
LGBTQ+ Affirming Care May Increase Awareness and Understanding of Undetectable = Untransmittable among Midlife and Older Gay and Bisexual Men in the US South

 , and
, and
Abstract
:1. Introduction
2. Data and Methods
2.1. U = U Measures
2.2. Affirming Care Measures
2.3. Covariates
2.4. Analytic Strategy
3. Results
3.1. LGBTQ Affirming Care
3.2. Awareness of U = U
3.3. Believability of U = U
3.4. Understanding of U = U
3.5. Impact of U = U on Risk Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| US Census Household Pulse Survey, Weeks 34–39 | |||||
|---|---|---|---|---|---|
| VUSNAPS Wave 1 | South | Difference | Sample States Only | National | |
| Gender | |||||
| Male | 0.5470 | 0.5394 | −0.0076 | 0.5014 | 0.5459 |
| Female | 0.3798 | 0.3915 | 0.0117 | 0.3895 | 0.3862 |
| Transgender | 0.0629 | 0.0575 | −0.0054 | 0.0897 | 0.0580 |
| None of these | 0.0104 | 0.0116 | 0.0012 | 0.0193 | 0.0099 |
| Sexual Orientation | |||||
| Gay or lesbian | 0.8591 | 0.6232 | −0.2359 | 0.5581 | 0.6202 |
| Straight | 0.0080 | 0.0643 | 0.0563 | 0.0864 | 0.0588 |
| Bisexual | 0.1091 | 0.2584 | 0.1493 | 0.2731 | 0.2829 |
| Something else | 0.2070 | 0.0198 | −0.1872 | 0.0494 | 0.0180 |
| I don’t know | 0.0032 | 0.0334 | 0.0302 | 0.0329 | 0.0189 |
| Age | |||||
| 50–54 | 0.2158 | 0.2433 | 0.0275 | 0.1921 | 0.2176 |
| 55–59 | 0.3392 | 0.2777 | −0.0615 | 0.3094 | 0.2986 |
| 60–64 | 0.2205 | 0.1956 | −0.0249 | 0.2013 | 0.2000 |
| 65–69 | 0.1481 | 0.1803 | 0.0322 | 0.1794 | 0.1652 |
| 70–74 | 0.0709 | 0.0774 | 0.0065 | 0.0805 | 0.0938 |
| 75–76 | 0.0056 | 0.0258 | 0.0202 | 0.0373 | 0.0249 |
| Race | |||||
| White only | 0.8615 | 0.6636 | −0.1979 | 0.6139 | 0.6689 |
| African American/Black only | 0.0796 | 0.1143 | 0.0347 | 0.1691 | 0.0914 |
| Latino/Hispanic | 0.0104 | 0.1694 | 0.1590 | 0.1406 | 0.1578 |
| Asian only | 0.0040 | 0.0143 | 0.0103 | 0.0147 | 0.0315 |
| Other/Multiracial | 0.0446 | 0.0384 | −0.0062 | 0.0318 | 0.0504 |
| Education | |||||
| High school or less | 0.0537 | 0.3873 | 0.3336 | 0.4505 | 0.3515 |
| Some college/AA | 0.2384 | 0.2931 | 0.0547 | 0.2629 | 0.2945 |
| College degree | 0.3157 | 0.1572 | −0.1585 | 0.1184 | 0.1640 |
| Graduate degree | 0.3922 | 0.1624 | −0.2298 | 0.1682 | 0.1899 |
| Marital Status | |||||
| Married | 0.4307 | 0.4112 | −0.0195 | 0.4000 | 0.4202 |
| Widowed | 0.0358 | 0.0623 | 0.0265 | 0.0652 | 0.0496 |
| Divorced | 0.1513 | 0.1829 | 0.0316 | 0.2095 | 0.1694 |
| Separated | 0.0183 | 0.0306 | 0.0123 | 0.0173 | 0.0313 |
| Never married | 0.3639 | 0.3131 | −0.0508 | 0.3080 | 0.3294 |
References
- National Institute of Allergy and Infectious Diseases HIV Undetectable=Untransmittable (U=U), or Treatment as Prevention. Available online: https://www.niaid.nih.gov/diseases-conditions/treatment-prevention (accessed on 9 December 2021).
- American Medical Association AMA Adopts New Public Health Policies to Improve Health of National American Medical Association. Available online: https://www.ama-assn.org/press-center/press-releases/ama-adopts-new-public-health-policies-improve-health-nation-3 (accessed on 9 December 2021).
- US Centers for Disease Control and Prevention HIV Treatment as Prevention. Available online: https://www.cdc.gov/hiv/risk/art/index.html (accessed on 9 December 2021).
