

Moderate and Severe Dental Fluorosis in the Rural Population of Anantapur, India: Change in Their Biological Susceptibility?

 , and
, and
Abstract
:1. Introduction
2. Materials and Method
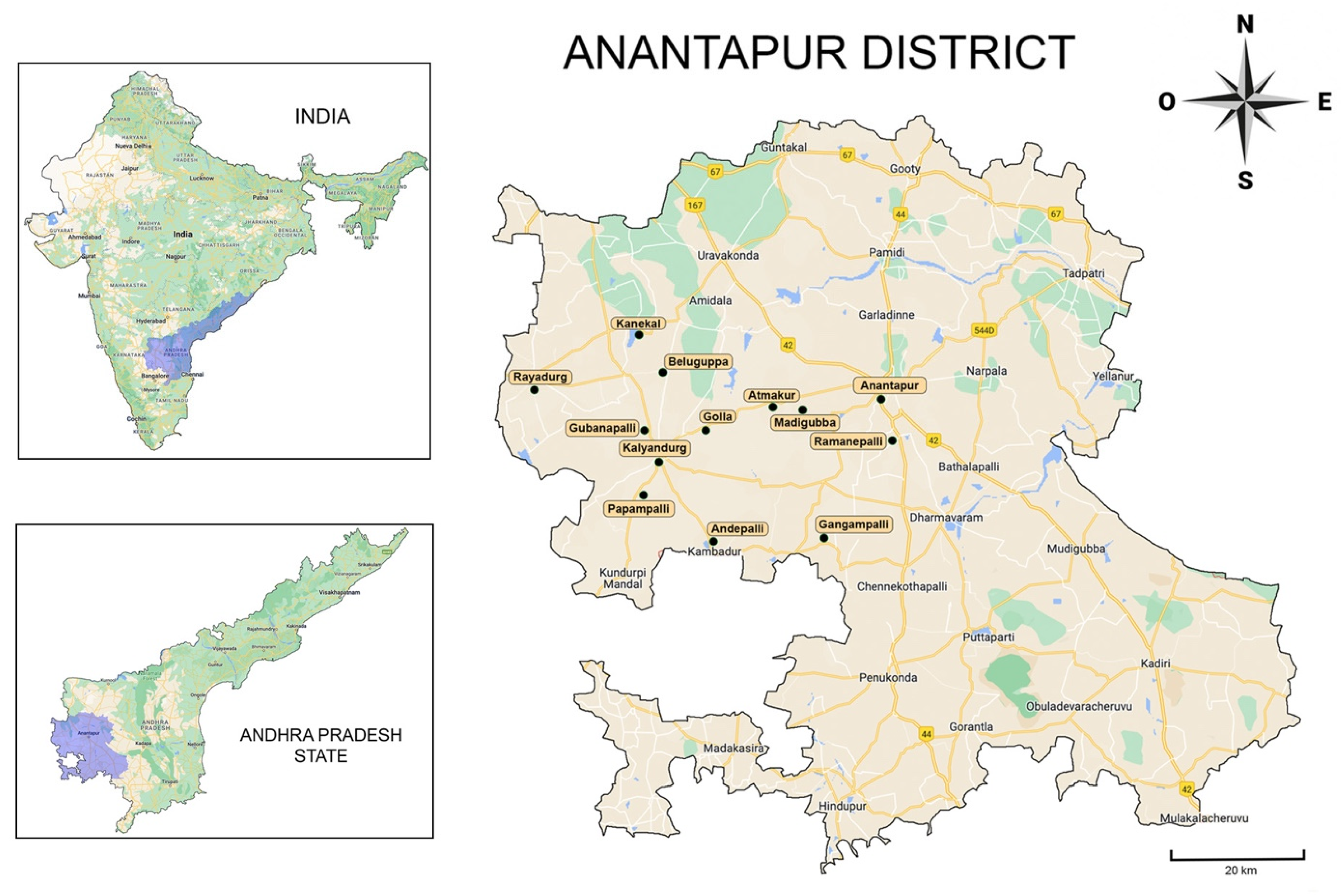
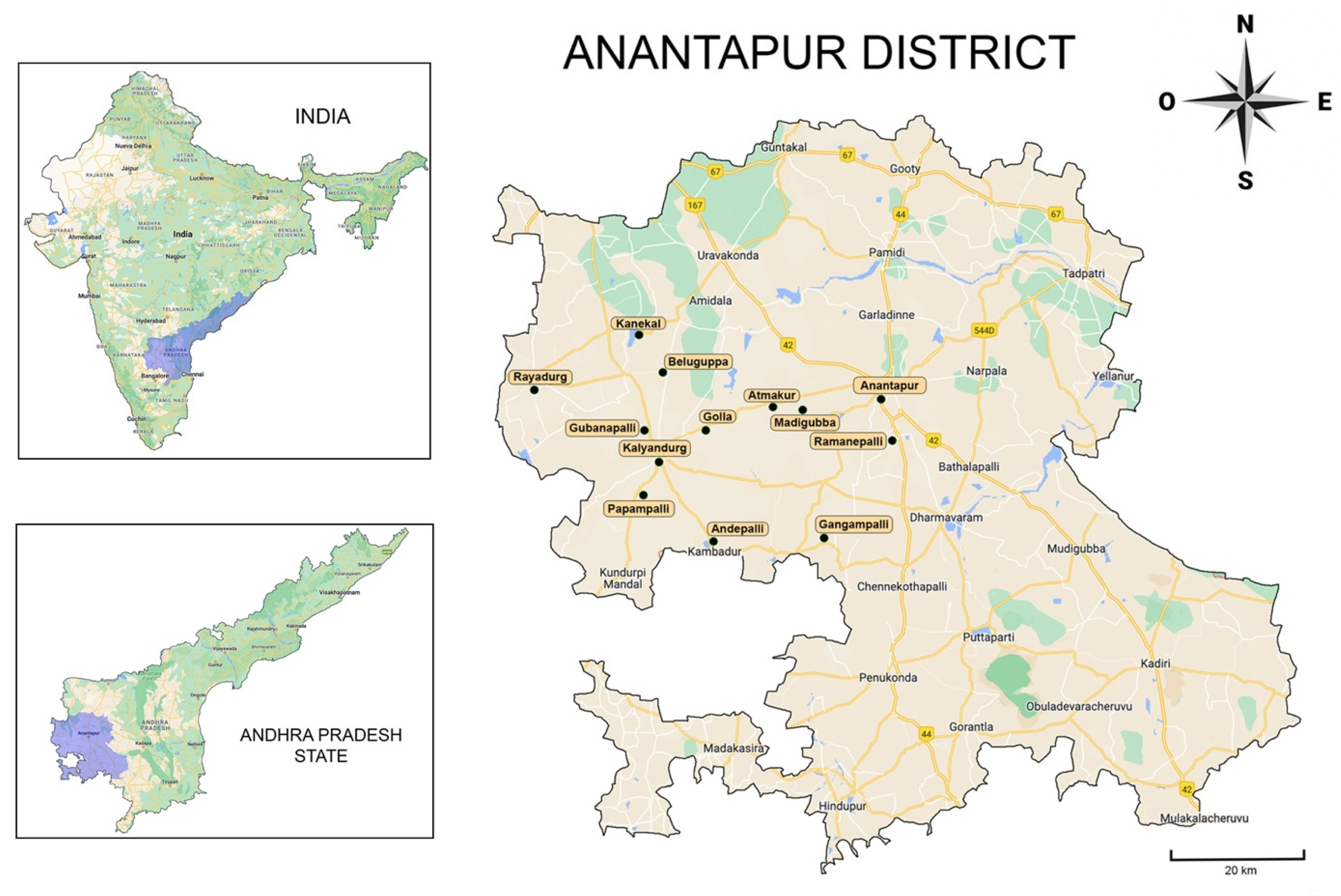
2.1. Study Characteristics, Population, and Ethical Aspects
2.2. Inclusion/Exclusion Criteria
- Patients of both genders.
- Patients born in the rural community of Anantapur.
- Patients with at least two teeth in each dental group, without dental destruction due to caries or trauma (independent of age).
- Patients who declared to consume water from untreated sources (groundwater).
- The exclusion criteria were:
- Patients with orofacial malformations or pathologies that could alter or increase the difficulty of the examination.
- Patients with systemic pathology affecting fluoride metabolism.
- Patients without permanent or definitive teeth.
- Patients with dental surface wear or stains due to tobacco, betel, or another chewing habit, impairing an adequate dental examination.
- Patients with an excess of bacterial dental plaque or calculus impairing an adequate dental examination.
- Patients requiring urgent dental attention.
- Patients who did not answer all the questions and those from whom it was difficult to obtain valid information.
- Patients whose parents or grandparents came from another community outside Anantapur.
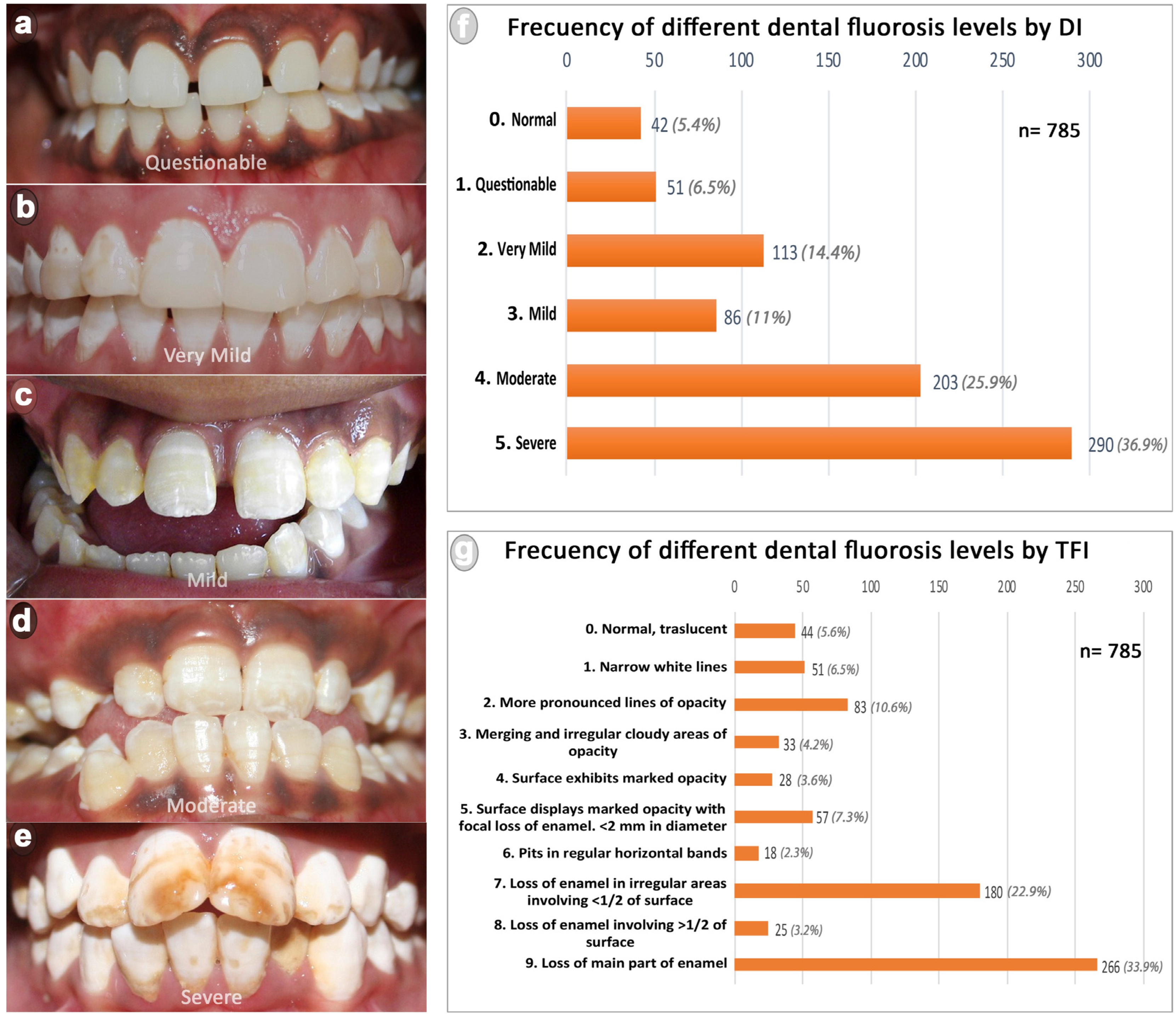
2.3. Indices Used for Dental Fluorosis Classifications
2.4. Collection and Analysis of Water Samples
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Studied Population and Water Samples
3.2. Dental Fluorosis Prevalence and Association with the Variables Studied
