
Exercise to Improve Postural Stability in Older Adults with Alzheimer’s Disease: A Systematic Review of Randomized Control Trials



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Selection of Studies
2.4. Methodological Quality Assessment
2.5. Data Extraction and Synthesis
3. Results
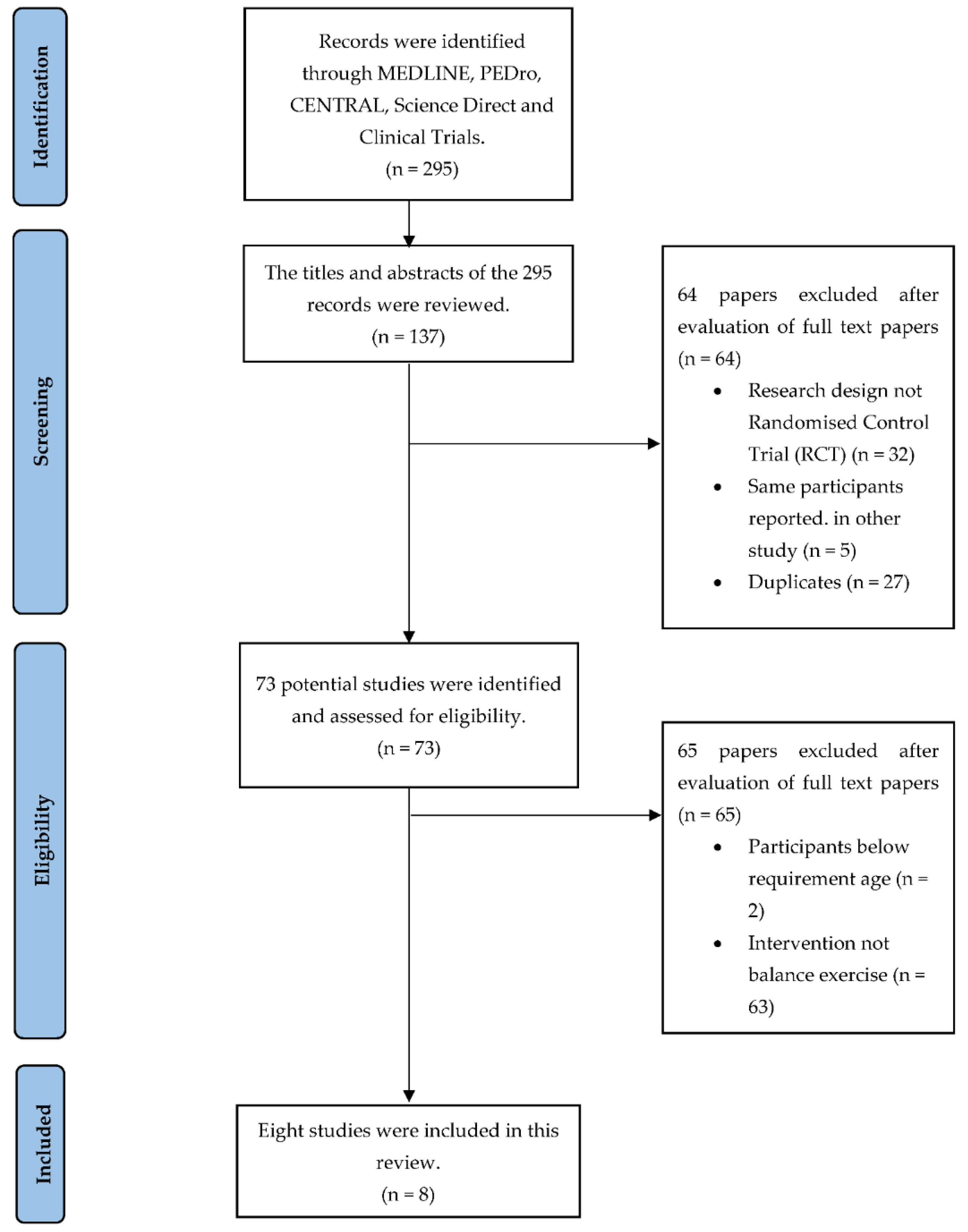
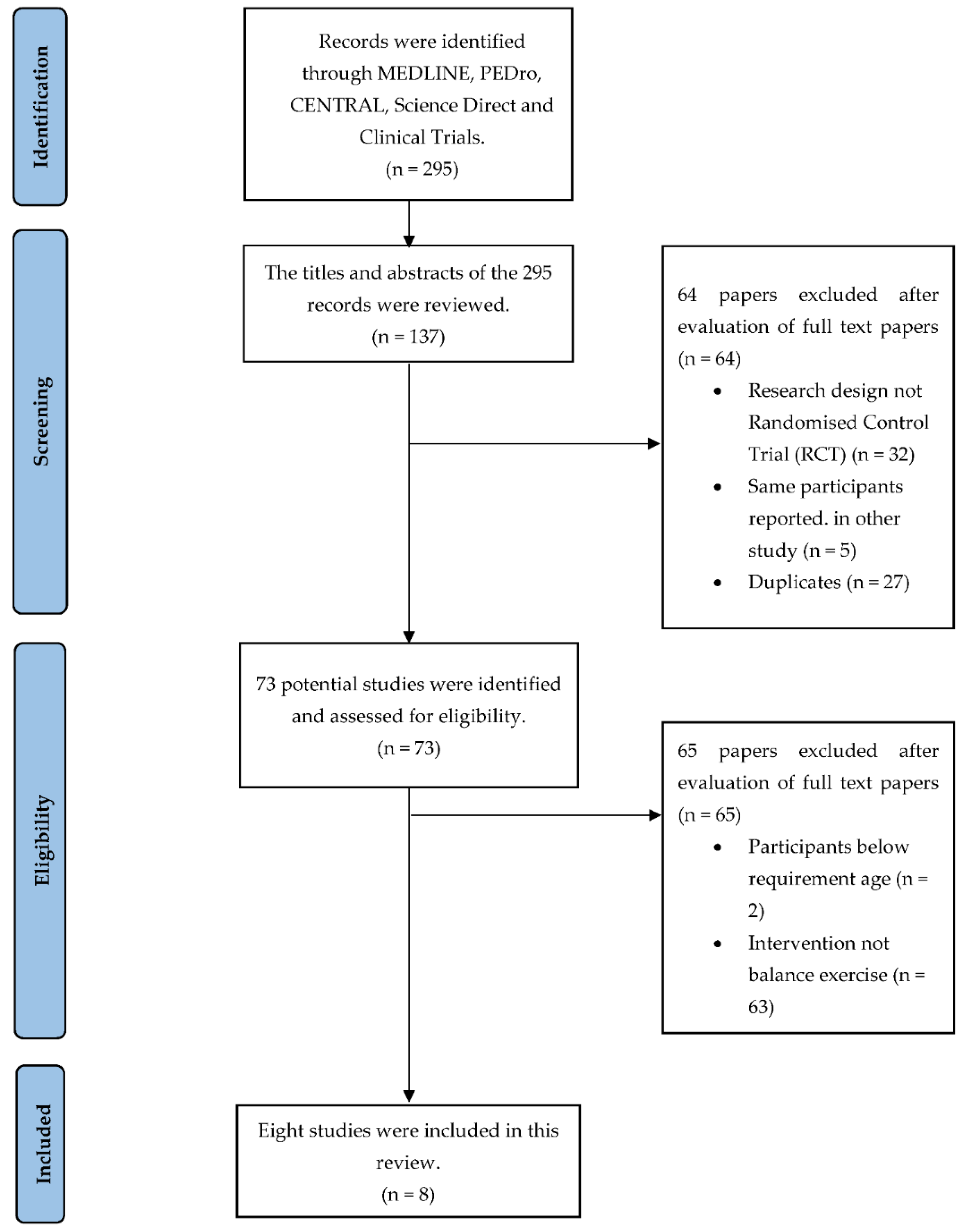
3.1. Search Results
3.2. Methodological Quality of Included Study
3.3. Study Characteristics
3.4. Outcome Measures to Evaluate Cognitive Function
3.5. Outcome Measures to Evaluate Postural Instability
3.6. Intervention for Older Adults with AD
4. Discussion
Limitation of the Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Posner, H.; Curiel, R.; Edgar, C.; Hendrix, S.; Liu, E.; Loewenstein, D.A.; Morrison, G.; Shinobu, L.; Wesnes, K.; Harvey, P.D. Outcomes Assessment in Clinical Trials of Alzheimer’s Disease and its Precursors: Readying for Short-term and Long-term Clinical Trial Needs. Innov. Clin. Neurosci. 2017, 14, 22–29. [Google Scholar] [PubMed]
- Reitz, C.; Brayne, C.; Mayeux, R. Epidemiology of Alzheimer disease. Nat. Rev. Neurol. 2011, 7, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Ali, G.-C.; Guerchet, M.; Prince, M.; Prina, M.; Wu, Y.-T. World Alzheimer Report 2015. Alzheimer’s Dis. Int. 2015. Available online: https://www.alzint.org/resource/world-alzheimer-report-2015/ (accessed on 20 November 2021).
