
Validation of the Computerized Cognitive Assessment Test: NNCT

Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Instruments
2.3.1. Cambridge Cognitive Examination-Revised (CAMCOG-R) Scale
2.3.2. Mini-Mental State Examination (MMSE)
2.3.3. Clock Drawing Test (CDT)
2.3.4. Global Deterioration Scale (GDS)
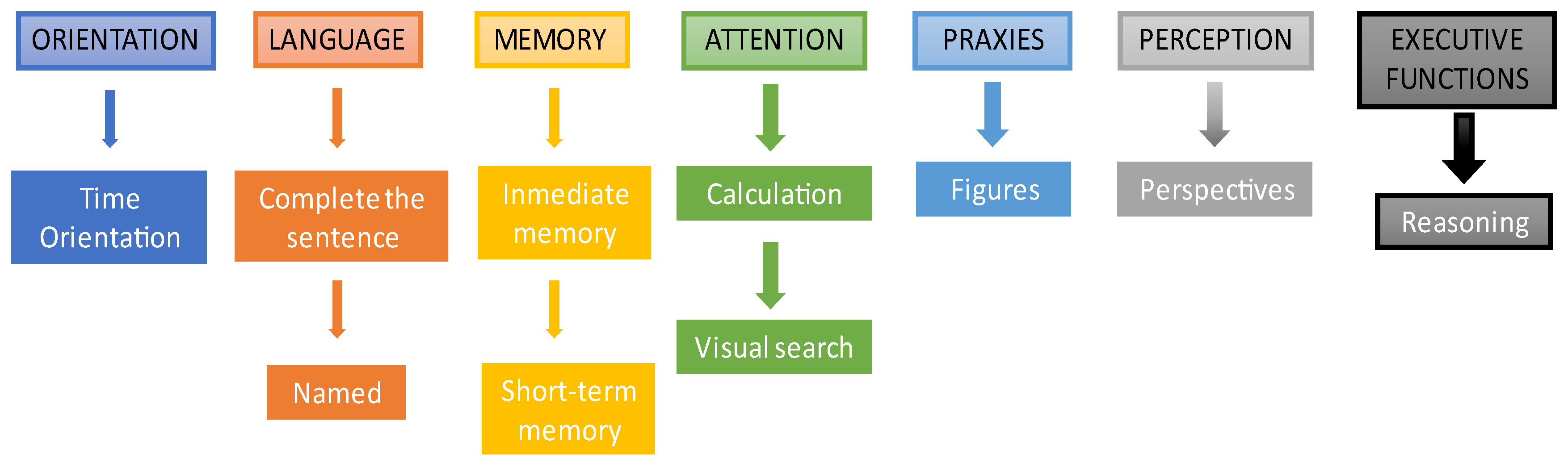
2.3.5. NAIHA Neuro Cognitive Test (NNCT)
3. Results
3.1. Convergent Validity
3.2. Establishment of Judges’ Criteria
3.3. Sensitivity Tests for the General Scale
3.3.1. Healthy Older Adults vs. MCI
3.3.2. Healthy Older Adults Vs. Dementia AD
3.3.3. MCI Vs. Dementia AD
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- WHO. Aging & Health; World Health Organization: Genève, Switzerland, 2021; Available online: https://www.who.int/es/news-room/fact-sheets/detail/envejecimiento-y-salud (accessed on 16 June 2022).
- Castro-Suarez, S. Envejecimiento saludable y deterioro cognitivo. Revista de Neuro-Psiquiatria 2019, 81, 215. [Google Scholar] [CrossRef]
- Morrison, R.L.; Pei, H.; Novak, G.; Kaufer, D.I.; Welsh-Bohmer, K.A.; Ruhmel, S.; Narayan, V.A. A computerized, self-administered test of verbal episodic memory in elderly patients with mild cognitive impairment and healthy participants: A randomized, crossover, validation study. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2018, 10, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.Y.; Chignell, M. A Person-Centered Design Framework for Serious Games for Dementia. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting; SAGE Publications: Los Angeles, CA, USA, 2020; Volume 64, pp. 18–22. [Google Scholar]
- Zygouris, S.; Tsolaki, M. Computerized cognitive testing for older adults: A review. Am. J. Alzheimers Dis. Other Dement. 2015, 30, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Mackin, R.S.; Rhodes, E.; Insel, P.S.; Nosheny, R.; Finley, S.; Ashford, M.; Camacho, M.R.; Truran, D.; Seabrook, K.; Morrison, G.; et al. Home-Based Self-Administration of a Computerized Cognitive Tests of List Learning and Memory using Speech Recognition. Aging Neuropsychol. Cogn. 2021. [Google Scholar] [CrossRef] [PubMed]
- Öhman, F.; Hassenstab, J.; Berron, D.; Schöll, M.; Papp, K.V. Current advances in digital cognitive assessment for preclinical Alzheimer’s disease. In Alzheimer’s and Dementia: Diagnosis, Assessment and Disease Monitoring; John Wiley and Sons Inc.: Hoboken, NJ, USA, 2021; Volume 13. [Google Scholar] [CrossRef]
- Kaplan, E.; Weintraub, Y.S. Boston Naming Test; Lea y Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643. [Google Scholar] [CrossRef]
- Nordlund, A.; Påhlsson, L.; Holmberg, C.; Lind, K.; Wallin, A. The Cognitive Assessment Battery (CAB): A rapid test of cognitive domains. Int. Psychogeriatr. 2011, 23, 1144–1151. [Google Scholar] [CrossRef]
- Fredrickson, J.; Maruff, P.; Woodward, M.; Moore, L.; Fredrickson, A.; Sach, J.; Darby, D. Evaluation of the usability of a brief computerized cognitive screening test in older people for epidemiological studies. Neuroepidemiology 2010, 34, 65–75. [Google Scholar] [CrossRef]
- Snyder, P.J.; Jackson, C.E.; Petersen, R.C.; Khachaturian, A.S.; Kaye, J.; Albert, M.S.; Weintraub, S. Assessment of cognition in mild cognitive impairment: A comparative study. Alzheimers Dement. 2011, 7, 338–355. [Google Scholar] [CrossRef]
- Mielke, M.M.; Weigand, S.D.; Wiste, H.J.; Vemuri, P.; MacHulda, M.M.; Knopman, D.S.; Lowe, V.; Roberts, R.O.; Kantarci, K.; Rocca, W.A.; et al. Independent comparison of CogState computerized testing and a standard cognitive battery with neuroimaging. Alzheimers Dement. 2014, 10, 779–789. [Google Scholar] [CrossRef]
