
Study on the Measurement and Influencing Factors of Care Service Demand of Disabled Elderly in Urban and Rural China


Abstract
:1. Introduction
2. Literature Review and Theory
2.1. Literature Review
2.1.1. Care Service Demand and Measurement
2.1.2. Care service Demand Satisfaction
2.1.3. Factors Influencing the Care Services Demand
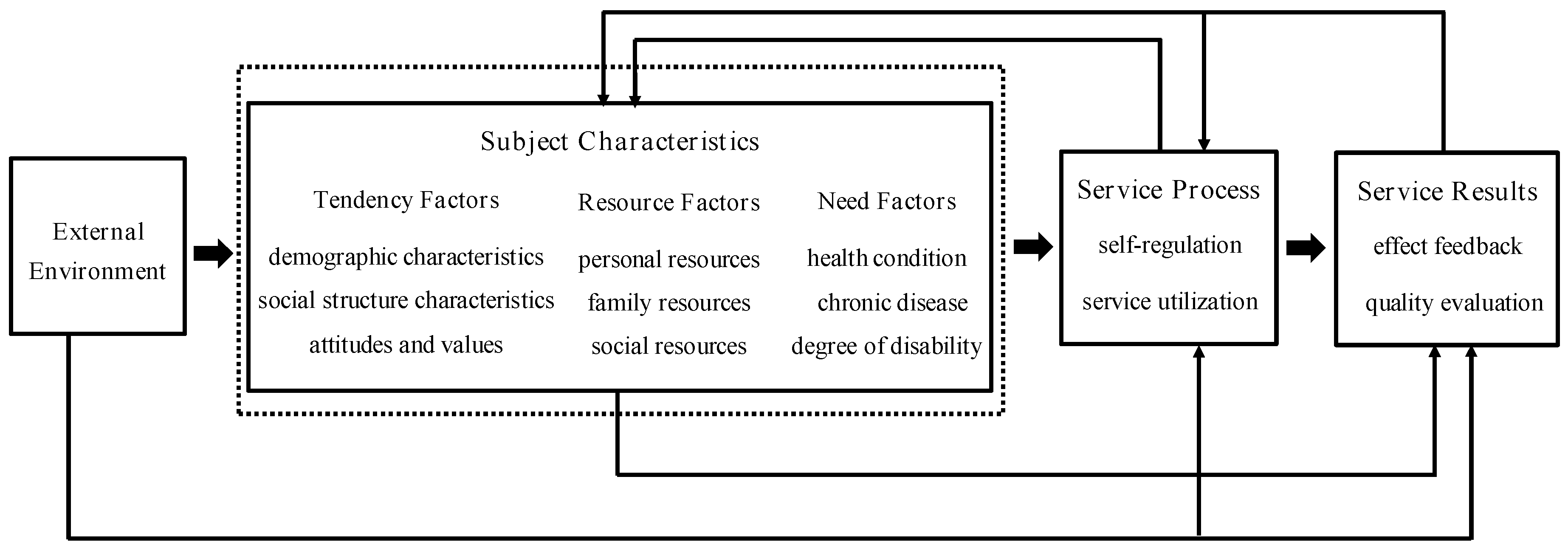
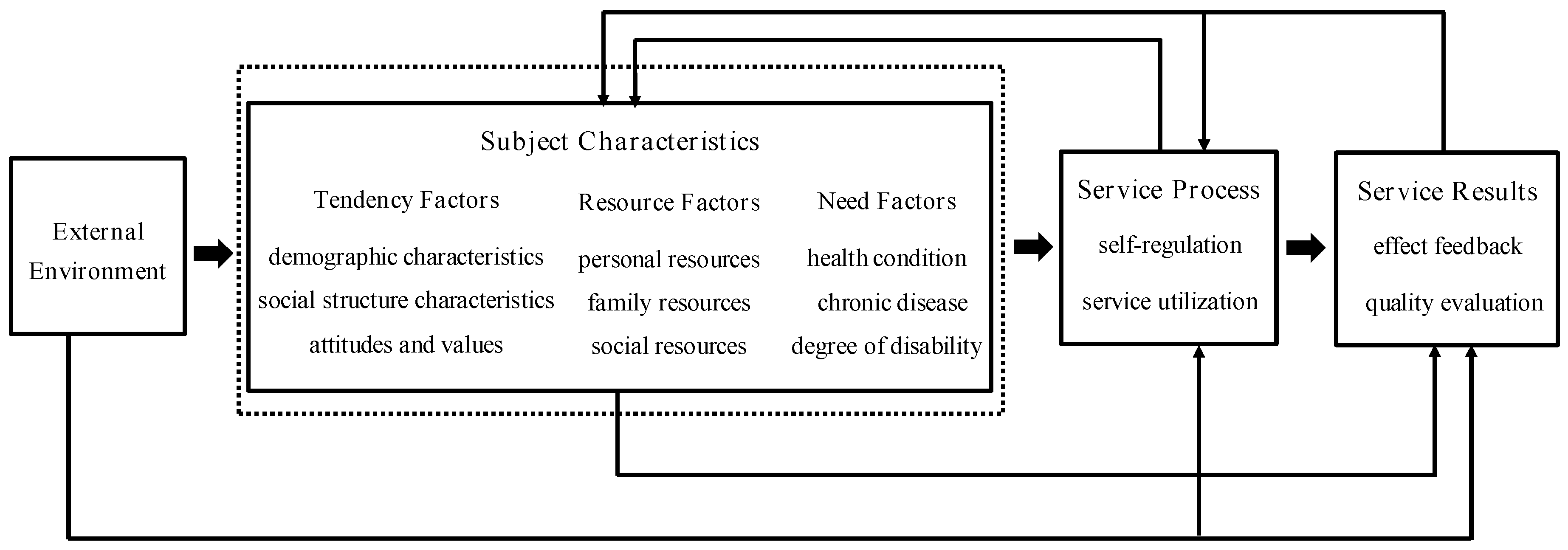
2.2. Theory and Hypotheses
3. Methods
3.1. Sampling
3.2. Descriptive Analysis
3.3. Measures
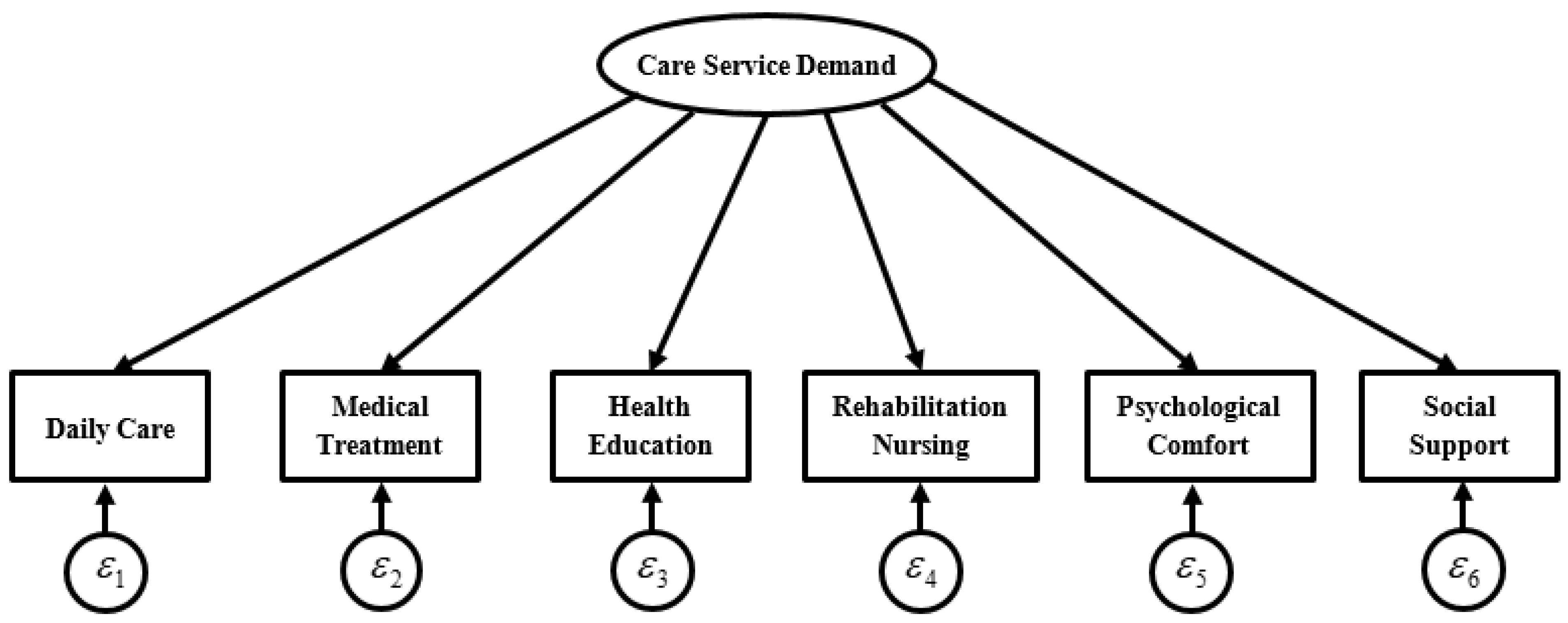
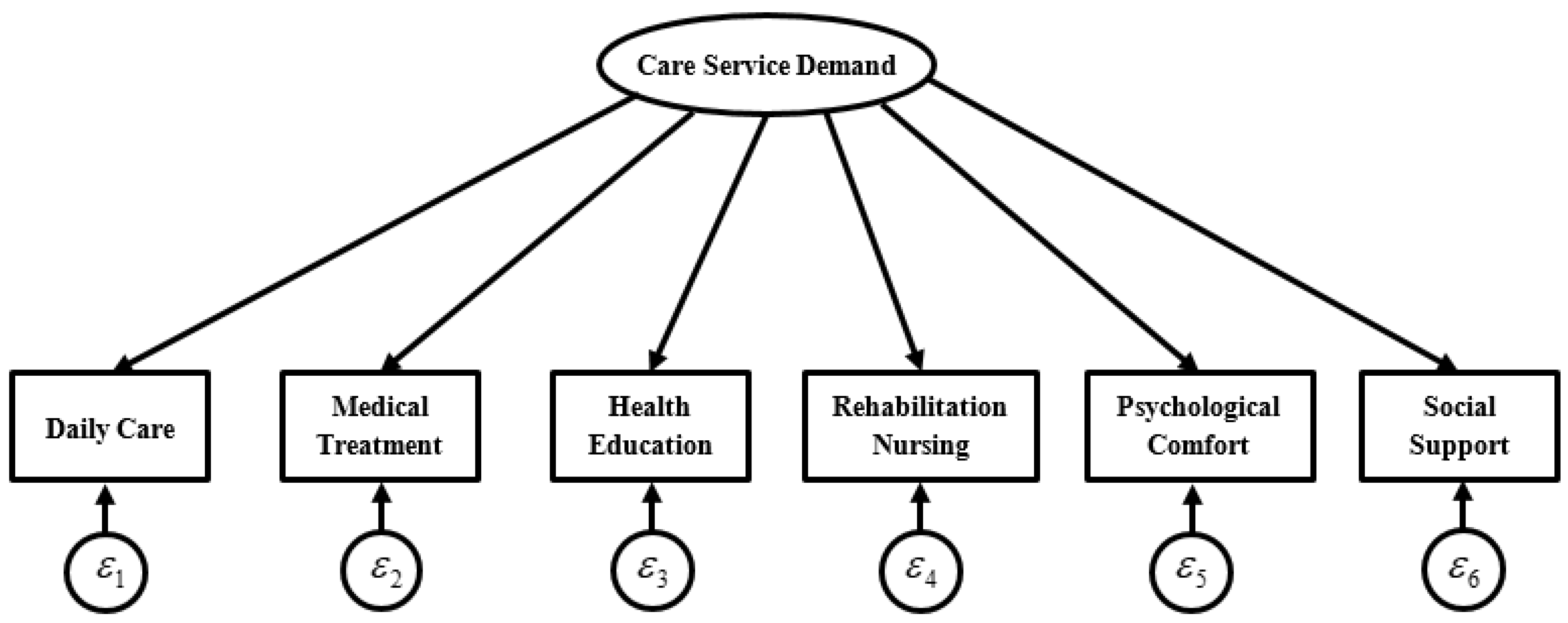
3.3.1. Explained Variable: Care Service Demand
3.3.2. Explanatory Variable