- Puente-González, A.S.; Sánchez-González, F.; Hernández-Xumet, J.E.; Sánchez-Sánchez, M.C.; Barbero-Iglesias, F.J.; Méndez-Sánchez, R. Short and medium-term effects of a multicomponent physical exercise program with a Mediterranean diet on bone mineral density, gait, balance, and fall risk for patients with Alzheimer disease: Randomized controlled clinical trial study protocol. Medicine 2020, 99, e22385. [Google Scholar] [CrossRef]
- Sköldunger, A.; Johnell, K.; Winblad, B.; Wimo, A. Mortality and treatment costs have a great impact on the cost-effectiveness of disease modifying treatment in Alzheimer’s disease—A simulation study. Curr. Alzheimer Res. 2013, 10, 207–216. [Google Scholar] [CrossRef]
- Binns, E.; Kerse, N.; Peri, K.; Cheung, G.; Taylor, D. Combining cognitive stimulation therapy and fall prevention exercise (CogEx) in older adults with mild to moderate dementia: A feasibility randomised controlled trial. Pilot Feasibility Stud. 2020, 6, 108. [Google Scholar] [CrossRef]
- Rivan, N.F.M.; Singh, D.K.A.; Shahar, S.; Wen, G.J.; Rajab, N.F.; Din, N.C.; Mahadzir, H.; Kamaruddin, M.Z.A. Cognitive frailty is a robust predictor of falls, injuries, and disability among community-dwelling older adults. BMC Geriatr. 2021, 21, 593. [Google Scholar] [CrossRef]
- Won, H.; Singh, D.K.A.; Din, N.C.; Badrasawi, M.; Manaf, Z.A.; Tan, S.T.; Tai, C.C.; Shahar, S. Relationship between physical performance and cognitive performance measures among community-dwelling older adults. Clin. Epidemiol. 2014, 6, 343–350. [Google Scholar]
- Heaw, Y.C.; Singh, D.K.A.; Tan, M.P.; Kumar, S. Bidirectional association between executive and physical functions among older adults: A systematic review. Australas. J. Ageing 2022, 41, 20–41. [Google Scholar] [CrossRef]
- Alexander, N.B.; Mollo, J.M.; Giordani, B.; Ashton-Miller, J.A.; Schultz, A.B.; Grunawalt, J.A.; Foster, N.L. Maintenance of balance, gait patterns, and obstacle clearance in Alzheimer’s disease. Neurology 1995, 45, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Toots, A.; Wiklund, R.; Littbrand, H.; Nordin, E.; Nordström, P.; Lundin-Olsson, L.; Gustafson, Y.; Rosendahl, E. The Effects of Exercise on Falls in Older People with Dementia Living in Nursing Homes: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2019, 20, 835–842. [Google Scholar] [CrossRef] [PubMed]
- de Souto Barreto, P.; Denormandie, P.; Lepage, B.; Armaingaud, D.; Rapp, T.; Chauvin, P.; Vellas, B.; Rolland, Y. Effects of a long-term exercise programme on functional ability in people with dementia living in nursing homes: Research protocol of the LEDEN study, a cluster randomised controlled trial. Contemp. Clin. Trials 2016, 47, 289–295. [Google Scholar] [CrossRef]
- Pinheiro, M.B.; Oliveira, J.; Bauman, A.; Fairhall, N.; Kwok, W.; Sherrington, C. Evidence on physical activity and osteoporosis prevention for people aged 65+ years: A systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Murukesu, R.R.; Singh, D.K.A.; Shahar, S.; Subramaniam, P. A Multi-Domain Intervention Protocol for the Potential Reversal of Cognitive Frailty: “WE-RISE” Randomized Controlled Trial. Front. Public Health 2020, 8, 471. [Google Scholar] [CrossRef]
- Murukesu, R.R.; Singh, D.K.A.; Shahar, S.; Subramaniam, P. Physical activity patterns, psychosocial well-being and coping strategies among older persons with cognitive frailty of the “we-rise” trial throughout the covid-19 movement control order. Clin. Interv. Aging 2021, 16, 415–429. [Google Scholar] [CrossRef]
- Hoffmann, K.; Sobol, N.A.; Frederiksen, K.S.; Beyer, N.; Vogel, A.; Vestergaard, K.; Brændgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; et al. Moderate-to-High Intensity Physical Exercise in Patients with Alzheimer’s Disease: A Randomized Controlled Trial. J. Alzheimer’s Dis. 2016, 50, 443–453. [Google Scholar] [CrossRef]
