
Long-Time Trend of Colorectal Cancer Mortality Attributable to High Processed Meat Intake in China and a Bayesian Projection from 2020 to 2030: A Model-Based Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Data
2.2. Definitions of Measurements
2.3. Statistical Analysis
2.3.1. Age-Period-Cohort Model
2.3.2. Joinpoint Analysis
2.3.3. Bayesian Age-Period-Cohort Analysis
3. Results
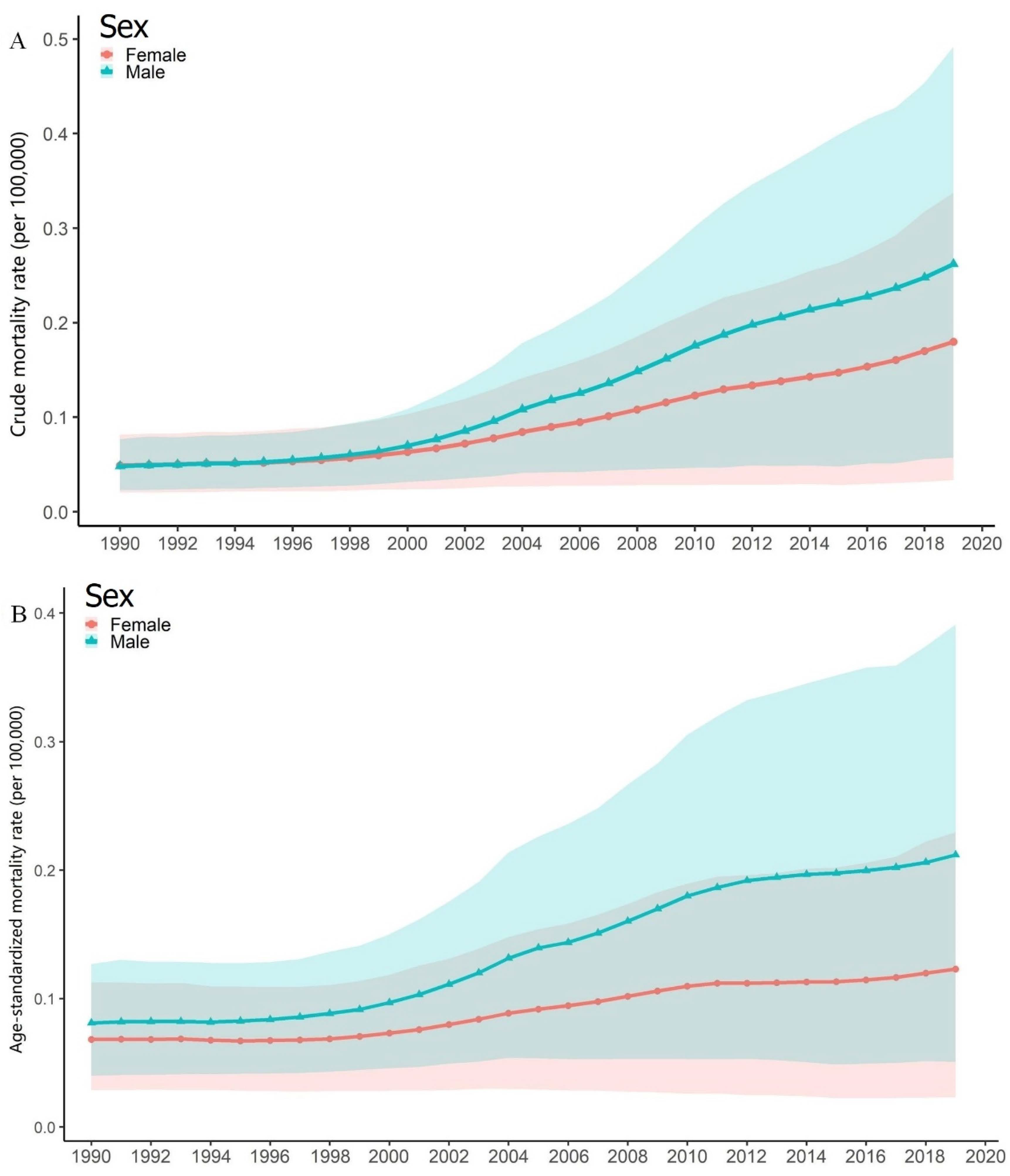
3.1. General Trend of the Attributed CRC Mortality
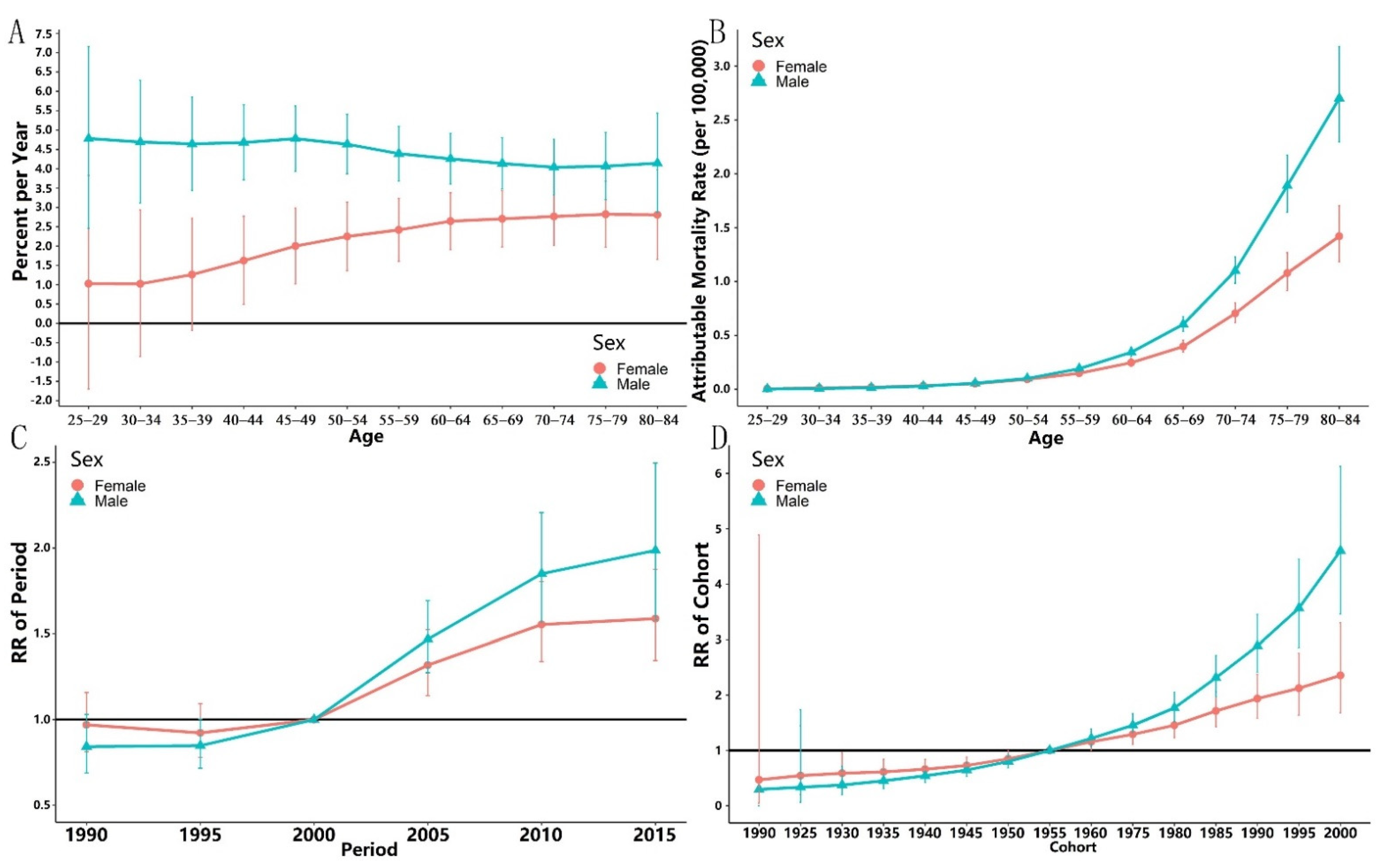
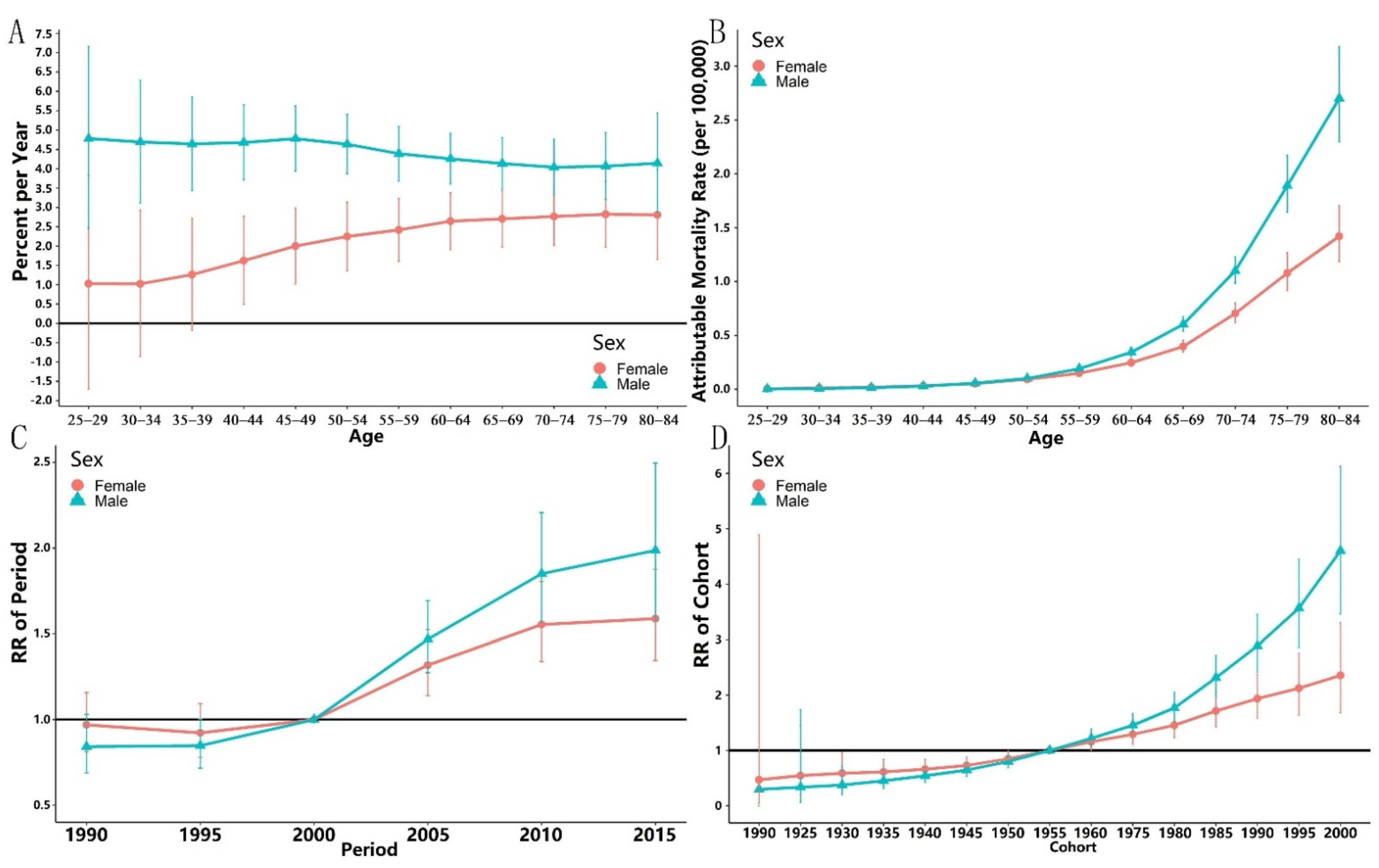
3.2. Local and Net Drifts
3.3. Age-Period-Cohort Analysis
3.4. Joinpoint Analysis
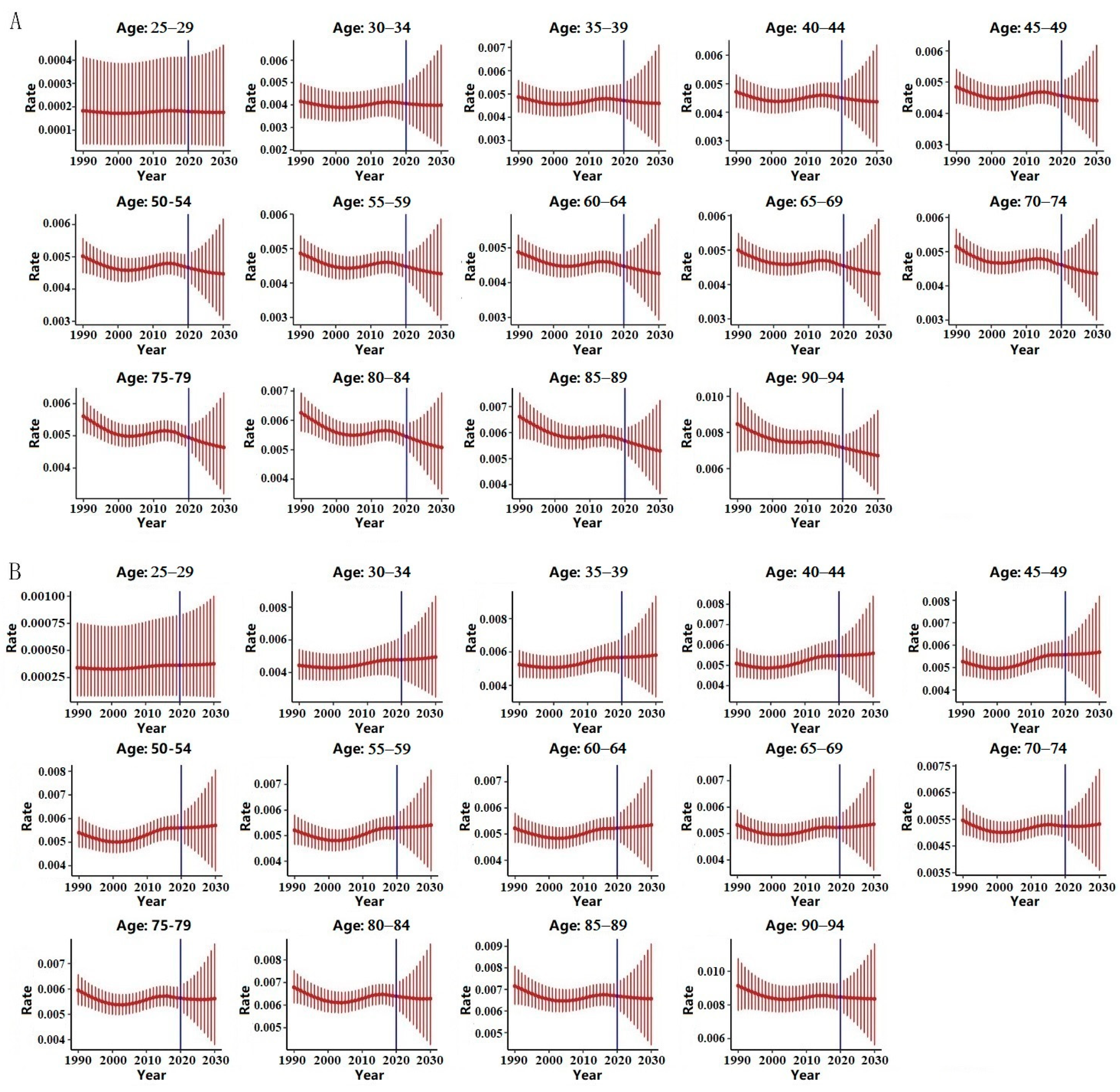
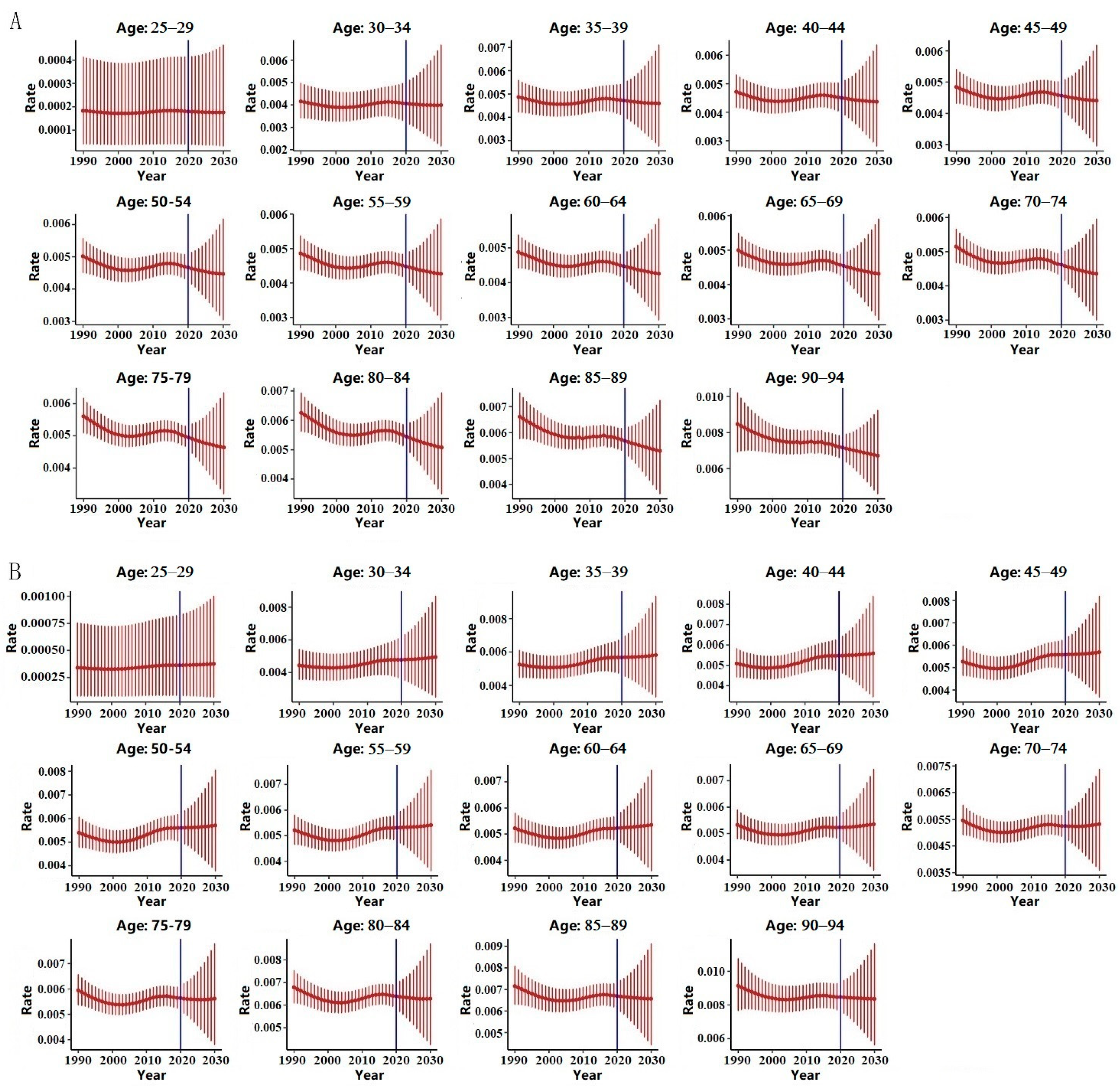
3.5. Bayesian Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Tang, Z.; Jiang, Y.; Huang, H.; Luo, P.; Qing, B.; Zhang, S.; Tang, R. IL-8 Is Involved in Estrogen-Related Receptor α-Regulated Proliferation and Migration of Colorectal Cancer Cells. Dig. Dis. Sci. 2017, 62, 3438–3446. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Ding, H.; Wang, J.; Chan, P.; Huang, J. Prevalence and risk factors of colorectal cancer in Asia. Intest. Res. 2019, 17, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Zhang, S.; Zeng, H.; Wang, S.; Sun, K.; Chen, R. Cancer incidence and mortality in China, 2016. J. Natl. Cancer Cent. 2022, 2, 1–9. [Google Scholar] [CrossRef]
- Li, Z. A Retrospective Study of Advanced Early-Onset Colorectal Cancer Later-Onset Colorectal Cancer. Master’s Thesis, Chinese China Academy of Chinese Medical Sciences, Beijing China, 2020. [Google Scholar]
- Kim, S.; Kim, H.; Lee, J.; Park, S.; Lim, H.; Park, Y. The impact of microsatellite instability status and sidedness of the primary tumor on the effect of bevacizumab-containing chemotherapy in patients with metastatic colorectal cancer. J. Cancer 2018, 9, 1791–1796. [Google Scholar] [CrossRef]
- Yang, L.; Xiong, Z.; Xie, Q.; He, W.; Liu, S.; Kong, P.; Jiang, C.; Guo, G.; Xia, L. Prognostic value of total number of lymph nodes retrieved differs between left-sided colon cancer and right-sided colon cancer in stage III patients with colon cancer. BMC Cancer 2018, 18, 558. [Google Scholar] [CrossRef]
