
Comparison of Secular Trends in Esophageal Cancer Mortality in China and Japan during 1990–2019: An Age-Period-Cohort Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
3.1. Trends in Esophageal Cancer Mortality
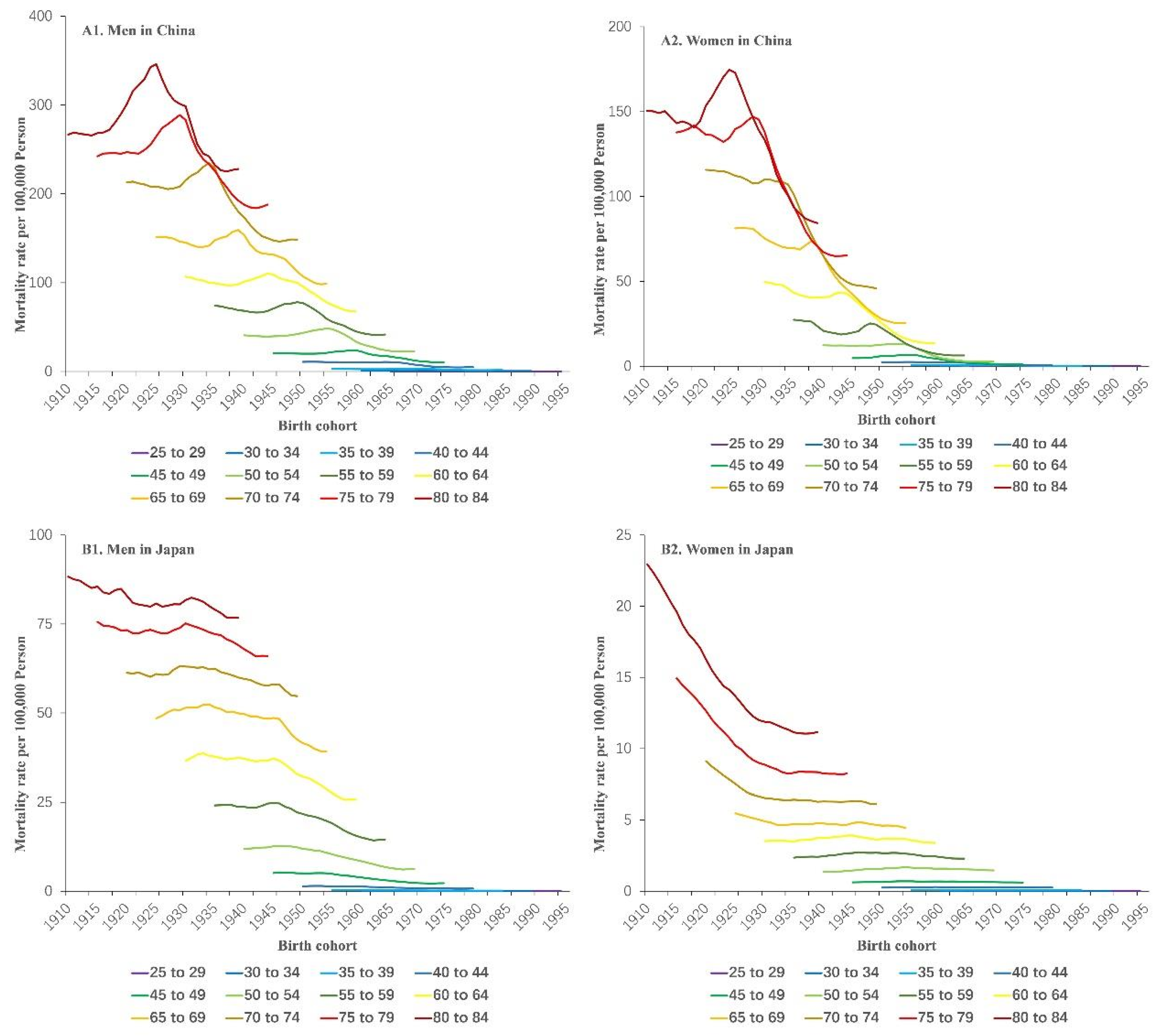
3.2. Trends in Age- and Cohort-Specific Esophageal Cancer Mortality
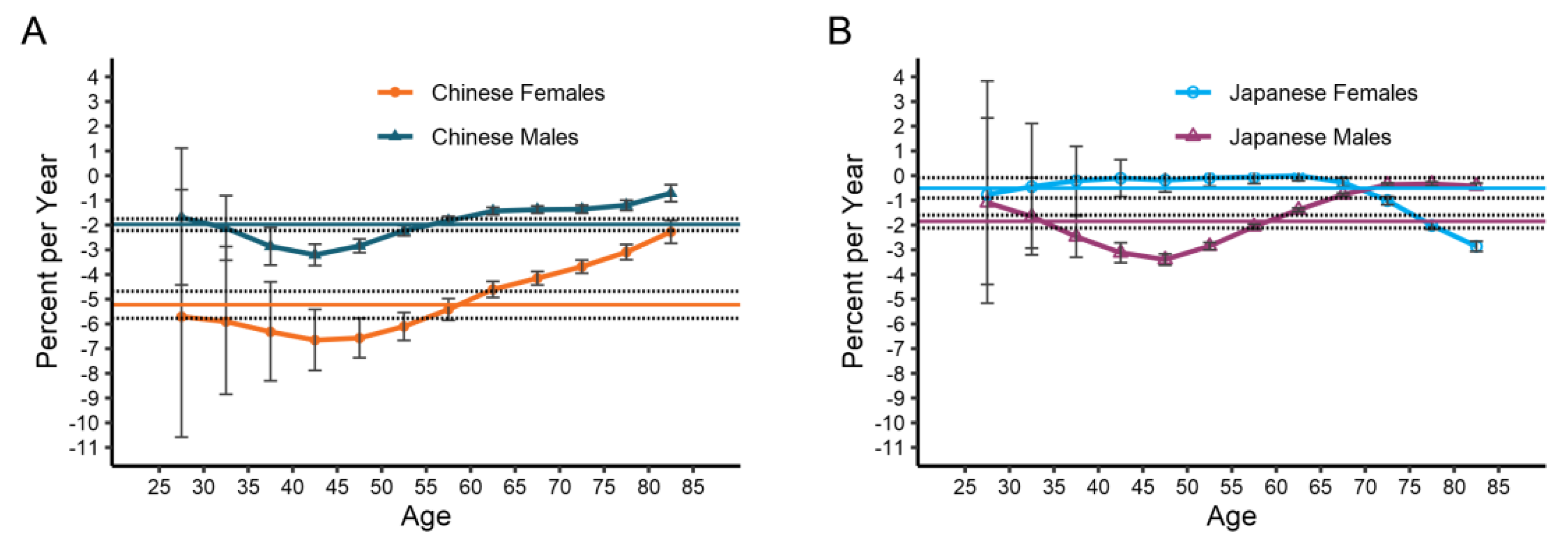
3.3. Net Drift and Local Drift in Different Age Groups
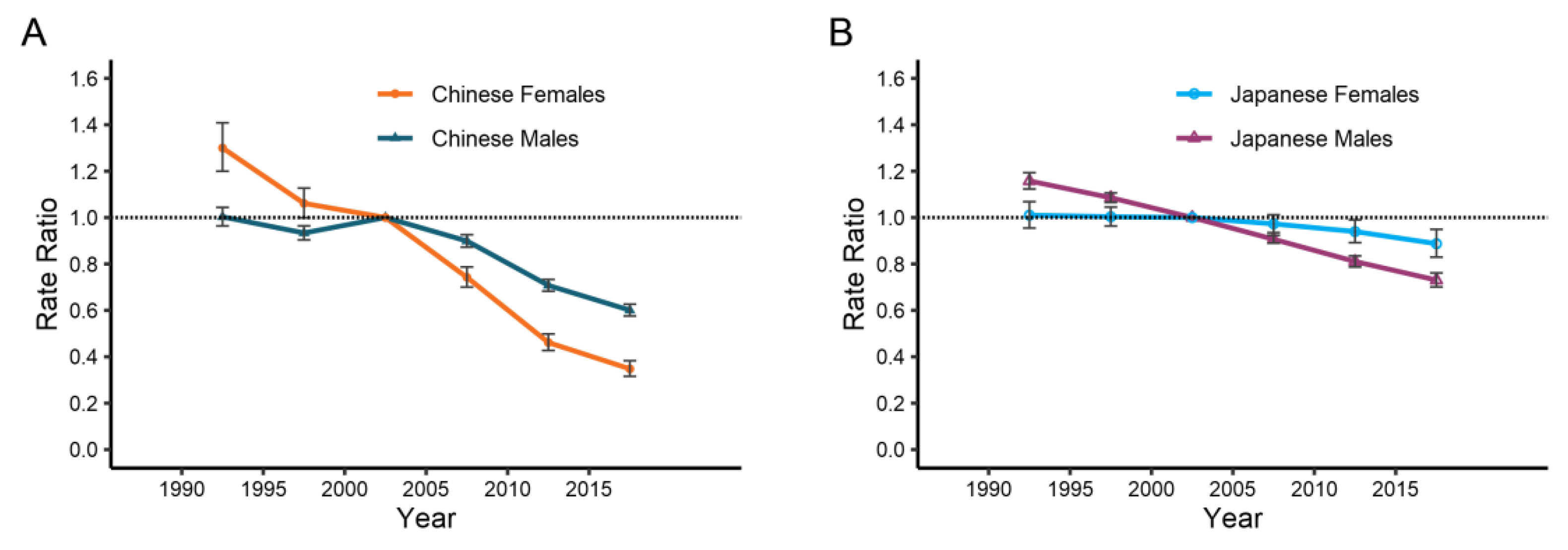
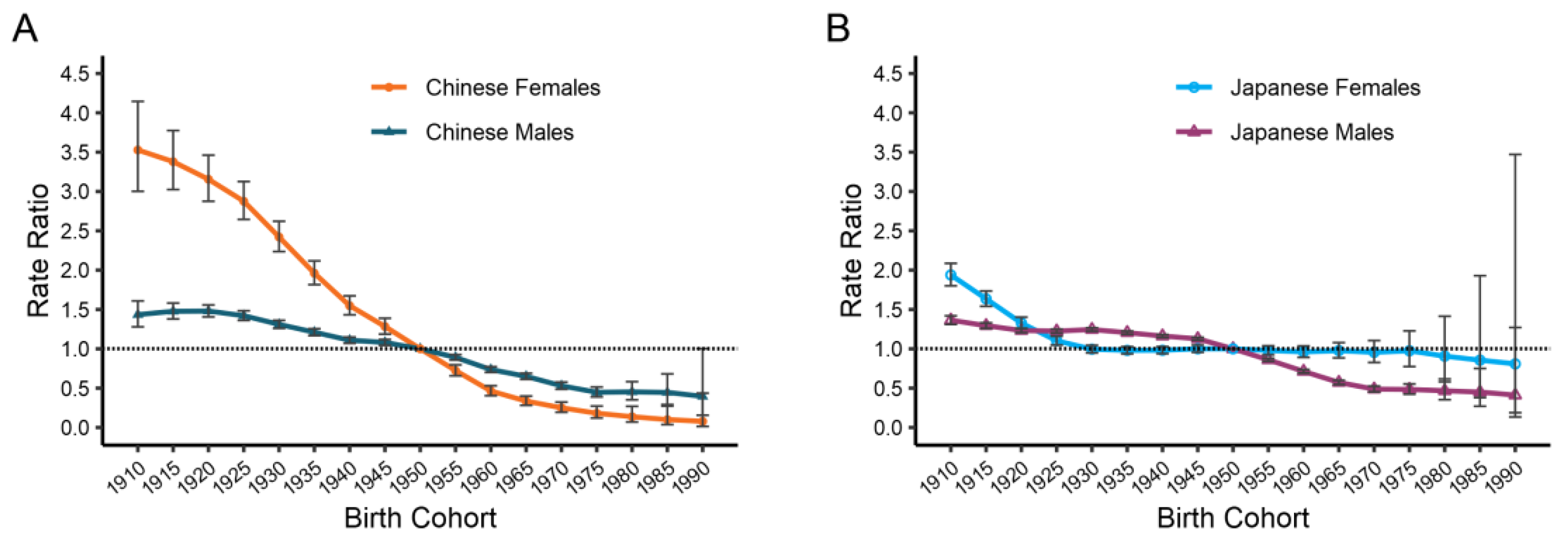
3.4. The Age, Period, and Cohort Effects on Esophageal Cancer Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Ferlay, J.; van Berge Henegouwen, M.I.; Soerjomataram, I. Global Burden of Oesophageal and Gastric Cancer by Histology and Subsite in 2018. Gut 2020, 69, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Kamangar, F.; Nasrollahzadeh, D.; Safiri, S.; Sepanlou, S.G.; Fitzmaurice, C.; Ikuta, K.S.; Bisignano, C.; Islami, F.; Roshandel, G.; Lim, S.S.; et al. The Global, Regional, and National Burden of Oesophageal Cancer and Its Attributable Risk Factors in 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 582–597. [Google Scholar] [CrossRef]
- Gao, X.; Wang, Z.; Kong, C.; Yang, F.; Wang, Y.; Tan, X. Trends of Esophageal Cancer Mortality in Rural China from 1989 to 2013: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2017, 14, 218. [Google Scholar] [CrossRef]
