
Changing Primary School Children’s Engagement in Active School Travel Using Safe Routes to School Interventions: A Rapid Realist Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
Rapid Realist Review
2.2. Advisory Panels
2.3. Literature Scoping
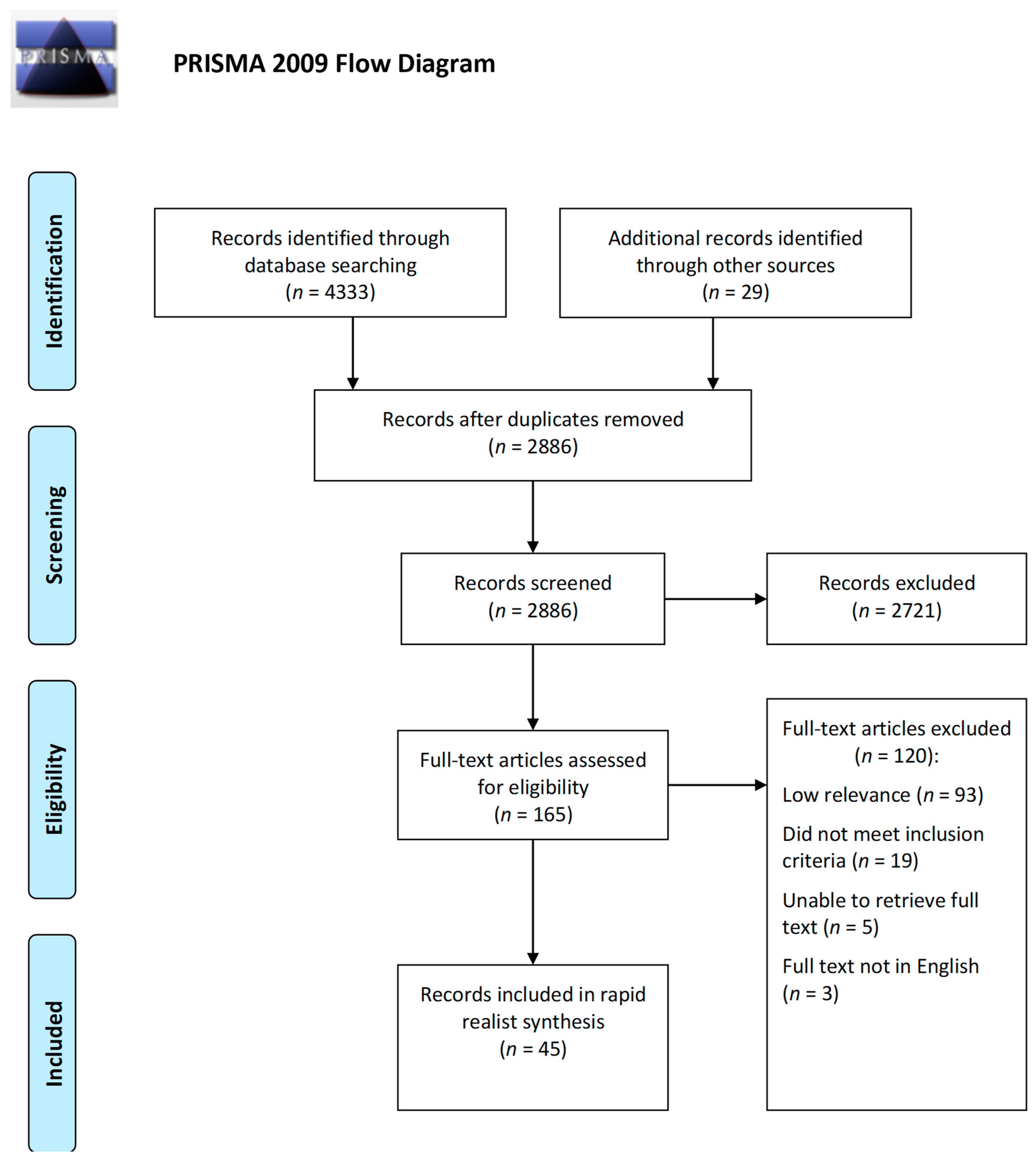
2.4. Literature Searching and Screening
2.5. Document Selection and Appraisal
2.6. Data Extraction
2.7. Data Analysis and Synthesis
3. Results
3.1. Document Characteristics
3.2. CMOCs and Program Theory
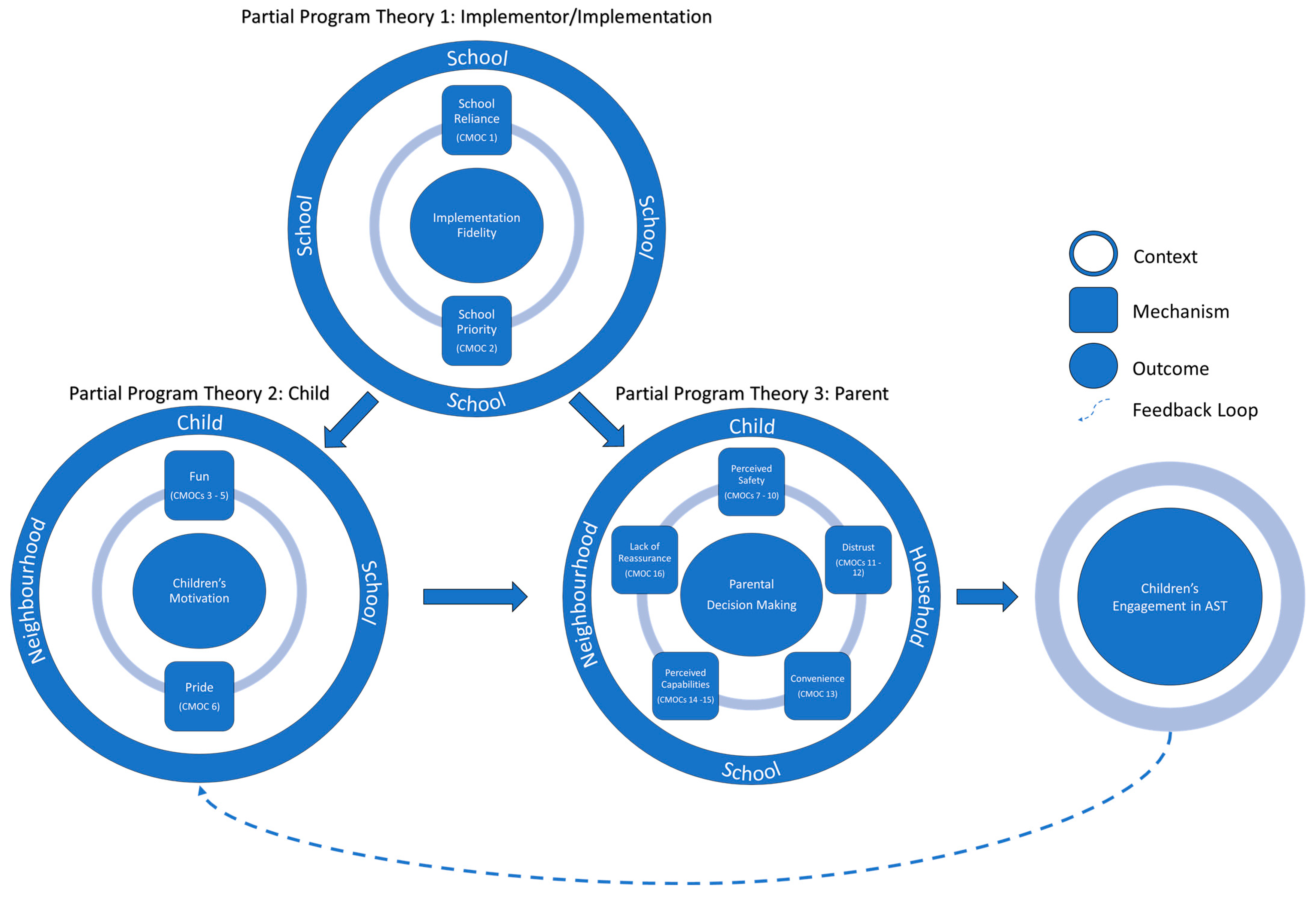
3.2.1. Partial Program Theory One: Implementor/Implementation
Overreliance on Facilitator/Reliance on Champion (CMOC 1)
“[Who the] facilitator is, can, in my experience, make or break the success of the school travel plan. I think it is very important that they believe in the program. If it is just kind of a thing that they have to do… I don’t find that it is nearly as successful as someone who really believes in the program, gets it, is passionate about it, and drives it and makes it happen.”
Perceived Priority Relative to Support (CMOC 2)
[…schools appeared to have other important issues to deal with, which meant that “add-on” programs like the Ride2School program received less attention than other key priority issues… these schools appeared to require greater levels of support and resources to implement the program…]
[Overall, the demands of the facilitator role was [sic] acknowledged to be one of the greatest challenges and potential liabilities for program success.]
Summary of Partial Program Theory One: Implementor/Implementation
3.2.2. Partial Program Theory Two: Child
