

Sex Differences in Age-Associated Rate of Decline in Grip Strength When Engaging in Vigorous Physical Activity



Abstract
:1. Introduction
2. Materials and Methods
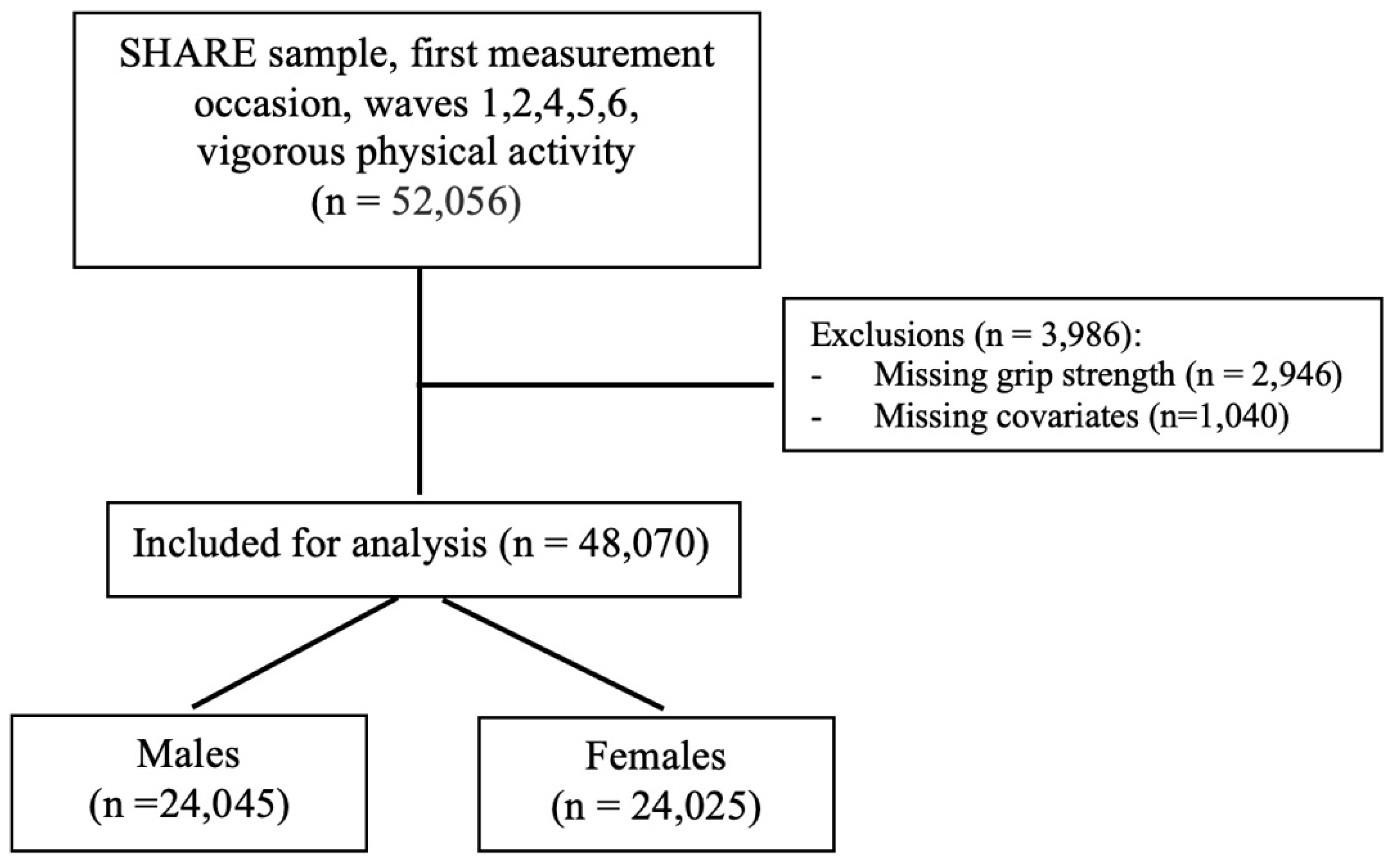
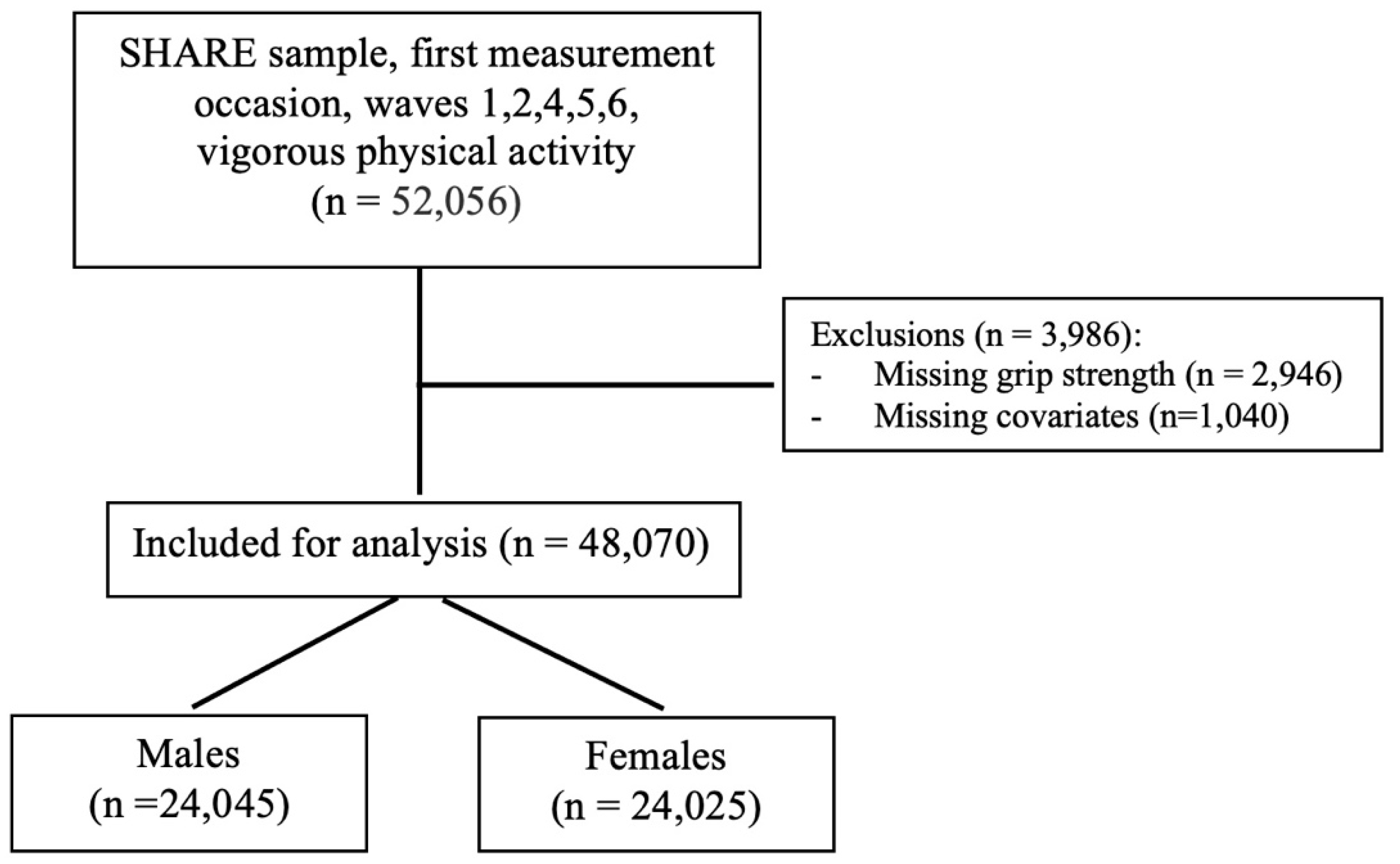
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
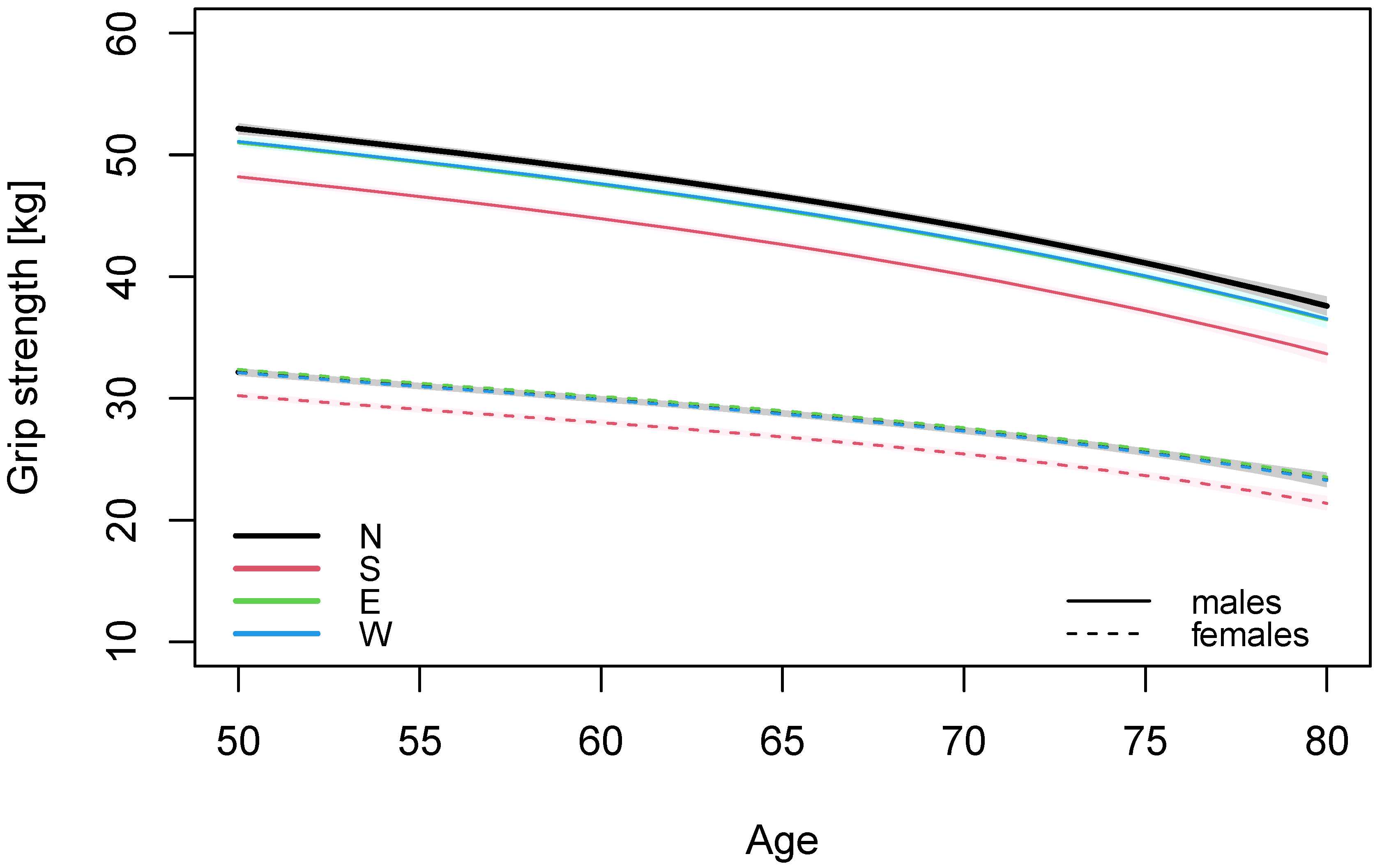
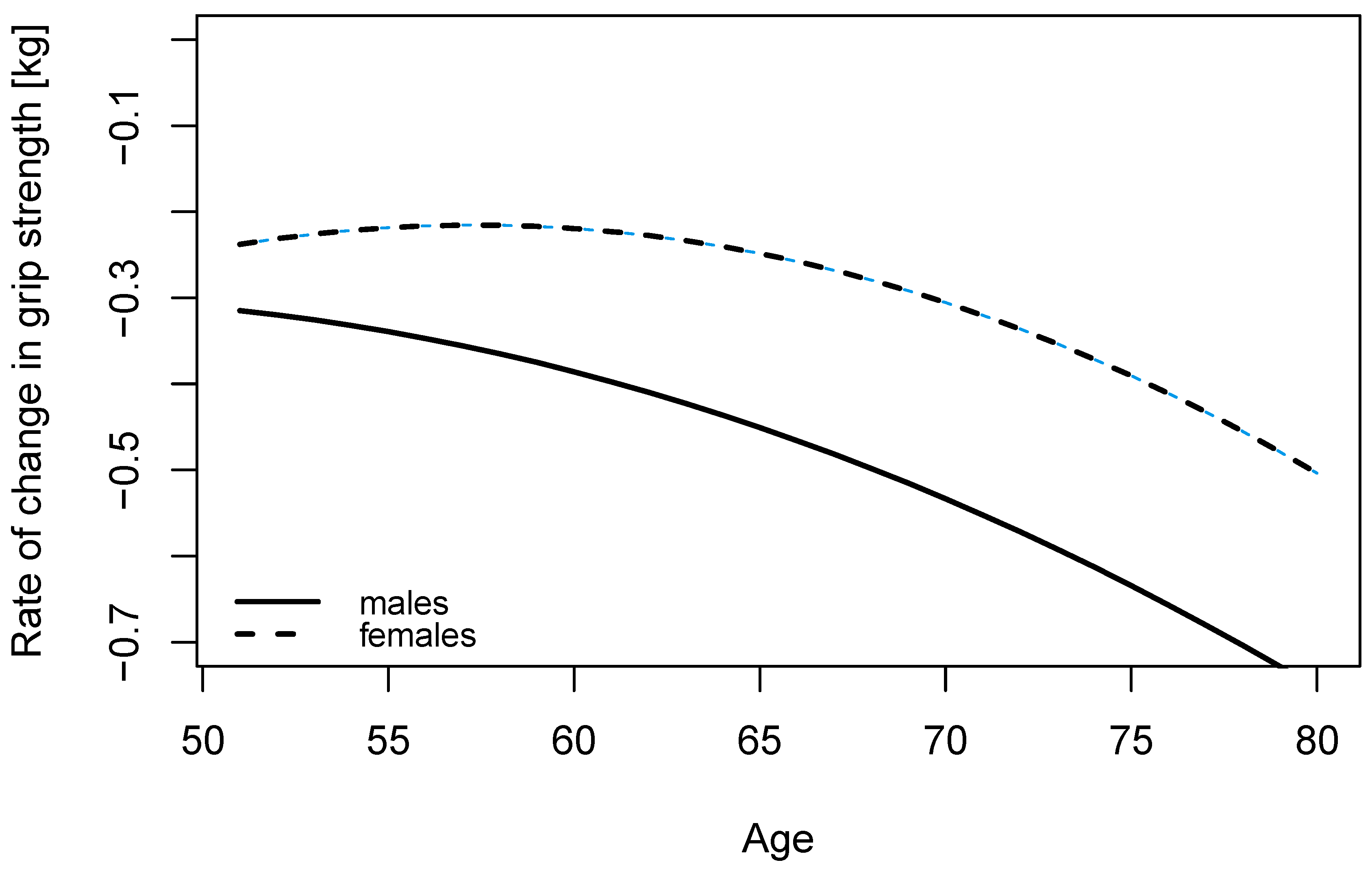
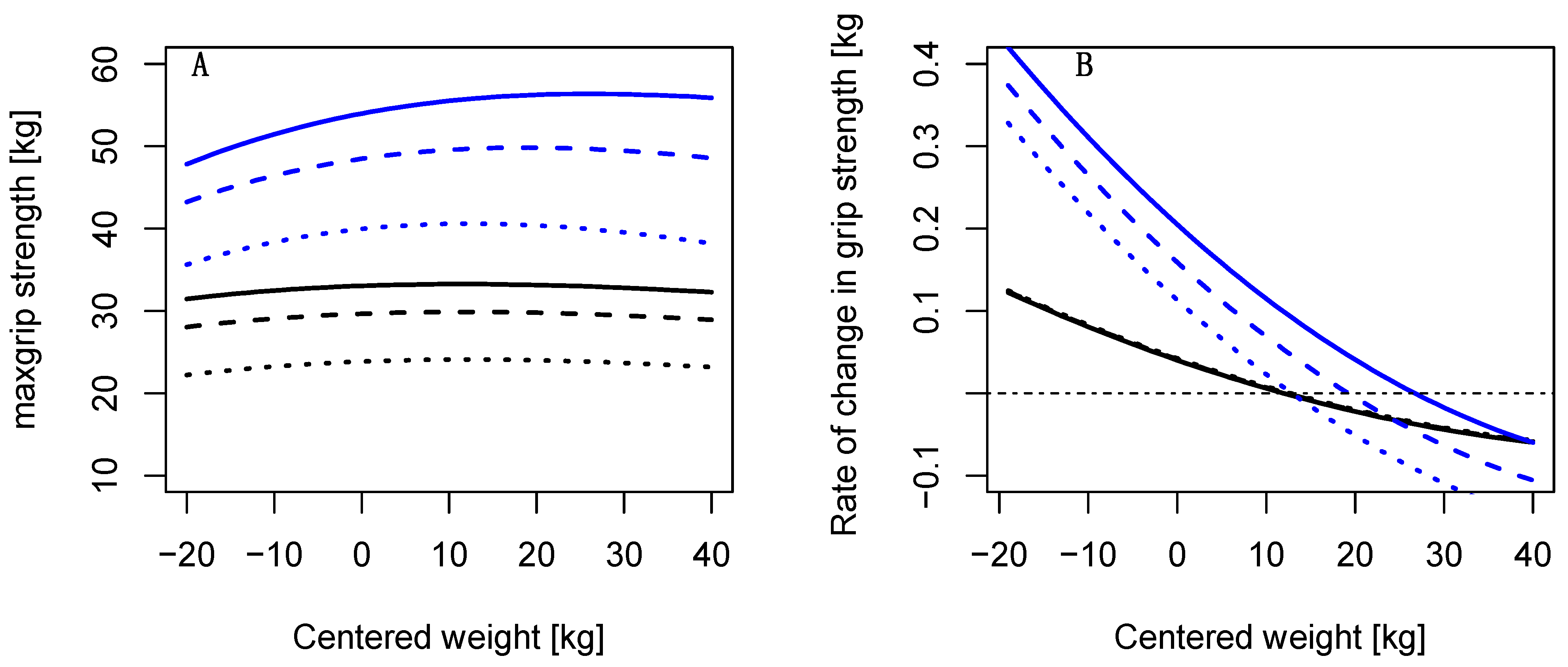
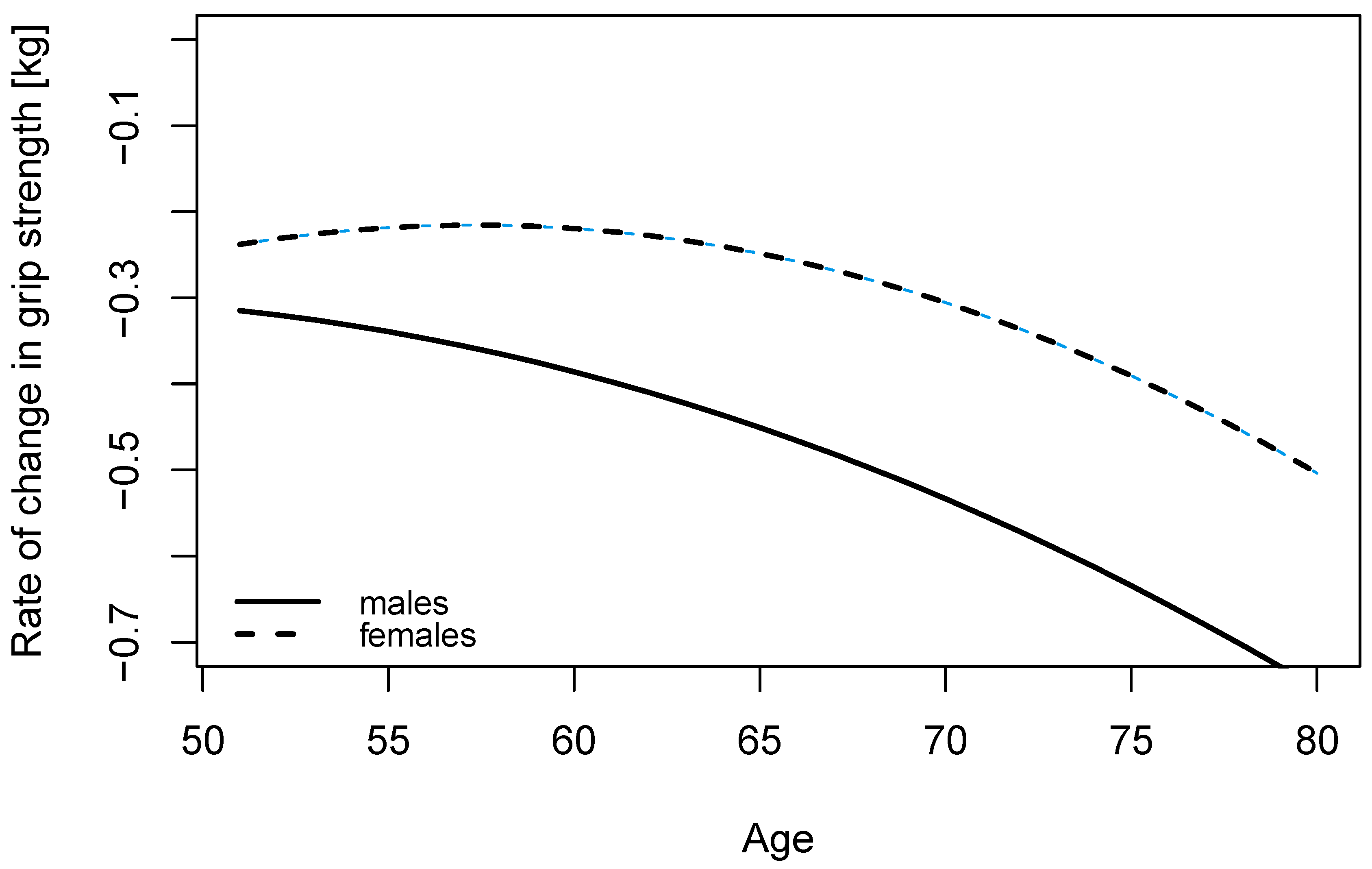
3. Results
4. Discussion
4.1. Sex Differences in the Age-Associated Decline in Grip Strength
4.2. Nonlinearity in Decline of Grip Strength
4.3. Body Mass and Grip Strength at Different Ages
4.4. Regional Differences in Grip Strength
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Roubenoff, R.; Castaneda, C. Sarcopenia—Understanding the Dynamics of Aging Muscle. JAMA 2001, 286, 1230–1231. [Google Scholar] [CrossRef] [PubMed]
- Volpi, E.; Nazemi, R.; Fujita, S. Muscle Tissue Changes with Aging. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 405–410. [Google Scholar] [CrossRef]
- McGrath, R.P.; Kraemer, W.J.; Snih, S.A.; Peterson, M.D. Handgrip Strength and Health in Aging Adults. Sports Med. 2018, 48, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Duchowny, K.A.; Clarke, P.J.; Peterson, M.D. Muscle Weakness and Physical Disability in Older Americans: Longitudinal Findings from the U.S. Health and Retirement Study. J. Nutr. Health Aging 2018, 22, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, H.; Hjelmborg, J.; Mortensen, J.; McGue, M.; Vaupel, J.W.; Christensen, K. Age Trajectories of Grip Strength: Cross-Sectional and Longitudinal Data among 8,342 Danes Aged 46 to 102. Ann. Epidemiol. 2006, 16, 554–562. [Google Scholar] [CrossRef]