- Okoli, C.; Van De Velde, N.; Richman, B.; Allan, B.; Castellanos, E.; Young, B.; Brough, G.; Eremin, A.; Corbelli, G.M.; Britton, M.M.; et al. Undetectable equals untransmittable (U = U): Awareness and associations with health outcomes among people living with HIV in 25 countries. Sex Transm. Infect. 2021, 97, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Bor, J.; Fischer, C.; Modi, M.; Richman, B.; Kinker, C.; King, R.; Calabrese, S.K.; Mokhele, I.; Sineke, T.; Zuma, T.; et al. Changing Knowledge and Attitudes Towards HIV Treatment-as-Prevention and “Undetectable = Untransmittable”: A Systematic Review. AIDS Behav. 2021, 25, 4209–4224. [Google Scholar] [CrossRef] [PubMed]
- Holt, M.; Lea, T.; Schmidt, H.M.; Murphy, D.; Rosengarten, M.; Crawford, D.; Ellard, J.; Kolstee, J.; de Wit, J. Increasing Belief in the Effectiveness of HIV Treatment as Prevention: Results of Repeated, National Surveys of Australian Gay and Bisexual Men, 2013–2015. AIDS Behav. 2016, 20, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, P.B.; Westmoreland, D.A.; Patel, V.V.; Grov, C. Awareness and Acceptability of Undetectable = Untransmittable Among a U.S. National Sample of HIV-Negative Sexual and Gender Minorities. AIDS Behav. 2021, 25, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kahle, E.M.; Sullivan, S.P.; Stephenson, R. Birth Cohort Variations Across Functional Knowledge of HIV Prevention Strategies, Perceived Risk, and HIV-Associated Behaviors Among Gay, Bisexual, and Other Men Who Have Sex with Men in the United States. Am. J. Mens Health 2018, 12, 1824–1834. [Google Scholar] [CrossRef]
- Siegel, K.; Meunier, É. Awareness and Perceived Effectiveness of HIV Treatment as Prevention Among Men Who Have Sex with Men in New York City. AIDS Behav. 2019, 23, 1974–1983. [Google Scholar] [CrossRef]
- Carter, A.; Lachowsky, N.; Rich, A.; Forrest, J.I.; Sereda, P.; Cui, Z.; Roth, E.; Kaida, A.; Moore, D.; Montaner, J.S.G.; et al. Gay and bisexual men’s awareness and knowledge of treatment as prevention: Findings from the Momentum Health Study in Vancouver, Canada. J. Int. AIDS Soc. 2015, 18, 20039. [Google Scholar] [CrossRef]
- Rendina, H.J.; Parsons, J.T. Factors associated with perceived accuracy of the Undetectable = Untransmittable slogan among men who have sex with men: Implications for messaging scale-up and implementation. J. Int. AIDS Soc. 2018, 21, e25055. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. HIV in the Southern United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019; Volume 29, pp. 1–4. [Google Scholar]
- Centers for Disease Control and Prevention. Estimated HIV Incidence and Prevalence in the United States, 2015–2019; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; Volume 26. [Google Scholar]
- Petroll, A.E.; Mosack, K.E. Physician awareness of sexual orientation and preventive health recommendations to men who have sex with men. Sex. Transm. Dis. 2011, 38, 63–67. [Google Scholar] [CrossRef]
- Ng, B.E.; Moore, D.; Michelow, W.; Hogg, R.; Gustafson, R.; Robert, W.; Kanters, S.; Thumath, M.; McGuire, M.; Gilbert, M. Relationship between disclosure of same-sex sexual activity to providers, HIV diagnosis and sexual health services for men who have sex with men in Vancouver, Canada. Can. J. Public Health 2014, 105, e186–e191. [Google Scholar] [CrossRef]
- Khalili, J.; Leung, L.B.; Diamant, A.L. Finding the Perfect Doctor: Identifying Lesbian, Gay, Bisexual, and Transgender–Competent Physicians. Am. J. Public Health 2015, 105, 1114. [Google Scholar] [CrossRef] [PubMed]
- Rossman, K.; Salamanca, P.; Macapagal, K. A Qualitative Study Examining Young Adults’ Experiences of Disclosure and Nondisclosure of LGBTQ Identity to Health Care Providers. J. Homosex. 2017, 64, 1390–1410. [Google Scholar] [CrossRef]
- MetLife Mature Market Institute. Still Out, Still Aging: The MetLife Study of Lesbian, Gay, Bisexual, and Transgender Baby Boomers; MetLife: Westport, CT, USA, 2010. [Google Scholar]
- Simpson, T.L.; Balsam, K.F.; Cochran, B.N.; Lehavot, K.; Gold, S.D. Veterans administration health care utilization among sexual minority veterans. Psychol. Serv. 2013, 10, 223–232. [Google Scholar] [CrossRef] [PubMed]
- American Medical Association Creating an LGBTQ-Friendly Practice. Available online: https://www.ama-assn.org/delivering-care/population-care/creating-lgbtq-friendly-practice (accessed on 13 December 2021).
