
Well-Being Benefits of Horticulture-Based Activities for Community Dwelling People with Dementia: A Systematic Review

 ,
, 
 and
and
Abstract
:1. Introduction
1.1. Background
1.2. The Need for Non-Pharmacological Intervention for Community-Based Persons with Dementia
1.3. Therapuetic Horticulture
1.4. Biophilia and the Aesthetic Experience of Nature
1.5. Review Objectives and Research Questions
- What evidence exists about the impact of using horticulture-based activities and interventions to enhance well-being for PLWD in community settings?
- What is known about the impact of using horticulture-based activities and interventions on behaviors and symptoms associated with dementia?
- Are there commonalities in evaluation and measurement, i.e., potentially suitable measures and methods that may inform evidence-based practice and future research?
2. Methods
2.1. Information Sources and Search Strategy
- Dementia OR Alzheimer disease OR cognitive impairment;
- AND “Respite care” OR “Respite Community Health” OR “Community Health Service” OR “Home Care” OR “Day care” OR “Domiciliary Care” OR Domiciliary OR “Home Care” OR “Home” OR “Home Service” OR “Independent living” OR “Aging in Place” OR “Community Dwelling” OR “Community” OR Dwelling* OR Community OR Living OR Independent;
- AND “Horticultural therapy” OR “Recreational Therapy” OR horticult* OR “Horticultural Therapy” OR “Nature assisted therapy” OR “green care” OR garden* OR “nature assisted” OR “sociohorticultur” OR “ecotherapy” OR “nature based”.
2.2. Study Eligibility
2.2.1. Inclusion Criteria
2.2.2. Intervention/Activity
2.2.3. Exclusion Criteria
2.2.4. Quality Appraisal
2.2.5. Screening and Data Extraction
2.2.6. Synthesis
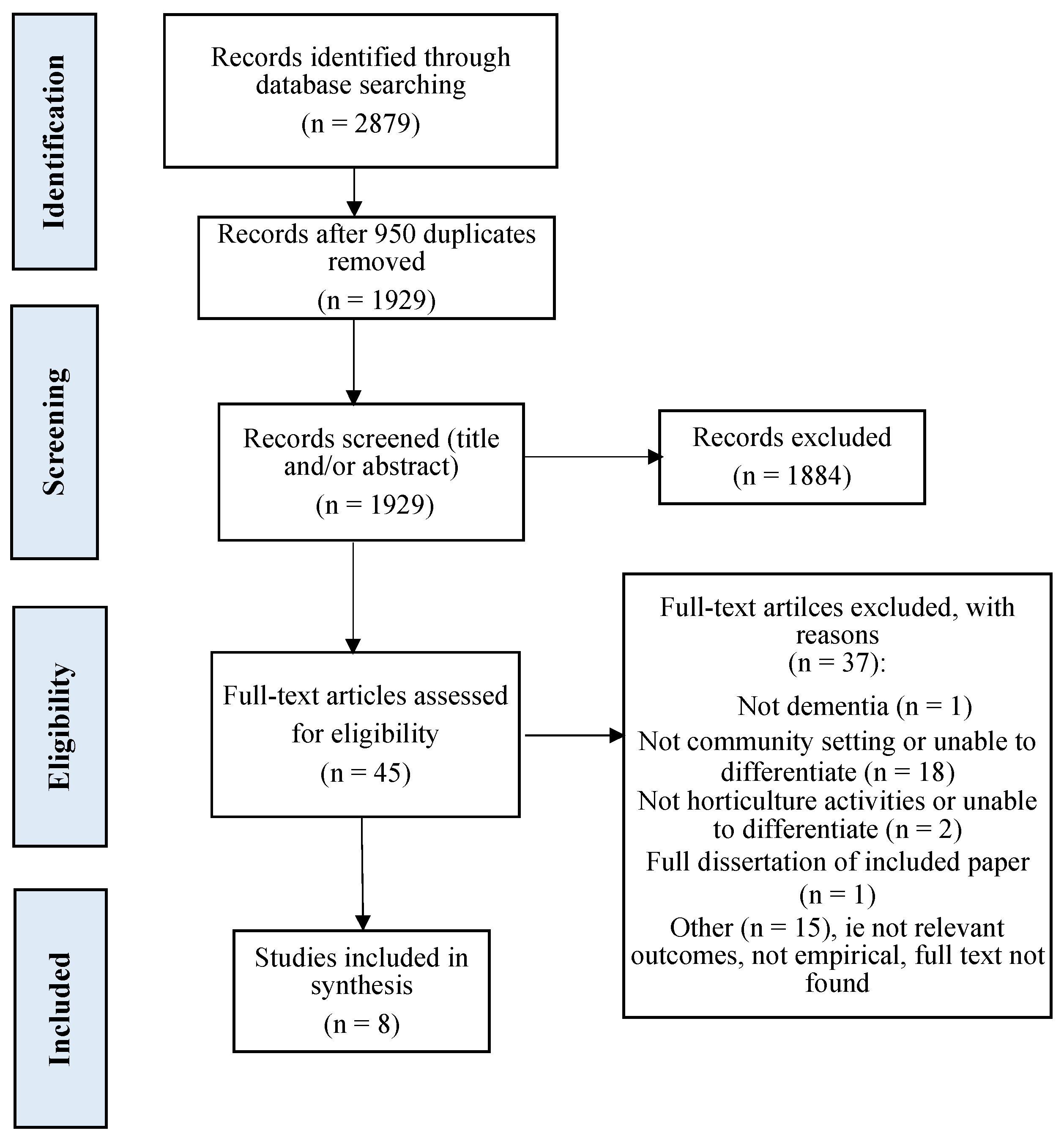
3. Results
3.1. Overview of Studies
3.2. Study Quality
3.3. Outcome Domains
3.4. Measurement
3.5. Program Design and Dosage
3.6. Program Outcomes
3.6.1. Cognitive Function

{kind=link}
| Study | Author(s), Year, Country | Aims | Design | Participants | Intervention or Activity and Intensity | Outcomes | Methods of Data Collection | Main Findings |
|---|---|---|---|---|---|---|---|---|
| [47] | Hall et al., (2016) Canada | To examine if and how to increase engagement in horticultural activities through an improved garden design and person-centered recreational programming, compared with more traditional day program activities. | Mixed methods approach. Descriptive analysis and validated observational tool. | A total of 14 participants in early-to-moderate stages of dementia, i.e., diagnosis or suspected diagnosis of dementia, MMSE 16–26, and prior interest in gardening. M = 84 years; 28.6% female. | A structured horticultural therapy program at adult daycare program, 2 times per week for 10 weeks. Activities included herb garden tour, educational presentations, pet therapy or music therapy in the garden, shelling peas, planting seeds, watering plants, cleaning up the garden, etc. | Well-being and engagement. Lasting impacts of engagement in horticultural therapy program. | ‘Dementia care mapping’ tool [52], assessed based on observations of participants every 5 min during the program. Questionnaire on lasting impact of the intervention completed by the care partners at the end of 10-week program. | For 77.42% of the time, participants had high well-being and engagement with the horticultural therapy. Participants talked more about their experiences in the garden club, expressed happy and enthusiastic emotion, and viewed their gardening work as their personal accomplishment. Four themes identified from qualitative data:
|