3.4. Data analysis Methods
3.4.1. Factor Analysis Method
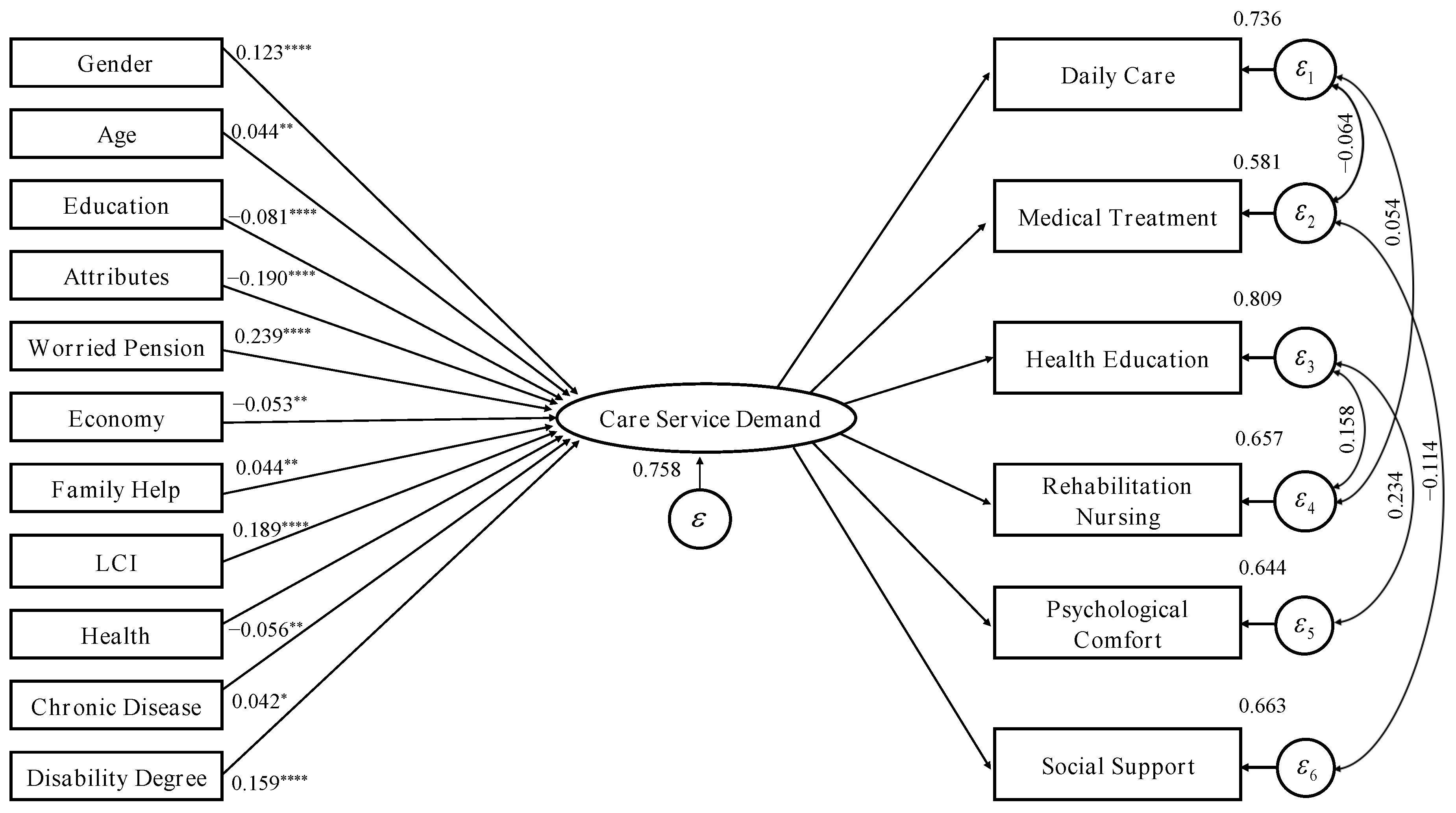
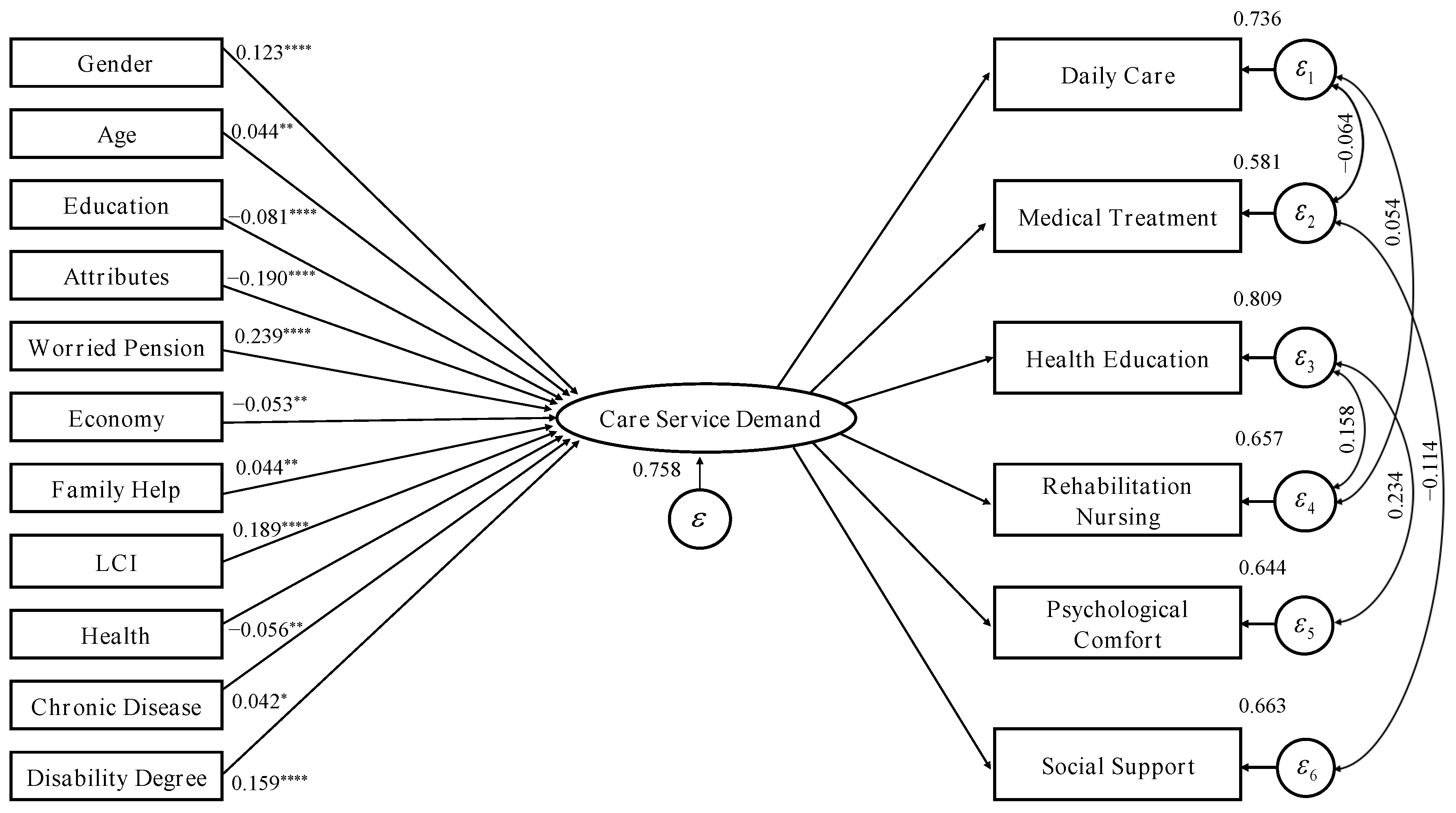
3.4.2. MIMIC Structural Equation Model
4. Results
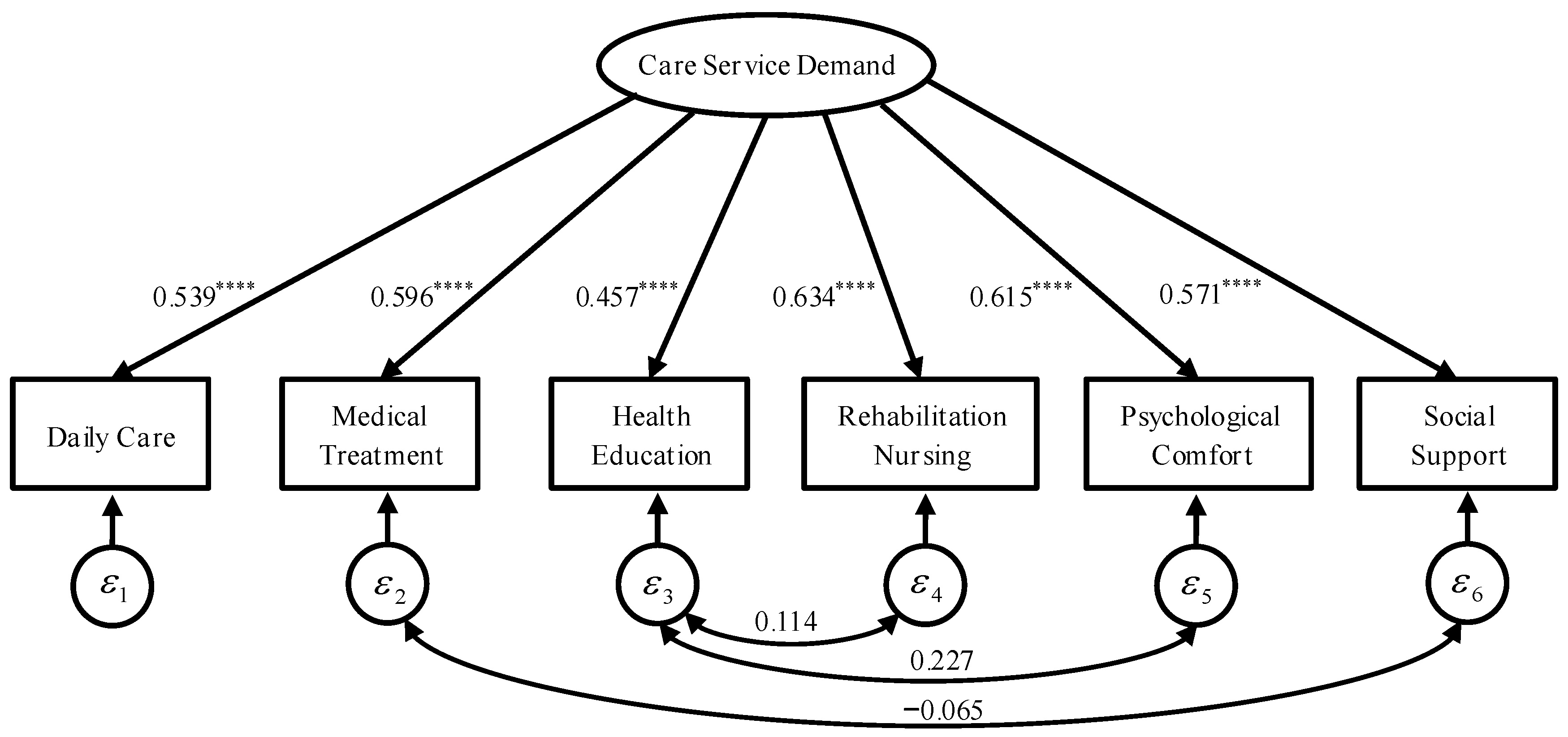
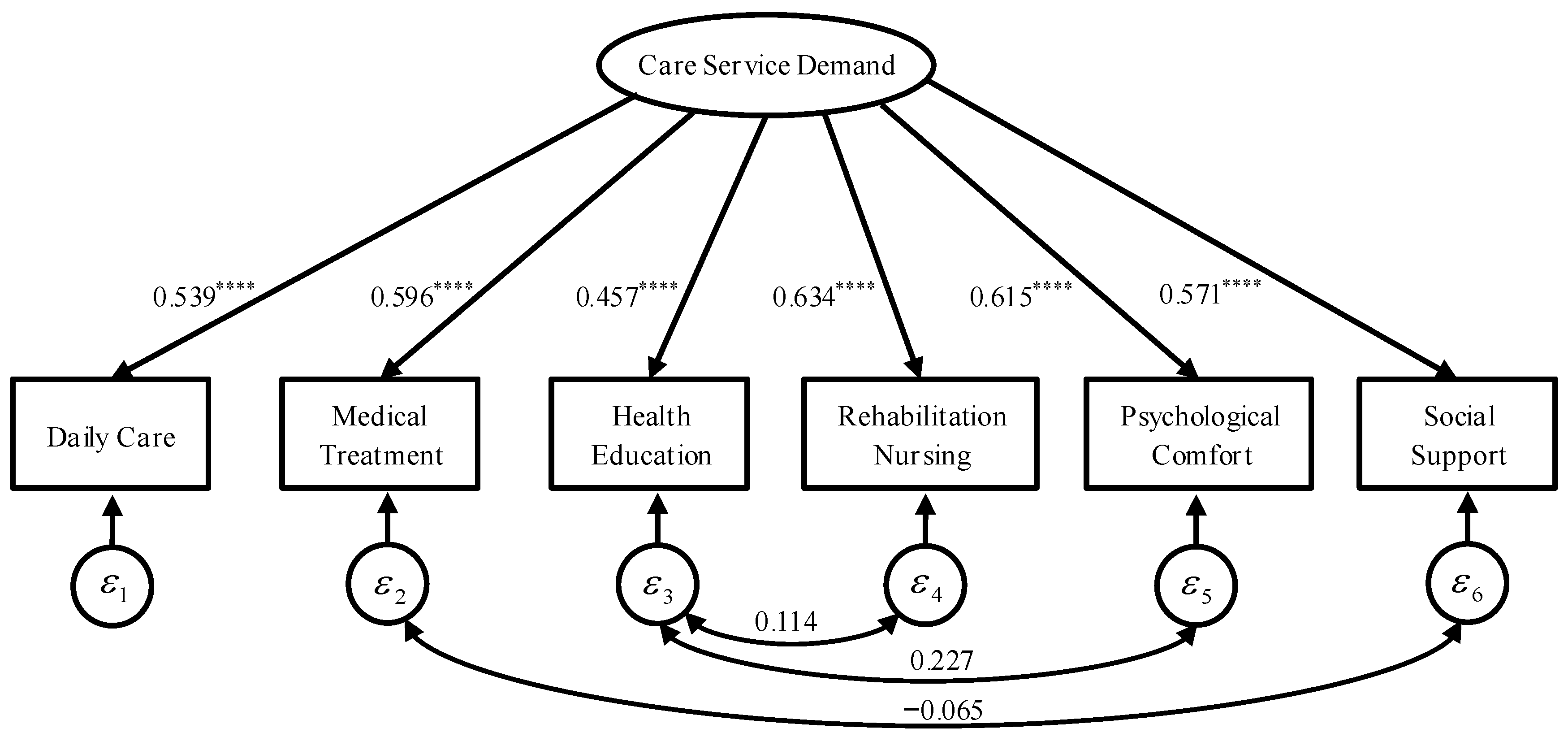
4.1. Measurement of Care Service Demand
4.2. Influencing Factor Model Estimation
4.3. Model Robustness Examination
4.4. Comparison of the Influencing Factors in Different Family Types
5. Discussion
6. Study Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The State Council Information Office. The State Information Office Held a Press Conference on 2021 National Economic Performance. Available online: https://www.scio.gov.cn/xwfbh/xwbfbh/wqfbh/47673/47722/index.htm (accessed on 4 March 2022).