- Sitkin, N.A.; Pachankis, J.E. Specialty Choice Among Sexual and Gender Minorities in Medicine: The Role of Specialty Prestige, Perceived Inclusion, and Medical School Climate. LGBT Health 2016, 3, 451. [Google Scholar] [CrossRef] [PubMed]
- Sabin, J.A.; Riskind, R.G.; Nosek, B.A. Health Care Providers’ Implicit and Explicit Attitudes Toward Lesbian Women and Gay Men. Am. J. Public Health 2015, 105, 1831. [Google Scholar] [CrossRef]
- Aleshire, M.E.; Ashford, K.; Fallin-Bennett, A.; Hatcher, J. Primary Care Providers’ Attitudes Related to LGBTQ People: A Narrative Literature Review. Health Promot. Pract. 2019, 20, 173–187. [Google Scholar] [CrossRef]
- Marlin, R.; Kadakia, A.; Ethridge, B.; Mathews, W.C. Physician Attitudes Toward Homosexuality and HIV: The PATHH-III Survey. LGBT Health 2018, 5, 431. [Google Scholar] [CrossRef]
- Obedin-Maliver, J.; Goldsmith, E.S.; Stewart, L.; White, W.; Tran, E.; Brenman, S.; Wells, M.; Fetterman, D.M.; Garcia, G.; Lunn, M.R. Lesbian, Gay, Bisexual, and Transgender–Related Content in Undergraduate Medical Education. JAMA 2011, 306, 971–977. [Google Scholar] [CrossRef]
- Keuroghlian, A.S.; Ard, K.L.; Makadon, H.J. Advancing health equity for lesbian, gay, bisexual and transgender (LGBT) people through sexual health education and LGBT-affirming health care environments. Sex Health 2017, 14, 119–122. [Google Scholar] [CrossRef]
- Parameshwaran, V.; Cockbain, B.C.; Hillyard, M.; Price, J.R. Is the Lack of Specific Lesbian, Gay, Bisexual, Transgender and Queer/Questioning (LGBTQ) Health Care Education in Medical School a Cause for Concern? Evidence From a Survey of Knowledge and Practice Among UK Medical Students. J. Homosex. 2017, 64, 367–381. [Google Scholar] [CrossRef]
- Mimiaga, M.J.; Goldhammer, H.; Belanoff, C.; Tetu, A.M.; Mayer, K.H. Men who have sex with men: Perceptions about sexual risk, HIV and sexually transmitted disease testing, and provider communication. Sex Transm. Dis. 2007, 34, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Makadon, H.J. Improving Health Care for the Lesbian and Gay Communities. New Engl. J. Med. 2006, 354, 895–897. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.H.; Bradford, J.B.; Makadon, H.J.; Stall, R.; Goldhammer, H.; Landers, S. Sexual and Gender Minority Health: What We Know and What Needs to Be Done. Am. J. Public Health 2008, 98, 989. [Google Scholar] [CrossRef]
- Stupiansky, N.W.; Liau, A.; Rosenberger, J.; Rosenthal, S.L.; Tu, W.; Xiao, S.; Fontenot, H.; Zimet, G.D. Young Men’s Disclosure of Same Sex Behaviors to Healthcare Providers and the Impact on Health: Results from a US National Sample of Young Men Who Have Sex with Men. AIDS Patient Care 2017, 31, 342–347. [Google Scholar] [CrossRef]
- Metheny, N.; Stephenson, R. Disclosure of Sexual Orientation and Uptake of HIV Testing and Hepatitis Vaccination for Rural Men Who Have Sex with Men. Ann. Fam. Med. 2016, 14, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Nahata, L.; Quinn, G.P.; Caltabellotta, N.M.; Tishelman, A.C. Mental Health Concerns and Insurance Denials among Transgender Adolescents. LGBT Health 2017, 4, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Movement Advancement Project Equality Maps: Healthcare Laws and Policies. Available online: https://www.lgbtmap.org/equality-maps/healthcare_laws_and_policies (accessed on 22 August 2022).
- Human Rights Campaign. Healthcare Equality Index 2020; Human Rights Campaign Foundation: Washington, DC, USA, 2020. [Google Scholar]
- Stone, A.L. The Geography of Research on LGBTQ Life: Why sociologists should study the South, rural queers, and ordinary cities. Sociol. Compass 2018, 12, e12638. [Google Scholar] [CrossRef]
- The Williams Institute LGBT Data & Demographics. Available online: https://williamsinstitute.law.ucla.edu/visualization/lgbt-stats/?topic=LGBT&area=4#density (accessed on 29 May 2020).
