
Assessment of the Correlation between the Levels of Physical Activity and Technology Usage among Children with Down Syndrome in the Riyadh Region

 , ,
, ,
Abstract
:1. Introduction
2. Methodology
2.1. Design
2.2. Participants
2.3. Data Collection
2.4. Measures Included in the Questionnaires
2.4.1. Demographic Variables
2.4.2. Children’s Physical Activity Questionnaire (CPAQ)
2.4.3. Research Questionnaire to Evaluate the Impact of Technology Usage on C-DS
2.5. Translation of the Questionnaires
2.6. Pilot Study
2.7. Data Analysis
3. Results
3.1. Description about Mothers of C-DS
3.2. Description of C-DS
3.3. Descriptive Information on the Child’s Technology Acquisition
3.4. Relationship between Technology Use and the Characteristics of the Mother
3.5. Technology-Usage Pattern by C-DS
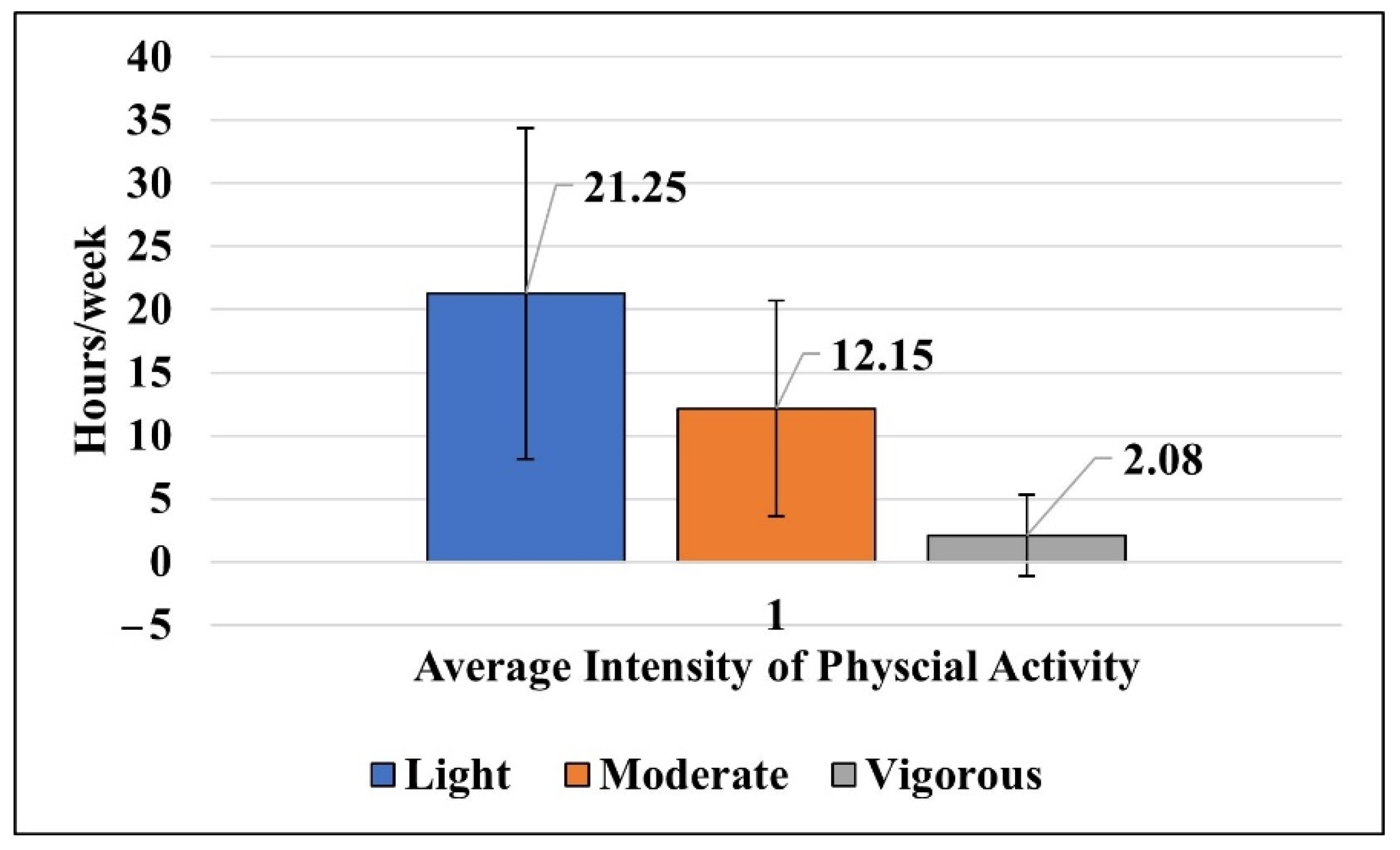
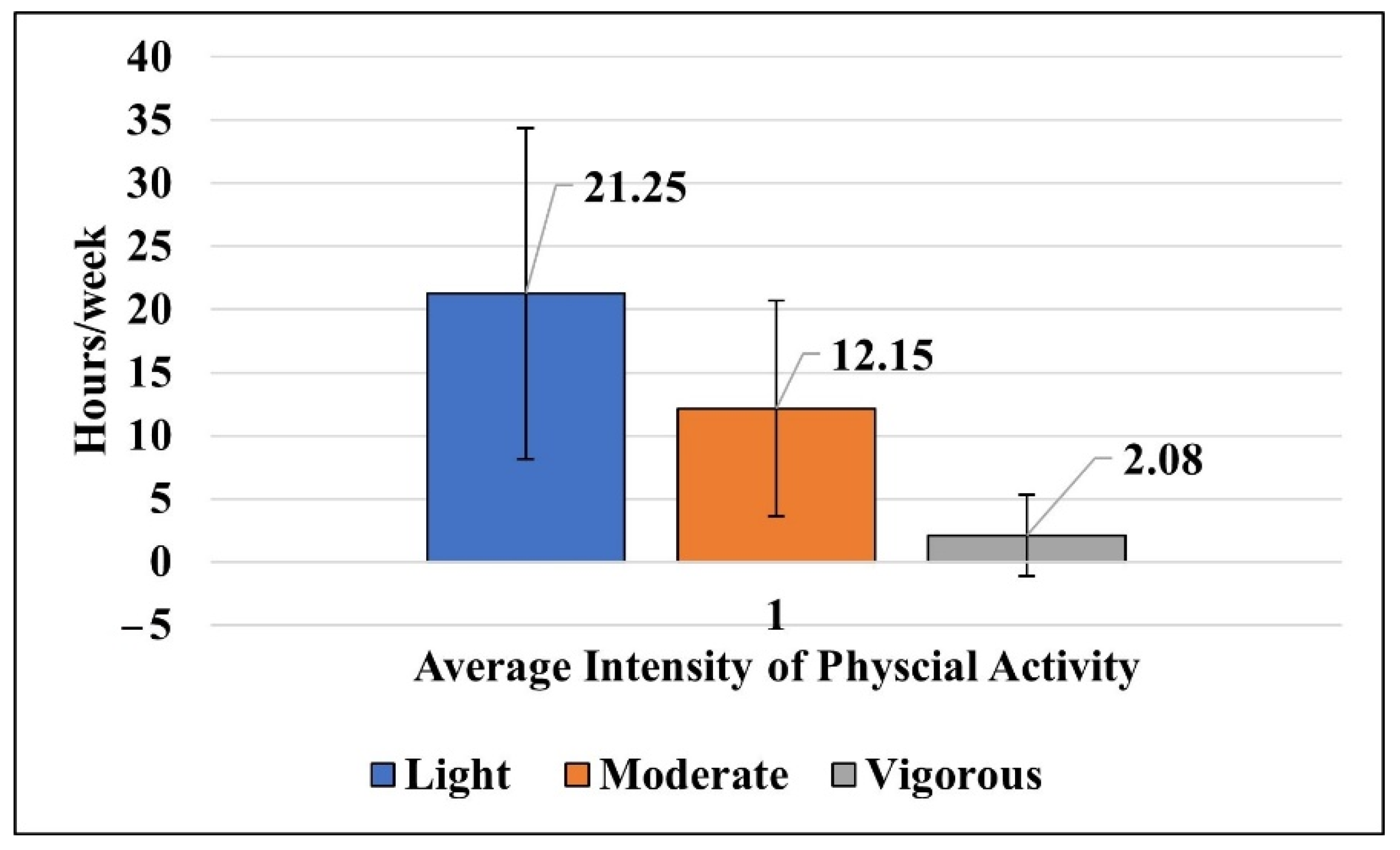
3.6. Evaluation of Physical Activity