- Office of the National Working Committee on Aging. Release of the Results of the Fourth Sampling Survey on the Living Conditions of the Elderly in Urban and Rural China. Available online: https://old.cnr.cn/2016csy/gundong/20161010/t20161010_523186698.shtm (accessed on 10 February 2022).
- Luo, Y.; Su, B.; Zheng, X. Trends and Challenges for Population and Health During Population Aging—China, 2015–2050. China CDC Wkly. 2021, 3, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ji, W.; Qian, C. The Development Trend of China’s Deep Aging and Demand for Elderly Care Services. Reform 2022, 2, 1–21. [Google Scholar]
- Han, Z.; Liang, Y. Research on the Construction of Long-term Care Insurance System for the Elderly in China—Necessity, Experience, Effect and Proposals. J. Southeast Univ. (Philos. Soc. Sci.) 2012, 14, 38–42. [Google Scholar]
- Dai, W. The System of Long-Term Care Insurance in Oecd Countries; China Social Sciences Press: Beijing, China, 2015. [Google Scholar]
- Zhou, Z. Family Pension and Family Pension Weakening in Demand Tension and Bridge. Northwest Popul. J. 2014, 35, 45–49. [Google Scholar]
- World Health Organization. Establishing an International Consensus on Long-Term Care Policies for the Elderly; World Health Organization: Geneva, Switzerland, 2000.
- Tang, J.; Feng, L. A Global Consensus and Concept Frame for Long-Term Care. Soc. Policy Res. 2021, 1, 18–38. [Google Scholar]
- General Office of the State Council. Several Opinions of The State Council on Accelerating the Development of Old-Age Service Industry. Available online: https://www.gov.cn/zwgk/2013-09/13/content_2487704.htm (accessed on 4 March 2022).
- National Healthcare Security Administration. The National Health Insurance Administration and the Ministry of Civil Affairs Issued Standards for the Evaluation of Long-Term Care Disability Levels. Available online: https://www.nhsa.gov.cn/art/2021/8/3/art_14_5693.html (accessed on 10 March 2022).