- Chai, X.; Li, Y.; Yin, Z.; Wu, F.; Hu, P.; Liu, X.; Tong, S.; Zhuang, P.; Zhang, Y.; Zheng, W.; et al. Association of Meat Subtypes with Colorectal Polyp Prevalence: Finding from the Lanxi Pre-colorectal Cancer Cohort in China. Front. Nutr. 2022, 9, 833571. [Google Scholar] [CrossRef]
- Galanakis, C. Sustainable Meat Production and Processing, 1st ed.; Academic Press: London, UK, 2018; pp. 18–22. [Google Scholar]
- Jang, Y.; Lee, H.; Kim, B.; Lee, Y.; Lee, H.; Moon, J.; Kim, C.I. Revised dietary guidelines for Koreans. Asia Pac. J. Clin. Nutr. 2008, 17 (Suppl. S1), 55–58. [Google Scholar]
- Chinese Nutrition Society. The Chinese Dietary Guidelines; People’s Health Publishing House Co., Ltd.: Beijing, China, 2016. [Google Scholar]
- Bouvard, V.; Loomis, D.; Guyton, K.; Grosse, Y.; Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef]
- Huang, Y.; Cao, D.; Chen, Z.; Chen, B.; Li, J.; Guo, J.; Dong, Q.; Liu, L.; Wei, Q. Red and processed meat consumption and cancer outcomes: Umbrella review. Food Chem. 2021, 356, 129697. [Google Scholar] [CrossRef]