- Yang, S.; Lin, S.; Li, N.; Deng, Y.; Wang, M.; Xiang, D.; Xiang, G.; Wang, S.; Ye, X.; Zheng, Y.; et al. Burden, Trends, and Risk Factors of Esophageal Cancer in China from 1990 to 2017: An up-to-Date Overview and Comparison with Those in Japan and South Korea. J. Hematol. Oncol. 2020, 13, 146. [Google Scholar] [CrossRef]
- Wang, J.; Bai, Z.; Wang, Z.; Yu, C. Comparison of Secular Trends in Cervical Cancer Mortality in China and the United States: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2016, 13, 1148. [Google Scholar] [CrossRef]
- Xie, S.-H.; Chen, J.; Zhang, B.; Wang, F.; Li, S.-S.; Xie, C.-H.; Tse, L.-A.; Cheng, J.-Q. Time Trends and Age-Period-Cohort Analyses on Incidence Rates of Thyroid Cancer in Shanghai and Hong Kong. BMC Cancer 2014, 14, 975. [Google Scholar] [CrossRef]
- GBD 2019 Risk Factors Collaborators Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, Morbidity, and Risk Factors in China and Its Provinces, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar] [CrossRef]
- Nomura, S.; Sakamoto, H.; Glenn, S.; Tsugawa, Y.; Abe, S.K.; Rahman, M.M.; Brown, J.C.; Ezoe, S.; Fitzmaurice, C.; Inokuchi, T.; et al. Population Health and Regional Variations of Disease Burden in Japan, 1990-2015: A Systematic Subnational Analysis for the Global Burden of Disease Study 2015. Lancet 2017, 390, 1521–1538. [Google Scholar] [CrossRef]
- Rosenberg, P.S.; Check, D.P.; Anderson, W.F. A Web Tool for Age-Period-Cohort Analysis of Cancer Incidence and Mortality Rates. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Menon, S.; Trudgill, N. How Commonly Is Upper Gastrointestinal Cancer Missed at Endoscopy? A Meta-Analysis. Endosc. Int. Open 2014, 2, E46–E50. [Google Scholar] [CrossRef] [PubMed]