| [48] | Hendriks et al., (2016) Netherlands | To develop an approach and decisional tool for personalized nature activities for PLWD. | Mixed methods. Phases 1 and 2: qualitative descriptive design. Phase 3: qualitative descriptive pilot one-group design; thematic and descriptive statistical analysis. | A total of 34 participants across study 3 phases. | Individual and personalized nature activity, e.g., nature walk or a gardening activity, e.g., sowing, watering, fertilizing, harvesting, and cooking with home-grown vegetables. Pilot study executed in Spring 2015; duration of activity engagement recommended as 45–60 min. | Phase 1: preferred or important aspects or activities in nature or outdoor spaces for PLWD. Phase 2: n/a, tool development. Phase 3: (a) behaviors and mood dysregulation and (b) feasibility of personalized nature activities. | Phases 1 and 2: focus group. Phase 3: semi-structured interviews. Observed Emotion Rating Scale [51], Interact instrument (Dorset HealthCare NHS Trust). | Eight themes emerged when being in nature: pleasure; relaxation; feeling fit; enjoying the beauty of nature; feeling free; the social aspect of nature; feeling useful; memories. Preferred activities: walking, cycling, swimming, exercising, sitting outdoors, watching and talking about nature, activities involving animals, flowers or plants, watching films about nature or handcraft with flowers. The decision tools for designing person-centered activities are considered highly to reasonably feasible. |
| [42] | Hewitt et al., (2013) U.K. | Explore changes in well-being resulting from participation in a structured group gardening program for people with young-onset dementia. | Mixed methods qualitative and quantitative; pretest and posttest. | A total of 12 people with young-onset dementia. Inclusion: confirmed diagnosis of dementia, being physically active and interested in gardening, having a caregiver available, access to transport to attend the program. | Structured group gardening program, 2 h weekly for 46 sessions, across one year. Participants helped plan session activities, which included digging and planting with spring flowering bulbs, sweeping leaves, etc. | Cognitive level, activity participation, daily living activities, well-being. | MMSE [43] completed at baseline and again at study mid- and end-points; Bradford Wellbeing Profile [52] by staff observations; semi-structured interviews with care partners’ pretest and posttest. | Results of MMSE and the Well-being Profile showed increased well-being for participants, despite cognitive functioning continuing to decline over the one-year period. Caregivers reported that participants displayed a renewed sense of purpose, independence, and self-esteem. |
| [49] | Jarrott et al., (2002) USA | To compare horticultural activity program to usual activities such as games and crafts. | Quasi-experimental design. | Nine community-dwelling PLWD attending an adult day service. | Horticultural therapy program activities, three times per week across 10 weeks; sessions were 30–45 min. Activities were mostly outside, planting, tending to plants and seedlings. | Activity engagement and affect. | Observational, coding for activity and affect. Affect scale adapted from the Dementia Care Mapping tool [52]. | Participants significantly more engaged during the horticultural activity sessions compared with usual activities. Affect indicated ‘moderate well-being’, although not statistically different between activity conditions. |