Fun (CMOCs 3–5)
[The children enjoyed walking to school… it gave them the opportunity to be with their friends, play games, talk about “things” that mattered to them such as “Star Wars and Lego”, and arrange play dates.]
“I would rather walk but no one who lives down my street walks. If I walked I would have to do it by myself.”
“I like walking past trees because they look nice. They have flowers that I really like and sometimes I want to pick some flowers and take them to school.”
[Parents reported how their children thought it was fun to put stickers on the board for every kilometer they walked or biked to and from school; they were trying to meet the challenge and were motivated to use AST.]
Pride (CMOC 6)
[They expressed that their children were proud of being part of this project… Halfway into the intervention, they received a cap with the text ‘I walk and bike to school’ (in Swedish), which served as an acknowledgement of being part of the project. This made them engage in more walking and biking…]
Summary of Partial Program Theory Two: Child
3.2.3. Partial Program Theory Three: Parent
Perceived Safety (CMOCs 7–10)
[Parents claimed that they have witnessed repeated incidents of cars refusing to stop at pedestrian crossings en route to school and cars regularly driving down the wrong side of the road to get around stationary traffic. Two parents said that concerns over road safety led them to drive to school as they felt their children were not provided with a safe walking environment.]
“… And the infrastructure is there, and we’ve got the bike paths or the footpaths to do it safely.”