- Cheng, T.; Chaousis, S.; Gamage, S.; Lam, A.; Gopalan, V. Polycyclic Aromatic Hydrocarbons Detected in Processed Meats Cause Genetic Changes in Colorectal Cancers. Int. J. Mol. Sci. 2021, 22, 10959. [Google Scholar] [CrossRef] [PubMed]
- Ullah, H.; Hussain, Y.; Santarcangelo, C.; Baldi, A.; Di Minno, A.; Khan, H.; Xiao, J.; Daglia, M. Natural Polyphenols for the Preservation of Meat and Dairy Products. Molecules 2022, 27, 1906. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.; Coulter, S.; Yoshihara, E.; Oh, T.; Fang, S.; Cayabyab, F.; Zhu, Q.; Zhang, T.; Leblanc, M.; Liu, S.; et al. FXR Regulates Intestinal Cancer Stem Cell Proliferation. Cell 2019, 176, 1098–1112.e18. [Google Scholar] [PubMed]
- Cavestro, G.; Mannucci, A.; Zuppardo, R.; Leo, M.; Stoffel, E.; Tonon, G. Early onset sporadic colorectal cancer: Worrisome trends and oncogenic features. Dig. Liver Dis. 2018, 50, 521–532. [Google Scholar] [PubMed]
- Gausman, V.; Dornblaser, D.; Anand, S.; Hayes, R.; O’Connell, K.; Du, M.; Liang, P.S. Risk Factors Associated with Early-Onset Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 2752–2759.e2. [Google Scholar] [PubMed]
- Chouhan, H.; Ferrandon, S.; DeVecchio, J.; Kalady, M.; Church, J. A Changing Spectrum of Colorectal Cancer Biology with Age: Implications for the Young Patient. Dis. Colon. Rectum. 2019, 62, 21–26. [Google Scholar]
- GBD 2019 Viewpoint Collaborators. Five insights from the Global Burden of Disease Study 2019. Lancet 2020, 396, 1135–1159. [Google Scholar]
- Kocarnik, J.; Compton, K.; Dean, F.; Fu, W.; Gaw, B.; Global Burden of Disease 2019 Cancer Collaboration. Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar]
- Global Burden of Disease Study 2019 (GBD 2019). Data Input Sources Tool. Available online: https://ghdx.healthdata.org/gbd-2019/data-input-sources (accessed on 15 March 2022).
- World Health Organization. International Classification of Diseases: 9th Revision, Basic Tabulation List with Alphabetic Index. Available online: https://apps.who.int/iris/handle/10665/39473 (accessed on 1 March 2021).
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed. Available online: https://apps.who.int/iris/handle/10665/42980 (accessed on 1 March 2021).