4. Discussion
4.1. The Situation of Anantapur District, Andhra Pradesh State
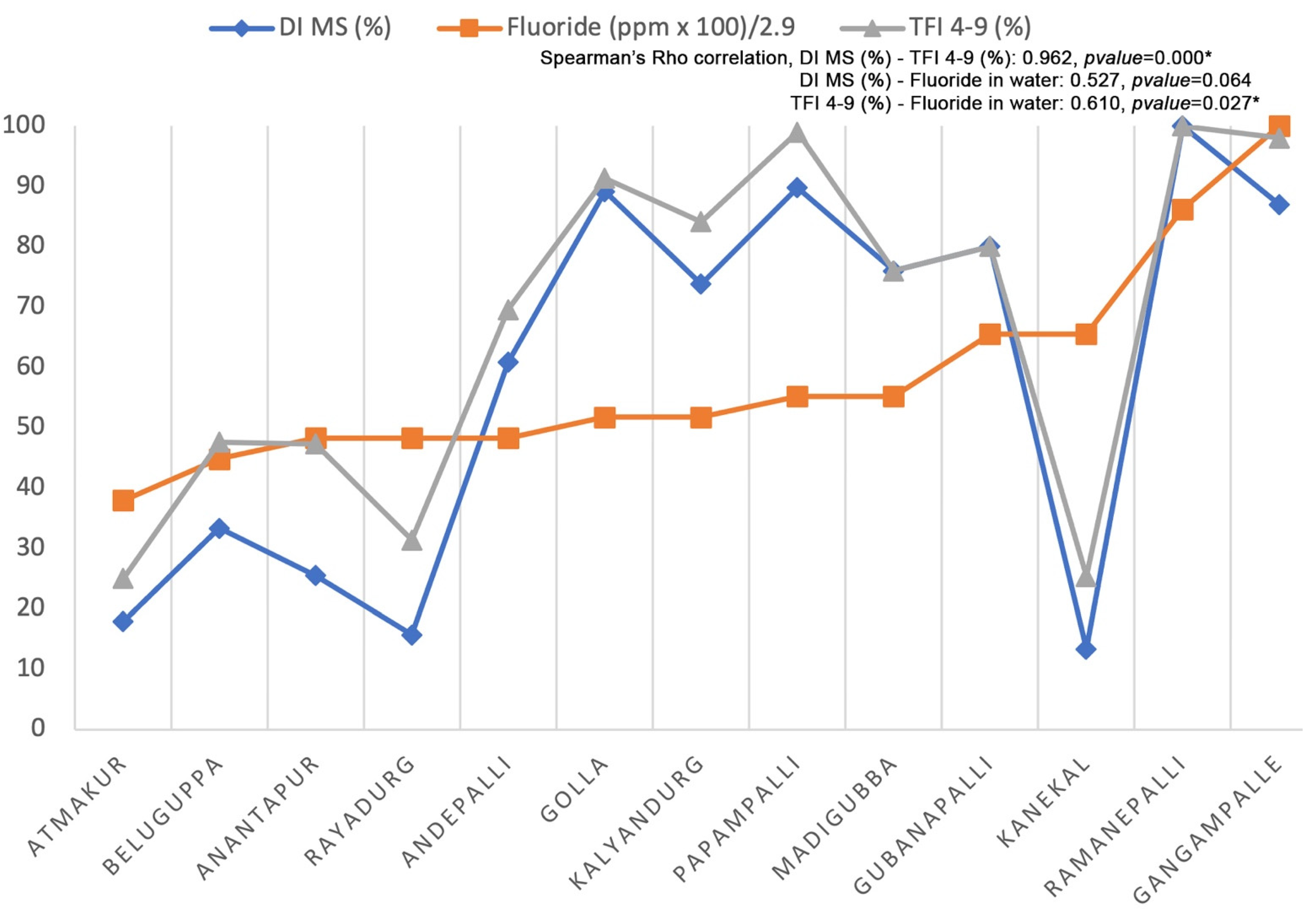
4.2. Dental Fluorosis in the Studied Population and Its Relation to the Regional Drinking Water
4.3. Polymorphism, Epigenetic and Genotoxicity Associated to Fluoride: Potential Changes in the Biological Susceptibility of the Organism against Fluoride as a Toxin
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Canada Communication Group. Inorganic Fluorides (Priority Substances List Assessment Report); Environment Canada: Ottawa, ON, Canada, 1993; ISBN 978-0-662-21070-2. [Google Scholar]
- Ayoob, S.; Gupta, A.K. Fluoride in Drinking Water: A Review on the Status and Stress Effects. Crit. Rev. Environ. Sci. Technol. 2006, 36, 433–487. [Google Scholar] [CrossRef]
- World Health Organization. Fluorides and Human Health, No. 59; WHO Monograph Series; World Health Organization: Geneva, Switzerland, 1970. [Google Scholar]
- World Health Organization. Fluorides and Oral Health, No. 846; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Fawell, J.; Bailey, K.; Chilton, J.; Dahi, E.; Fewtrell, L.; Magara, Y. World Health Organization Fluoride in Drinking-Water; IWA Publishing: London, UK, 2006. [Google Scholar]
- Bhagavan, S.V.B.K.; Raghu, V. Utility of Check Dams in Dilution of Fluoride Concentration in Ground Water and the Resultant Analysis of Blood Serum and Urine of Villagers, Anantapur District, Andhra Pradesh, India. Environ. Geochem. Health 2005, 27, 97–108. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for Drinking-Water Quality [Electronic Resource]: Incorporating 1st and 2nd Addenda, Vol. 1, Recommendations, 3rd ed.; World Health Organization: Geneva, Switzerland, 2008; ISBN 978-92-4-154761-1. [Google Scholar]