- Artiga, S.; Damico, A. Health and Health Coverage in the South: A Data Update; Kaiser Family Foundation: Washington, DC, USA, 2016. [Google Scholar]
- Mendoza, N.S.; Moreno, F.A.; Hishaw, G.A.; Gaw, A.C.; Fortuna, L.R.; Skubel, A.; Porche, M.V.; Roessel, M.H.; Shore, J.; Gallegos, A. Affirmative Care Across Cultures: Broadening Application. Focus Am. Psychiatr. Publ. 2020, 18, 31–39. [Google Scholar] [CrossRef]
- Smith, D.M.; Mathews, W.C. Physicians’ attitudes toward homosexuality and HIV: Survey of a California Medical Society- revisited (PATHH-II). J. Homosex. 2007, 52, 1–9. [Google Scholar] [CrossRef]
- Young, S.D.; Bendavid, E. The relationship between HIV testing, stigma, and health service usage. AIDS Care 2010, 22, 373–380. [Google Scholar] [CrossRef]
| Overall (N = 633) | HIV Negative Men (N = 502) | Men Living with HIV (N = 131) | p | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Has LGBTQ Affirming Provider | 413 | 65.2 | 299 | 59.6 | 114 | 87.0 | *** |
| Ever Tested for HIV | 544 | 85.9 | 413 | 82.3 | 138 | 100.0 | *** |
| State of Residence | |||||||
| Alabama | 106 | 16.7 | 83 | 16.5 | 23 | 17.6 | |
| Georgia | 161 | 25.4 | 119 | 23.7 | 42 | 32.1 | |
| North Carolina | 176 | 27.8 | 149 | 29.7 | 27 | 20.6 | |
| Tennessee | 190 | 30.0 | 151 | 30.1 | 39 | 29.8 | |
| Age (M/sd) | 59.4 | 6.30 | 59.7 | 6.4 | 58.5 | 6.0 | |
| Education | ** | ||||||
| High School or less | 29 | 4.6 | 18 | 3.6 | 11 | 8.4 | |
| Some College | 145 | 22.9 | 106 | 21.1 | 39 | 29.8 | |
| College Degree | 218 | 34.4 | 173 | 34.5 | 45 | 34.4 | |
| Graduate/Professional Degree | 241 | 38.1 | 205 | 40.8 | 36 | 27.5 | |
| Race/Ethnicity | *** | ||||||
| White | 559 | 88.3 | 460 | 91.6 | 99 | 75.6 | |
| Black | 38 | 6.0 | 20 | 4.0 | 18 | 13.7 | |
| Other\Multiracial | 36 | 5.7 | 22 | 4.4 | 14 | 10.7 | |
| Partnered | 382 | 60.3 | 329 | 65.5 | 53 | 40.5 | *** |
| Has LGBTQ Affirming Care Provider (N = 633) | Ever Tested for HIV (HIV Negative Men Only; N = 502) | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Living with HIV | 7.10 *** | (3.94–12.80) | ||
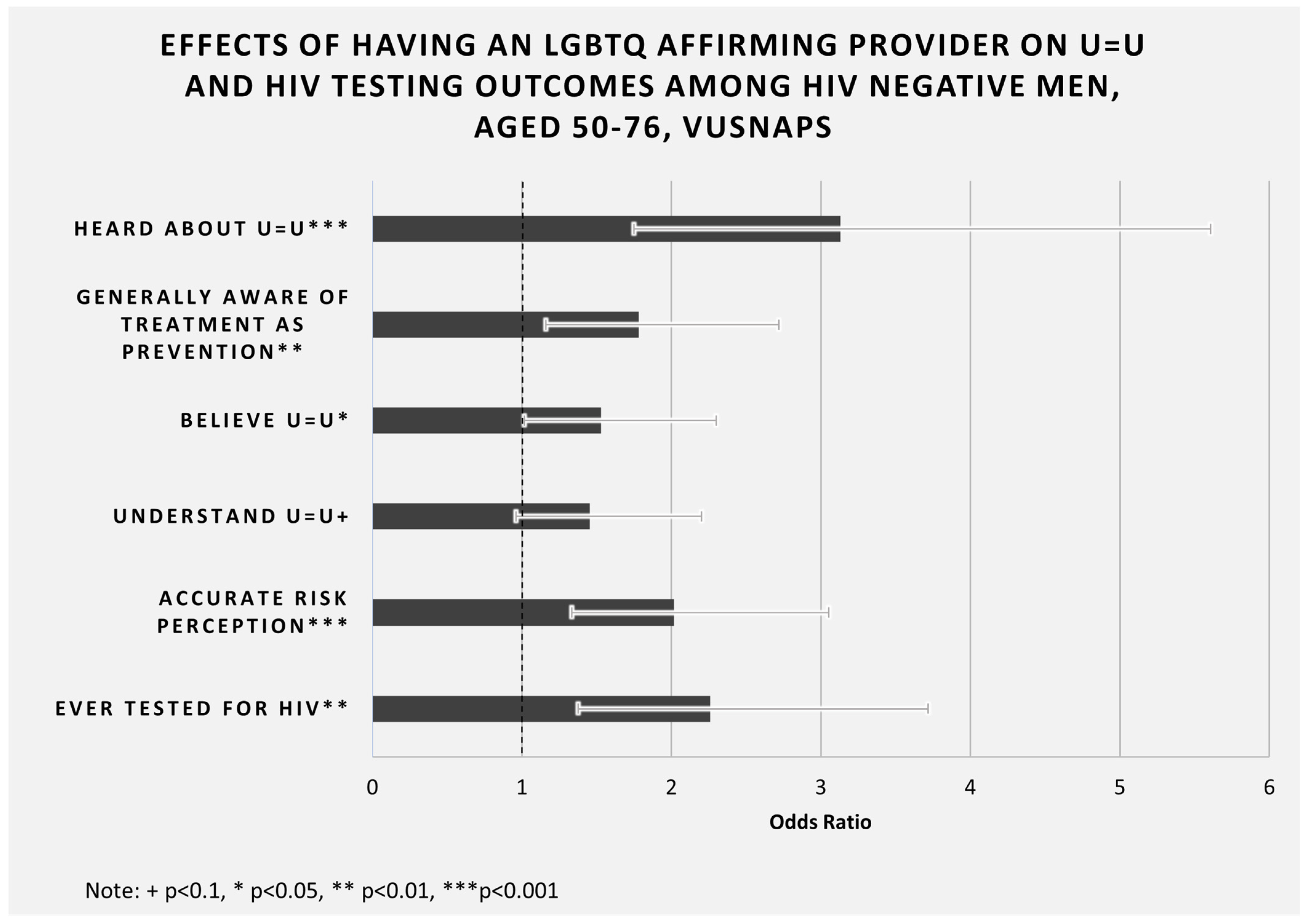
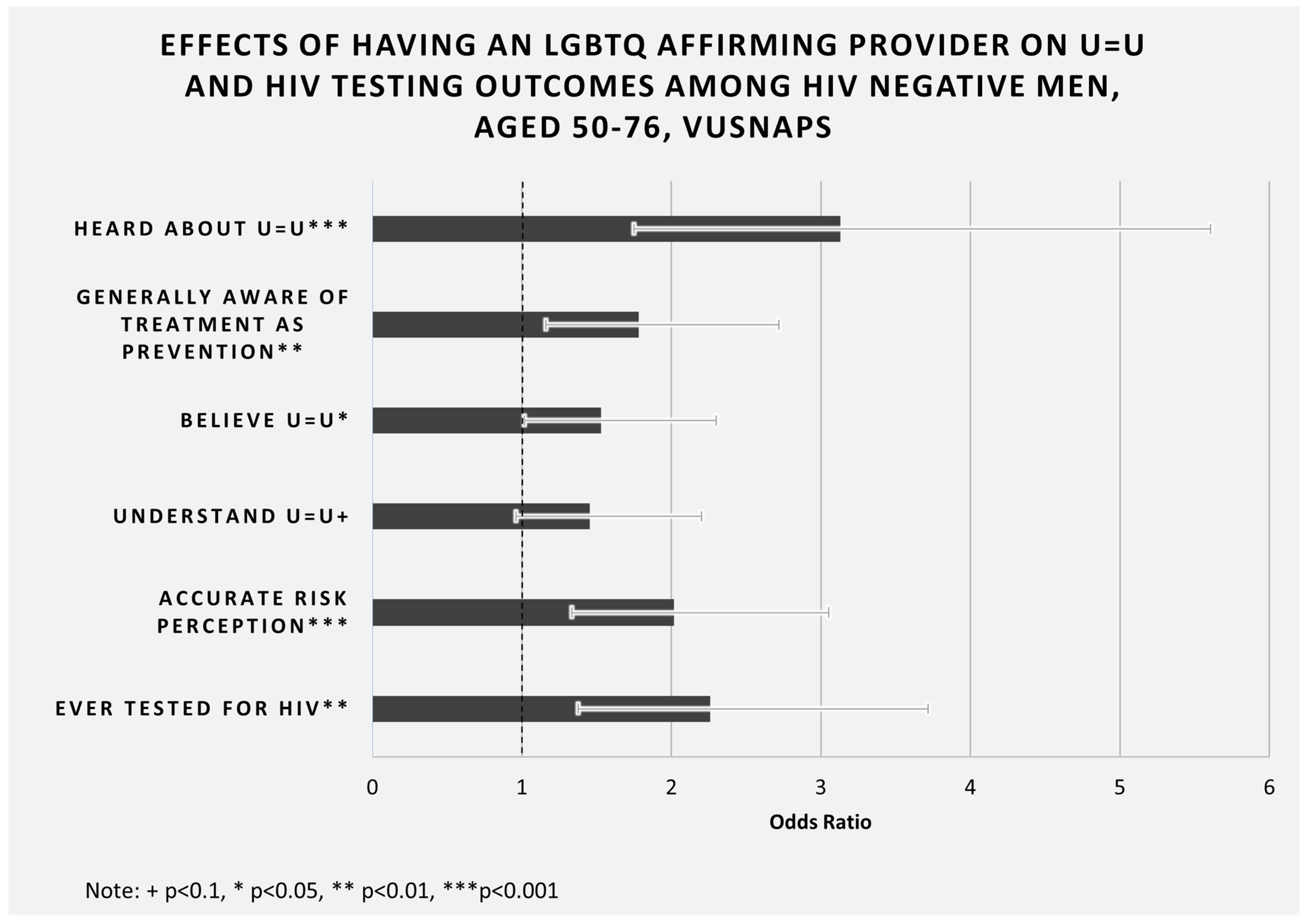
| Has LGBTQ Affirming Provider | -- | 2.260 ** | (1.38–3.72) | |
| State of Residence | ||||
| Georgia | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Alabama | 0.82 | (0.48–1.42) | 0.89 | (0.43–1.85) |
| North Carolina | 1.58 + | (0.96–2.58) | 1.28 | (0.65–2.49) |
| Tennessee | 1.16 | (0.72–1.85) | 1.38 | (0.71–2.68) |