- He, W. Elderly care services: Expanding resources and optimizing allocation. Acad. Bimest. 2015, 1, 88–93. [Google Scholar]
- Jiang, C.; Zhang, J. Effect, Problems and Suggestions of Long-Term Care Insurance System in China. China Econ. Trade Her. 2020, 19, 29–33. [Google Scholar]
- Dai, W. Elderly demands for long-term care and its influencing factors—based on the survey of Anhui and Jiangsu. Popul. Res. 2011, 4, 86–94. [Google Scholar]
- Wang, X.; Zheng, C. Empirical analysis of the elderly health and long-term care. J. Shandong Univ. (Philos. Soc. Sci.) 2014, 3, 30–41. [Google Scholar]
- Zeng, W.; Hu, J.; Zhang, R.; Wu, Y. Social determinants of long-term care needs for rural needy elderly in China—taking Ankang as an example. J. Xi’an Jiaotong Univ. (Soc. Sci.) 2014, 4, 61–68. [Google Scholar]
- Tang, J.; Feng, L. Who needs long-term care insurance: Investigation and analysis of the long-term care needs of the disabled elderly. China Soc. Secur. 2016, 6, 26–27. [Google Scholar]
- Cao, Y.; Chen, J.; Lian, H.; Liu, P. The influencing factors of long-term care insurance demand in China: An empirical study based on Jiangsu Province. Chin. J. Health Policy 2018, 4, 19–23. [Google Scholar]
- Liao, X. The demand for long-term care services and its influencing factors in rural disabled elderly—An empirical evidence based on province Hunan. Popul. Dev. 2019, 1, 119–128. [Google Scholar]
- Chen, W. The reforms in tendance service system for senior citizen in developed countries and its use for reference. Nankai J. 2002, 3, 58–64. [Google Scholar]
- Pei, X.; Fang, L. Introduction to Long-Term Care for the Elderly; Social Science Literature Publishing House: Beijing, China, 2010. [Google Scholar]
- Zhang, Y. Long-Term Care for the Elderly: Institutional Selection and International Comparison; Economics and Management Press: Beijing, China, 2015. [Google Scholar]
- Dai, W. Research on the Construction of China’s Long-Term Care Service System; Social Science Literature Publishing House: Beijing, China, 2018. [Google Scholar]
- World Health Organization. Global report on aging and health. World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Zhu, W.; Guo, Y. An empirical analysis on the demand and influencing factors of the long-term care for the elders. Chin. Nurs. Manag. 2010, 12, 57–60. [Google Scholar]
- Zhou, Y. Influencing factors of demand for long-term care insurance of urban residents in China. Chin. J. Health Policy 2018, 4, 12–18. [Google Scholar]
- Lv, Y.; Zhao, X. An analysis of influencing factors of long-term care insurance demand of rural residents. Tax. Econ. 2020, 4, 51–56. [Google Scholar]
- Wang, X.; Li, X. Research on long-term care insurance demand forecast and insurance mechanism. Dongyue Trib. 2020, 1, 144–156. [Google Scholar]
- Gao, M. Demand measurement and satisfaction of long-term care services for urban and rural elderly groups: A case study in Zhejiang province. Soc. Work. Manag. 2019, 5, 61–67, +92. [Google Scholar]
- Zhu, Y.; Cheng, J. A probe into long-term care willingness and needs of the elderly in China: Based on sample survey of urban households. Welf. Res. 2019, 10, 17–26. [Google Scholar]
- Li, S.; Yang, Y. Multidimensional measurement and influencing factors of long-term care needs. Macroeconomics 2021, 1, 162–175. [Google Scholar]
- Gu, D.; Vlosky, D. Long-Term Care Needs and Related Issues in China. In Social Sciences in Health Care and Medicine; Nova Science Publishers, Inc.: Long Island, NY, USA, 2008; pp. 52–84. [Google Scholar]
- Peng, R.; Ling, L.; He, Q. Self-rated health status transition and long-term care need, of the oldest Chinese. Health Policy 2010, 97, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H. Unmet needs in long-term care and their associated factors among the oldest old in China. BMC Geriatr. 2015, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Wang, J. Unmet long-term care needs and depression: The double disadvantage of community-dwelling older people in rural China. Health Soc. Care Community 2019, 27, 126–138. [Google Scholar] [CrossRef]
- Meng, D.; Xu, G.; Davidson, P. Perceived unmet needs for community-based long-term care services among urban older adults: A cross sectional study. Geriatr. Nurs. 2021, 42, 740–747. [Google Scholar] [CrossRef]
- Landry, M.; Jagral, S.; Wodchis, W.; Cheryl, C. Analysis of factors affecting demand for rehabilitation services in Ontario, Canada: A health-policy perspective. Disabil. Rehabil. 2008, 24, 1837–1847. [Google Scholar] [CrossRef]
- Peng, X.; Song, L.; Huang, J. Determinants of long-term care services among disabled older adults in China: A quantitative study based on andersen’s Behavioral Model. Popul. Res. 2017, 4, 46–59. [Google Scholar]
- Li, M.; Yang, L. Research progress on long-term care needs and influencing factors of the disabled elderly. Nurs. Res. 2017, 20, 2440–2443. [Google Scholar]
- Lei, X.; Wang, X. The demand over-flow of long-term care for elderly in urban and rural areas: Theoretical analysis and empirical testing. Chin. J. Health Policy 2019, 7, 11–17. [Google Scholar]
- Hu, H.; Si, Y.; Li, B. Decomposing Inequality in long-term care Need Among Older Adults with Chronic Diseases in China: A Life Course Perspective. Int. J. Environ. Res. Public Health 2020, 7, 2559. [Google Scholar] [CrossRef] [PubMed]
- Nieboer, A.; Koolman, X.; Stolk, E. Preferences for long-term care services: Willingness to pay estimates derived from a discrete choice experiment. Soc. Sci. Med. 2010, 9, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yuan, C. Research on the demand for long-term care of the elderly and its influencing factors. Shandong Social Sciences 2015, 12, 67–72. [Google Scholar]