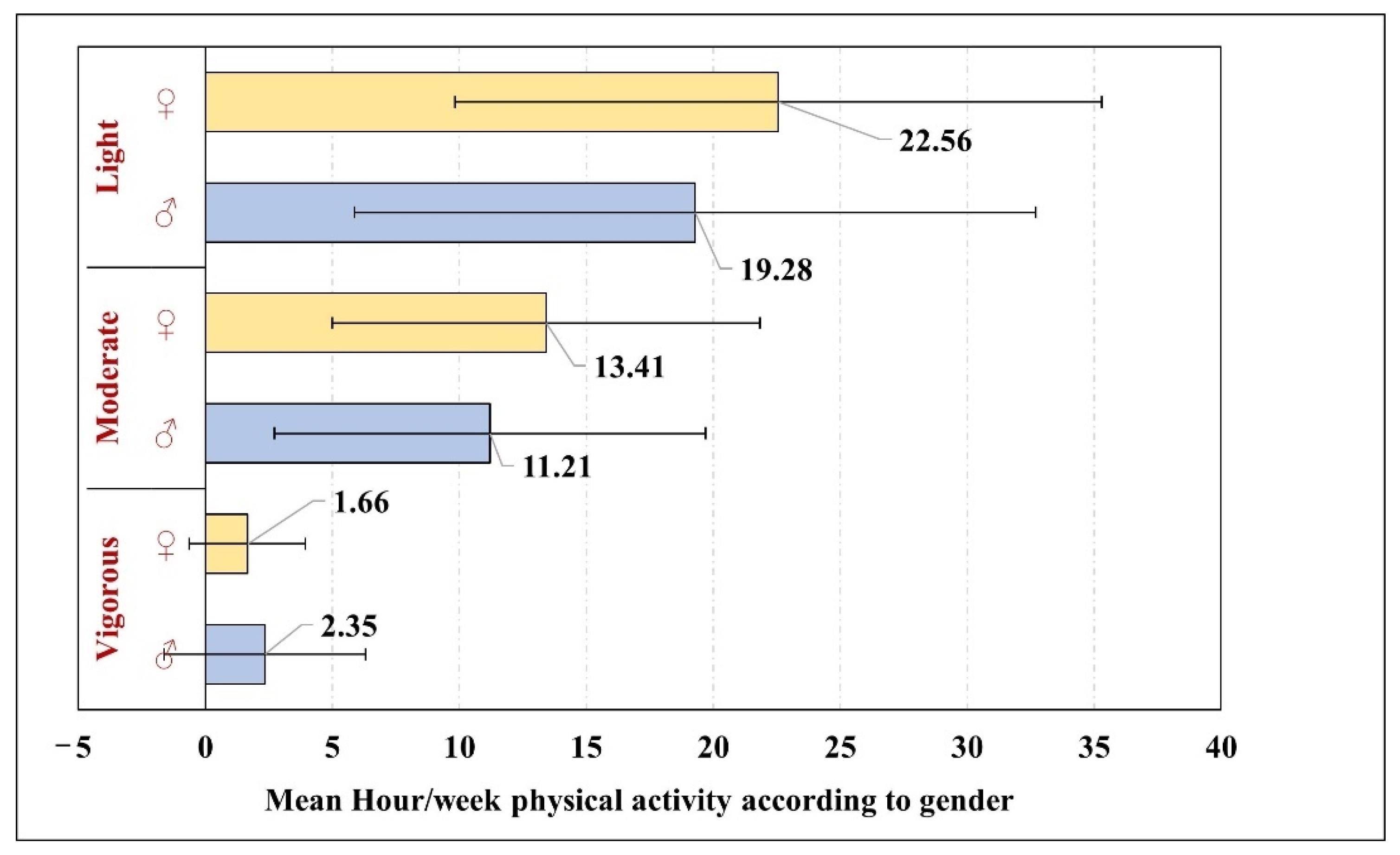
3.7. Relationship between Physical Activity and Gender of the Child with DS
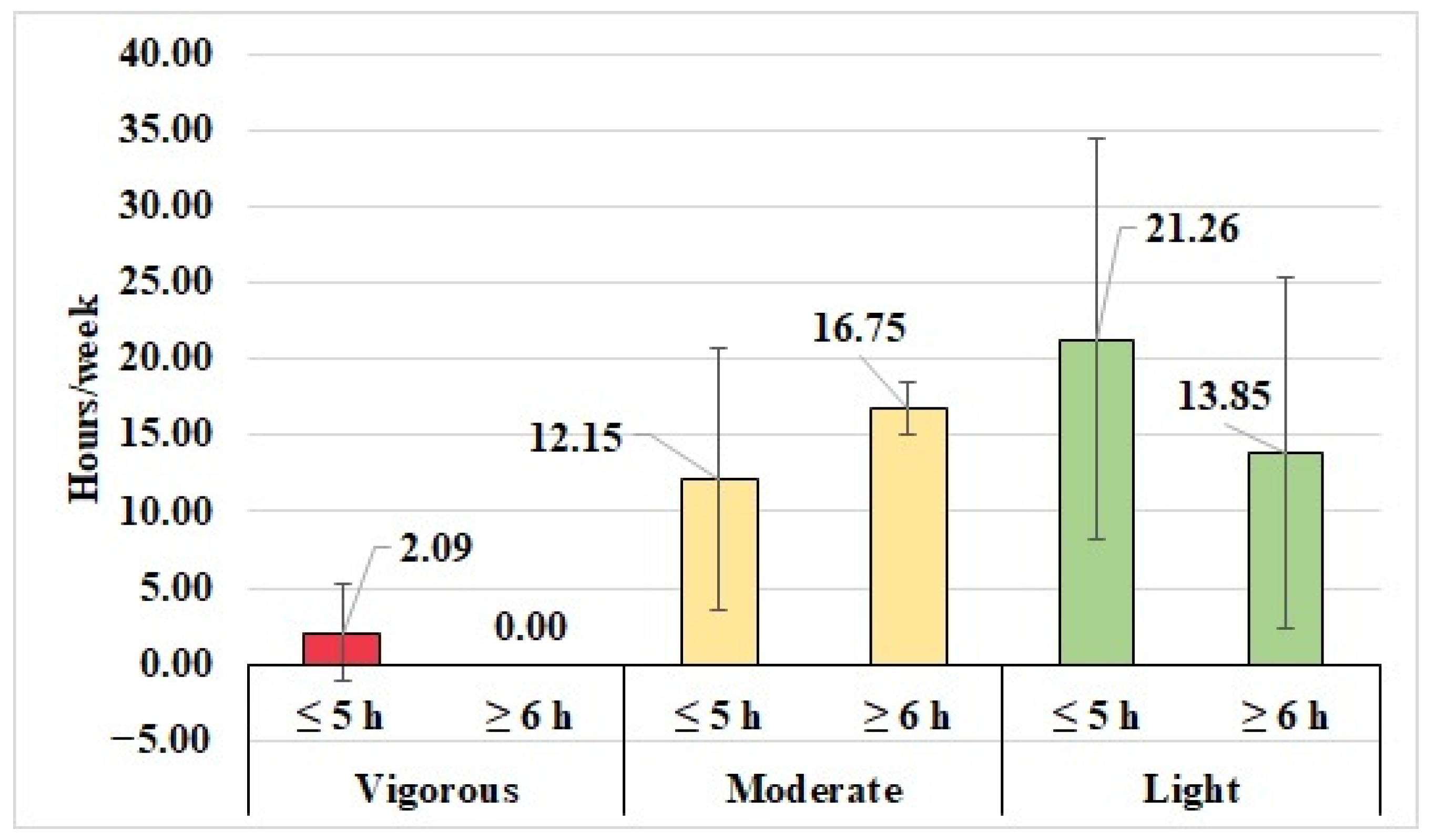
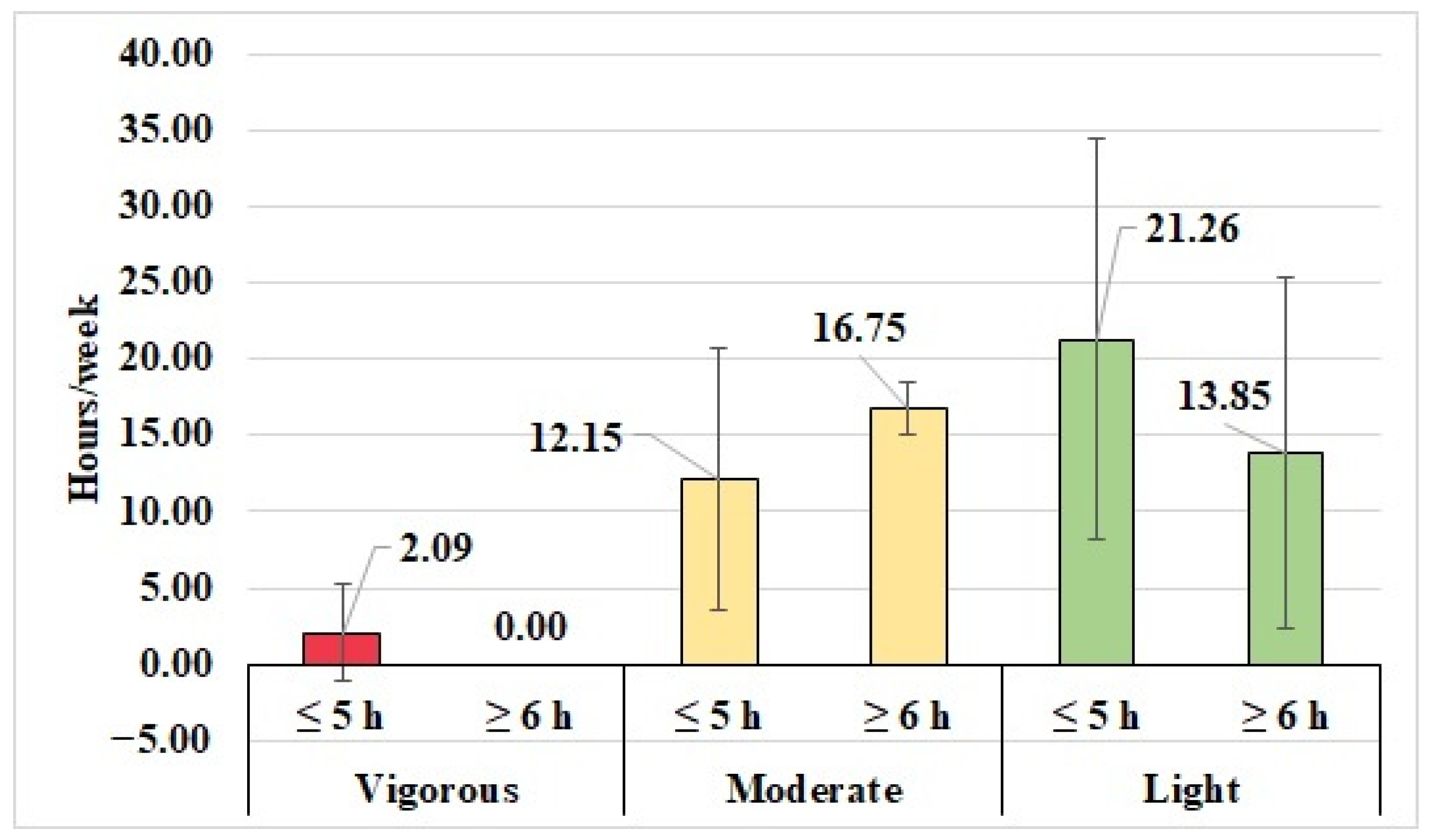
3.8. Relationship between Physical Activity and Technology Use
4. Discussion
5. Conclusions
6. Limitations
7. Recommendations
8. Prospects of This Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pitetti, K.; Baynard, T.; Agiovlasitis, S. Children and adolescents with Down syndrome, physical fitness and physical activity. J. Sport Health Sci. 2013, 2, 47–57. [Google Scholar] [CrossRef]
- CDC. Data and Statistics on Down Syndrome USA: Centers for Disease Control and Prevention. 2020. Available online: https://www.cdc.gov/ncbddd/birthdefects/downsyndrome/data.html#:~:text=Babies%3A,in%20every%20700%20babies%20born (accessed on 24 May 2022).
- DSA. 2021. Available online: https://www.downs-syndrome.org.uk/our-work/information-services/dsa-journal/ (accessed on 24 May 2022).