| [50] | Lassell et al., (2021) USA | To explore quality of life indicators after engagement in adaptive gardening compared with adaptive horse riding for PLWD. | Descriptive case study design. | Eight participants in early-to-moderate stages of dementia; 4 persons self-selected into the community-based adaptive gardening condition, aged 60–98 years (M = 82). | Weekly, one hour-long community-based gardening for eight weeks, compared with an adaptive (horse) riding program. Activities included planting, harvesting, weeding, exploring the garden. | Quality of life indicators: participation and apparent affect (e.g., anxiety, fear pleasure, interest, gaze). | Modified Activity-in-Context-in-Time, observational tool [53] used to code total of 31 h of videotaped data | Both activities supported ‘positive’ and ‘neutral’ quality of life indicators. Riding provided more opportunities for complex activities compared with gardening (U = 15, p = 0.057), however gardening provided a range of adaptations from more relaxed (e.g., reminiscing, watering) to more active participation (weeding). |
| [57] | Makizako et al., (2019) Japan | To compare the efficacy of physical exercise, horticulture activities, and control condition. | Single blind RCT | A total of 89 participants with depressive symptoms and mild-memory decline, across 3 conditions: horticulture activities, exercise, control. | Weekly, 60–90 min horticulture-based activity program for 20 weeks. Cultivating, growing, harvesting, group gardening, e.g., planting flowers in public gardens. Exercise included dual-task physical and cognitive, e.g., simple calculation tasks while performing stepping exercises. Control group, education classes involved two 90-min classes, topics, e.g., traffic safety, disaster prevention. | Primary outcome(s) measures, depressive symptoms (Geriatric Depression Scale, GDS-15) [45], and memory performance (Wechsler Memory Scale-Revised) [46]. | Three groups compared at baseline, 6 months post-intervention, and 12 months follow-up. Physical performance, social network (Lubben Social Network Scale (LSNS-6) [58], life space, daily physical activity levels (triaxial accelerometer). | GDS-15 scores showed no significant improvements across all groups. Exercise group only obtained higher immediate and delayed recall logical memory scores. Horticulture activity did not improve memory function. Horticulture and control groups showed no differences. |
| [55] | Noone and Jenkins (2018) UK, Glasgow, Scotland | Exploration of the subjective experience of community-based gardening focused on first person experiences (participants with dementia) and caregivers’ views. | Qualitative design, action research approach. | Six participants with diagnosis of any type of dementia (disease stage not specified) recruited from a day center and three program staff. | Community gardening sessions held once per week for six weeks. Activities included planting seeds and seedlings, making bird feeders. | Qualitative thematic analysis of participants’ experiences attending community-based gardening program and views of day center staff. | Semi-structed group interviews with participants and individual interviews with three staff following each of the gardening sessions; researcher reflections. | Gardening is an articulation of identity and selfhood and an expression of agency. It also helps develop new social bonds based on shared interests. Three themes to emerge from interviews were: (i) identity, (ii) agency, (iii) community. |