- Sayer, A.A.; Kirkwood, T.B.L. Grip Strength and Mortality: A Biomarker of Ageing? Lancet 2015, 386, 226–227. [Google Scholar] [CrossRef]
- Morley, J.E.; Baumgartner, R.N.; Roubenoff, R.; Mayer, J.; Nair, K.S. Sarcopenia. J. Lab. Clin. Med. 2001, 137, 231–243. [Google Scholar] [CrossRef]
- Dag, F.; Tas, S.; Cimen, O.B. Hand-Grip Strength Is Correlated with Aerobic Capacity in Healthy Sedentary Young Females. Montenegrin J. Sports Sci. Med. 2021, 10, 55–60. [Google Scholar] [CrossRef]
- Kuh, D.; Bassey, E.J.; Butterworth, S.; Hardy, R.; Wadsworth, M.E.J. Musculoskeletal Study Team Grip Strength, Postural Control, and Functional Leg Power in a Representative Cohort of British Men and Women: Associations with Physical Activity, Health Status, and Socioeconomic Conditions. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 224–231. [Google Scholar] [CrossRef]
- Cooper, A.; Lamb, M.; Sharp, S.J.; Simmons, R.K.; Griffin, S.J. Bidirectional Association between Physical Activity and Muscular Strength in Older Adults: Results from the UK Biobank Study. Int. J. Epidemiol. 2017, 46, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Cooper, R.; Stamatakis, E.; Hamer, M. Associations of Sitting and Physical Activity with Grip Strength and Balance in Mid-Life: 1970 British Cohort Study. Scand. J. Med. Sci. Sports 2020, 30, 2371–2381. [Google Scholar] [CrossRef] [PubMed]
- Cronin, J.; Lawton, T.; Harris, N.; Kilding, A.; McMaster, D.T. A Brief Review of Handgrip Strength and Sport Performance. J. Strength Cond. Res. 2017, 31, 3187–3217. [Google Scholar] [CrossRef]
- Andersen-Ranberg, K.; Petersen, I.; Frederiksen, H.; Mackenbach, J.P.; Christensen, K. Cross-National Differences in Grip Strength among 50+ Year-Old Europeans: Results from the SHARE Study. Eur. J. Ageing 2009, 6, 227–236. [Google Scholar] [CrossRef]