“… I start worrying about [him] because he’s not on a main road if anything happens, no one’s going to see what happened if you know what I mean…”
“It can also just be scary if the groups of middle school kids come and they’re intimidating to the little kids”
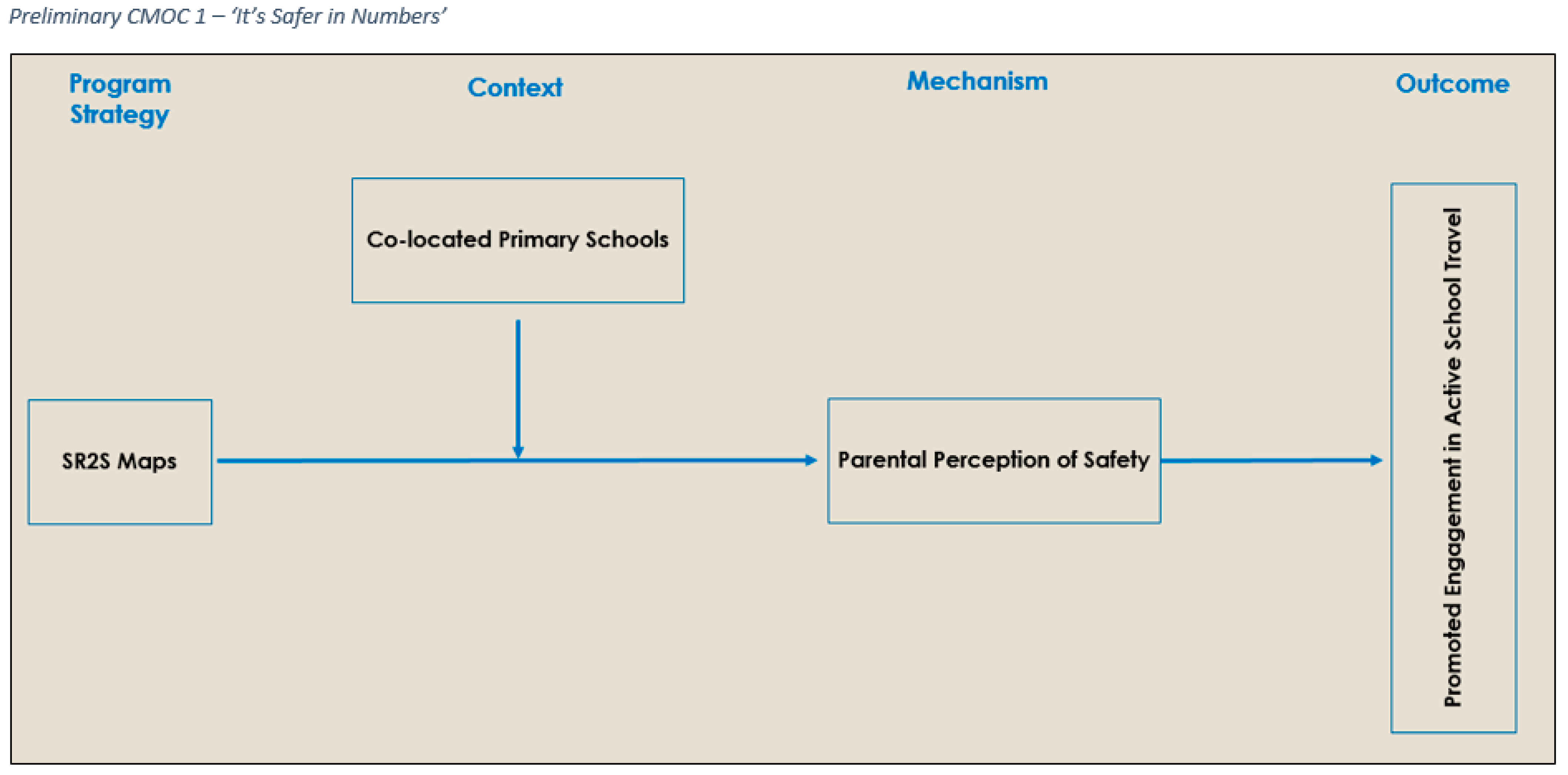
[“if it’s a whole bunch of kids walking up at the same time” because there is “safety in numbers”]
“I always feel more secure if I know there’s other people who might keep an eye on my kids or might help my kids if they need help”
Distrust (CMOCs 11–12)
“… I don’t find it as safe as what it used to be when I was growing up. I remember walking around and it didn’t matter, but now you just can’t trust anyone, really, especially if you don’t know them.”
“… At least when it’s you with them you can control things a little bit more but when they meet up with other kids you just have no idea what’s going to happen.”
Convenience (CMOC 13)
[For many parents, the timing of the school start and their work made it impossible to bike or walk with their child, and so they preferred to drop their child off on their way to work…]
[For some parents walking was the preference because they lived close to the school. Some parents said it is quicker to walk than drive due to road congestion and parking constrains.]
Perceived Capabilities (CMOCs 14–15)
“School is about 30 minutes’ walk. He’s four and he’s a tiny four so it’s quite a long walk really. When my son gets older he might be able to walk further.”
“I don’t think she can cross this main road at the bottom on her own… I don’t think she’s really got that concept yet of crossing the road properly…”
“I was skeptical [sic] before, and felt like the study would force us to change our way of managing transport to school, but afterwards, when I realized that she managed to go to school by herself with a friend, then it was only positive…”
Reassurance (CMOC 16)
“If I wouldn’t be able to know if they had arrived safely to school, then I wouldn’t be able to relax at work, I need some kind of confirmation to be able to unwind, you know, ok now they are at school, now I can breathe out”
Summary of Partial Program Theory Three: Parent
3.2.4. Overarching Program Theory
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Physical Activity Fact Sheet. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 30 June 2022).
- World Health Organisation. Global Recommendations on Physical Activity for Health. 2010. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 16 March 2022).