| [54] | Smith-Carrier et al., (2019) Canada | To explore emotional and sensory experiences of therapeutic gardening for persons with dementia. | Qualitative design. | Six persons with early-stage dementia attending an adult day center. | Therapeutic group gardening program, six waves across five months of spring and fall activities, e.g., planting, harvesting, pruning, clean-up, etc. | Interpretive analysis of participants’ reflections on sensory and emotional experiences in the gardening process. | Six repeated interviews with participants with dementia. | Themes derived from analysis of interviews provided support for the value of gardening for activating the senses, meaningful occupation, socialization, and mental and physical well-being. |
3.6.2. Memory
3.6.3. Physical Function
3.6.4. Social Interaction
3.6.5. Well-Being and Quality of Life
4. Discussion
4.1. Key Features of Programs Promoting Well-Being
4.2. Alleviating Behaviors and Symptoms Associated with Dementia
4.3. Implications for Future Research
4.4. Limitations of Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alzheimer Europe. Prevalence of Dementia in Europe. Available online: www.alzheimer-europe.org (accessed on 9 December 2020).
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Alzheimer’s Disease International. 2015. Available online: http://www.alz.co.uk/research/world-report-2015 (accessed on 2 November 2021).
- Miller, E.A.; Weissert, W.G. Predicting elderly people’s risk for nursing home placement, hospitalization, functional impairment, and mortality: A synthesis. Med. Care Res. Rev. 2000, 57, 259–297. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.; Pedersen, I.; Bergland, A.; Enders-Slegers, M.J.; Jøranson, N.; Calogiuri, G.; Ihlebæk, C. Differences in quality of life in home-dwelling persons and nursing home residents with dementia–a cross-sectional study. BMC Geriatr. 2016, 16, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moniz-Cook, E.; Vernooij-Dassen, M.; Woods, B.; Orrell, M.; Network, I. Psychosocial interventions in dementia care research: The INTERDEM manifesto. Aging Ment. Health 2011, 15, 283–290. [Google Scholar] [CrossRef]
- Nyman, S.R.; Szymczynska, P. Meaningful activities for improving the wellbeing of people with dementia: Beyond mere pleasure to meeting fundamental psychological needs. Perspect. Public Health 2016, 136, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.E.; Wall, M.M.; Kane, R.L.; Menk, J.S.; Sarsour, K.; Johnston, J.A.; Newcomer, R. Does caregiver burden mediate the effects of behavioral disturbances on nursing home admission? Am. J. Geriatr. Psychiatry 2011, 19, 497–506. [Google Scholar] [CrossRef]
- Moyle, W.; Kellett, U.; Ballantyne, A.; Gracia, N. Dementia and loneliness: An Australian perspective. J. Clin. Nurs. 2011, 20, 1445–1453. [Google Scholar] [CrossRef]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef]
- Tilvi, R.S.; Kahonen-Vare, M.H.; Jolkkonen, J.; Valvanne, J.; Pitkala, K.H.; Strandberg, T.E. Predictors of cognitive de-cline and mortality of aged people over a 10-year period. J. Gerontol. 2004, 59, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Bakker, C.; de Vugt, M.E.; van Vliet, D.; Verhey, F.R.; Pijnenburg, Y.A.; Vernooij-Dassen, M.J.; Koopmans, R.T. Predictors of the time to institutionalization in young-versus late-onset dementia: Results from the Needs in Young Onset Dementia (NeedYD) study. J. Am. Med. Dir. Assoc. 2013, 14, 248–253. [Google Scholar] [CrossRef]
- Luppa, M.; Luck, T.; Brähler, E.; König, H.H.; Riedel-Heller, S.G. Prediction of institutionalisation in dementia. Dement. Geriatr. Cogn. Disord. 2008, 26, 65–78. [Google Scholar] [CrossRef]