- Alsop, B.R.; Sharma, P. Esophageal Cancer. Gastroenterol. Clin. N. Am. 2016, 45, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Epidemiology of Esophageal Cancer. World J. Gastroenterol. 2013, 19, 5598. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Minamide, T.; Yano, T. Role of Photodynamic Therapy in the Treatment of Esophageal Cancer. Dig. Endosc. 2019, 31, 508–516. [Google Scholar] [CrossRef]
- di Pietro, M.; Canto, M.I.; Fitzgerald, R.C. Endoscopic Management of Early Adenocarcinoma and Squamous Cell Carcinoma of the Esophagus: Screening, Diagnosis, and Therapy. Gastroenterology 2018, 154, 421–436. [Google Scholar] [CrossRef]
- Wei, W.-Q.; Chen, Z.-F.; He, Y.-T.; Feng, H.; Hou, J.; Lin, D.-M.; Li, X.-Q.; Guo, C.-L.; Li, S.-S.; Wang, G.-Q.; et al. Long-Term Follow-Up of a Community Assignment, One-Time Endoscopic Screening Study of Esophageal Cancer in China. J. Clin. Oncol. 2015, 33, 1951–1957. [Google Scholar] [CrossRef]
- Zheng, X.; Mao, X.; Xu, K.; Lü, L.; Peng, X.; Wang, M.; Xu, G.; Hua, Z.; Wang, J.; Xue, H.; et al. Massive Endoscopic Screening for Esophageal and Gastric Cancers in a High-Risk Area of China. PLoS ONE 2015, 10, e0145097. [Google Scholar] [CrossRef]