- Newman, C. Biostatical Methods in Epidemiology; John Wiley & Sons, Inc.: New York, NY, USA, 2003; pp. 249–262. [Google Scholar]
- Rosenberg, P.; Check, D.; Anderson, W. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2296–2302. [Google Scholar]
- Riebler, A.; Held, L. Projecting the future burden of cancer: Bayesian age-period-cohort analysis with integrated nested Laplace approximations. Biom. J. 2017, 59, 531–549. [Google Scholar]
- Sun, C.; Liu, Y.; Li, B.; Rang, W. Colorectal Cancer Incidence and Mortality Trends and Analysis of Risk Factors in China from 2005 to 2015. Int. J. Gen. Med. 2021, 14, 9965–9976. [Google Scholar] [CrossRef] [PubMed]
- Fan, X. Study on the Relationship between Red Meat, Dietary Neu5Gc Intake and Anti-Neu5Gc Antibody. Master’s Thesis, Xiamen University, Xiamen, China, 2015. [Google Scholar]
- Cheng, Y.; Liu, X.; Kang, B.; Tao, W.; Wei, Z.; Peng, D. Comparison of surgical and oncologic outcomes in very elderly patients (≥80 years old) and elderly (65–79 years old) colorectal cancer patients: A propensity score matching. BMC Gastroenterol. 2022, 22, 205. [Google Scholar] [CrossRef] [PubMed]
- Salazar, N.; Valdés-Varela, L.; González, S.; Gueimonde, M.; de Los Reyes-Gavilán, C.G. Nutrition and the gut microbiome in the elderly. Gut Microbes 2017, 8, 82–97. [Google Scholar] [CrossRef]
- Early Diagnosis and Early Treatment Guidelines Development Expert Group, National Cancer Center China Colorectal Cancer Screening. China guideline for the screening, early detection and early treatment of colorectal cancer. Chin. J. Oncol. 2020, 43, 16–38. [Google Scholar] [CrossRef]
- Qu, C.; Tao, C.; Niu, L.; Wang, S.; Zhao, B.; Guo, Y. Status of and Trends in the Meat Processing Industry in China during the 13th Five-Year Plan Period. Meat Res. 2021, 11, 44–49. [Google Scholar]
- Li, A.; Li, W.; Teng, X.; Zhai, H.; Wang, Y.; Jia, Z. Investigation on Meat Consumption in China. China Anim. Health Insp. 2020, 37, 35–38. [Google Scholar] [CrossRef]
- Zhang, S. Research on Chinese Standard System for Meat and Meat Products. Ph.D. Thesis, China Agricultural University, Beijing, China, 2007. [Google Scholar]
- National Health Commision of the P. R. China. National Food Safety Standard of the P. R. China—Cured Meat Products GB2730-2015. Available online: http://www.nhc.gov.cn/sps/s7891/201510/3ba3419aab8a41a09f4f924788f73793.shtml (accessed on 30 October 2015).
- National Health Commision of the P. R. China. National Food Safety Standard of the P. R. China—Cooked Meat Products GB2726-2016. Available online: http://www.nhc.gov.cn/sps/s7891/201701/77b8a50e61c94522a589b925dc3b994f.shtml (accessed on 9 January 2017).
- Wrobel, P.; Ahmed, S. Current status of immunotherapy in metastatic colorectal cancer. Int. J. Colorectal. Dis. 2019, 34, 13–25. [Google Scholar] [CrossRef]
- Kanani, A.; Veen, T.; Søreide, K. Neoadjuvant immunotherapy in primary and metastatic colorectal cancer. Br. J. Surg. 2021, 108, 1417–1425. [Google Scholar] [CrossRef]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Brändstedt, J.; Wangefjord, S.; Nodin, B.; Eberhard, J.; Jirström, K.; Manjer, J. Associations of hormone replacement therapy and oral contraceptives with risk of colorectal cancer defined by clinicopathological factors, beta-catenin alterations, expression of cyclin D1, p53, and microsatellite-instability. BMC Cancer 2014, 14, 371. [Google Scholar] [CrossRef]
- Colorectal Cancer Professional Committee of China Anti-Cancer Association. Changes in gender, age and location of colorectal cancer patients in China: Preliminary analysis of 31,246 cases in 18 hospitals. In Proceedings of the 2009 Eurasian Conference on Colorectal Surgery, Guangzhou, China, 1 November 2009; pp. 14–19. Available online: https://d.wanfangdata.com.cn/conference/7213021 (accessed on 27 June 2010).
- Patel, S.; Murphy, C.; Lieu, C.; Hampel, H. Early age onset colorectal cancer. Adv. Cancer Res. 2021, 151, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Yu, W. Analysis of the Clinical Characteristics of Colorectal Cancer in Female Patients. Master’s Thesis, Shandong University, Jinan, China, 2020. [Google Scholar]
- Shi, J. Status of Cancer Incidence and Mortality in Hebei Province, 2014 and Incidence Prediction for the Main Cancers. Master’s Thesis, Hebei Medical University, Shijiazhuang, China, 2017. [Google Scholar]
- Bray, F.; Møller, B. Predicting the future burden of cancer. Nat. Rev. Cancer 2006, 6, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y. Meat industry in China—Statistics & Facts. Available online: https://www.statista.com/topics/5264/meat-industry-in-china (accessed on 16 April 2022).