- Banerjee, S.; Smith, S.C.; Lamping, D.L.; Harwood, R.H.; Foley, B.; Smith, P.; Murray, J.; Prince, M.; Levin, E.; Mann, A.; et al. Quality of life in dementia: More than just cognition. An analysis of associations with quality of life in dementia. J. Neurol. Neurosurg. Psychiatry 2006, 77, 146–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, Y.-C.; Huang, C.-Y.; Kolanowski, A.M.; Huang, H.-L.; Shyu, Y.; Lee, S.-H.; Hsu, W.-C. The effects of participation in leisure activities on neuropsychiatric symptoms of persons with cognitive impairment: A cross-sectional study. Int. J. Nurs. Stud. 2013, 50, 1314–1325. [Google Scholar] [CrossRef] [PubMed]
- Olazarán, J.; Reisberg, B.; Clare, L.; Cruz, I.; Peña-Casanova, J.; Del Ser, T.; Muñiz, R. Nonpharmacological therapies in Alzheimer’s disease: A systematic review of efficacy. Dement. Geriatr. Cogn. Disord. 2010, 30, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Relf, D.; Dorn, S. Horticulture: Meeting the needs of special populations. HortTechnology 1995, 5, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Scott, T.L. Horticultural Therapy. In Encyclopedia of Geropsychology; Pachana, N.A., Ed.; Springer: Singapore, 2015; pp. 1–5. [Google Scholar]
- Simson, S.P.; Staus, M.C. Horticulture as Therapy: Principles and Practice; The Hawthorne Press: Binghamton, NY, USA, 1998. [Google Scholar]
- Cohen-Mansfield, J.; Werner, P. The effects of an enhanced environment on nursing home residents who pace. Gerontologist 1998, 38, 199–208. [Google Scholar] [CrossRef]
- Gonzalez, M.T.; Kirkevold, M. Benefits of sensory garden and horticultural activities in dementia care: A modified scoping review. J. Clin. Nurs. 2014, 23, 2698–2715. [Google Scholar] [CrossRef]
- Lovering, M.J.; Cott, C.A.; Wells, D.L.; Taylor, J.S.; Wells, L.M. A study of a secure garden in the care of people with Alzheimer’s disease. Can. J. Aging/Rev. Can. Vieil. 2002, 21, 417–427. [Google Scholar] [CrossRef]
- Lu, L.-C.; Lan, S.-H.; Hsieh, Y.-P.; Yen, Y.-Y.; Chen, J.-C.; Lan, S.-J. Horticultural therapy in patients with dementia: A systematic review and meta-analysis. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 1533317519883498. [Google Scholar] [CrossRef]
- Marsh, P.; Courtney-Pratt, H.; Campbell, M. The landscape of dementia inclusivity. Health Place 2018, 52, 174–179. [Google Scholar] [CrossRef]
- Whear, R.; Coon, J.T.; Bethel, A.; Abbott, R.; Stein, K.; Garside, R. What is the impact of using outdoor spaces such as gardens on the physical and mental well-being of those with dementia? A systematic review of quantitative and qualitative evidence. J. Am. Med. Dir. Assoc. 2014, 15, 697–705. [Google Scholar] [CrossRef] [Green Version]
- Chalfont, G. Design for Nature in Dementia Care; Jessica Kingsley Publishers: London, UK, 2007. [Google Scholar]
- Brooker, D. What is person-centred care in dementia? Rev. Clin. Gerontol. 2004, 13, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Mcsweeney, J.; Rainham, D.; Johnson, S.A.; Sherry, S.B.; Singleton, J. Indoor nature exposure (INE): A health-promotion framework. Health Promot. Int. 2014, 30, 126–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Kim, S. Effects of indoor gardening on sleep, agitation, and cognition in dementia patients—A pilot study. Int. J. Geriatr. Psychiatry 2008, 23, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.L.; Masser, B.M.; Pachana, N.A. Positive aging benefits of home and community gardening activities: Older adults report enhanced self-esteem, productive endeavours, social engagement and exercise. SAGE Open Med. 2020, 8, 2050312120901732. [Google Scholar] [CrossRef]
- Yotti’Kingsley, J.; Townsend, M. Dig in’to social capital: Community gardens as mechanisms for growing urban social connectedness. Urban Policy Res. 2006, 24, 525–537. [Google Scholar] [CrossRef]
- Wilson, E. Biophilia; Harvard University Press: Cambridge, UK, 1984. [Google Scholar]