- McDonagh, M.S.; Whiting, P.F.; Wilson, P.M.; Sutton, A.J.; Chestnutt, I.; Cooper, J.; Misso, K.; Bradley, M.; Treasure, E.; Kleijnen, J. Systematic Review of Water Fluoridation. BMJ 2000, 321, 855–859. [Google Scholar] [CrossRef] [PubMed]
- Shashi, A.; Kumar, M.; Bhardwaj, M. Incidence of Skeletal Deformities in Endemic Fluorosis. Trop. Doct. 2008, 38, 231–233. [Google Scholar]
- Vilasrao, G.S.; Kamble, K.M.; Sabat, R.N. Child Fluorosis in Chhattisgarh, India: A Community-Based Survey. Indian Pediatr. 2014, 51, 903–905. [Google Scholar] [CrossRef]
- Jarquín-Yñezá, L.; Alegría-Torres, J.A.; Castillo, C.G.; de Jesús Mejía-Saavedra, J. Dental Fluorosis and a Polymorphism in the COL1A2 Gene in Mexican Children. Arch. Oral Biol. 2018, 96, 21–25. [Google Scholar] [CrossRef]
- Pramanik, S.; Saha, D. The Genetic Influence in Fluorosis. Environ. Toxicol. Pharmacol. 2017, 56, 157–162. [Google Scholar] [CrossRef]
- Bali, R.K.; Mathur, V.B.; Talwar, P.P.; Chanana, H.B. National Oral Health Survey and Fluoride Mapping 2002–2003; Dental Council of India: New Delhi, India, 2004. [Google Scholar]
- Jagtap, S.; Yenkie, M.K.; Labhsetwar, N.; Rayalu, S. Fluoride in Drinking Water and Defluoridation of Water. Chem. Rev. 2012, 112, 2454–2466. [Google Scholar] [CrossRef]
- Reddy, B.M.; Sunitha, V.; Prasad, M.; Reddy, Y.S.; Reddy, M.R. Evaluation of Groundwater Suitability for Domestic and Agricultural Utility in Semi-Arid Region of Anantapur, Andhra Pradesh State, South India. Groundw. Sustain. Dev. 2019, 9, 100262. [Google Scholar] [CrossRef]