- Onyon, E.; Hsu, W.; Chang, L.; Lee, Y.; Wu, M.; Chiu, H. The Rise of Colorectal Cancer in Asia: Epidemiology, Screening, and Management. Curr. Gastr. Rep. 2019, 21, 36. [Google Scholar] [CrossRef]
- World Health Organization. Latest Global Cancer Data: Cancer Burden Rises to 19.3 Million New Cases and 10.0 Million Cancer Deaths in 2020. Available online: https://www.iarc.fr/fr/news-events/latest-global-cancer-data-cancer-burden-rises-to-19-3-million-new-cases-and-10-0-million-cancer-deaths-in-2020/ (accessed on 16 December 2020).
- Pauw, R.; Claessens, M.; Gorasso, V.; Drieskens, S.; Faes, C.; Devleesschauwer, B. Past, present, and future trends of overweight and obesity in Belgium using Bayesian ageperiod-cohort models. BMC Public Health 2022, 22, 1309. [Google Scholar] [CrossRef]
- Chen, N.; Fong, D.; Wong, J. Trends in Musculoskeletal Rehabilitation Needs in China From 1990 to 2030: A Bayesian Age-Period-Cohort Modeling Study. Front. Public Health 2022, 10, 869239. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Yang, D.; Wu, Y.; Xue, W.; Li, D.; Zhang, J.; He, Y.-Q.; Jia, W.-H. Burden, trends, and risk factors for breast cancer in China from 1990 to 2019 and its predictions until 2034: An up-to-date overview and comparison with those in Japan and South Korea. BMC Cancer 2022, 22, 826. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Age-Standardized Mortality Rates (ASMRs) | Crude Mortality Rates (CMRs) | ||||||
|---|---|---|---|---|---|---|---|
| Time Period | AVPC (95%CI) | t (p) | Time Period | AVPC (95%CI) | t (p) | ||
| Female | Trend 1 | 1990~1997 | −0.2 (−0.4,0) | −2.7 (0.020) | 1990~1997 | 1.5 (1.3,1.7) | 15.0 (<0.001) |
| Trend 2 | 1997~2000 | 2.5 (1.1,3.9) | 3.9 (0.002) | 1997~2001 | 5.4 (4.7,6.1) | 17.2 (<0.001) | |
| Trend 3 | 2000~2004 | 5.2 (4.5,5.8) | 17.4 (<0.001) | 2001~2004 | 8.1 (6.9,9.2) | 15.4 (<0.001) | |
| Trend 4 | 2004~2011 | 3.5 (3.3,3.7) | 41.5 (<0.001) | 2004~2011 | 6.4 (6.2,6.5) | 97.0 (<0.001) | |
| Trend 5 | 2011~2016 | 0.2 (−0.1,0.5) | 1.5 (0.146) | 2011~2016 | 3.3 (3.1,3.5) | 34.0 (<0.001) | |
| Trend 6 | 2016~2019 | 2.6 (2.1,3.2) | 11.0 (<0.001) | 2016~2019 | 5.6 (5.3,5.9) | 40.8 (<0.001) | |
| AAPC | - | 2.0 (1.9,2.2) | 22.7 (<0.001) | - | 4.6 (4.4,4.8) | 59.2 (<0.001) | |
| Male | Trend 1 | 1990~1996 | 0.3 (−0.4,1.0) | 1.0 (0.342) | 1990~1996 | 1.8 (1.1,2.5) | 5.7 (<0.001) |
| Trend 2 | 1996~2000 | 3.6 (1.8,5.5) | 4.3 (0.001) | 1996~2000 | 6.3 (4.6,8.1) | 8.2 (<0.001) | |
| Trend 3 | 2000~2004 | 8.1 (6.6,9.7) | 11.3 (<0.001) | 2000~2004 | 11.9 (10.6,13.3) | 20.2 (<0.001) | |
| Trend 4 | 2004~2011 | 5.4 (5,5.8) | 28.7 (<0.001) | 2004~2011 | 8.4 (8.2,8.7) | 66.8 (<0.001) | |
| Trend 5 | 2011~2019 | 1.4 (1.1,1.6) | 12.7 (<0.001) | 2011~2017 | 3.8 (3.5,4) | 30.9 (<0.001) | |
| Trend 6 | - | - | - | 2017~2019 | 5.0 (3.9,6.1) | 10.3 (<0.001) | |
| AAPC | - | 3.3 (3,3.7) | 19.2 (<0.001) | - | 6.0 (5.7,6.3) | 38.2 (<0.001) | |
| Age Group | Rate (95%CI) | ||
|---|---|---|---|
| 2019 | 2020 | 2030 | |
| 25–29 | 0.00018 (0.00004,0.00041) | 0.00018 (0.00004,0.00041) | 0.00018 (0.00003,0.00046) |
| 30–34 | 0.00408 (0.00331,0.00495) | 0.00406 (0.00323,0.00502) | 0.00399 (0.00217,0.00667) |
| 35–39 | 0.00474 (0.00411,0.00541) | 0.00472 (0.00402,0.00548) | 0.00460 (0.00277,0.00710) |
| 40–44 | 0.00452 (0.00404,0.00503) | 0.00450 (0.00397,0.00507) | 0.00437 (0.00282,0.00636) |
| 45–49 | 0.00458 (0.00418,0.00501) | 0.00457 (0.00411,0.00505) | 0.00441 (0.00296,0.00618) |
| 50–54 | 0.00469 (0.00433,0.00507) | 0.00466 (0.00424,0.00511) | 0.00447 (0.00305,0.00617) |