- Ahrenfeldt, L.J.; Scheel-Hincke, L.L.; Kjærgaard, S.; Möller, S.; Christensen, K.; Lindahl-Jacobsen, R. Gender Differences in Cognitive Function and Grip Strength: A Cross-National Comparison of Four European Regions. Eur. J. Public Health 2019, 29, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Günther, C.M.; Bürger, A.; Rickert, M.; Crispin, A.; Schulz, C.U. Grip Strength in Healthy Caucasian Adults: Reference Values. J. Hand Surg. Am. 2008, 33, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Samson, M.M.; Meeuwsen, I.B.; Crowe, A.; Dessens, J.A.; Duursma, S.A.; Verhaar, H.J. Relationships between Physical Performance Measures, Age, Height and Body Weight in Healthy Adults. Age Ageing 2000, 29, 235–242. [Google Scholar] [CrossRef]
- Bann, D.; Hire, D.; Manini, T.; Cooper, R.; Botoseneanu, A.; McDermott, M.M.; Pahor, M.; Glynn, N.W.; Fielding, R.; King, A.C.; et al. Light Intensity Physical Activity and Sedentary Behavior in Relation to Body Mass Index and Grip Strength in Older Adults: Cross-Sectional Findings from the Lifestyle Interventions and Independence for Elders (LIFE) Study. PLoS ONE 2015, 10, e0116058. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Kauhanen, H.; Komi, P.V.; Häkkinen, K. Standardization and Validation of the Body Weight Adjustment Regression Equations in Olympic Weightlifting. J. Strength Cond. Res. 2002, 16, 58–74. [Google Scholar]
- Arandjelović, O. On Self-Propagating Methodological Flaws in Performance Normalization for Strength and Power Sports. Sports Med. 2013, 43, 451–461. [Google Scholar] [CrossRef]
- Perperoglou, A.; Huebner, M. Quantile Foliation for Modeling Performance across Body Mass and Life Span in Olympic Weightlifting. Stat. Model. 2021, 21, 546–563. [Google Scholar] [CrossRef]