- Öhman, H.; Savikko, N.; Strandberg, T.; Kautiainen, H.; Raivio, M.; Laakkonen, M.L.; Tilvis, R.; Pitkälä, K.H. Effects of Exercise on Functional Performance and Fall Rate in Subjects with Mild or Advanced Alzheimer’s Disease: Secondary Analyses of a Randomized Controlled Study. Dement. Geriatr. Cogn. Disord. 2016, 41, 233–241. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Lamb, S.E.; Sheehan, B.; Atherton, N.; Nichols, V.; Collins, H.; Mistry, D.; Dosanjh, S.; Slowther, A.M.; Khan, I.; Petrou, S.; et al. DAPA Trial Investigators. Dementia And Physical Activity (DAPA) trial of moderate to high intensity exercise training for people with dementia: Randomised controlled trial. BMJ 2018, 361, k1675. [Google Scholar] [CrossRef]
- Pitkälä, K.H.; Pöysti, M.M.; Laakkonen, M.L.; Tilvis, R.S.; Savikko, N.; Kautiainen, H.; Strandberg, T.E. Effects of the Finnish Alzheimer disease exercise trial (FINALEX): A randomized controlled trial. JAMA Intern. Med. 2013, 173, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Roach, K.E.; Tappen, R.M.; Kirk-Sanchez, N.; Williams, C.L.; Loewenstein, D. A Randomized Controlled Trial of an Activity Specific Exercise Program for Individuals with Alzheimer Disease in Long-term Care Settings. J. Geriatr. Phys. Ther. 2011, 34, 50–56. [Google Scholar] [CrossRef]
- Santana-Sosa, E.; Barriopedro, M.I.; López-Mojares, L.M.; Pérez, M.; Lucia, A. Exercise training is beneficial for Alzheimer’s patients. Int. J. Sports Med. 2008, 29, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Pillard, F.; Klapouszczak, A.; Reynish, E.; Thomas, D.; Andrieu, S.; Rivière, D.; Vellas, B. Exercise program for nursing home residents with Alzheimer’s disease: A 1-year randomized, controlled trial. J. Am. Geriatr. Soc. 2007, 55, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Woodbridge, R.; Sullivan, M.P.; Harding, E.; Crutch, S.; Gilhooly, K.J.; Gilhooly, M.; McIntyre, A.; Wilson, L. Use of the physical environment to support everyday activities for people with dementia: A systematic review. Dementia 2018, 17, 533–572. [Google Scholar] [CrossRef]
- Mesbah, N.; Perry, M.; Hill, K.D.; Kaur, M.; Hale, L. Postural stability in older adults with alzheimer disease. Phys. Ther. 2017, 97, 290–309. [Google Scholar]
- Foster, P.P.; Rosenblatt, K.P.; Kuljiš, R.O. Exercise-induced cognitive plasticity, implications for mild cognitive impairment and Alzheimer’s disease. Front. Neurol. 2011, 2, 28. [Google Scholar] [CrossRef]
- Valenzuela, M.; Brayne, C.; Sachdev, P.; Wilcock, G. Fiona Matthews on Behalf of the Medical Research Council Cognitive Function and Ageing Study. Cognitive lifestyle and long-term risk of dementia and survival after diagnosis in a multicenter population-based cohort. Am. J. Epidemiol. 2011, 173, 1004–1012. [Google Scholar] [CrossRef]
- Cipryan, L.; Tschakert, G.; Hofmann, P. Acute and post-exercise physiological responses to high-intensity interval training in endurance and sprint athletes. J. Sports Sci. Med. 2017, 16, 219–229. [Google Scholar]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- McDermott, A.; Mernitz, H. Exercise and the Elderly: Guidelines and Practical Prescription Applications for the Clinician. J. Clin. Outcomes Manag. 2004, 11, 117–128. [Google Scholar]

{kind=link}
| Study | Random Allocation | Concealed Allocation | Groups Similar at Baseline | Participant Blinding | Therapist BLINDING | Assessor Blinding | <15% Dropouts | Intention-to-Treat Analysis | Between-Group Difference Reported | Point Estimate and Variability Reported | Total (0 to 10) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Binns et al. (2020) [7] | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 4 |