- Aubert, S.; Barnes, J.; Abdeta, C.; Abi Nader, P.; Adeniyi, A.; Aguilar-Farias, N.; Andrade Tenesaca, D.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis from 49 Countries. J. Phys. Act. Health 2018, 15, 251–273. [Google Scholar] [CrossRef] [PubMed]
- van Sluijs, E.; Fearne, V.; Mattocks, C.; Riddoch, C.; Griffin, S.; Ness, A. The Contribution of Active Travel to Children’s Physical Activity Levels: Cross-Sectional Results from the ALSPAC Study. Prev. Med. 2009, 48, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Denstel, K.; Broyles, S.; Larouche, R.; Sarmiento, O.; Barreira, T.; Chaput, J.; Church, T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. Active School Transport and Weekday Physical Activity In 9–11-Year-Old Children from 12 Countries. Int. J. Obes. Suppl. 2015, 5, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Saunders, T.; John Faulkner, G.; Colley, R.; Tremblay, M. Associations between Active School Transport and Physical Activity, Body Composition, and Cardiovascular Fitness: A Systematic Review of 68 Studies. J. Phys. Act. Health 2014, 11, 206–227. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Boreham, C.; Kelly, P.; Foster, C. The Relationship Between Active Travel to School and Health-Related Fitness in Children and Adolescents: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 5. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.; Gray, C.; Akinroye, K.; Harrington, D.; Katzmarzyk, P.; Lambert, E.; Liukkonen, J.; Maddison, R.; Ocansey, R.; Onywera, V.; et al. Physical Activity of Children: A Global Matrix of Grades Comparing 15 Countries. J. Phys. Act. Health 2014, 11, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Fyhri, A.; Hjorthol, R.; Mackett, R.; Fotel, T.; Kyttä, M. Children’s Active Travel and Independent Mobility in Four Countries: Development, Social Contributing Trends and Measures. Transp. Policy 2011, 18, 703–710. [Google Scholar] [CrossRef]
- van der Ploeg, H.; Merom, D.; Corpuz, G.; Bauman, A. Trends in Australian Children Traveling to School 1971–2003: Burning Petrol or Carbohydrates? Prev. Med. 2008, 46, 60–62. [Google Scholar] [CrossRef]
- Aranda-Balboa, M.; Huertas-Delgado, F.; Herrador-Colmenero, M.; Cardon, G.; Chillón, P. Parental Barriers to Active Transport to School: A Systematic Review. Int. J. Public Health 2019, 65, 87–98. [Google Scholar] [CrossRef]
- Lu, W.; McKyer, E.; Lee, C.; Goodson, P.; Ory, M.; Wang, S. Perceived Barriers to Children’s Active Commuting to School: A Systematic Review of Empirical, Methodological and Theoretical Evidence. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 140. [Google Scholar] [CrossRef]
- Villa-González, E.; Barranco-Ruiz, Y.; Evenson, K.; Chillón, P. Systematic Review of Interventions for Promoting Active School Transport. Prev. Med. 2018, 111, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Mammen, G.; Rowe, D.; Faulkner, G. Effectiveness of Active School Transport Interventions: A Systematic Review and Update. BMC Public Health 2018, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Blackburn, N.; Woods, C.; Byrne, M.; van Nassau, F.; Tully, M. Interventions Promoting Active Transport to School in Children: A Systematic Review and Meta-Analysis. Prev. Med. 2019, 123, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Safe Routes Partnership. History of Safe Routes to School. 2017. Available online: https://www.saferoutespartnership.org/safe-routes-school/101/history (accessed on 18 March 2022).
- US Department of Transportation. Safe Routes to School Programs. 2015. Available online: https://www.transportation.gov/mission/health/Safe-Routes-to-School-Programs (accessed on 18 March 2022).
- Safe Routes Partnership. The 6 E’s of Safe Routes to School. 2020. Available online: https://www.saferoutespartnership.org/safe-routes-school/101/6-Es (accessed on 18 March 2022).
- Pang, B.; Kubacki, K.; Rundle-Thiele, S. Promoting Active Travel to School: A Systematic Review (2010–2016). BMC Public Health 2017, 17, 638. [Google Scholar] [CrossRef]
- Chillón, P.; Evenson, K.; Vaughn, A.; Ward, D. A Systematic Review of Interventions for Promoting Active Transportation to School. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 10. [Google Scholar] [CrossRef]
- Buttazzoni, A.; Van Kesteren, E.; Shah, T.; Gilliland, J. Active School Travel Intervention Methodologies in North America: A Systematic Review. Am J Prev. Med. 2018, 55, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Sarmiento, O.; Broyles, S.; Denstel, K.; Church, T.; Barreira, T.; Chaput, J.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. Are the Correlates of Active School Transport Context-Specific? Int. J. Obes. Suppl. 2015, 5, 89–99. [Google Scholar] [CrossRef]
- Jagosh, J. Realist Synthesis for Public Health: Building an Ontologically Deep Understanding of How Programs Work, For Whom, and In Which Contexts. Annu. Rev. Public Health 2019, 40, 361–372. [Google Scholar] [CrossRef]
- Pawson, R. Evidence-Based Policy: A Realist Perspective; SAGE Publications Inc.: London, UK, 2006; ISBN 9781412910606. [Google Scholar]
- Pawson, R.; Wong, G.; Owen, L. Known Knowns, Known Unknowns, Unknown Unknowns. Am. J. Eval. 2011, 32, 518–546. [Google Scholar] [CrossRef]
- Saul, J.; Willis, C.; Bitz, J.; Best, A. A Time-Responsive Tool for Informing Policy Making: Rapid Realist Review. Implement. Sci. 2013, 8, 103. [Google Scholar] [CrossRef]
- Wong, G.; Greenhalgh, T.; Westhorp, G.; Buckingham, J.; Pawson, R. RAMESES Publication Standards: Realist Syntheses. BMC Med. 2013, 11, 21. [Google Scholar] [CrossRef]
- Brown, S.; Lhussier, M.; Dalkin, S.; Eaton, S. Care Planning: What Works, For Whom, and In What Circumstances? A Rapid Realist Review. Qual. Health Res. 2018, 28, 2250–2266. [Google Scholar] [CrossRef] [PubMed]
- Mukumbang, F.; Marchal, B.; Van Belle, S.; van Wyk, B. Using the Realist Interview Approach to Maintain Theoretical Awareness in Realist Studies. Qual. Res. 2019, 20, 485–515. [Google Scholar] [CrossRef]
- Booth, A. Searching for Qualitative Research for Inclusion in Systematic Reviews: A Structured Methodological Review. Syst. Rev. 2016, 5, 74. [Google Scholar] [CrossRef]
- The World Bank. High Income Indicators. 2020. Available online: https://data.worldbank.org/income-level/high-income?view=chart (accessed on 9 April 2020).
- Pawson, R. Digging for Nuggets: How ‘Bad’ Research Can Yield ‘Good’ Evidence. Int. J. Soc. Res. Methodol. Theory Pract. 2006, 9, 127–142. [Google Scholar] [CrossRef]
- Price, T.; Wong, G.; Withers, L.; Wanner, A.; Cleland, J.; Gale, T.; Prescott-Clements, L.; Archer, J.; Bryce, M.; Brennan, N. Optimising the Delivery of Remediation Programmes for Doctors: A Realist Review. Med. Educ. 2021, 55, 995–1010. [Google Scholar] [CrossRef]
- McLeroy, K.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Microsoft Corporation. Microsoft Excel. 2019. Available online: https://office.microsoft.com/excel (accessed on 31 May 2022).