| Age | 0.99 | (0.96–1.01) | 0.97 | (0.93–1.01) |
| Education | ||||
| High School or less | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Some College- | 2.01 | (0.82–4.93) | 0.41 | (0.11–1.56) |
| College Degree | 2.53 * | (1.06–6.15) | 1.21 | (0.31–4.70) |
| Graduate/Professional Degree | 4.62 *** | (1.90–11.21) | 0.78 | (0.20–3.02) |
| Race/Ethnicity | ||||
| White | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Black | 0.86 | (0.39–1.89) | 1.14 | (0.31–4.18) |
| Other\Multiracial | 0.59 | (0.27–1.26) | 0.43 + | (0.16–1.15) |
| Partnered | 1.72 ** | (1.19–2.48) | 0.68 | (0.40–1.16) |
| pseudo R-sq | 0.10 | 0.07 | ||
| Full Sample (N = 633) | |||||||
|---|---|---|---|---|---|---|---|
| Overall | No Affirming Care | Affirming Care | |||||
| N | % | N | % | N | % | p | |
| Heard of U = U Prior to Survey | 160 | 25.3 | 24 | 10.9 | 136 | 32.9 | *** |
| Generally Aware of Treatment as Prevention | 475 | 76.0 | 148 | 67.3 | 327 | 79.4 | *** |
| U = U Believable | 391 | 61.8 | 114 | 51.8 | 277 | 67.1 | *** |
| Correct Application of U = U | 303 | 47.9 | 76 | 34.5 | 227 | 55.0 | *** |
| U = U Decreases Perception of Risk | 351 | 56.3 | 88 | 40.0 | 263 | 63.8 | *** |
| Total | 633 | 100.0 | 220 | 100.0 | 413 | 100.0 | |
| HIV Negative Men (N = 502) | |||||||
| Overall | No Affirming Care | Affirming Care | |||||
| N | % | N | % | N | % | p | |
| Heard of U = U Prior to Survey | 87 | 17.3 | 19 | 9.4 | 68 | 22.7 | *** |
| Generally Aware of Treatment as Prevention | 362 | 71.7 | 135 | 65.5 | 227 | 75.9 | * |
| U = U Believable | 290 | 57.8 | 100 | 49.3 | 190 | 63.5 | *** |
| Correct Application of U = U | 207 | 41.2 | 66 | 32.5 | 141 | 47.2 | *** |
| U = U Decreases Perception of Risk | 238 | 47.4 | 73 | 36.0 | 165 | 55.2 | *** |
| Total | 502 | 100.0 | 203 | 100.0 | 299 | 100.0 | |
| Men Living with HIV (N = 131) | |||||||
| Overall | No Affirming Care | Affirming Care | |||||
| N | % | N | % | N | % | p | |
| Heard of U = U Prior to Survey | 73 | 55.7 | 5 | 29.4 | 68 | 59.6 | * |
| Generally Aware of Treatment as Prevention | 102 | 77.3 | 14 | 82.4 | 88 | 76.5 | |
| U = U Believable | 101 | 77.1 | 14 | 82.4 | 87 | 76.3 | |
| Correct Application of U = U | 96 | 73.3 | 10 | 58.8 | 86 | 75.4 | |
| U = U Decreases Perception of Risk | 113 | 88.3 | 15 | 88.2 | 98 | 88.3 | |
| Total | 131 | 100.0 | 17 | 100.0 | 114 | 100.0 | |
| Heard about U = U | ||||
|---|---|---|---|---|
| HIV Negative Men (N = 502) | Men Living with HIV (N = 131) | |||
| OR | 95% CI | OR | 95% CI | |