- AlSalloum, A.; El Mouzan, M.I.; AlHerbish, A.; AlOmer, A.; Qurashi, M. Prevalence of selected congenital anomalies in Saudi children: A community-based study. Ann. Saudi Med. 2015, 35, 107–110. [Google Scholar] [CrossRef]
- Alhusaini, A.A.; Ali Al-Walah, M.; Melam, G.R.; Buragadda, S. Pedometer-determined physical activity levels of healthy children and children with Down’s syndrome. Somatosens. Mot. Res. 2017, 34, 219–225. [Google Scholar] [CrossRef]
- Alghamdi, S.; Banakhar, M.; Badr, H.; Alsulami, S. Physical activity among children with down syndrome: Maternal perception. Int. J. Qual. Stud. Health Well-Being 2021, 16, 1932701. [Google Scholar] [CrossRef]
- Asim, A.; Kumar, A.; Muthuswamy, S.; Jain, S.; Agarwal, S. Down syndrome: An insight of the disease. J. Biomed. Sci. 2015, 22, 41. [Google Scholar] [CrossRef]
- Whitt-Glover, M.C.; O’Neill, K.L.; Stettler, N. Physical activity patterns in children with and without Down syndrome. Pediatr. Rehabil. 2006, 9, 158–164. [Google Scholar] [CrossRef]
- WHO. Physical Activity: World Health Organization. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 24 May 2022).
- Phillips, A.C.; Holland, A.J. Assessment of Objectively Measured Physical Activity Levels in Individuals with Intellectual Disabilities with and without Down’s Syndrome. PLoS ONE 2011, 6, e28618. [Google Scholar] [CrossRef]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef]
- Shields, N.; Synnot, A.J.; Barr, M. Perceived barriers and facilitators to physical activity for children with disability: A systematic review. Br. J. Sports Med. 2012, 46, 989–997. [Google Scholar] [CrossRef]
- Anaby, D.; Hand, C.; Bradley, L.; DiRezze, B.; Forhan, M.; DiGiacomo, A.; Law, M. The effect of the environment on participation of children and youth with disabilities: A scoping review. Disabil. Rehabil. 2013, 35, 1589–1598. [Google Scholar] [CrossRef]
- Farías-Valenzuela, C.; Cofré-Bolados, C.; Ferrari, G.; Espoz-Lazo, S.; Arenas-Sánchez, G.; Álvarez-Arangua, S.; Espinoza-Salinas, A.; Valdivia-Moral, P. Effects of Motor-Games-Based Concurrent Training Program on Body Composition Indicators of Chilean Adults with Down Syndrome. Sustainability 2021, 13, 5737. [Google Scholar] [CrossRef]
- MacMullin, J.A.; Lunsky, Y.; Weiss, J.A. Plugged in: Electronics use in youth and young adults with autism spectrum disorder. Autism Int. J. Res. Pract. 2016, 20, 45–54. [Google Scholar] [CrossRef]
- Fritz, M.N. The Impact of Technology on Individuals with Down Syndrome and Their Families. Rehabilitation, Human Resources and Communication Disorders Undergraduate Honors Theses. 2017. Available online: https://scholarworks.uark.edu/rhrcuht/49 (accessed on 27 May 2022).