- Pawson, R.; Tilley, N. Realistic Evaluation; SAGE Publications Inc.: London, UK, 1997; ISBN 9780761950097. [Google Scholar]
- Buttazzoni, A.; Coen, S.; Gilliland, J. Supporting Active School Travel: A Qualitative Analysis of Implementing a Regional Safe Routes to School Program. Soc. Sci. Med. 2018, 212, 181–190. [Google Scholar] [CrossRef]
- Atteberry, H.; Dowdy, D.; Oluyomi, A.; Nichols, D.; Ory, M.; Hoelscher, D. A Contextual Look at Safe Routes to School Implementation in Texas. Environ. Behav. 2016, 48, 192–209. [Google Scholar] [CrossRef]
- Crawford, S.; Garrard, J. A Combined Impact-Process Evaluation of a Program Promoting Active Transport to School: Understanding the Factors that Shaped Program Effectiveness. J. Environ. Public Health 2013, 2013, 816961. [Google Scholar] [CrossRef]
- McDonald, N.; Steiner, R.; Lee, C.; Rhoulac Smith, T.; Zhu, X.; Yang, Y. Impact of the Safe Routes to School Program on Walking and Bicycling. J. Am. Plan. Assoc. 2014, 80, 153–167. [Google Scholar] [CrossRef]
- McDonald, N.; Yang, Y.; Abbott, S.; Bullock, A. Impact of the Safe Routes to School Program on Walking and Biking: Eugene, Oregon Study. Transp. Policy 2013, 29, 243–248. [Google Scholar] [CrossRef]
- Mammen, G.; Stone, M.; Buliung, R.; Faulkner, G. “Putting School Travel on the Map”: Facilitators and Barriers to Implementing School Travel Planning in Canada. J. Transp. Health 2015, 2, 318–326. [Google Scholar] [CrossRef]
- Stewart, O.; Moudon, A.; Claybrooke, C. Multistate Evaluation of Safe Routes to School Programs. Am. J. Health Promot. 2014, 28, 89–96. [Google Scholar] [CrossRef]
- Hinckson, E. Perceived Challenges and Facilitators of Active Travel Following Implementation of the School Travel-Plan Programme in New Zealand Children and Adolescents. J. Transp. Health 2016, 3, 321–325. [Google Scholar] [CrossRef]
- Savolainen, E.; Rutberg, S.; Backman, Y.; Lindqvist, A. Long-Term Perspectives of a School-Based Intervention to Promote Active School Transportation. Int. J. Environ. Res. Public Health 2020, 17, 5006. [Google Scholar] [CrossRef]
- Teller, K.; Abbey-Lambertz, M.; Sharma, N.; Waite, A.; Ickes, S.; Mendoza, J. Parent Perceptions on a Walking School Bus Program among Low-Income Families: A Qualitative Study. J. Phys. Act. Health 2019, 16, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Nikitas, A.; Wang, J.; Knamiller, C. Exploring Parental Perceptions about School Travel and Walking School Buses: A Thematic Analysis Approach. Transp. Res. Part A Policy Pract. 2019, 124, 468–487. [Google Scholar] [CrossRef]
- Race, D.; Sims-Gould, J.; Lee, N.; Frazer, A.; Voss, C.; Naylor, P.; McKay, H. Urban and Suburban Children’s Experiences with School Travel—A Case Study. J. Transp. Health 2017, 4, 305–315. [Google Scholar] [CrossRef]
- Scharoun Benson, S.M.; Bruner, B.; Mayer, A. Encouraging Active Transportation to School: Lessons Learned from Implementing a Walking School Bus Program in Northeastern Ontario. J. Transp. Health 2020, 19, 100914. [Google Scholar] [CrossRef]
- Chaufan, C.; Yeh, J.; Fox, P. The Safe Routes to School Program in California: An Update. Am. J. Public Health 2012, 102, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.; Bennetts, S.; Hackworth, N.; Green, J.; Graesser, H.; Cooklin, A.; Matthews, J.; Strazdins, L.; Zubrick, S.; D’Esposito, F.; et al. Worries, ‘Weirdos’, Neighborhoods and Knowing People: A Qualitative Study with Children and Parents Regarding Children’s Independent Mobility. Health Place 2017, 45, 131–139. [Google Scholar] [CrossRef]
- Zhou, H.; Yang, J.; Hsu, P.; Chen, S. Factors Affecting Students’ Walking/Biking Rates: Initial Findings from a Safe Route to School Survey in Florida. J. Transp. Saf. Secur. 2010, 2, 14–27. [Google Scholar] [CrossRef]
- Forsberg, H.; Rutberg, S.; Mikaelsson, K.; Lindqvist, A. It’s about Being the Good Parent: Exploring Attitudes and Beliefs Towards Active School Transportation. Int. J. Circumpolar. Health 2020, 79, 1798113. [Google Scholar] [CrossRef] [PubMed]
- Florida Department of Health. Walking School Bus Initiative Final Evaluation Report. 2012. Available online: http://cfgis.org/hostedcfgis/srtsweb/Documents/ResourceDocuments/CPPWWalkSchoolBusFinalEvalReport.pdf (accessed on 7 April 2020).