| Has LGBTQ Affirming Provider | 3.13 *** | (1.75–5.61) | 4.87 * | (1.31–18.05) |
| Ever Tested for HIV | 1.82 | (0.84–3.93) | -- | |
| State of Residence | ||||
| Georgia | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Alabama | 1.15 | (0.55–2.41) | 3.31 + | (0.88–12.49) |
| North Carolina | 0.56 + | (0.29–1.11) | 0.80 | (0.27–2.38) |
| Tennessee | 0.67 | (0.35–1.29) | 0.51 | (0.19–1.35) |
| Age | 0.98 | (0.95–1.02) | 1.01 | (0.94–1.08) |
| Education | ||||
| High School or less | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Some College | 4.45 | (0.54–36.66) | 3.09 | (0.68–14.09) |
| College Degree | 2.69 | (0.33–21.82) | 0.87 | (0.20–3.84) |
| Graduate/Professional Degree | 3.71 | (0.46–29.85) | 1.55 | (0.34–7.09) |
| Race/Ethnicity | ||||
| White | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Black | 1.94 | (0.67–5.58) | 1.01 | (0.32–3.26) |
| Other\Multiracial | 1.45 | (0.45–4.65) | 3.14 | (0.72–13.59) |
| Partnered | 0.67 | (0.40–1.13) | 3.48 ** | (1.43–8.47) |
| pseudo R-sq | 0.074 | 0.156 | ||
| General Awareness of Treatment as Prevention | ||||
|---|---|---|---|---|
| HIV Negative Men (N = 502) | Men Living with HIV (N = 131) | |||
| OR | 95% CI | OR | 95% CI | |
| Has LGBTQ Affirming Provider | 1.78 ** | (1.16–2.72) | 0.14 | (0.01–1.65) |
| Ever Tested for HIV | 1.73 * | (1.04–2.88) | -- | |
| State of Residence | ||||
| Georgia | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Alabama | 1.05 | (0.53–2.08) | 0.75 | (0.09–6.13) |
| North Carolina | 0.90 | (0.50–1.62) | 0.20 + | (0.03–1.20) |
| Tennessee | 0.45 ** | (0.26–0.79) | 0.35 | (0.06–1.94) |
| Age | 0.98 | (0.95–1.01) | 1.01 | (0.91–1.14) |
| Education | ||||
| High School or less | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Some College | 0.92 | (0.29–2.91) | 1.54 | (0.20–11.86) |
| College Degree | 0.92 | (0.30–2.83) | 2.51 | (0.32–19.62) |
| Graduate/Professional Degree | 1.08 | (0.35–3.33) | 2.32 | (0.28–19.06) |
| Race/Ethnicity | ||||
| White | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Black | 0.65 | (0.24–1.77) | 0.10 ** | (0.02–0.41) |
| Other\Multiracial | 1.04 | (0.98–2.84) | 0.36 | (0.06–2.26) |
| Partnered | 0.65 + | (0.42–1.02) | 0.49 | (0.14–1.71) |
| pseudo R-sq | 0.049 | 0.171 | ||
| Believe U = U | ||||
|---|---|---|---|---|
| HIV Negative Men (N = 502) | Men Living with HIV (N = 131) | |||
| OR | 95% CI | OR | 95% CI | |
| Has LGBTQ Affirming Provider | 1.53 * | (1.02–2.30) | 0.41 | (0.09–1.86) |