- Hammers, D.; Spurgeon, E.; Ryan, K.; Persad, C.; Barbas, N.; Heidebrink, J.; Darby, D.; Giordani, B. Validity of a brief computerized cognitive screening test in dementia. J. Geriatr. Psychiatry Neurol. 2012, 25, 89–99. [Google Scholar] [CrossRef]
- Doniger, G.M.; Zucker, D.M.; Schweiger, A.; Dwolatzky, T.; Chertkow, H.; Crystal, H.; Simon, E.S. Towards Practical Cognitive Assessment for Detection of Early Dementia: A 30-Minute Computerized Battery Discriminates as Well as Longer Testing. Curr. Alzheimer Res. 2005, 2, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Dwolatzky, T.; Dimant, L.; Simon, E.S.; Doniger, G.M. Validity of a short computerized assessment battery for moderate cognitive impairment and dementia. Int. Psychogeriatr. 2010, 22, 795–803. [Google Scholar] [CrossRef]
- Gold, M.; Amatniek, J.; Carrillo, M.C.; Cedarbaum, J.M.; Hendrix, J.A.; Miller, B.B.; Robillard, J.M.; Rice, J.J.; Soares, H.; Tome, M.B.; et al. Digital technologies as biomarkers, clinical outcomes assessment, and recruitment tools in Alzheimer’s disease clinical trials. In Alzheimer’s and Dementia: Translational Research and Clinical Interventions; Elsevier Inc.: Amsterdam, The Netherlands, 2018; Volume 4, pp. 234–242. [Google Scholar] [CrossRef]
- Piau, A.; Wild, K.; Mattek, N.; Kaye, J. Current state of digital biomarker technologies for real-life, home-based monitoring of cognitive function for mild cognitive impairment to mild Alzheimer disease and implications for clinical care: Systematic review. J. Med. Internet Res. 2019, 21, e12785. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Sun, K.; Huynh, D.; Phi, H.Q.; Ko, B.; Huang, B.; Ghomi, R.H. A Computerized Cognitive Test Battery for Detection of Dementia and Mild Cognitive Impairment: Instrument Validation Study. JMIR Aging 2022, 5, e36825. [Google Scholar] [CrossRef] [PubMed]
- Bayahya, A.Y.; Alhalabi, W.; AlAmri, S.H. Smart Health System to Detect Dementia Disorders Using Virtual Reality. Healthcare 2021, 9, 810. [Google Scholar] [CrossRef] [PubMed]
- Takechi, H.; Yoshino, H. Usefulness of CogEvo, a computerized cognitive assessment and training tool, for distinguishing patients with mild Alzheimer’s disease and mild cognitive impairment from cognitively normal older people. Geriatr. Gerontol. Int. 2021, 21, 192–196. [Google Scholar] [CrossRef]
- Zhao, X.; Hu, R.; Wen, H.; Xu, G.; Pang, T.; He, X.; Zhang, Y.; Zhang, J.; Chen, C.; Wu, X.; et al. A voice recognition-based digital cognitive screener for dementia detection in the community: Development and validation study. Front. Psychiatry 2022, 13, 899729. [Google Scholar] [CrossRef]
- Ding, Z.; Lee, T.; Chan, A.S. Digital Cognitive Biomarker for Mild Cognitive Impairments and Dementia: A Systematic Review. J. Clin. Med. 2022, 11, 4191. [Google Scholar] [CrossRef]
- Royall, D.R.; Palmer, R.; Chiodo, L.K.; Polk, M.J.; Royall, D.; Psychiatry, Ã. Executive Control Mediates Memory’s Association with Change in Instrumental Activities of Daily Living: The Freedom House Study. J. Am. Geriatr. Soc. 2005, 53, 11–17. [Google Scholar] [CrossRef]
- Xiao, Y.; Jia, Z.; Dong, M.; Song, K.; Li, X.; Bian, D.; Li, Y.; Jiang, N.; Shi, C.; Li, G. Development and validity of computerized neuropsychological assessment devices for screening mild cognitive impairment: Ensemble of models with feature space heterogeneity and retrieval practice effect. J. Biomed. Inform. 2022, 131, 104108. [Google Scholar] [CrossRef]