- Cooper, R.; Mishra, G.; Clennell, S.; Guralnik, J.; Kuh, D. Menopausal Status and Physical Performance in Midlife: Findings from a British Birth Cohort Study. Menopause 2008, 15, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Huebner, M.; Meltzer, D.E.; Perperoglou, A. Age-Associated Performance Decline and Sex Differences in Olympic Weightlifting. Med. Sci. Sports Exerc. 2019, 51, 2302–2308. [Google Scholar] [CrossRef] [PubMed]
- Gava, P.; Ravara, B. Master World Records Show Minor Gender Differences of Performance Decline with Aging. Eur. J. Transl. Myol. 2019, 29, 8327. [Google Scholar] [CrossRef]
- Anton, M.M.; Spirduso, W.W.; Tanaka, H. Age-Related Declines in Anaerobic Muscular Performance: Weightlifting and Powerlifting. Med. Sci. Sports Exerc. 2004, 36, 143–147. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S.; on behalf of the SHARE Central Coordination Team. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Lusa, L.; Huebner, M. Organizing and Analyzing Data from the SHARE Study with an Application to Age and Sex Differences in Depressive Symptoms. Int. J. Environ. Res. Public Health 2021, 18, 9684. [Google Scholar] [CrossRef]
- Lusa, L.; Huebner, M. Repository with R Vignettes to Support Data Organization and Analysis for the Share Study; OSF, 2021. [Google Scholar] [CrossRef]
- Harrell, F.E. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis, 2nd ed.; Springer: Cham, Switzerland, 2015; ISBN 978-3-319-19424-0. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Horstman, A.M.; Dillon, E.L.; Urban, R.J.; Sheffield-Moore, M. The Role of Androgens and Estrogens on Healthy Aging and Longevity. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1140–1152. [Google Scholar] [CrossRef]
- Maltais, M.L.; Desroches, J.; Dionne, I.J. Changes in Muscle Mass and Strength after Menopause. J. Musculoskelet. Neuronal. Interact. 2009, 9, 186–197. [Google Scholar]