- Nakatani, H. Population Aging in Japan: Policy Transformation, Sustainable Development Goals, Universal Health Coverage, and Social Determinates of Health. Glob. Health Med. 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Fang, E.F.; Xie, C.; Schenkel, J.A.; Wu, C.; Long, Q.; Cui, H.; Aman, Y.; Frank, J.; Liao, J.; Zou, H.; et al. A Research Agenda for Ageing in China in the 21st Century (2nd Edition): Focusing on Basic and Translational Research, Long-Term Care, Policy and Social Networks. Ageing Res. Rev. 2020, 64, 101174. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Liu, Z.; Mao, X.; Tong, X.; Zhang, T.; Suo, C.; Chen, X. Global Trends in the Incidence and Mortality of Esophageal Cancer from 1990 to 2017. Cancer Med. 2020, 9, 6875–6887. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Cao, M.; Li, H.; He, S.; Chen, W. China Cancer Burden and Trends in China: A Review and Comparison with Japan and South Korea. Chin. J. Cancer Res. 2020, 32, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Goss, P.E.; Strasser-Weippl, K.; Lee-Bychkovsky, B.L.; Fan, L.; Li, J.; Chavarri-Guerra, Y.; Liedke, P.E.R.; Pramesh, C.S.; Badovinac-Crnjevic, T.; Sheikine, Y.; et al. Challenges to Effective Cancer Control in China, India, and Russia. Lancet Oncol. 2014, 15, 489–538. [Google Scholar] [CrossRef]
- Yang, W.X.; Lu, S.X.; Liu, G.T.; Li, J. Etiological Prevention Trial for Esophageal Cancer among High-Risk Population in Linzhou City, China. China Cancer 2008, 17, 548–552. [Google Scholar]
- Liang, T.G. On the Meaning and Content of Health Care Investment in China’s Rural Areas under the Economic Crisis. J. Shandong Admin. Univ. 2009, 3, 72–74. [Google Scholar]