- Ulrich, R.S. Biophilia, biophobia, and natural landscapes. In The Biophilia Hypothesis; Kellert, S.R., Wilson, E.O., Eds.; Island Press: Washington, DC, USA, 1993; pp. 73–137. [Google Scholar]
- Kaplan, R.; Kapla, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Liao, M.L.; Ou, S.J.; Heng Hsieh, C.; Li, Z.; Ko, C.C. Effects of garden visits on people with dementia: A pilot study. Dementia 2020, 19, 1009–1028. [Google Scholar] [CrossRef]
- Newton, R.; Keady, J.; Tsekleves, E.; Obe, S.A. ‘My father is a gardener…’: A systematic narrative review on access and use of the garden by people living with dementia. Health Place 2021, 68, 102516. [Google Scholar] [CrossRef]
- Olsson, A.; Lampic, C.; Skovdahl, K.; Engström, M. Persons with early-stage dementia reflect on being outdoors: A repeated interview study. Aging Ment. Health 2013, 17, 793–800. [Google Scholar] [CrossRef]
- Mmako, N.J.; Courtney-Pratt, H.; Marsh, P. Green spaces, dementia and a meaningful life in the community: A mixed studies review. Health Place 2020, 63, 102344. [Google Scholar] [CrossRef]
- Murroni, V.; Cavalli, R.; Basso, A.; Borella, E.; Meneghetti, C.; Melendugno, A.; Pazzaglia, F. Effectiveness of therapeutic gardens for people with dementia: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 9595. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT); version 2018; Registration of Copyright (#1148552); Canadian Intellectual Property Office, Industry Canada: Gatineau, Gatineau, 2018.
- Hewitt, P.; Watts, C.; Hussey, J.; Power, K.; Williams, T. Does a structured gardening programme improve well-being in young-onset dementia? A preliminary study. Br. J. Occup. Ther. 2013, 76, 355–361. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘Mini-mental state’. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Makizako, H.; Tsutsumimoto, K.; Doi, T.; Makino, K.; Nakakubo, S.; Liu-Ambrose, T.; Shimada, H. Exercise and horticultural programs for older adults with depressive symptoms and memory problems: A randomized controlled trial. J. Clin. Med. 2019, 9, 99. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS) Recent Evidence and Development of a Shorter Version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Memory Scale-Revised; Psychological Corporation: San Antonio, TX, USA, 1987. [Google Scholar]
- Hall, J.; Mitchell, G.; Webber, C.; Johnson, K. Effect of horticultural therapy on wellbeing among dementia day care programme participants: A mixed-methods study (Innovative Practice). Dementia 1987, 17, 611–620. [Google Scholar] [CrossRef]
- Hendriks, I.H.; van Vliet, D.; Gerritsen, D.L.; Dröes, R.-M. Nature and dementia: Development of a person-centered approach. Int. Psychogeriatr. 2016, 28, 1455–1470. [Google Scholar] [CrossRef]
- Jarrott, S.E.; Kwack, H.R.; Relf, D. An observational assessment of a dementia-specific horticultural therapy program. HortTechnology 2002, 12, 403–410. [Google Scholar] [CrossRef] [Green Version]
- Lassell, R.; Wood, W.; Schmid, A.A.; Cross, J.E. A comparison of quality of life indicators during two complementary interventions: Adaptive gardening and adaptive riding for people with dementia. Complementary Ther. Med. 2021, 57, 102658. [Google Scholar] [CrossRef]
- Lawton, M.P.; Van Haitsma, K.; Klapper, J. Observed affect in nursing home residents with Alzheimer’s disease. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1996, 51, P3–P14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradford Dementia Group Division of Dementia Studies. University of Bradford: Bradford, UK. 2021. Available online: https://www.bradford.ac.uk/dementia/ (accessed on 9 December 2020).