- Kurina, L.M.; Gulati, M.; Everson-Rose, S.A.; Chung, P.J.; Karavolos, K.; Cohen, N.J.; Kandula, N.; Lukezic, R.; Dugan, S.A.; Sowers, M.; et al. The Effect of Menopause on Grip and Pinch Strength: Results from the Chicago, Illinois, Site of the Study of Women’s Health Across the Nation. Am. J. Epidemiol. 2004, 160, 484–491. [Google Scholar] [CrossRef]
- García-Alfaro, P.; García, S.; Rodríguez, I.; Pérez-López, F.R. Handgrip Strength, Dynapenia, and Related Factors in Postmenopausal Women. Menopause 2022, 29, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Huebner, M.; Meltzer, D.; Ma, W.; Arrow, H. The Masters Athlete in Olympic Weightlifting: Training, Lifestyle, Health Challenges, and Gender Differences. PLoS ONE 2020, 15, e0243652. [Google Scholar] [CrossRef] [PubMed]
- Solberg, P.A.; Hopkins, W.G.; Paulsen, G.; Haugen, T.A. Peak Age and Performance Progression in World-Class Weightlifting and Powerlifting Athletes. Int. J. Sports Physiol. Perform. 2019, 14, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Huebner, M.; Meltzer, D.E.; Perperoglou, A. Strength in Numbers Women in Olympic-Style Weightlifting. Significance 2021, 18, 20–25. [Google Scholar] [CrossRef]
- Cheval, B.; Boisgontier, M.P.; Orsholits, D.; Sieber, S.; Guessous, I.; Gabriel, R.; Stringhini, S.; Blane, D.; van der Linden, B.W.A.; Kliegel, M.; et al. Association of Early- and Adult-Life Socioeconomic Circumstances with Muscle Strength in Older Age. Age Ageing 2018, 47, 398–407. [Google Scholar] [CrossRef]
- Bertoni, M.; Maggi, S.; Weber, G. Work, Retirement, and Muscle Strength Loss in Old Age. Health Econ. 2018, 27, 115–128. [Google Scholar] [CrossRef]
- Altman, D.G.; Royston, P. The Cost of Dichotomising Continuous Variables. BMJ 2006, 332, 1080. [Google Scholar] [CrossRef]