- Fareed, M.; Afzal, M. Genetics of Consanguinity and Inbreeding in Health and Disease. Ann. Hum. Biol. 2017, 44, 99–107. [Google Scholar] [CrossRef]
- Juyal, G.; Mondal, M.; Luisi, P.; Laayouni, H.; Sood, A.; Midha, V.; Heutink, P.; Bertranpetit, J.; Thelma, B.K.; Casals, F. Population and Genomic Lessons from Genetic Analysis of Two Indian Populations. Hum. Genet. 2014, 133, 1273–1287. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Baez, R.J.; World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-154864-9. [Google Scholar]
- Thylstrup, A.; Fejerskov, O. Clinical Appearance of Dental Fluorosis in Permanent Teeth in Relation to Histologic Changes. Community Dent. Oral Epidemiol. 1978, 6, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Forum on Fluoridation. Chapter 12 Controlling Dental Fluorosis. Report of the Forum on Fluoridation; Stationery Office: Dublín, Ireland, 2002; p. 126. [Google Scholar]
- Mabelya, L.; van ’t Hof, M.A.; König, K.G.; van Palenstein Helderman, W.H. Comparison of Two Indices of Dental Fluorosis in Low, Moderate and High Fluorosis Tanzanian Populations. Community Dent. Oral Epidemiol. 1994, 22, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Puri, A. A Review of Permissible Limits of Drinking Water. Indian J. Occup. Environ. Med. 2012, 16, 40–44. [Google Scholar]
- Home Government of India. Available online: https://censusindia.gov.in/census.website/ (accessed on 25 August 2022).
- Drinking Water Sectional Committee. Drinking Water Specification, Second Revision; Bureau of Indian Standards: New Delhi, India, 2012. [Google Scholar]
- Home Department TBPHLC Circle Anantapuramu Profile. Available online: https://ananthapuramu.ap.gov.in/tbphlc-circle-anantapuramu-profile/ (accessed on 25 August 2022).