- Liu, Y.; Feng, Y.; Wang, Y. long-term care needs and influencing factors of the disabled elderly. Chin. J. Gerontol. 2016, 6, 1482–1484. [Google Scholar]
- Si, M.; Kong, F.; Wu, J.; Li, S. Review on the demand of long-term care of the elderly and its influencing factors. Chin. Health Serv. Manag. 2018, 2, 157–160. [Google Scholar]
- Sun, L.; Su, C.; Du, Q. Factors on rural elders’ decision—Making behavior of elderly caring. Popul. Dev. 2019, 6, 107–116. [Google Scholar]
- Zeng, Y.; Yuan, Z.; Fang, Y. Healthcare seeking behavior among Chinese older adults: Patterns and predicting factors. Chin. J. Health Stat. 2020, 2, 2969. [Google Scholar] [CrossRef]
- Chen, N.; Wang, C. Determinants of unmet need among disabled elderly living alone in China. Mod. Prev. Med. 2020, 1, 65–68. [Google Scholar]
- Yang, Y.; Jia, H. Measurement of the Chinese’s social health and its influencing factors: Based on MIMIC structural equation model. Chin. J. Health Policy 2018, 1, 28–36. [Google Scholar]
- Yin, S.; Du, P. The research of long-term care needs condition and tendency of the elderly. Popul. J. 2012, 2, 49–56. [Google Scholar]
- Xiao, Y.; Deng, R.; Liu, X. Differences and countermeasures between urban and rural areas in disability elders community home care services. Soc. Secur. Stud. 2014, 5, 24–31. [Google Scholar]
- Zhai, X.; Zhu, Q.; Li, H.; Li, Y. The elderly disability situation and influencing factors in Shandong Province. Chin. Nurs. Manag. 2016, 12, 1633–1638. [Google Scholar]
- Ding, H.; Yan, J. Research on disability rate estimation of Chinese elderly and its trend. Chin. J. Popul. Sci. 2018, 3, 97–108. [Google Scholar]
- Du, E.; Ning, P.; Du, C.; Wu, B.; Qiao, X. Study on the influence of education level on the life expectancy of the elderly in Shandong Province. Chin. J. Health Stat. 2021, 1, 51–53. [Google Scholar]
- Liu, Y.; Guo., H. A Study on the Old Age’s Worry About the Old People with Urban and Rural Integrated Subsistence Allowance. Res. Financ. Econ. Issues 2019, 10, 95–102. [Google Scholar]
- Ji, J. Can social care services substitute for the family cares for the elders?—An empirical analysis based on CLHLS Longitudinal Data. South China Popul. 2020, 3, 12. [Google Scholar]
- Liu, B.; Kou, E. The interaction mechanism of society care and family care under social elderly care trend. Popul. Econ. 2015, 1, 22–33. [Google Scholar]
- Cao, Y.; Du, P. Changing face of the extent to which needs were met among disabled older persons in China and its determinants. Popul. Dev. 2021, 1, 96–104. [Google Scholar]
- Kong, L.; Zhao, M.; Bao, C.; Luo, J.; Zhang, Z.; Wang, J. Analysis of the needs and influencing factors of home care services for the elderly in the community. J. Nurs. Sci. 2016, 7, 15–17. [Google Scholar]
- Tan, G.; Cui, M.; Yang, L.; Cheng, Y.; Hu, X.; Wang, F.; Feng, B.; Zhang, X.; Wu, Y.; Yao, D. Health care needs of elderly with chronic diseases in Guangxi and related factors. J. Nurs. Sci. 2019, 2, 69–72. [Google Scholar]
- Wu, F.; Fan, H.; Xiao, S.; Yang, X.; Xiao, Y.; Wu, Y. The demand for care and its influencing factors in community-dwelling disabled elderly in Beijing. Chin. J. Nurs. 2018, 7, 841–845. [Google Scholar]
- Lin, M.; Liang, Y.; Liu, L. Research on the Types, Demands and Service Support of China’s Poor Families—Based on the Investigation of the Project “Construction of Social Policy Support System for Families in Difficulty in China’s Urban and Rural Areas”. J. Tianjin Adm. Inst. 2014, 3, 3–11. [Google Scholar]
- Dai, W. The function change and value turn of Chinese family elder care. J. Anhui Norm. Univ. (Hum. Soc. Sci.) 2021, 1, 64–73. [Google Scholar]
- Jiang, X.; Liu, N.; Wei, M. Study on current life situation and community care service demand of disabled elders. Sci. Res. Aging 2014, 7, 30–36. [Google Scholar]
- Du, P. An analysis on the health status of the older persons in China. Popul. Econ. 2013, 6, 3–9. [Google Scholar]
- Cao, Y.; Wu, B.; Dai, J. Analysis of the elders’ long-term care arrangement and its influencing factors in rural China—Based on a comparative analysis between Shanghai and Hubei. J. Dalian Univ. Technol. (Soc. Sci.) 2014, 1, 117–123. [Google Scholar]
- He, W.; Yang, Y. Research on the subsidy system for the care services of the disabled elderly. Soc. Policy Res. 2020, 2, 26–39. [Google Scholar]
- He, W. Optimal allocation of resources in China’s social security system. Chin. Soc. Secur. Rev. 2018, 4, 3–13. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | PCFA | PFA | IPFA | |||
|---|---|---|---|---|---|---|
| Eigenvalue | Factor Loadings | Eigenvalue | Factor Loadings | Eigenvalue | Factor Loadings | |
| Factor 1 | 2.69 | 0.62 | 1.96 | 0.51 | 2.14 | 0.52 |
| Factor 2 | 0.82 | 0.66 | 0.06 | 0.55 | 0.25 | 0.56 |
| Factor 3 | 0.71 | 0.65 | −0.07 | 0.55 | 0.13 | 0.59 |
| Factor 4 | 0.67 | 0.72 | −0.07 | 0.63 | 0.04 | 0.67 |
| Factor 5 | 0.60 | 0.73 | −0.12 | 0.64 | 0.01 | 0.69 |
| Factor 6 | 0.51 | 0.64 | −0.20 | 0.53 | −0.0002 | 0.53 |
| Weighted Average | Eastern Region | Central Region | Western Region | Variance Analysis |
|---|---|---|---|---|
| Urban and Rural Weighted Average | 1.09 | 1.24 | 1.39 | F = 17.25 (p = 0.00 < 0.05) |
| Urban Weighted Average | 0.88 | 1.09 | 1.20 | F = 14.70 (p = 0.00 < 0.05) |
| Rural Weighted Average | 1.39 | 1.45 | 1.61 | F = 4.16 (p = 0.02 < 0.05) |
| Model | Estimation Methods | (1) | (2) | (3) | (4) | (5) | (6) |
|---|---|---|---|---|---|---|---|
| ml | ml + robust | mlmv + robust | bootstrap | gsem | jackknife | ||