- Lim, S.H.; Kim, Y.H.; Lee, J.S. Normative Data on Grip Strength in a Population-Based Study with Adjusting Confounding Factors: Sixth Korea National Health and Nutrition Examination Survey (2014–2015). Int. J. Environ. Res. Public Health 2019, 16, E2235. [Google Scholar] [CrossRef]
- Keevil, V.L.; Luben, R.; Dalzell, N.; Hayat, S.; Sayer, A.A.; Wareham, N.J.; Khaw, K.-T. Cross-Sectional Associations between Different Measures of Obesity and Muscle Strength in Men and Women in a British Cohort Study. J. Nutr. Health Aging 2015, 19, 3–11. [Google Scholar] [CrossRef]
- Jeune, B.; Skytthe, A.; Cournil, A.; Greco, V.; Gampe, J.; Berardelli, M.; Andersen-Ranberg, K.; Passarino, G.; Debenedictis, G.; Robine, J.-M. Handgrip Strength among Nonagenarians and Centenarians in Three European Regions. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 707–712. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Trappenburg, M.C.; Hogrel, J.-Y.; McPhee, J.S.; Piasecki, M.; Sipila, S.; Salpakoski, A.; Butler-Browne, G.; Pääsuke, M.; et al. Handgrip Strength Cannot Be Assumed a Proxy for Overall Muscle Strength. J. Am. Med. Dir. Assoc. 2018, 19, 703–709. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Males n = 24,045 | Females n = 24,025 | |
|---|---|---|
| Age [years] | 60 (54, 67) | 59 (54, 66) |
| Age group | ||
| 50–59 | 48% (11,539) | 52% (12,433) |
| 60–69 | 35% (8452) | 33% (7991) |
| 70–80 | 17% (4054) | 15% (3601) |
| Body mass [kg] | 82 (75, 90) | 68 (60, 77) |
| Height [cm] | 176 (171, 180) | 164 (160, 168) |
| Education, high | 25% (6100) | 23% (5626) |
| Current smoker, yes | 24% (5748) | 19% (4450) |
| Region | ||
| West | 44% (10,554) | 44% (10,504) |
| North | 14% (3252) | 13% (3109) |
| South | 18% (4261) | 18% (4240) |