- World Health Organisation. Appropriate Use of Fluoride for Human Health; World Health Organization: Belgium, Germany, 1986. [Google Scholar]
- Aoba, T.; Fejerskov, O. Dental Fluorosis: Chemistry and Biology. Crit. Rev. Oral Biol. Med. 2002, 13, 155–170. [Google Scholar] [CrossRef]
- Rwenyonyi, C.M.; Birkeland, J.M.; Haugejorden, O.; Bjorvatn, K. Age as a Determinant of Severity of Dental Fluorosis in Children Residing in Areas with 0.5 and 2.5 Mg Fluoride per Liter in Drinking Water. Clin. Oral Investig. 2000, 4, 157–161. [Google Scholar] [CrossRef]
- Strużycka, I.; Olszewska, A.; Bogusławska-Kapała, A.; Hryhorowicz, S.; Kaczmarek-Ryś, M.; Grabarek, B.O.; Staszkiewicz, R.; Kuciel-Polczak, I.; Czajka-Jakubowska, A. Assessing Fluorosis Incidence in Areas with Low Fluoride Content in the Drinking Water, Fluorotic Enamel Architecture, and Composition Alterations. Int. J. Environ. Res. Public Health 2022, 19, 7153. [Google Scholar] [CrossRef]
- Gdalia, I. Urinary Fluorine Levels of Children and Adults. J. Dent. Res. 1958, 37, 601–604. [Google Scholar] [CrossRef]
- Gedalia, J.; Brzezinski, A.; Bercovici, B. Urinary Fluorine Levels in Women during Pregnancy and after Delivery. J. Dent. Res. 1959, 38, 548–551. [Google Scholar] [CrossRef]
- Samarasimha-Reddy, D.K.; Narasimha-Rao, K.L. Incidence of Fluorosis in India with Special Reference to Andhra Pradesh. In Geosciences and Water Resources: Environmental Data Modeling; Bardinet, C., Royer, J.-J., Eds.; Data and Knowledge in a Changing World; Springer: Berlin/Heidelberg, Germany, 1997; pp. 77–84. ISBN 978-3-642-60627-4. [Google Scholar]
- Reddy, B.M.; Sunitha, V.; Reddy, M.R. Prevalence of Dental Fluorosis in Southeastern Part of Anantapur District, Andhra Pradesh. J. Chem. Pharm. Res. 2016, 8, 179–185. [Google Scholar]
- Shekar, C.; Cheluvaiah, M.B.; Namile, D. Prevalence of Dental Caries and Dental Fluorosis among 12 and 15 Years Old School Children in Relation to Fluoride Concentration in Drinking Water in an Endemic Fluoride Belt of Andhra Pradesh. Indian J. Public Health 2012, 56, 122–128. [Google Scholar] [CrossRef]
- Sukhabogi, J.R.; Parthasarathi, P.; Anjum, S.; Shekar, B.; Padma, C.; Rani, A. Dental Fluorosis and Dental Caries Prevalence among 12 and 15-Year-Old School Children in Nalgonda District, Andhra Pradesh, India. Ann. Med. Health Sci. Res. 2014, 4, S245–S252. [Google Scholar] [CrossRef] [PubMed]
- Sudhir, K.M.; Suresh, S.; Prashant, G.M.; Reddy, V.V.S.; Shafiulla, M.; Chandu, G.N. Distribution Patterns of Enamel Fluorosis in Permanent Dentition. Oral Health Prev. Dent. 2012, 10, 167–174. [Google Scholar] [PubMed]
- Shanthi, M.; Reddy, B.V.; Venkataramana, V.; Gowrisankar, S.; Reddy, B.V.T.; Chennupati, S. Relationship Between Drinking Water Fluoride Levels, Dental Fluorosis, Dental Caries and Associated Risk Factors in 9-12 Years Old School Children of Nelakondapally Mandal of Khammam District, Andhra Pradesh, India: A Cross-Sectional Survey. J. Int. Oral Health 2014, 6, 106–110. [Google Scholar] [PubMed]
- Sebastian, S.T.; Soman, R.R.; Sunitha, S. Prevalence of Dental Fluorosis among Primary School Children in Association with Different Water Fluoride Levels in Mysore District, Karnataka. Indian J. Dent. Res. 2016, 27, 151–154. [Google Scholar] [CrossRef]
- Mahantesha, T.; Dixit, U.B.; Nayakar, R.P.; Ashwin, D.; Ramagoni, N.K.; Kamavaram Ellore, V.P. Prevalence of Dental Fluorosis and Associated Risk Factors in Bagalkot District, Karnataka, India. Int. J. Clin. Pediatr. Dent. 2016, 9, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Akpata, E.S.; Fakiha, Z.; Khan, N. Dental Fluorosis in 12-15-Year-Old Rural Children Exposed to Fluorides from Well Drinking Water in the Hail Region of Saudi Arabia. Community Dent. Oral Epidemiol. 1997, 25, 324–327. [Google Scholar] [CrossRef] [PubMed]
- AlDosari, A.M.; Akpata, E.S.; Khan, N. Associations among Dental Caries Experience, Fluorosis, and Fluoride Exposure from Drinking Water Sources in Saudi Arabia. J. Public Health Dent. 2010, 70, 220–226. [Google Scholar] [CrossRef]