| Heard of U = U Prior to Survey | 8.06 *** | (3.75–17.31) | 1.53 | (0.57–4.10) |
| Ever Tested for HIV | 1.39 | (0.84–2.30) | -- | |
| State of Residence | ||||
| Georgia | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Alabama | 0.68 | (0.36–1.28) | 0.24 + | (0.06–1.03) |
| North Carolina | 0.61 + | (0.36–1.05) | 0.28 + | (0.07–1.16) |
| Tennessee | 0.52 * | (0.31–0.89) | 0.24 * | (0.07–0.87) |
| Age | 0.98 | (0.95–1.01) | 1.00 | (0.92–1.08) |
| Education | ||||
| High School or less | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Some College | 1.71 | (0.59–4.98) | 0.27 | (0.03–2.55) |
| College Degree | 1.46 | (0.52–4.09) | 0.28 | (0.03–2.63) |
| Graduate/Professional Degree | 1.69 | (0.60–4.77) | 0.52 | (0.05–5.39) |
| Race/Ethnicity | ||||
| White | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Black | 0.81 | (0.29–2.24) | 0.47 | (0.14–1.66) |
| Other\Multiracial | 1.70 | (0.64–4.50) | 0.41 | (0.11–1.54) |
| Partnered | 0.82 | (0.54–1.25) | 0.72 | (0.28–1.83) |
| pseudo R-sq | 0.11 | 0.10 | ||
| Understands U = U | ||||
|---|---|---|---|---|
| HIV Negative Men (N = 502) | Men Living with HIV (N = 131) | |||
| OR | 95% CI | OR | 95% CI | |
| Has LGBTQ Affirming Provider | 1.45 + | (0.96–2.20) | 1.50 | (0.36–6.23) |
| Heard of U = U Prior to Survey | 3.58 *** | (2.11–6.06) | 9.41 *** | (3.04–29.13) |
| Ever Tested for HIV | 1.31 | (0.77–2.22) | -- | |
| State of Residence | ||||
| Georgia | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Alabama | 0.69 | (0.38–1.28) | 0.24 + | (0.06–1.04) |
| North Carolina | 1.01 | (0.60–1.71) | 0.79 | (0.19–3.24) |
| Tennessee | 0.43 ** | (0.25–0.73) | 0.46 | (0.14–1.51) |
| Age | 0.99 | (0.96–1.02) | 1.00 | (0.92–1.09) |
| Education | ||||
| High School or less | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Some College | 1.89 | (0.56–6.40) | 1.09 | (0.20–5.85) |
| College Degree | 1.72 | (0.52–5.64) | 2.47 | (0.48–12.89) |
| Graduate/Professional Degree | 2.41 | (0.73–7.91) | 2.30 | (0.40–13.17) |
| Race/Ethnicity | ||||
| White | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Black | 0.57 | (0.20–1.59) | 0.48 | (0.14–1.67) |
| Other\Multiracial | 0.25 * | (0.08–0.78) | 6.41 | (0.58–70.79) |
| Partnered | 0.88 | (0.58–1.34) | 1.04 | (0.36–3.00) |
| pseudo R-sq | 0.09 | 0.23 | ||
| U = U Decreases Perception of Risk | ||||
|---|---|---|---|---|
| HIV Negative Men (N = 495) | Men Living with HIV (N = 128) | |||
| OR | 95% CI | OR | 95% CI | |
| Has LGBTQ Affirming Provider | 2.02 *** | (1.33–3.05) | 0.25 | (0.03–2.27) |