- Ostrov, J.M.; Hart, E. Observational methods. In The Oxford Handbook of Quantitative Methods Volume I: Foundations; Little, T.D., Ed.; Oxford University Press: New York, NY, USA, 2014; pp. 286–304. [Google Scholar]
- Smith-Carrier, T.A.; Béres, L.; Johnson, K.; Blake, C.; Howard, J. Digging into the experiences of therapeutic gardening for people with dementia: An interpretative phenomenological analysis. Dementia 2019, 20, 130–147. [Google Scholar] [CrossRef] [PubMed]
- Noone, S.; Jenkins, N. Digging for Dementia: Exploring the experience of community gardening from the perspectives of people with dementia. Aging Ment. Health 2018, 22, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Fischer, J.S. Neuropsychological Assessment; Oxford University Press: Oxford, MS, USA, 2004. [Google Scholar]
- Makizako, H.; Shimada, H.; Park, H.; Doi, T.; Yoshida, D.; Uemura, K.; Tsutsumimoto, K.; Suzuki, T. Evaluation of multidimensional neurocognitive function using a tablet personal computer: Test-retest reliability and validity in community-dwelling older adults. Geriatr. Gerontol. Int. 2013, 13, 860–866. [Google Scholar] [CrossRef]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an Abbreviated Version of the Lubben Social Network Scale Among Three European Community-Dwelling Older Adult Populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Gandek, B. Overview of the SF-36 health survey and the International Quality of Life Assessment (IQOLA) Project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Pedrinolla, A.; Tamburin, S.; Brasioli, A.; Sollima, A.; Fonte, C.; Muti, E.; Venturelli, M. An indoor therapeutic garden for behavioral symptoms in alzheimer’s disease: A randomized controlled trial. J. Alzheimer’s Dis. 2019, 71, 813–823. [Google Scholar] [CrossRef]
- Cummings, J. The Neuropsychiatric Inventory: Development and Applications. J. Geriatr. Psychiatry Neurol. 2020, 33, 73–84. [Google Scholar] [CrossRef]
- van Alphen, H.J.; Hortobágyi, T.; van Heuvelen, M.J. Barriers, motivators, and facilitators of physical activity in dementia patients: A systematic review. Arch. Gerontol. Geriatr. 2016, 66, 109–118. [Google Scholar] [CrossRef]
- Kales, H.C.; Gitlin, L.N.; Lyketsos, C.G. Assessment and management of behavioral and psychological symptoms of dementia. BMJ 2015, 350, 369. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J.R. Discovering deviance: The visibility mechanisms through which one becomes a person with dementia in interaction. J. Aging Stud. 2019, 48, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Low, L.F.; White, F.; Jeon, Y.H.; Gresham, M.; Brodaty, H. Desired characteristics and outcomes of community care services for persons with dementia: What is important according to clients, service providers and policy? Australas. J. Ageing 2013, 32, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Travers, C.; Brooks, D.; Hines, S.; O’Reilly, M.; McMaster, M.; He, W.; Beattie, E. Effectiveness of meaningful occupation interventions for people living with dementia in residential aged care: A systematic review. JBI Evid. Synth. 2016, 14, 163–225. [Google Scholar] [CrossRef] [PubMed]
- Phinney, A.; Chaudhury, H.; O’Connor, D.L. Doing as much as I can do: The meaning of activity for people with dementia. Aging Ment. Health 2007, 11, 384–393. [Google Scholar] [CrossRef]
- Johnson, S. Hope in terminal illness: An evolutionary concept analysis. Int. J. Palliat. Nurs. 2007, 13, 451–459. [Google Scholar] [CrossRef]
- Patterson, K. Growth. In Positive Psychology Approaches to Dementia; Clarke, C., Wolverson, E., Eds.; Jessica Kingsley Publishers: London, UK, 2016. [Google Scholar]
- Scott, T.L.; Masser, B.M.; Pachana, N.A. Exploring the health and wellbeing benefits of gardening for older adults. Ageing Soc. 2015, 35, 2176–2200. [Google Scholar] [CrossRef] [Green Version]