- Irigoyen, M.E.; Molina, N.; Luengas, I. Prevalence and Severity of Dental Fluorosis in a Mexican Community with Above-Optimal Fluoride Concentration in Drinking Water. Community Dent. Oral Epidemiol. 1995, 23, 243–245. [Google Scholar] [CrossRef]
- Manji, F.; Baelum, V.; Fejerskov, O. Dental Fluorosis in an Area of Kenya with 2 ppm Fluoride in the Drinking Water. J. Dent. Res. 1986, 65, 659–662. [Google Scholar] [CrossRef]
- Ibrahim, Y.E.; Affan, A.A.; Bjorvatn, K. Prevalence of Dental Fluorosis in Sudanese Children from Two Villages with 0.25 and 2.56 ppm Fluoride in the Drinking Water. Int. J. Paediatr. Dent. 1995, 5, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Rao, K.V.; Mahajan, C.L. Fluoride Content of Some Common South Indian Foods and Their Contribution to Fluorosis. J. Sci. Food Agric. 1990, 51, 275–279. [Google Scholar] [CrossRef]
- Bronckers, A.L.J.J.; Lyaruu, D.M.; DenBesten, P.K. The Impact of Fluoride on Ameloblasts and the Mechanisms of Enamel Fluorosis. J. Dent. Res. 2009, 88, 877–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshingkar, P. Migration, Remote Rural Areas and Chronic Poverty in INDIA; Overseas Development Institute: London, UK, 2010. [Google Scholar]
- Mastana, S.S.; Papiha, S.S. Genomic and Gene Diversity among the People of the Indian Subcontinent. In Genetic Disorders of the Indian Subcontinent; Kumar, D., Ed.; Springer: Dordrecht, The Netherlands, 2004; pp. 57–80. ISBN 978-1-4020-2231-9. [Google Scholar]
- Russell, A.L. Dental Fluorosis in Grand Rapids during the Seventeenth Year of Fluoridation. J. Am. Dent. Assoc. 1962, 65, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.E.; Zwemer, J.D. Community Water Fluoride Levels, Preschool Dietary Patterns, and the Occurrence of Fluoride Enamel Opacities. J. Public Health Dent. 1990, 50, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Ba, Y.; Cui, L.; Cheng, X.; Zhu, J.; Zhang, Y.; Yan, P.; Zhu, C.; Kilfoy, B.; Zhang, Y. COL1A2 gene polymorphisms (Pvu II and Rsa I), serum calciotropic hormone levels, and dental fluorosis. Community Dent. Oral Epidemiol. 2008, 36, 517–522. [Google Scholar] [CrossRef]
- Küchler, E.C.; Tannure, P.N.; de Oliveira, D.S.B.; Charone, S.; Nelson-Filho, P.; da Silva, R.A.B.; de Castro Costa, M.; Antunes, L.S.; Calasans Maia, M.D.; Antunes, L.A.A. Polymorphisms in Genes Involved in Enamel Development Are Associated with Dental Fluorosis. Arch. Oral Biol. 2017, 76, 66–69. [Google Scholar] [CrossRef]
- Dalledone, M.; Cunha, A.S.; Ramazzotto, L.A.; Pecharki, G.D.; Nelson-Filho, P.; Scariot, R.; Trevilatto, P.C.; Vieira, A.R.; Küchler, E.C.; Brancher, J.A. Estrogen Receptor Gene Is Associated with Dental Fluorosis in Brazilian Children. Clin. Oral Investig. 2019, 23, 3565–3570. [Google Scholar] [CrossRef]
- Ba, Y.; Zhang, H.; Wang, G.; Wen, S.; Yang, Y.; Zhu, J.; Ren, L.; Yang, R.; Zhu, C.; Li, H.; et al. Association of Dental Fluorosis with Polymorphisms of Estrogen Receptor Gene in Chinese Children. Biol. Trace Elem. Res. 2011, 143, 87–96. [Google Scholar] [CrossRef]
- Jiang, M.; Mu, L.; Wang, Y.; Yan, W.; Jiao, Y. The Relationship between Alu I Polymorphisms in the Calcitonin Receptor Gene and Fluorosis Endemic to Chongqing, China. Med. Princ. Pract. 2015, 24, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Toteja, D.G.S.; Meena, C.; Bala, K.; Mohanty, S.S. Association of COL1A2 Gene Polymorphism with Dental Fluorosis in Children of Jaipur District of Rajasthan, India. Asian Pac. J. Health Sci. 2016, 3, 249–255. [Google Scholar]
- Rahila, C.; Aswath Narayanan, M.B.; Ramesh Kumar, S.G.; Leena Selvamary, A.; Sujatha, A.; John Kirubaharan, J. Association of COL1A2 (PvuII) Gene Polymorphism with Risk and Severity of Dental Fluorosis-A Case Control Study. Saudi Dent. J. 2019, 31, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Saha, D.; Goswami, R.; Majumdar, K.K.; Sikdar, N.; Pramanik, S. Evaluating the Association between Dental Fluorosis and Polymorphisms in Bone Development and Mineralization Genes Among Population from a Fluoride Endemic Region of Eastern India. Biol. Trace Elem. Res. 2021, 199, 1–8. [Google Scholar] [CrossRef]