- Ginja, S.; Arnott, B.; Araujo-Soares, V.; Namdeo, A.; McColl, E. Process Evaluation of a Pilot Study to Test the Feasibility of an Incentive Scheme to Increase Active Travel to School. J. Transp. Health 2019, 15, 100663. [Google Scholar] [CrossRef]
- Donnellan, N.; Egli, V.; Smith, M. ‘I’d Paint Rainbows and Unicorns on it’: Understanding Children’s School Travel Behaviours and the Impact of a New Shared Path. J. Transp. Health 2020, 17, 100838. [Google Scholar] [CrossRef]
- Rutberg, S.; Lindqvist, A. Children’s Motivation Overcame Parental Hesitation: Active School Transportation in Sweden. Health Promot. Int. 2019, 34, 1149–1156. [Google Scholar] [CrossRef]
- Rutberg, S.; Lindqvist, A. Active School Transportation is an Investment in School Health. Health Behav. Policy Rev. 2018, 5, 88–97. [Google Scholar] [CrossRef]
- Lindqvist, A.; Löf, M.; Ek, A.; Rutberg, S. Active School Transportation in Winter Conditions: Biking Together is Warmer. Int. J. Environ. Res. Public Health 2019, 16, 234. [Google Scholar] [CrossRef] [PubMed]
- Ahern, S.; Arnott, B.; Chatterton, T.; de Nazelle, A.; Kellar, I.; McEachan, R. Understanding Parents’ School Travel Choices: A Qualitative Study Using the Theoretical Domains Framework. J. Transp. Health 2017, 4, 278–293. [Google Scholar] [CrossRef]
- Ahlport, K.; Linnan, L.; Vaughn, A.; Evenson, K.; Ward, D. Barriers to and Facilitators of Walking and Bicycling to School: Formative Results from the Non-Motorized Travel Study. Health Educ. Behav. 2006, 35, 221–244. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, G.; Richichi, V.; Buliung, R.; Fusco, C.; Moola, F. What’s “Quickest and Easiest?”: Parental Decision Making about School Trip Mode. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 62. [Google Scholar] [CrossRef]
- Francis, J.; Martin, K.; Wood, L.; Foster, S. ‘I’ll Be Driving You to School for the Rest of Your Life’: A Qualitative Study of Parents’ Fear of Stranger Danger. J. Environ. Psychol. 2017, 53, 112–120. [Google Scholar] [CrossRef]
- Greves, H.; Lozano, P.; Liu, L.; Busby, K.; Cole, J.; Johnston, B. Immigrant Families’ Perceptions on Walking to School and School Breakfast: A Focus Group Study. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 64. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.; Brown, A. A Qualitative Study of ‘Fear’ as a Regulator of Children’s Independent Physical Activity in the Suburbs. Health Place 2013, 24, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Thompson, J.; Page, A.; Brockman, R.; Cartwright, K.; Fox, K. Licence to be Active: Parental Concerns and 10–11-Year-Old Children’s Ability to be Independently Physically Active. J. Public Health 2009, 31, 472–477. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Dierenfield, L.; Alexander, D.A.; Prose, M.; Peterson, A.C. Hawai’i’s Opportunity for Active Living Advancement (HO’ĀLA): Addressing Childhood Obesity through Safe Routes to School. Hawaii Med. J. 2011, 70, 21–26. [Google Scholar] [PubMed]
- Henderson, S.; Tanner, R.; Klanderman, N.; Mattera, A.; Webb, L.; Steward, J. Safe Routes to School: A Public Health Practice Success Story—Atlanta, 2008–2010. J. Phys. Act. Health 2013, 10, 141–142. [Google Scholar] [CrossRef]
- Hoelscher, D.; Ory, M.; Dowdy, D.; Miao, J.; Atteberry, H.; Nichols, D.; Evans, A.; Menendez, T.; Lee, C.; Wang, S. Effects of Funding Allocation for Safe Routes to School Programs on Active Commuting to School and Related Behavioral, Knowledge, and Psychosocial Outcomes: Results from the Texas Childhood Obesity Prevention Policy Evaluation (T-COPPE) Study. Environ. Behav. 2016, 48, 210–229. [Google Scholar] [CrossRef]
- Delaware Center for Transportation. Safe Routes to School Mode Share Analysis. 2011. Available online: https://cpb-us-w2.wpmucdn.com/sites.udel.edu/dist/1/1139/files/2013/10/Rpt.-219-Safe-Routes-to-School-1vjhbnf.pdf (accessed on 7 April 2020).
- Mineta Transportation Institute. Measuring Success for Safe Routes to School Programs. 2020. Available online: https://transweb.sjsu.edu/mctm/research/utc/Measuring-Success-Safe-Routes-School-Programs (accessed on 7 April 2020).
- National Center for Safe Routes to School. Shifting Modes: A Comparative Analysis of Safe Routes to School Program Elements and Travel Mode Outcomes. 2012. Available online: https://www.saferoutespartnership.org/resources/evaluation-report/shifting-modes (accessed on 7 April 2020).
- Oregon Transportation Research and Education Consortium. Evaluation of Safe Routes to School Programs: Qualitative and Quantitative Analysis of Parental Decision-Making. 2011. Available online: https://pdxscholar.library.pdx.edu/cgi/viewcontent.cgi?article=1056&context=trec_reports (accessed on 7 April 2020).
- Safe Routes to School National Partnership. Taking Back the Streets and Sidewalks: How Safe Routes to School and Community Safety Initiatives Can Overcome Violence and Crime. 2015. Available online: https://www.saferoutespartnership.org/sites/default/files/resource_files/taking-back-the-streets-and-sidewalks.pdf (accessed on 7 April 2020).
- Safe Transportation Research and Education Center. Safe Routes to School Local School Project: A Health Evaluation at 10 Low-Income Schools. 2010. Available online: http://escholarship.org/uc/item/37m6x95t?query=safetrec%5Cnhttp://trid.trb.org/view/1083715 (accessed on 7 April 2020).