| 55–59 | 0.00450 (0.00418,0.00484) | 0.00448 (0.00409,0.00488) | 0.00427 (0.00293,0.00586) |
| 60–64 | 0.00450 (0.00419,0.00482) | 0.00447 (0.00410,0.00487) | 0.00426 (0.00293,0.00583) |
| 65–69 | 0.00457 (0.00427,0.00488) | 0.00454 (0.00417,0.00492) | 0.00431 (0.00297,0.00590) |
| 70–74 | 0.00464 (0.00435,0.00494) | 0.00461 (0.00425,0.00500) | 0.00436 (0.00301,0.00595) |
| 75–79 | 0.00498 (0.00466,0.00530) | 0.00494 (0.00455,0.00535) | 0.00464 (0.00320,0.00633) |
| 80–84 | 0.00549 (0.00514,0.00586) | 0.00545 (0.00501,0.00590) | 0.00508 (0.00350,0.00694) |
| 85–89 | 0.00573 (0.00532,0.00616) | 0.00568 (0.00520,0.00619) | 0.00530 (0.00365,0.00724) |
| 90–94 | 0.00721 (0.00661,0.00784) | 0.00717 (0.00649,0.00788) | 0.00672 (0.00462,0.00922) |
| Age Group | Rate (95%CI) | ||
|---|---|---|---|
| 2019 | 2020 | 2030 | |
| 25–29 | 0.00036 (0.00009,0.00082) | 0.00036 (0.00008,0.00083) | 0.00038 (0.00007,0.00100) |
| 30–34 | 0.00478 (0.00368,0.00606) | 0.00478 (0.00360,0.00618) | 0.00495 (0.00250,0.00868) |
| 35–39 | 0.00566 (0.00473,0.00670) | 0.00567 (0.00465,0.00682) | 0.00581 (0.00330,0.00933) |
| 40–44 | 0.00547 (0.00475,0.00625) | 0.00547 (0.00469,0.00633) | 0.00558 (0.00344,0.00840) |
| 45–49 | 0.00557 (0.00497,0.00621) | 0.00557 (0.00491,0.00630) | 0.00568 (0.00368,0.00818) |
| 50–54 | 0.00560 (0.00506,0.00617) | 0.00560 (0.00500,0.00625) | 0.00571 (0.00378,0.00805) |
| 55–59 | 0.00530 (0.00485,0.00577) | 0.00530 (0.00478,0.00586) | 0.00541 (0.00362,0.00756) |
| 60–64 | 0.00521 (0.00479,0.00566) | 0.00523 (0.00473,0.00575) | 0.00535 (0.00360,0.00744) |
| 65–69 | 0.00522 (0.00482,0.00564) | 0.00523 (0.00475,0.00573) | 0.00535 (0.00361,0.00743) |
| 70–74 | 0.00525 (0.00486,0.00565) | 0.00525 (0.00478,0.00574) | 0.00532 (0.00359,0.00737) |
| 75–79 | 0.00565 (0.00524,0.00607) | 0.00564 (0.00514,0.00616) | 0.00561 (0.00380,0.00778) |
| 80–84 | 0.00641 (0.00594,0.00690) | 0.00639 (0.00582,0.00699) | 0.00628 (0.00425,0.00871) |
| 85–89 | 0.00671 (0.00619,0.00727) | 0.00669 (0.00607,0.00735) | 0.00657 (0.00443,0.00910) |
| 90–94 | 0.00847 (0.00772,0.00926) | 0.00847 (0.00762,0.00937) | 0.00836 (0.00563,0.01162) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, F.; Chen, S.; Luo, Y.; Si, A.; Yang, Y.; Li, Y.; Hu, W.; Zhang, Y. Long-Time Trend of Colorectal Cancer Mortality Attributable to High Processed Meat Intake in China and a Bayesian Projection from 2020 to 2030: A Model-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 10603. https://doi.org/10.3390/ijerph191710603
Chen F, Chen S, Luo Y, Si A, Yang Y, Li Y, Hu W, Zhang Y. Long-Time Trend of Colorectal Cancer Mortality Attributable to High Processed Meat Intake in China and a Bayesian Projection from 2020 to 2030: A Model-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(17):10603. https://doi.org/10.3390/ijerph191710603
Chicago/Turabian StyleChen, Fangyao, Shiyu Chen, Yaqi Luo, Aima Si, Yuhui Yang, Yemian Li, Weiwei Hu, and Yuxiang Zhang. 2022. "Long-Time Trend of Colorectal Cancer Mortality Attributable to High Processed Meat Intake in China and a Bayesian Projection from 2020 to 2030: A Model-Based Study" International Journal of Environmental Research and Public Health 19, no. 17: 10603. https://doi.org/10.3390/ijerph191710603
APA StyleChen, F., Chen, S., Luo, Y., Si, A., Yang, Y., Li, Y., Hu, W., & Zhang, Y. (2022). Long-Time Trend of Colorectal Cancer Mortality Attributable to High Processed Meat Intake in China and a Bayesian Projection from 2020 to 2030: A Model-Based Study. International Journal of Environmental Research and Public Health, 19(17), 10603. https://doi.org/10.3390/ijerph191710603