- Everett, E.T.; McHenry, M.a.K.; Reynolds, N.; Eggertsson, H.; Sullivan, J.; Kantmann, C.; Martinez-Mier, E.A.; Warrick, J.M.; Stookey, G.K. Dental Fluorosis: Variability among Different Inbred Mouse Strains. J. Dent. Res. 2002, 81, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.P.G.F.; Hanocock, R.; Eggertsson, H.; Everett, E.T.; Grynpas, M.D. Tooth Quality in Dental Fluorosis Genetic and Environmental Factors. Calcif. Tissue Int. 2005, 76, 17–25. [Google Scholar] [CrossRef]
- Ribeiro, D.A.; Yujra, V.Q.; da Silva, V.H.P.; Claudio, S.R.; Estadella, D.; de Barros Viana, M.; Oshima, C.T.F. Putative Mechanisms of Genotoxicity Induced by Fluoride: A Comprehensive Review. Environ. Sci. Pollut. Res. Int. 2017, 24, 15254–15259. [Google Scholar] [CrossRef] [PubMed]
- Daiwile, A.P.; Tarale, P.; Sivanesan, S.; Naoghare, P.K.; Bafana, A.; Parmar, D.; Kannan, K. Role of Fluoride Induced Epigenetic Alterations in the Development of Skeletal Fluorosis. Ecotoxicol. Environ. Saf. 2019, 169, 410–417. [Google Scholar] [CrossRef]
- Manivannan, J.; Sinha, S.; Ghosh, M.; Mukherjee, A. Evaluation of Multi-Endpoint Assay to Detect Genotoxicity and Oxidative Stress in Mice Exposed to Sodium Fluoride. Mutagen. Res. 2013, 751, 59–65. [Google Scholar]
- Suzuki, M.; Bandoski, C.; Bartlett, J.D. Fluoride induces oxidative damage and SIRT1/autophagy through ROS-mediated JNK signalling. Free Radic. Biol. Med. 2015, 89, 369–378. [Google Scholar] [CrossRef]
- Suzuki, M.; Ikeda, A.; Bartlett, J.D. Sirt1 Overexpression Suppresses Fluoride-Induced P53 Acetylation to Alleviate Fluoride Toxicity in Ameloblasts Responsible for Enamel Formation. Arch. Toxicol. 2018, 92, 1283–1293. [Google Scholar] [CrossRef]
- Miousse, I.R.; Currie, R.; Datta, K.; Ellinger-Ziegelbauer, H.; French, J.E.; Harrill, A.H.; Koturbash, I.; Lawton, M.; Mann, D.; Meehan, R.R.; et al. Importance of Investigating Epigenetic Alterations for Industry and Regulators: An Appraisal of Current Efforts by the Health and Environmental Sciences Institute. Toxicology 2015, 335, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Xavier, M.J.; Roman, S.D.; Aitken, R.J.; Nixon, B. Transgenerational inheritance: How impacts to the epigenetic and genetic information of parents affect offspring health. Hum. Reprod. Update 2019, 25, 518–540. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Rural Community | Patients Included | Female | Male | Age Mean (Range) | Drinking Water Sources Analyzed | Fluoride Quantity in Water (ppm) | DI Normal + QVM (a) | DI MS (b) | TFI Normal + 1–3 (c) | TFI 4–9 (d) |
|---|---|---|---|---|---|---|---|---|---|---|
| Anantapur | 55 | 35 | 20 | 27.5 (10–60) | 1 | 1.4 | 41 | 14 | 29 | 26 |
| Andepalli | 23 | 19 | 4 | 18.5 (10–40) | 1 | 1.4 | 9 | 14 | 7 | 16 |
| Atmakur | 28 | 18 | 10 | 28.8 (16–51) | 1 | 1.1 | 23 | 5 | 21 | 7 |
| Beluguppa | 21 | 16 | 5 | 35.1 (11–60) | 1 | 1.3 | 14 | 7 | 11 | 10 |
| Gangampalli | 100 | 46 | 54 | 29.9 (10–60) | 1 | 2.9 | 13 | 87 | 2 | 98 |
| Golla | 46 | 26 | 20 | 25.6 (10–60) | 1 | 1.5 | 5 | 41 | 4 | 42 |
| Gubanapalli | 10 | 6 | 4 | 24.7 (12–55) | 1 | 1.9 | 2 | 8 | 2 | 8 |
| Kalyandurg | 233 | 149 | 84 | 19.2 (10–60) | 2 | 1.5 | 61 | 172 | 37 | 196 |
| Kanekal | 75 | 31 | 44 | 28.0 (10–55) | 1 | 1.9 | 65 | 10 | 56 | 19 |
| Madigubba | 25 | 12 | 13 | 25.8 (11–55) | 1 | 1.6 | 6 | 19 | 6 | 19 |
| Papampalli | 98 | 63 | 35 | 13.1 (11–20) | 2 | 1.6 | 10 | 88 | 1 | 97 |
| Ramanepalli | 20 | 10 | 10 | 27.5 (16.50) | 1 | 2.5 | 0 | 20 | 0 | 20 |
| Rayadurg | 51 | 32 | 19 | 27.9 (10–60) | 1 | 1.4 | 43 | 8 | 35 | 16 |
| Dean Index (a) n = 785 | Thylstrup Fejerskov Index (a) n = 785 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| MS (%) | Normal + QVM (%) | p Value | SP | OR (CI 95%) (d) | 4–9 (%) | Normal + 1–3 (%) | p Value | SP | OR (CI 95%) (d) | ||
| Age range (y = years) | |||||||||||
| up to 15 y | 269 (34.2) | 47 (5.9) | 0.000 * (b) | 1.0 | 295 (37.5) | 21 (2.6) | 0.000 * (b) | 1.0 | |||
| 16–25 y | 103 (13.1) | 97 (12.3) | 131 (16.6) | 69 (8.7) | |||||||
| 26–35 y | 51 (6.4) | 78 (9.9) | 66 (8.4) | 63 (8.0) | |||||||
| 36–45 y | 41 (5.2) | 36 (4.5) | 46 (5.8) | 31 (3.9) | |||||||