- Gigliotti, C.M.; Jarrott, S.E. Effects of horticulture therapy on engagement and affect. Can. J. Aging/Rev. Can. Vieil. 2005, 24, 367–377. [Google Scholar] [CrossRef]
- Gibson, G.; Chalfont, G.E.; Clarke, P.D.; Torrington, J.M.; Sixsmith, A.J. Housing and connection to nature for people with dementia: Findings from the INDEPENDENT project. J. Hous. Elder. 2007, 21, 55–72. [Google Scholar] [CrossRef]
- Logsdon, R.G.; Gibbons, L.E.; McCurry, S.M.; Teri, L. Assessing quality of life in older adults with cognitive impairment. Psychosom. Med. 2002, 64, 510–519. [Google Scholar] [CrossRef]
- O’Connor, D.; Phinney, A.; Smith, A.; Small, J.; Purves, B.; Perry, J.; Beattie, L. Personhood in dementia care: Developing a research agenda for broadening the vision. Dementia 2007, 6, 121–142. [Google Scholar] [CrossRef]
- Tsekleves, E.; Bingley, A.F.; Luján Escalante, M.A.; Gradinar, A. Engaging people with dementia in designing playful and creative practices: Co-design or co-creation? Dementia 2018, 19, 915–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilliam, C.M.; Steffen, A.M. The relationship between caregiving self-efficacy and depressive symptoms in dementia family caregivers. Aging Ment. Health 2006, 10, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, L.; Jones, S.C. Use of day centers for respite by help-seeking caregivers of individuals with dementia. J. Gerontol. Nurs. 2012, 38, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Werner, P.; Mittelman, M.S.; Goldstein, D.; Heinik, J. Family stigma and caregiver burden in Alzheimer’s disease. Gerontologist 2012, 52, 89–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Types of studies | All study designs that focus on horticulture-based activities or interventions, group, or individual gardening programs. | Editorials, commentaries, opinions pieces, and unpublished grey literature. |
| Population | People living with dementia or dyads (PLWD and their family members/care partners); age open (living with young- or late-onset dementia included). | Studies that focus exclusively on care partners not included. |
| Condition | Dementia, all types included. | Delirium not included. |
| Setting | PLWD in the community. | Studies that focus on PLWD in residential care facilities, assisted living, or nursing homes not included. |
| Sources | All studies published in peer reviewed journals, empirical, interventions, case studies in the community. | Publications in languages other than English. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scott, T.L.; Jao, Y.-L.; Tulloch, K.; Yates, E.; Kenward, O.; Pachana, N.A. Well-Being Benefits of Horticulture-Based Activities for Community Dwelling People with Dementia: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10523. https://doi.org/10.3390/ijerph191710523
Scott TL, Jao Y-L, Tulloch K, Yates E, Kenward O, Pachana NA. Well-Being Benefits of Horticulture-Based Activities for Community Dwelling People with Dementia: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(17):10523. https://doi.org/10.3390/ijerph191710523
Chicago/Turabian StyleScott, Theresa L., Ying-Ling Jao, Kristen Tulloch, Eloise Yates, Oliver Kenward, and Nancy A. Pachana. 2022. "Well-Being Benefits of Horticulture-Based Activities for Community Dwelling People with Dementia: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 17: 10523. https://doi.org/10.3390/ijerph191710523
APA StyleScott, T. L., Jao, Y.-L., Tulloch, K., Yates, E., Kenward, O., & Pachana, N. A. (2022). Well-Being Benefits of Horticulture-Based Activities for Community Dwelling People with Dementia: A Systematic Review. International Journal of Environmental Research and Public Health, 19(17), 10523. https://doi.org/10.3390/ijerph191710523