- Hawley, G.; Witten, K.; Hosking, J.; Mackie, H.; Smith, M. The Journey to Learn: Perspectives on Active School Travel from Exemplar Schools in New Zealand. J. Transp. Health 2019, 14, 100600. [Google Scholar] [CrossRef]
- Sweeney, S.; Von Hagen, L. Stranger Danger, Cell Phones, Traffic, and Active Travel to and from Schools: Perceptions of Parents and Children. Transp. Res. Rec. 2016, 2582, 1–7. [Google Scholar] [CrossRef]
- Clark, E.; Dumas, A. Children’s Active Outdoor Play: ‘Good’ Mothering and the Organisation of Children’s Free Time. Sociol. Health Illn. 2020, 42, 1229–1242. [Google Scholar] [CrossRef]
- McDonald, N.; Aalborg, A. Why Parents Drive Children to School: Implications for Safe Routes to School Programs. J. Am. Plan. Assoc. 2009, 75, 331–342. [Google Scholar] [CrossRef]
- Buckley, A.; Lowry, M.; Brown, H.; Barton, B. Evaluating Safe Routes to School Events that Designate Days for Walking and Bicycling. Transp. Policy 2013, 30, 294–300. [Google Scholar] [CrossRef]
- Zuniga, K. From Barrier Elimination to Barrier Negotiation: A Qualitative Study of Parents’ Attitudes about Active Travel for Elementary School Trips. Transp. Policy 2012, 20, 75–81. [Google Scholar] [CrossRef]
- Pont, K.; Ziviani, J.; Wadley, D.; Abbott, R. The Model of Children’s Active Travel (M-CAT): A Conceptual Framework for Examining Factors Influencing Children’s Active Travel. Aust. Occup. Ther. J. 2010, 58, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Funnell, S.C.; Rodgers, P. Purposeful Program Theory: Effective Use of Theories of Change and Logic Models; Jossey-Bass: San Francisco, CA, USA, 2011; ISBN 978-0-470-47857-8. [Google Scholar]
- Jacob, V.; Chattopadhyay, S.K.; Reynolds, J.A.; Hopkins, D.P.; Morgan, J.A.; Brown, D.R.; Kochtitzky, C.S.; Cuellar, A.E.; Kumanyika, S.K. Economics of Interventions to Increase Active Travel to School: A Community Guide Systematic Review. Am. J. Prev. Med. 2021, 60, e27–e40. [Google Scholar] [CrossRef]
- Community Preventive Service Task Force. Physical Activity: Interventions to Increase Active Travel to School. 2018. Available online: https://www.thecommunityguide.org/findings/physical-activity-interventions-increase-active-travel-school (accessed on 26 June 2022).
- Burke, J.G.; O’Campo, P.; Peak, G.L.; Gielen, A.C.; McDonnell, K.A.; Trochim, W.M.K. An Introduction to Concept Mapping as a Participatory Public Health Research Method. Qual. Health Res. 2005, 15, 1392–1410. [Google Scholar] [CrossRef] [PubMed]
- Sunshine Coast Council. RideScore Active Schools. 2022. Available online: https://ridescore.org.au/ (accessed on 4 May 2022).

{kind=link}
{kind=link}
{kind=link}
| Database Name: Scopus | |||
| Date of Search: 26 March 2020 | |||
| Field Codes: Title, Abstract, and Keywords (TITLE-ABS-KEY) | |||
| Search # | Concept | Search Terms | No. of Results |
| #1 | Active Travel | Walking OR Cycling OR Bicycling OR “Active Transport*” OR “Active School Transport*” OR “Active School Travel” OR “Active* Travel*” OR Commut* OR “Independent* Mobil*” OR “Independent* Travel*” OR “Independent Licence*” | 515,402 |
| #2 | Intervention | “Safe Routes to School” OR “Safe Routes” OR “SRTS” OR “SR2S” | 2091 |
| #3 | Population | Child* OR “School Child*” OR “Elementary School*” OR “Primary School*” OR Boys OR Girls OR Youth* | 3,576,701 |
| #4 | #1 AND #2 AND #3 | 121 | |
| Characteristics | n | % |
|---|---|---|
| Country | ||
| United States | 23 | 51.1 |
| Canada | 6 | 13.3 |
| Sweden | 5 | 11.1 |
| Australia | 4 | 8.9 |
| United Kingdom | 4 | 8.9 |
| New Zealand | 3 | 6.7 |
| Document Type | ||
| Peer reviewed research articles | 38 | 84.4 |
| Grey literature reports | 6 | 13.3 |
| Commentary | 1 | 2.2 |
| Research Methodology | ||
| Qualitative | 25 | 55.6 |
| Mixed method | 10 | 22.2 |
| Quantitative | 9 | 20.0 |
| N/A | 1 | 2.2 |
| Intervention type | ||
| SR2S only | 18 | 40.0 |
| Walking school bus | 4 | 8.9 |
| SR2S + other | 2 | 4.4 |
| Gamification | 2 | 4.4 |
| Incentives | 1 | 2.2 |
| School travel plan | 1 | 2.2 |
| Standalone environmental infrastructure | 1 | 2.2 |
| Non-intervention | 16 | 35.6 |
| Partial Program Theory 1: Implementor/Implementation | Supporting References | |
|---|---|---|
| School Reliance | ||
| CMOC 1—Overreliance on Facilitator/Reliance on Internal Champion | Schools that had an uncommitted internal program champion/facilitator (C), management unsupportive of promoting AST (C), and/or low readiness to support AST initiatives (C), became complacent because they developed an overreliance on the uncommitted program champion/facilitator for intervention implementation (M), which led to low implementation fidelity (O). | [37,38,39,40,41,42,43] |
| School Priority | ||
| CMOC 2—Perceived Priority Relative to Support | Schools that had a management unsupportive of AST (C), low readiness to support AST initiatives (C), and/or competing priorities (C), perceived AST interventions as ‘add on’ initiatives and assigned resources to higher priority initiatives (M), and the staff responsible for implementation of low priority interventions became overwhelmed because they were not given the time or support to promote AST as well as meeting the demand from other priorities (M), which led to low implementation fidelity (O). | [37,38,39,40,41,42,43] |
| Partial Program Theory 1: Child | Supporting References | |
| Child Fun | ||
| CMOC 3—Socialising | Children that had friends or an older sibling to walk to school with (C), perceived walking to school as being fun because they could socialise on the way (M), which promoted children’s motivation to engage in AST (O). | [40,43,44,45,46,47,48,49,50,51,52,53,54,55,56] |
| CMOC 4—Engaging with Nature | Children that had access to open footpaths located away from main roads (C), and/or the presence of nature aspects on the route to school (C), perceived walking to school as being fun because they could engage with nature (M), which promoted children’s motivation to engage in AST (O). | [47,53,56] |