| East | 25% (5978) | 26% (6172) |
| Males | Females | |||||
|---|---|---|---|---|---|---|
| Variable | Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value |
| Intercept | 51.315 | (50.97, 51.66) | <0.001 | 31.717 | (31.48, 31.96) | <0.001 |
| Age [10 years] | −3.126 | (−4.16, −2.09) | <0.001 | −2.416 | (−3.15, −1.68) | <0.001 |
| Age 2 | −0.214 | (−1.13, 0.7) | 0.646 | 0.383 | (−0.28, 1.05) | 0.258 |
| Age 3 | −0.120 | (−0.34, 0.1) | 0.288 | −0.187 | (−0.35, −0.02) | 0.026 |
| Weight [10 kg] | −0.187 | (−0.35, −0.02) | <0.001 | 0.540 | (0.43, 0.65) | <0.001 |
| Weight 2 | 1.784 | (1.62, 1.94) | <0.001 | −0.132 | (−0.17, −0.09) | <0.001 |
| Weight 3 | −0.303 | (−0.36, −0.25) | <0.001 | 0.008 | (0.002, 0.012) | 0.002 |
| Height [10 cm] | 0.017 | (0.01, 0.02) | 0.002 | 2.290 | (2.16, 2.42) | <0.001 |
| Education, high | −0.221 | (−0.46, 0.02) | 0.066 | 0.393 | (0.21, 0.57) | <0.001 |
| Smoking, yes | −0.174 | (−0.42, 0.07) | 0.157 | 0.172 | (−0.02, 0.36) | 0.078 |
| Region, South | −2.880 | (−3.17, −2.59) | <0.001 | −1.882 | (−2.09, −1.67) | <0.001 |
| Region, North | 1.057 | (0.75, 1.37) | <0.001 | 0.048 | (−0.19, 0.28) | 0.687 |
| Region, East | −0.098 | (−0.35, 0.16) | 0.451 | 0.272 | (0.09, 0.46) | 0.004 |
| Age × Weight | −0.029 | (−0.04, −0.02) | <0.001 | 0.000 | (−0.01, 0.01) | 0.903 |
| Age | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|
| North | South | East | West | North | South | East | West | |
| 50 | 52.2 (51.7, 52.6) | 48.2 (47.8, 48.6) | 51.0 (50.6, 51.4) | 51.1 (50.7, 51.5) | 32.2 (31.9, 32.5) | 30.2 (29.9, 30.5) | 32.4 (32.1, 32.7) | 32.1 (31.8, 32.4) |
| 55 | 50.5 (50.2, 50.9) | 46.6 (46.2, 46.9) | 49.4 (49, 49.7) | 49.5 (49.2, 49.7) | 31.0 (30.8, 31.3) | 29.1 (28.8, 29.3) | 31.2 (31, 31.5) | 31.0 (30.8, 31.2) |