- Lin, L.Y.; Cherng, R.J.; Chen, Y.J.; Chen, Y.J.; Yang, H.M. Effects of television exposure on developmental skills among young children. Infant Behav. Dev. 2015, 38, 20–26. [Google Scholar] [CrossRef]
- Zamani, E.; Chashmi, M.; Hedayati, N. Effect of addiction to computer games on physical and mental health of female and male students of guidance school in city of isfahan. Addict. Health 2009, 1, 98–104. [Google Scholar]
- Girimaji, S.; Pradeep, A. Intellectual disability in international classification of Diseases-11: A developmental perspective. Indian J. Soc. Psychiatry 2018, 34, 68–74. [Google Scholar] [CrossRef]
- Corder, K.; van Sluijs, E.M.; Wright, A.; Whincup, P.; Wareham, N.J.; Ekelund, U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report? Am. J. Clin. Nutr. 2009, 89, 862–870. [Google Scholar] [CrossRef]
- Bacelis-Rivero, A.P.; Vázquez-Rodríguez, A.; Carrasco-Legleu, C.E.; De León, L.G.; Reza-López, S.A. Assessment of Physical Activity in Adults: A Review of Validated Questionnaires from a Nutritionist’s Point of View. Eval. Health Prof. 2020, 43, 235–254. [Google Scholar] [CrossRef]
- Alotaibi, T.; Almuhanna, R.; Alhassan, J.; Alqadhib, E.; Mortada, E.; Alwhaibi, R. The Relationship between Technology Use and Physical Activity among Typically-Developing Children. Healthcare 2020, 8, 488. [Google Scholar] [CrossRef]
- Mesman, G.R.; Kuo, D.Z.; Carroll, J.L.; Ward, W.L. The Impact of Technology Dependence on Children and Their Families. J. Pediatr. Health Care 2013, 27, 451–459. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.; Terkawi, A. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, 80–89. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32 (Suppl. S9), S498–S504. [Google Scholar] [CrossRef] [Green Version]
- Christakis, D.A. The effects of infant media usage: What do we know and what should we learn? Acta Paediatr. 2009, 98, 8–16. [Google Scholar] [CrossRef]
- Mai, C.T.; Kucik, J.E.; Isenburg, J.; Feldkamp, M.L.; Marengo, L.K.; Bugenske, E.M.; Thorpe, P.G.; Jackson, J.M.; Correa, A.; Rickard, R.; et al. Selected birth defects data from population-based birth defects surveillance programs in the United States, 2006 to 2010: Featuring trisomy conditions. Birth Defects Res. Part A Clin. Mol. Teratol. 2013, 97, 709–725. [Google Scholar] [CrossRef]
- Kovaleva, N.V. Prenatal Diagnosis and Screening for Down Syndrome [Internet], 2011th ed.; Dey, S., Ed.; IntechOpen: London, UK, 2011; Available online: https://www.intechopen.com/chapters/17999 (accessed on 30 May 2022).