| Heard of U = U Prior to Survey | 4.28 *** | (2.41–7.60) | 3.93 + | (0.82–18.94) |
| Ever Tested for HIV | 1.96 * | (1.15–3.35) | -- | |
| State of Residence | ||||
| Georgia | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Alabama | 0.72 | (0.39–1.34) | 0.57 | (0.06–5.85) |
| North Carolina | 0.64 | (0.38–1.09) | 0.27 | (0.04–2.04) |
| Tennessee | 0.54 * | (0.32–0.92) | 0.26 | (0.04–1.53) |
| Age | 0.98 | (0.95–1.01) | 1.02 | (0.90–1.16) |
| Education | ||||
| High School or less | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Some College | 1.68 | (0.55–5.18) | 0.18 | (0.02–1.95) |
| College Degree | 1.58 | (0.53–4.68) | 1.02 | (0.08–13.15) |
| Graduate/Professional Degree | 1.43 | (0.48–4.25) | 1.31 | (0.09–19.28) |
| Race/Ethnicity | ||||
| White | 1.00 | (1.00–1.00) | 1.00 | (1.00–1.00) |
| Black | 1.30 | (0.48–3.55) | 0.18 * | (0.04–0.86) |
| Other\Multiracial | 0.80 | (0.31–2.03) | 0.72 | (0.06–8.07) |
| Partnered | 0.72 | (0.48–1.10) | 1.65 | (0.36–7.61) |
| pseudo R-sq | 0.10 | 0.23 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKay, T.; Akré, E.-R.; Henne, J.; Kari, N.; Conway, A.; Gothelf, I. LGBTQ+ Affirming Care May Increase Awareness and Understanding of Undetectable = Untransmittable among Midlife and Older Gay and Bisexual Men in the US South. Int. J. Environ. Res. Public Health 2022, 19, 10534. https://doi.org/10.3390/ijerph191710534
McKay T, Akré E-R, Henne J, Kari N, Conway A, Gothelf I. LGBTQ+ Affirming Care May Increase Awareness and Understanding of Undetectable = Untransmittable among Midlife and Older Gay and Bisexual Men in the US South. International Journal of Environmental Research and Public Health. 2022; 19(17):10534. https://doi.org/10.3390/ijerph191710534
Chicago/Turabian StyleMcKay, Tara, Ellesse-Roselee Akré, Jeffrey Henne, Nitya Kari, Adam Conway, and Isabel Gothelf. 2022. "LGBTQ+ Affirming Care May Increase Awareness and Understanding of Undetectable = Untransmittable among Midlife and Older Gay and Bisexual Men in the US South" International Journal of Environmental Research and Public Health 19, no. 17: 10534. https://doi.org/10.3390/ijerph191710534
APA StyleMcKay, T., Akré, E.-R., Henne, J., Kari, N., Conway, A., & Gothelf, I. (2022). LGBTQ+ Affirming Care May Increase Awareness and Understanding of Undetectable = Untransmittable among Midlife and Older Gay and Bisexual Men in the US South. International Journal of Environmental Research and Public Health, 19(17), 10534. https://doi.org/10.3390/ijerph191710534