- Dorociak, K.E.; Mattek, N.; Lee, J.; Leese, M.I.; Bouranis, N.; Imtiaz, D.; Doane, B.M.; Bernstein, J.P.K.; Kaye, J.A.; Hughes, A.M. The Survey for Memory, Attention, and Reaction Time (SMART): Development and Validation of a Brief Web-Based Measure of Cognition for Older Adults. Gerontology 2021, 67, 740–752. [Google Scholar] [CrossRef] [PubMed]
- Tsoy, E.; Zygouris, S.; Possin, K.L. Current State of Self-Administered Brief Computerized Cognitive Assessments for Detection of Cognitive Disorders in Older Adults: A Systematic Review. J. Prev. Alzheimers Dis. 2021, 8, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Roth, M.; Huppert, F.A.; Mountjoy, C.Q.; Tym, E. CAMDEX: The Cambridge Examination for Mental Disorders of the Elderly. In Cambridge Cognitive Examination (CAMCOG); Cambridge University: Cambridge, UK, 1988; pp. 19–28. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Cacho, J.; García-García, R.; Arcaya, J.; Vicente, J.L.; Lantada, N. Una propuesta de aplicación y puntuación del test del reloj en la enfermedad de Alzheimer. Rev. Neurol. 1999, 28, 648–655. [Google Scholar] [PubMed]
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subscales | Correlation (p<) | Subscale MMSE | Subscale CAMCOG | Total MMSE | CDT |
|---|---|---|---|---|---|
| Orientation | 0.001 | 0.735 | 0.732 | 0.464 | 0.582 |
| Language | 0.001 | 0.220 | 0.312 | 0.253 | 0.224 |
| Memory | 0.001 | 0.263 | 0.401 | 0.275 | 0.328 |
| Attention | 0.001 | 0.401 | 0.307 | 0.304 | |
| Praxis | 0.001 | 0.240 | 0.183 | 0.276 | |
| Executive Function | 0.05 | 0.174 1 |
| NNCT Scores | Sensibility | Specificity |
|---|---|---|
| 22.5 | 0.943 | 0.159 |
| 23.5 | 0.9 | 0.25 |
| 24.5 | 0.857 | 0.341 |
| 25.5 | 0.829 | 0.5 |
| 26.5 | 0.743 | 0.568 |
| 27.25 | 0.643 | 0.659 |
| 27.75 | 0.629 | 0.659 |
| 28.5 | 0.571 | 0.795 |
| 29.5 | 0.486 | 0.864 |
| 30.5 | 0.443 | 0.8861 1 |
| NNCT Scores | Sensibility | Specificity |
|---|---|---|
| 20.5 | 0.971 | 0.485 |
| 21.5 | 0.957 | 0.515 |
| 22.5 | 0.943 | 0.576 |
| 23.5 | 0.9 | 0.636 |
| 24.5 | 0.857 | 0.727 |
| 25.5 | 0.829 | 0.788 |
| 26.5 | 0.743 | 0.879 |
| 27.3 | 0.643 | 0.879 |
| 27.8 | 0,629 | 0.879 |
| 28.5 | 0.571 | 0.9093 3 |
| NNCT Scores | Sensibility | Specificity |
|---|---|---|
| 15.5 | 0.977 | 0.303 |
| 16.5 | 0.977 | 0.333 |
| 17.5 | 0.977 | 0.364 |
| 18.5 | 0.955 | 0.364 |
| 19.5 | 0.955 | 0.485 |
| 20.5 | 0.909 | 0.485 |
| 21.5 | 0.909 | 0.515 |
| 22.5 | 0.841 | 0.576 |
| 23.5 | 0.75 | 0.636 |
| 24.5 | 0.659 | 0.7275 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliva, I.; Losa, J. Validation of the Computerized Cognitive Assessment Test: NNCT. Int. J. Environ. Res. Public Health 2022, 19, 10495. https://doi.org/10.3390/ijerph191710495
Oliva I, Losa J. Validation of the Computerized Cognitive Assessment Test: NNCT. International Journal of Environmental Research and Public Health. 2022; 19(17):10495. https://doi.org/10.3390/ijerph191710495
Chicago/Turabian StyleOliva, Itxasne, and Joan Losa. 2022. "Validation of the Computerized Cognitive Assessment Test: NNCT" International Journal of Environmental Research and Public Health 19, no. 17: 10495. https://doi.org/10.3390/ijerph191710495
APA StyleOliva, I., & Losa, J. (2022). Validation of the Computerized Cognitive Assessment Test: NNCT. International Journal of Environmental Research and Public Health, 19(17), 10495. https://doi.org/10.3390/ijerph191710495