- Karmiloff-Smith, A.; Al-Janabi, T.; D’Souza, H.; Groet, J.; Massand, E.; Mok, K.; Startin, C.; Fisher, E.; Hardy, J.; Nizetic, D.; et al. The importance of understanding individual differences in Down syndrome. F1000Research 2016, 5, F1000 Faculty Rev-389. [Google Scholar] [CrossRef]
- Yaron, Y.; Wolman, I.; Kupferminc, M.J.; Ochshorn, Y.; Many, A.; Orr-Urtreger, A. Effect of fetal gender on first trimester markers and on Down syndrome screening. Prenat. Diagn. 2001, 21, 1027–1030. [Google Scholar] [CrossRef]
- Connell, S.L.; Lauricella, A.R.; Wartella, E. Parental Co-Use of Media Technology with their Young Children in the USA. J. Child. Media 2015, 9, 5–21. [Google Scholar] [CrossRef]
- Dumuid, D.; Olds, T.; Lewis, L.K.; Martín-Fernández, J.A.; Katzmarzyk, P.; Barreira, T.; Broyles, S.T.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; et al. Health-Related Quality of Life and Lifestyle Behavior Clusters in School-Aged Children from 12 Countries. J. Pediatr. 2017, 183, 178–183.e2. [Google Scholar] [CrossRef]
- Brindova, D.; Pavelka, J.; Ševčikova, A.; Žežula, I.; van Dijk, J.P.; Reijneveld, S.A.; Geckova, A.M. How parents can affect excessive spending of time on screen-based activities. BMC Public Health 2014, 14, 1261. [Google Scholar] [CrossRef]
- Carson, V.; Kuzik, N. Demographic correlates of screen time and objectively measured sedentary time and physical activity among toddlers: A cross-sectional study. BMC Public Health 2017, 17, 187. [Google Scholar] [CrossRef]
- Karani, N.F.; Sher, J.; Mophosho, M. The influence of screen time on children’s language development: A scoping review. S. Afr. J. Commun. Disord. 2022, 69, e1–e7. [Google Scholar] [CrossRef]
- Okuma, K.; Tanimura, M. A preliminary study on the relationship between characteristics of TV content and delayed speech development in young children. Infant Behav. Dev. 2009, 32, 312–321. [Google Scholar] [CrossRef]
- Brown, A. Media use by children younger than 2 years. Pediatrics 2011, 128, 1040–1045. [Google Scholar] [CrossRef]
- Lapierre, M.A.; Piotrowski, J.T.; Linebarger, D.L. Background Television in the Homes of US Children. Pediatrics 2012, 130, 839–846. [Google Scholar] [CrossRef]
- Li, C.; Cheng, G.; Sha, T.; Cheng, W.; Yan, Y. The Relationships between Screen Use and Health Indicators among Infants, Toddlers, and Preschoolers: A Meta-Analysis and Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7324. [Google Scholar] [CrossRef]
- Tsao, R.; Kindelberger, C. Variability of cognitive development in children with Down syndrome: Relevance of good reasons for using the cluster procedure. Res. Dev. Disabil. 2009, 30, 426–432. [Google Scholar] [CrossRef]
- Bull, M.J.; Committee on Genetics. Health Supervision for Children with Down Syndrome. Pediatrics 2011, 128, 393–406. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Shattuck, P.T.; Wagner, M.; Cooper, B.P. Prevalence and correlates of screen-based media use among youths with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 1757–1767. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Wenstrup, C. Television, Video Game and Social Media Use Among Children with ASD and Typically Developing Siblings. J. Autism Dev. Disord. 2013, 43, 1258–1271. [Google Scholar] [CrossRef]
- Sharav, T.; Bowman, T. Dietary practices, physical activity, and body-mass index in a selected population of Down syndrome children and their siblings. Clin. Pediatr. 1992, 31, 341–344. [Google Scholar] [CrossRef]
- Luke, A.; Sutton, M.; Schoeller, D.A.; Roizen, N.J. Nutrient intake and obesity in prepubescent children with Down syndrome. J. Am. Diet. Assoc. 1996, 96, 1262–1267. [Google Scholar] [CrossRef]
- Mendonca, G.V.; Pereira, F.D.; Fernhall, B. Reduced exercise capacity in persons with Down syndrome: Cause, effect, and management. Ther. Clin. Risk Manag. 2010, 6, 601–610. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics. Committee on Genetics. American Academy of Pediatrics: Health supervision for children with Down syndrome. Pediatrics 2001, 107, 442–449. [Google Scholar] [CrossRef]
- Cohen, W.I. Health Care Guidelines for Individuals with Down Syndrome—1999 Revision. In Down Syndrome: Visions for the 21st Century; Cohen, W.I., Nadel, L., Madnick, M.E., Eds.; Wiley-Liss: New York, NY, USA, 2002; pp. 237–245. [Google Scholar] [CrossRef]
