7 | (9.5) | 3 | (7.9) | 0.661 |
| Dislocation | 6 | (1.5) | 1 | (1.2) | 2 | (1.9) | 2 | (2.0) | 1 | (1.4) | 0 | (0.0) | 0.923 |
| Burn frostbite | 5 | (1.3) | 2 | (2.5) | 1 | (0.9) | 1 | (1.0) | 0 | (0.0) | 1 | (2.6) | 0.619 |
| Chemical burn, electric shock, chemical substances | 7 | (1.8) | 2 | (2.5) | 3 | (2.8) | 1 | (1.0) | 1 | (1.4) | 0 | (0.0) | 0.738 |
| Infection poisoning, thermal shock | 2 | (0.5) | 0 | (0.0) | 1 | (0.9) | 1 | (1.0) | 0 | (0.0) | 0 | (0.0) | 0.756 |
| Irritation mucous membranes | 10 | (2.5) | 2 | (2.5) | 4 | (3.7) | 4 | (4.1) | 0 | (0.0) | 0 | (0.0) | 0.341 |
| Penetration and irritation of foreign objects | 71 | (17.9) | 18 | (22.5) | 22 | (20.6) | 13 | (13.3) | 10 | (13.5) | 8 | (21.1) | 0.363 |
| Amputation | 3 | (0.8) | 0 | (0.0) | 0 | (0.0) | 3 | (3.1) | 0 | (0.0) | 0 | (0.0) | 0.056 |
| Mechanism of Injury | Number of Patients (Total 397) | |
|---|---|---|
| n | (%) | |
| Fall | 87 | (21.9) |
| Machine handling | 40 | (10.1) |
| Manual instruments | 68 | (17.1) |
| Driving a transport vehicle | 3 | (0.8) |
| Transport by hand | 11 | (2.8) |
| Moving, walking, running, climbing, tripping | 32 | (8.1) |
| Contaminating substances | 13 | (3.3) |
| Explosion, ignite burn, electrical contact | 8 | (2.0) |
| Driven into, run over | 2 | (0.5) |
| Entrapment bruise | 42 | (10.6) |
| Impact against object | 69 | (17.4) |
| Cut on an object | 18 | (4.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dethlefsen, R.; Orlik, L.; Müller, M.; Exadaktylos, A.K.; Scholz, S.M.; Klukowska-Rötzler, J.; Ziaka, M. Work-Related Injuries among Insured Construction Workers Presenting to a Swiss Adult Emergency Department: A Retrospective Study (2016–2020). Int. J. Environ. Res. Public Health 2022, 19, 11294. https://doi.org/10.3390/ijerph191811294
Dethlefsen R, Orlik L, Müller M, Exadaktylos AK, Scholz SM, Klukowska-Rötzler J, Ziaka M. Work-Related Injuries among Insured Construction Workers Presenting to a Swiss Adult Emergency Department: A Retrospective Study (2016–2020). International Journal of Environmental Research and Public Health. 2022; 19(18):11294. https://doi.org/10.3390/ijerph191811294
Chicago/Turabian StyleDethlefsen, Ralf, Luisa Orlik, Martin Müller, Aristomenis K. Exadaktylos, Stefan M. Scholz, Jolanta Klukowska-Rötzler, and Mairi Ziaka. 2022. "Work-Related Injuries among Insured Construction Workers Presenting to a Swiss Adult Emergency Department: A Retrospective Study (2016–2020)" International Journal of Environmental Research and Public Health 19, no. 18: 11294. https://doi.org/10.3390/ijerph191811294
APA StyleDethlefsen, R., Orlik, L., Müller, M., Exadaktylos, A. K., Scholz, S. M., Klukowska-Rötzler, J., & Ziaka, M. (2022). Work-Related Injuries among Insured Construction Workers Presenting to a Swiss Adult Emergency Department: A Retrospective Study (2016–2020). International Journal of Environmental Research and Public Health, 19(18), 11294. https://doi.org/10.3390/ijerph191811294