| Pitkälä et al. (2013) [21] | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Öhman et al. (2016) [18] | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 3 |
| Toots et al. (2019) [12] | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 7 |
| Lamb et al. (2018) [20] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Roach et al. (2011) [22] | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 4 |
| Santana-Sosa et al. (2008) [23] | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 4 |
| Rolland et al. (2007) [24] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Study | Design | Participants | Intervention (Type of Exercise) | Time, Frequency, Intensity | Outcome Measures |
|---|---|---|---|---|---|
| Binns et al. (2020) [7] | RCT | n = 23 Age (yr) = 71 (mean) Gender = 6 M, 17 F ADAS-Cog11 = 16.2 (SD 8.2) Set = long term care | Exp = CogEx (aerobic, balance and strengthening exercise) Con = CST | 1 h, 2x/week, 7 weeks Exp intensity: NR |
|
| Pitkälä et al. (2013) [21] | RCT | n = 210 Age (yr) = 77.7 (SD 5.4) Gender = 129 M, 81 F MMSE = 17.8 (SD 6.6) Set = community | Exp = Group 1: Home based exercise Group 2: Group based exercise (endurance, balance, strength training and brain training) | 1 h, 2x/week for 12 months Exp intensity: NR |
|
| Con = Community care (oral and written advice on nutrition and exercise) | |||||
| Öhman et al. (2016) [18] | RCT | n = 194 Age (yr) = 78 (SD 5.25) Gender = 119 M, 75 F MMSE = 22.9 (SD 3.6) Set = community | Exp = Group 1: Home based exercise. Group 2: Group based exercise (endurance, balance, and strength training) | 1 h, 2x/week, 12 months Exp intensity: NR |
|
| Con = no intervention | |||||
| Toots et al. (2019) [12] | RCT | n = 186 Age (yr) = 85.1 (SD 7.1) Gender = 141 M, 45 F MMSE = 14.9 (SD 3.5) Set = long term care | Exp = HIFE (lower limb strength, balance and mobility) Con = Interesting topic (local wildlife, seasons and holidays) | 8 to 12 repetitions 45 min, 2x/week, 12 months Exp intensity: moderate to high |
|
| Lamb et al. (2018) [20] | RCT | n = 494 Age (yr) = 78.4 (SD 7.6) Gender = 301 M, 193 F ADAS-Cog11 = 21.6 (SD 8.7) Set = community | Exp = aerobic and strength exercise Con = counseling, symptomatic treatment and advice on physical activity | 60−90 min, 2x/week in group), additional 1 h/week (at home), 12 months Exp intensity: progressive aerobic (25 min), strength (20 reps, 3 sets); both moderate to high intensity |
|
| Roach et al. (2011) [22] | RCT | n = 130 Age (yr) = 88.2 (SD 6.13) Gender = not stated MMSE = 10.2 (SD 7.6) Set = long term care | Exp = Group 1: aerobic, strength, flexibility, balance Group 2: aerobic group | 15−30 min, 5x/week, 4 months Exp intensity: aerobic (between 10 to 30 min); strength & balace (low to high intensity, 2−3 reps progressed to 7−9 reps) |
|
| Con = one-on-one conversation | |||||
| Santana-Sosa et al. (2008) [23] | RCT | n = 16 Age (yr) = 76.0 (SD 4.0) Gender = 6 male, 10 female MMSE = 20.45 (SD 4.0) Set = long term care | Exp = aerobic, flexibility, joint mobility exercise, resistance and balance/coordination training. Con = routine nursing/medical care. | 75 min, 3x/week, 3 months Exp intensity: aerobic (light-without breathlessness); stretching (gentle); resistance (3 sets, 15 reps, medium resistance band) |
|
| Rolland et al. (2007) [24] | RCT | n = 134 Age (yr) = 83.0 (SD 7.4) Gender = 33 male, 101 female MMSE = 8.8 (SD 6.6) Set = long term care | Exp = aerobic, strength, balance and flexibility exercise. Con = routine medical care | 60 min, 2x/week, 12 months Exp intensity: aerobic (light progressed to moderate breathlessness) |
|
| Study | Design | Target Group | Outcome Measures | Summary Findings |
|---|---|---|---|---|
| Binns et al. (2020) [7] | RCT | Age (yr) = 71 (mean) (n = 23) | Brief BESTest * |
|
| SPBB* |
| |||