| 46–55 y | 23 (2.9) | 21 (2.6) | 28 (3.5) | 16 (2.0) | |||||||
| over 55 y | 6 (0.7) | 13 (1.6) | 8 (1.0) | 11 (1.4) | |||||||
| Fluoride concentration | |||||||||||
| more than 1.5 ppm | 232 (29.5) | 96 (12.2) | 0.000 * (c) | 0.97 | 1.81 (1.34–2.45) * | 261 (33.2) | 67 (8.5) | 0.000 *(c) | 0.94 | 1.79 (1.28–2.5) * | |
| up to 1.5 ppm | 261 (33.2) | 196 (24.9) | 313 (39.8) | 144 (18.3) | |||||||
| Gender | |||||||||||
| female | 294 (37.4) | 169 (21.5) | 0.653 (c) | 1.08 (0.8–1.44) | 350 (44.5) | 113 (14.3) | 0.07 (c) | 1.35 (0.98–1.86) | |||
| male | 199 (25.3) | 123 (15.6) | 224 (28.5) | 98 (12.4) | |||||||
| Age range considering gender (y = years) | |||||||||||
| up to 15 y | female | 166 (52.5) | 30 (9.4) | 0.871 (c) | 0.91 (0.48–1.74) | 187 (59.1) | 9 (2.8) | 0.067 (c) | 2.31 (0.94–5.66) | ||
| male | 103 (32.5) | 17 (5.3) | 108 (34.1) | 12 (3.7) | |||||||
| 16–25 y | female | 57 (28.5) | 59 (29.5) | 0.475 (c) | 0.8 (0.45–1.4) | 76 (38) | 40 (20) | 1.000 (c) | 1 (0.55–1.81) | ||
| male | 46 (23) | 38 (19) | 55 (27.5) | 29 (14.5) | |||||||
| 26–35 y | female | 31 (24) | 44 (34.1) | 0.716 (c) | 1.2 (0.58–2.46) | 39 (30.2) | 36 (27.9) | 0.860 (c) | 1.08 (0.54–2.18) | ||
| male | 20 (15.5) | 34 (26.3) | 27 (20.9) | 27 (20.9) | |||||||
| 36–45 y | female | 26 (33.7) | 13 (16.8) | 0.023 * (c) | 1.0 | 3.07 (1.21–7.28) * | 28 (36.3) | 11 (14.2) | 0.038 * (c) | 0.99 | 2.83 (1.1–7.27) * |
| male | 15 (19.4) | 23 (29.8) | 18 (23.3) | 20 (25.9) | |||||||
| 46–55 y | female | 12 (27.2) | 15 (34) | 0.228 (c) | 0.44 (0.12–1.52) | 17 (38.6) | 10 (22.7) | 1.000 (c) | 0.93 (0.26–3.28) | ||
| male | 11 (25) | 6 (13.6) | 11 (25) | 6 (13.6) | |||||||
| over 55 y | female | 2 (10.5) | 8 (42.1) | 0.350 (c) | 0.31 (0.04–2.38) | 3 (15.7) | 7 (36.8) | 0.370 (c) | 0.34 (0.05–2.26) | ||
| male | 4 (21) | 5 (26.3) | 5 (26.3) | 4 (21) | |||||||
| Fluoride concentration in water considering gender | |||||||||||
| more than 1.5 ppm | female | 123 (37.5) | 45 (13.7) | 0.333 (c) | 1.28 (0.79–2.06) | 141 (42.9) | 27 (8.2) | 0.054 (c) | 0.88 | 1.74 (1.01–3) * | |
| male | 109 (33.2) | 51 (15.5) | 120 (36.5) | 40 (12.1) | |||||||
| up to 1.5 ppm | female | 171 (37.4) | 124 (27.1) | 0.628 (c) | 1.1 (0.75–1.62) | 209 (45.7) | 86 (18.8) | 0.171 (c) | 1.36 (0.9–2.04) | ||
| male | 90 (19.6) | 72 (15.7) | 104 (22.7) | 58 (12.6) | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Escobar, T.M.; Valdivia-Gandur, I.; Astudillo-Rozas, W.; Aceituno-Antezana, O.; Yamadala, B.; Lozano de Luaces, V.; Chimenos-Küstner, E.; Manzanares-Céspedes, M.C. Moderate and Severe Dental Fluorosis in the Rural Population of Anantapur, India: Change in Their Biological Susceptibility? Int. J. Environ. Res. Public Health 2022, 19, 11293. https://doi.org/10.3390/ijerph191811293
García-Escobar TM, Valdivia-Gandur I, Astudillo-Rozas W, Aceituno-Antezana O, Yamadala B, Lozano de Luaces V, Chimenos-Küstner E, Manzanares-Céspedes MC. Moderate and Severe Dental Fluorosis in the Rural Population of Anantapur, India: Change in Their Biological Susceptibility? International Journal of Environmental Research and Public Health. 2022; 19(18):11293. https://doi.org/10.3390/ijerph191811293
Chicago/Turabian StyleGarcía-Escobar, Trina Mylena, Iván Valdivia-Gandur, Wilson Astudillo-Rozas, Oscar Aceituno-Antezana, Balasubbaiah Yamadala, Vicente Lozano de Luaces, Eduardo Chimenos-Küstner, and María Cristina Manzanares-Céspedes. 2022. "Moderate and Severe Dental Fluorosis in the Rural Population of Anantapur, India: Change in Their Biological Susceptibility?" International Journal of Environmental Research and Public Health 19, no. 18: 11293. https://doi.org/10.3390/ijerph191811293
APA StyleGarcía-Escobar, T. M., Valdivia-Gandur, I., Astudillo-Rozas, W., Aceituno-Antezana, O., Yamadala, B., Lozano de Luaces, V., Chimenos-Küstner, E., & Manzanares-Céspedes, M. C. (2022). Moderate and Severe Dental Fluorosis in the Rural Population of Anantapur, India: Change in Their Biological Susceptibility? International Journal of Environmental Research and Public Health, 19(18), 11293. https://doi.org/10.3390/ijerph191811293