- Shields, N.; Hussey, J.; Murphy, J.; Gormley, J.; Hoey, H. An exploratory study of the association between physical activity, cardiovascular fitness and body size in children with Down syndrome. Dev. Neurorehabilit. 2017, 20, 92–98. [Google Scholar] [CrossRef]
- Watts, R.; Vyas, H. An overview of respiratory problems in children with Down’s syndrome. Arch. Dis. Child. 2013, 98, 812–817. [Google Scholar] [CrossRef]
- Mirsaeidi, M.; Motahari, H.; Taghizadeh Khamesi, M.; Sharifi, A.; Campos, M.; Schraufnagel, D.E. Climate Change and Respiratory Infections. Ann. Am. Thorac. Soc. 2016, 13, 1223–1230. [Google Scholar] [CrossRef]
- González-Agüero, A.; Vicente-Rodríguez, G.; Moreno, L.A.; Guerra-Balic, M.; Ara, I.; Casajús, J.A. Health-related physical fitness in children and adolescents with Down syndrome and response to training. Scand. J. Med. Sci. Sports 2010, 20, 716–724. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mother’s Age (Years) | Frequency | Percent (%) |
| 25–30 | 1 | 2.0 |
| 31–35 | 4 | 8.2 |
| 36–40 | 8 | 16.3 |
| 41–45 | 14 | 28.6 |
| above 45 | 22 | 44.9 |
| Marital status | Frequency | Percent |
| Married | 45 | 91.8 |
| Widow | 1 | 2.0 |
| Divorce | 1 | 2.0 |
| Separated | 2 | 4.1 |
| Education level | Frequency | Percent |
| Not educated | 1 | 2.0 |
| Under high school | 3 | 6.1 |
| High school diploma | 13 | 26.5 |
| Bachelor’s degree | 26 | 53.1 |
| Postgraduate | 6 | 12.2 |
| Number of children in the family | Frequency | Percent |
| 1 | 3 | 6.1 |
| 2 | 1 | 2.0 |
| 3 | 11 | 22.4 |
| 4 | 8 | 16.3 |
| 5 | 7 | 14.3 |
| 6 | 10 | 20.4 |
| 7 | 6 | 12.2 |
| 8 | 1 | 2.0 |
| 9 | 2 | 4.1 |
| Family monthly income | Frequency | Percent |
| less than 5000 | 6 | 12.2 |
| 5000–10,000 | 19 | 38.8 |
| 10,000–15,000 | 6 | 12.2 |
| 15,000–20,000 | 6 | 12.2 |
| more than 20,000 | 12 | 24.5 |
| Gender | Frequency | Percent |
| Male | 24 | 49.0 |
| Female | 25 | 51.0 |
| Age | Frequency | Percent |
| 6 | 15 | 30.6 |
| 7 | 2 | 4.1 |
| 8 | 7 | 14.3 |
| 9 | 8 | 16.3 |
| 10 | 6 | 12.2 |
| 11 | 5 | 10.2 |
| 12 | 6 | 12.2 |
| Mean Age= 8.55 | Standard Deviation= 2.14 | |
| IQ * Level | Frequency | Percent |
| IQ 50 or more | 39 | 79.6 |
| IQ between 49–35 | 10 | 20.4 |
| Does the Child Have an Electronic Device? | Frequency | Percent |
| Yes | 33 | 67.3 |
| No | 16 | 32.7 |
| Age of the child when he had his first device (years) | Frequency | Percent |
| 2 | 2 | 6.3 |
| 3 | 1 | 3.1 |
| 4 | 9 | 28.1 |
| 5 | 4 | 12.5 |
| 6 | 3 | 9.4 |
| 7 | 2 | 6.3 |
| 8 | 5 | 15.6 |
| 9 | 2 | 6.3 |
| 10 | 3 | 9.4 |
| 12 | 1 | 3.1 |
| Mean age for owning first device = 6.09 ± 2.57 | ||
| Number of devices | Frequency | Percent |
| 1 | 31 | 93.9 |
| 3 | 2 | 6.1 |
| Technology | Hours/Week | Frequency | Percent |
|---|---|---|---|
| TV | 1–10 | 40 | 81.6 |
| 10–20 | 9 | 18.4 | |
| Portable games console | 0 | 10 | 20.4 |
| 1–5 | 23 | 46.9 | |
| 5–10 | 9 | 18.4 | |
| >10 | 7 | 14.3 | |
| Social networking sites | 0 | 43 | 87.8 |
| 1–5 | 4 | 8.2 | |
| 5–10 | 1 | 2.0 | |
| >10 | 1 | 2.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alwhaibi, R.M.; Omer, A.B.; Khan, R.; Albashir, F.; Alkuait, N.; Alhazmi, R. Assessment of the Correlation between the Levels of Physical Activity and Technology Usage among Children with Down Syndrome in the Riyadh Region. Int. J. Environ. Res. Public Health 2022, 19, 10958. https://doi.org/10.3390/ijerph191710958
Alwhaibi RM, Omer AB, Khan R, Albashir F, Alkuait N, Alhazmi R. Assessment of the Correlation between the Levels of Physical Activity and Technology Usage among Children with Down Syndrome in the Riyadh Region. International Journal of Environmental Research and Public Health. 2022; 19(17):10958. https://doi.org/10.3390/ijerph191710958
Chicago/Turabian StyleAlwhaibi, Reem. M., Asma B. Omer, Ruqaiyah Khan, Felwa Albashir, Noura Alkuait, and Rawan Alhazmi. 2022. "Assessment of the Correlation between the Levels of Physical Activity and Technology Usage among Children with Down Syndrome in the Riyadh Region" International Journal of Environmental Research and Public Health 19, no. 17: 10958. https://doi.org/10.3390/ijerph191710958
APA StyleAlwhaibi, R. M., Omer, A. B., Khan, R., Albashir, F., Alkuait, N., & Alhazmi, R. (2022). Assessment of the Correlation between the Levels of Physical Activity and Technology Usage among Children with Down Syndrome in the Riyadh Region. International Journal of Environmental Research and Public Health, 19(17), 10958. https://doi.org/10.3390/ijerph191710958