| 60 | 48.7 (48.3, 49) | 44.8 (44.4, 45.1) | 47.5 (47.2, 47.8) | 47.6 (47.4, 47.9) | 29.9 (29.7, 30.2) | 28.0 (27.8, 28.3) | 30.2 (29.9, 30.4) | 29.9 (29.7, 30.1) |
| 65 | 46.6 (46.2, 46.9) | 42.6 (42.3, 43) | 45.4 (45.1, 45.7) | 45.5 (45.3, 45.8) | 28.8 (28.5, 29) | 26.8 (26.6, 27.1) | 29.0 (28.8, 29.2) | 28.7 (28.5, 28.9) |
| 70 | 44.1 (43.7, 44.4) | 40.1 (39.8, 40.5) | 42.9 (42.6, 43.3) | 43 (42.7, 43.3) | 27.4 (27.1, 27.6) | 25.4 (25.2, 25.7) | 27.6 (27.3, 27.8) | 27.3 (27.1, 27.5) |
| 75 | 41.1 (40.7, 41.5) | 37.2 (36.8, 37.6) | 40.0 (39.6, 40.3) | 40.1 (39.7, 40.4) | 25.6 (25.3, 25.9) | 23.7 (23.3, 24) | 25.8 (25.5, 26.1) | 25.5 (25.3, 25.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huebner, M.; Lawrence, F.; Lusa, L. Sex Differences in Age-Associated Rate of Decline in Grip Strength When Engaging in Vigorous Physical Activity. Int. J. Environ. Res. Public Health 2022, 19, 11009. https://doi.org/10.3390/ijerph191711009
Huebner M, Lawrence F, Lusa L. Sex Differences in Age-Associated Rate of Decline in Grip Strength When Engaging in Vigorous Physical Activity. International Journal of Environmental Research and Public Health. 2022; 19(17):11009. https://doi.org/10.3390/ijerph191711009
Chicago/Turabian StyleHuebner, Marianne, Frank Lawrence, and Lara Lusa. 2022. "Sex Differences in Age-Associated Rate of Decline in Grip Strength When Engaging in Vigorous Physical Activity" International Journal of Environmental Research and Public Health 19, no. 17: 11009. https://doi.org/10.3390/ijerph191711009
APA StyleHuebner, M., Lawrence, F., & Lusa, L. (2022). Sex Differences in Age-Associated Rate of Decline in Grip Strength When Engaging in Vigorous Physical Activity. International Journal of Environmental Research and Public Health, 19(17), 11009. https://doi.org/10.3390/ijerph191711009