| CMOC 5—Showing Off | Children that lacked motivation to actively travel (C), and/or were competitive in nature (C), perceived walking to school as fun because they could track and show off their travel behaviour to friends (M), which promoted children’s motivation to engage in AST (O). | [45,57,58,59] |
| Child Pride | ||
| CMOC 6—Pride | Children with low participation in extracurricular activities (C), and/or social or academic difficulties/issues at school (C), felt a sense of pride for their involvement and having their efforts acknowledged (M), which promoted children’s motivation to engage in AST (O). | [45,57,58,59] |
| Partial Program Theory 3: Parent | Supporting References | |
| Perceived Safety | ||
| CMOC 7—Traffic Safety | In neighbourhoods that had high-speed and heavy traffic roads (C), that lacked supporting infrastructure and/or maintenance (C), parents perceived AST to be unsafe for their children because of the risk that they might get injured (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [43,46,47,48,50,51,52,53,54,56,57,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76] |
| CMOC 8—Stranger Danger | When children had access to open footpaths located away from main roads (C), that had low community activity (C), or lived in a neighbourhood with high levels of crime (C), parents perceived AST to be unsafe for their children because of the risk of abduction (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [46,48,51,52,53,56,57,60,62,63,65,66,73,74,77,78,79] |
| CMOC 9—Bullying | Children that walked to school alone or in small groups (C), with the presence of older/high school children along the route (C), made parents perceive AST to be unsafe because of the risk of their child being bullied by the older children (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [51,56,61,64,66,70,73,74,76] |
| CMOC 10—Safety in Numbers | When children had friends or older siblings to walk to school with (C), on a route that had high community activity (C), parents perceived AST to be safe for their children because friends, siblings, and/or members of the community provided informal supervision (M), positively influencing parental decision making (O), which promoted children’s engagement in AST (O). | [45,51,52,53,61,62,63,65,73,77,78] |
| Distrust | ||
| CMOC 11—Community/Adults | Parents that were new to a neighbourhood (C), lived in a neighbourhood of low socioeconomic status and/or high crime (C), belonged to a minority group (C), and/or lived in a community that lacked social cohesion (C), were less inclined to trust members of their community to be around their children (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [46,51,56,63,64,65,66,74,75,78] |
| CMOC 12—Child Behaviour | When children had friends or older siblings to walk to school with (C), and these children were prone to misbehaving (C), parents were less inclined to trust their child/child’s friend to be well behaved (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [46,47,51,53,66] |
| Convenience | ||
| CMOC 13—Trip Chaining | Working parents that had limited time flexibility in the morning (C), and multiple children that attend different schools (C), perceived passive travel to be more convenient because they could trip chain and go straight to work (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [46,47,48,50,52,53,56,57,60,62,64,65,70,71,73,75,77,79,80,81] |
| Perceived Capabilities | ||
| CMOC 14—Physical | For parents of young children (C), that had to walk through a neighbourhood with hilly topography (C), lived a far distance from school (C), and/or were required to carry a heavy backpack (C), perceived their children to not have the physical capabilities to walk to school (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [40,43,47,49,61,64,67,79,81] |
| CMOC 15—Road & Traffic | In neighbourhoods that had high-speed and heavy traffic roads (C), and/or lacked supporting infrastructure/maintenance (C), parents perceived their children to not have the skill or knowledge capabilities to actively travel safely (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [46,47,51,56,57,60,61,62,65] |
| Reassurance | ||
| CMOC 16—Reassurance | Working parents that had limited time flexibility in the morning (C), perceived their neighbourhood to be unsafe (C), and/or their child’s school did not actively alert parents if their child failed to arrive (C), lacked the reassurance to let their child actively travel because they would not know if they have arrived at school safely (M), negatively influencing parental decision making (O), which detracted from children’s engagement in AST (O). | [46,49,53,57,61,65,77] |
| Corresponding CMOC | Intervention Strategy Recommendations |
|---|---|
| CMOC 3 |
|
| CMOC 4 |
|
| CMOC 7 |
|
| CMOC 8 |
|
| CMOC 9 |
|
| CMOC 11 |
|
| CMOC 13 |
|
| CMOC 16 |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasey, T.V.; Carroll, S.J.; Daniel, M.; Cargo, M. Changing Primary School Children’s Engagement in Active School Travel Using Safe Routes to School Interventions: A Rapid Realist Review. Int. J. Environ. Res. Public Health 2022, 19, 9976. https://doi.org/10.3390/ijerph19169976
Vasey TV, Carroll SJ, Daniel M, Cargo M. Changing Primary School Children’s Engagement in Active School Travel Using Safe Routes to School Interventions: A Rapid Realist Review. International Journal of Environmental Research and Public Health. 2022; 19(16):9976. https://doi.org/10.3390/ijerph19169976
Chicago/Turabian StyleVasey, Thomas V., Suzanne J. Carroll, Mark Daniel, and Margaret Cargo. 2022. "Changing Primary School Children’s Engagement in Active School Travel Using Safe Routes to School Interventions: A Rapid Realist Review" International Journal of Environmental Research and Public Health 19, no. 16: 9976. https://doi.org/10.3390/ijerph19169976
APA StyleVasey, T. V., Carroll, S. J., Daniel, M., & Cargo, M. (2022). Changing Primary School Children’s Engagement in Active School Travel Using Safe Routes to School Interventions: A Rapid Realist Review. International Journal of Environmental Research and Public Health, 19(16), 9976. https://doi.org/10.3390/ijerph19169976