| A. Structural Model | Gender | 0.06 **** | 0.06 **** | 0.05 **** | 0.06 **** | 0.35 **** | 0.06 **** |
| (5.21) | (5.21) | (5.11) | (5.23) | (5.07) | (5.19) | ||
| Age | 0.00 ** | 0.00 * | 0.00 | 0.00 * | 0.01 | 0.00 * | |
| (1.99) | (1.94) | (0.76) | (1.92) | (1.46) | (1.93) | ||
| Education | −0.02 **** | −0.02 **** | −0.02 *** | −0.02 **** | −0.10 *** | −0.02 **** | |
| (−3.43) | (−3.51) | (−3.24) | (−3.67) | (−2.65) | (−3.49) | ||
| Attributes | −0.09 **** | −0.09 **** | −0.10 **** | −0.09 **** | −0.54 **** | −0.09 **** | |
| (−7.91) | (−7.60) | (−8.85) | (−7.45) | (−7.40) | (−7.57) | ||
| Worried Pension | 0.11 **** | 0.11 **** | 0.06 **** | 0.11 **** | 0.72 **** | 0.11 **** | |
| (9.64) | (9.51) | (6.27) | (9.27) | (9.04) | (9.47) | ||
| Econmy | −0.01 ** | −0.01 ** | −0.02 ** | −0.01 ** | −0.08 * | −0.01 ** | |
| (−2.23) | (−2.24) | (−2.49) | (−2.23) | (−1.92) | (−2.23) | ||
| Family Help | 0.01 ** | 0.01 ** | 0.01 * | 0.01 ** | 0.05 ** | 0.01 ** | |
| (2.00) | (2.00) | (1.70) | (2.04) | (2.54) | (1.99) | ||
| LCI | 0.09 **** | 0.09 **** | 0.10 **** | 0.09 **** | 0.59 **** | 0.09 **** | |
| (8.07) | (8.33) | (8.57) | (8.08) | (7.94) | (8.30) | ||
| Health | −0.01 ** | −0.01 ** | −0.02 *** | −0.01 ** | −0.06 | −0.01 ** | |
| (−2.24) | (−2.23) | (−2.84) | (−2.24) | (−1.55) | (−2.22) | ||
| Chronic Disease | 0.01 * | 0.01 * | 0.01 ** | 0.01 * | 0.05 ** | 0.01 * | |
| (1.79) | (1.77) | (2.47) | (1.67) | (2.39) | (1.76) | ||
| Disability Degree | 0.05 **** | 0.05 **** | 0.07 **** | 0.05 **** | 0.26 **** | 0.05 **** | |
| (6.48) | (5.87) | (8.87) | (5.95) | (5.47) | (5.84) | ||
| B. Confirmatory Factor Model (Measurement Model) | Daily Care | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| _cons | 0.07 | 0.07 | 0.16 *** | 0.07 | — | 0.07 | |
| (1.09) | (1.08) | (2.74) | (1.06) | — | (1.08) | ||
| Medical Treatment | 1.42 **** | 1.42 **** | 1.32 **** | 1.42 **** | 1.32 **** | 1.42 **** | |
| (17.17) | (17.31) | (19.93) | (17.75) | (11.29) | (17.32) | ||
| _cons | 0.19 ** | 0.19 ** | 0.32 **** | 0.19 ** | — | 0.19 ** | |
| (2.32) | (2.31) | (4.21) | (2.26) | — | (2.30) | ||
| Health Education | 0.93 **** | 0.93 **** | 0.87 **** | 0.93 **** | 1.09 **** | 0.93 **** | |
| (13.67) | (12.88) | (14.66) | (12.41) | (11.14) | (12.89) | ||
| _cons | 0.18 *** | 0.18 *** | 0.25 **** | 0.18 *** | — | 0.18 *** | |
| (3.27) | (3.24) | (4.83) | (3.18) | — | (3.23) | ||
| Rehabilitation Nursing | 1.08 **** | 1.08 **** | 1.08 **** | 1.08 **** | 1.67 **** | 1.08 **** | |
| (17.69) | (16.73) | (20.18) | (16.70) | (10.98) | (16.76) | ||
| _cons | 0.01 | 0.01 | 0.10 | 0.01 | — | 0.01 | |
| (0.10) | (0.10) | (1.58) | (0.10) | — | (0.10) | ||
| Psychological Comfort | 1.29 **** | 1.29 **** | 1.21 **** | 1.29 **** | 1.59 **** | 1.29 **** | |
| (16.69) | (16.17) | (18.49) | (16.29) | (10.97) | (16.18) | ||
| _cons | 0.16 ** | 0.16 ** | 0.25 **** | 0.16 ** | — | 0.16 ** | |
| (2.05) | (2.03) | (3.61) | (1.99) | — | (2.02) | ||
| Social Support | 1.01 **** | 1.01 **** | 0.94 **** | 1.01 **** | 1.33 **** | 1.01 **** | |
| (16.10) | (15.32) | (16.78) | (15.42) | (11.16) | (15.35) | ||
| _cons | −0.01 | −0.01 | 0.06 | −0.01 | — | −0.01 | |
| (−0.18) | (−0.18) | (1.13) | (−0.17) | — | (−0.18) | ||
| C. Fit Metrics | n | 2362 | 2362 | 2917 | 2362 | 2365 | 2362 |
| R2 (CD) | 0.242 | 0.242 | 0.228 | 0.242 | — | 0.242 | |
| CFI | 0.941 | — | — | 0.941 | — | 0.941 | |
| RMSEA | 0.037 | — | — | 0.037 | — | 0.037 | |
| SRMR | 0.024 | 0.024 | — | 0.024 | — | 0.024 |
| Model | (1) | (2) | (3) |
|---|---|---|---|
| Difficult Families | Ordinary Families | Overall Families | |
| Gender | 0.256 **** | 0.015 | 0.216 **** |
| (5.53) | (0.16) | (5.23) | |
| Age | 0.005 * | 0.001 | 0.005 * |
| (1.67) | (0.10) | (1.69) | |
| Education | −0.076 *** | −0.015 | −0.068 *** |
| (−2.98) | (−0.34) | (−3.09) | |
| Attributes | −0.357 **** | −0.284 *** | −0.332 **** |
| (−7.58) | (−3.03) | (−7.93) | |
| Worried Pension | 0.442 **** | 0.497 **** | 0.452 **** |
| (9.66) | (5.68) | (11.14) | |
| Family Help | 0.031 ** | 0.027 | 0.027 ** |
| (2.06) | (0.96) | (2.09) | |
| LCI | 0.352 **** | 0.394 **** | 0.363 **** |
| (7.73) | (4.40) | (8.95) | |
| Health | −0.045 * | −0.081 | −0.052 ** |
| (−1.71) | (−1.54) | (−2.23) | |
| Chronic Disease | 0.027 ** | 0.016 | 0.026 ** |
| (2.02) | (0.56) | (2.13) | |
| Disability Degree | 0.200 **** | 0.065 | 0.185 **** |
| (6.54) | (0.90) | (6.62) | |
| _cons | 0.167 | 0.648 | 0.213 |
| (0.66) | (1.19) | (0.93) | |
| n | 1935 | 427 | 2362 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, H.; Xiao, S.; Hu, H.; He, H. Study on the Measurement and Influencing Factors of Care Service Demand of Disabled Elderly in Urban and Rural China. Int. J. Environ. Res. Public Health 2022, 19, 11112. https://doi.org/10.3390/ijerph191711112
Jiang H, Xiao S, Hu H, He H. Study on the Measurement and Influencing Factors of Care Service Demand of Disabled Elderly in Urban and Rural China. International Journal of Environmental Research and Public Health. 2022; 19(17):11112. https://doi.org/10.3390/ijerph191711112
Chicago/Turabian StyleJiang, Haixia, Suhua Xiao, Hongwei Hu, and Haotian He. 2022. "Study on the Measurement and Influencing Factors of Care Service Demand of Disabled Elderly in Urban and Rural China" International Journal of Environmental Research and Public Health 19, no. 17: 11112. https://doi.org/10.3390/ijerph191711112
APA StyleJiang, H., Xiao, S., Hu, H., & He, H. (2022). Study on the Measurement and Influencing Factors of Care Service Demand of Disabled Elderly in Urban and Rural China. International Journal of Environmental Research and Public Health, 19(17), 11112. https://doi.org/10.3390/ijerph191711112