| Pitkälä et al. (2013) [21] | RCT | Age (yr) = 77.7 (SD 5.4) (n = 210) | FIM * | 6 months
|
| SPPB |
| |||
| Öhman et al. (2016) [18] | RCT | Age (yr) = 78 (SD 5.25) (n = 194) | FIM * | 6 months
|
| Fall rate * |
| |||
| Toots et al. (2019) [12] | RCT | Age (yr) = 85.1 (SD 7.1) (n = 186) | BBS Fall rate | 6 months
|
| Lamb et al. (2018) [20] | RCT | Age (yr) = 78.4 (SD 7.6) (n = 494) | 6MWT * | 6 weeks:
|
| Fall rate | 12 month
| |||
| Roach et al. (2011) [22] | RCT | Age (yr) = 88.2 (SD 6.13) (n = 130) | 6MWT * | 6MWT mean scores of participants in:
|
| Santana-Sosa et al. (2008) [23] | RCT | Age (yr) = 76.0 (SD 4.0) (n = 16) | Tinetti Scale * |
|
| 8-foot up & go test * |
| |||
| Rolland et al. (2007) [24] | RCT | Age (yr) = 83.0 (SD 7.4) (n = 134) | 6-m walking test * | Between group effect
|
| TUG |
| |||
| One-leg balance test |
| |||
| Whithin group effect was not reported for all measures |
| Study | The Experimental Group (Intervention) | Control Group (Intervention) |
|---|---|---|
| Binns et al. (2020) [7] | CogEx: Aerobic, progressive strength and balance exercises | CST; planning, executing, naming and organizing tasks of (physical games, sounds, childhood. Food, current affairs, faces and scenes, associated words, being creative, categorizing objects, orientation, using money, number games, word games, team quiz) |
| Pitkälä et al. (2013) [21] | Physical exercises: Aerobic, strengthening, balance and exercise for improving executive functioning | Oral and written advice on exercise and nutrition |
| Öhman et al. (2016) [18] | Physical exercises: Aerobic, strengthening, balance and dual-tasking exercise | Advice on exercise, nutrition and regular treatment in the healthcare system |
| Toots et al. (2019) [12] | Physical exercises: Lower limb strengthening, balance and mobility | Structured interesting activities, including holidays, wildlife and seasons |
| Lamb et al. (2018) [20] | Physical exercises: Aerobic and strengthening | Counselling, symptomatic treatment and advice on physical activity |
| Roach et al. (2011) [22] | Physical exercises: aerobic, strength, balance and flexibility exercises. | One-on-one conversation on participants’ topic of interest |
| Santana-Sosa et al. (2008) [23] | Physical exercises: aerobic, strength, balance and flexibility exercises. | Routine nursing/medical care |
| Rolland et al. (2007) [24] | Physical exercises: aerobic, strength, balance and flexibility exercises. | Routine medical care |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adzhar, M.A.; Manlapaz, D.; Singh, D.K.A.; Mesbah, N. Exercise to Improve Postural Stability in Older Adults with Alzheimer’s Disease: A Systematic Review of Randomized Control Trials. Int. J. Environ. Res. Public Health 2022, 19, 10350. https://doi.org/10.3390/ijerph191610350
Adzhar MA, Manlapaz D, Singh DKA, Mesbah N. Exercise to Improve Postural Stability in Older Adults with Alzheimer’s Disease: A Systematic Review of Randomized Control Trials. International Journal of Environmental Research and Public Health. 2022; 19(16):10350. https://doi.org/10.3390/ijerph191610350
Chicago/Turabian StyleAdzhar, Mohamad Asyraf, Donald Manlapaz, Devinder Kaur Ajit Singh, and Normala Mesbah. 2022. "Exercise to Improve Postural Stability in Older Adults with Alzheimer’s Disease: A Systematic Review of Randomized Control Trials" International Journal of Environmental Research and Public Health 19, no. 16: 10350. https://doi.org/10.3390/ijerph191610350
APA StyleAdzhar, M. A., Manlapaz, D., Singh, D. K. A., & Mesbah, N. (2022). Exercise to Improve Postural Stability in Older Adults with Alzheimer’s Disease: A Systematic Review of Randomized Control Trials. International Journal of Environmental Research and Public Health, 19(16), 10350. https://doi.org/10.3390/ijerph191610350