- Kanasi, E.; Ayilavarapu, S.; Jones, J. The Aging Population: Demographics and the Biology of Aging. Periodontology 2000 2016, 72, 13–18. [Google Scholar] [CrossRef]
- Lutz, W.; Sanderson, W.; Scherbov, S. The Coming Acceleration of Global Population Ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef]
- Li, S.; Chen, H.; Man, J.; Zhang, T.; Yin, X.; He, Q.; Yang, X.; Lu, M. Changing Trends in the Disease Burden of Esophageal Cancer in China from 1990 to 2017 and Its Predicted Level in 25 Years. Cancer Med. 2021, 10, 1889–1899. [Google Scholar] [CrossRef]
- Santos, J.D.; Meira, K.C.; Simões, T.C.; Guimarães, R.M.; Telles, M.W.P.; Borges, L.F.; de Assis, A.C.P.; das Vitorias Silva, M.; Barbosa, I.R.; de Souza Giusti, A.C.B.; et al. Inequalities in Esophageal Cancer Mortality in Brazil: Temporal Trends and Projections. PLoS ONE 2018, 13, e0193135. [Google Scholar] [CrossRef]
- Gupta, B.; Kumar, N. Worldwide Incidence, Mortality and Time Trends for Cancer of the Oesophagus. Eur. J. Cancer Prev. 2017, 26, 107–118. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Tobacco Collaborators Smoking Prevalence and Attributable Disease Burden in 195 Countries and Territories, 1990-2015: A Systematic Analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [CrossRef]
- Education: A Missed Opportunity for Public Health Intervention. AJPH 2013, 103, 997–1001. Available online: https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2012.300993 (accessed on 29 March 2022). [CrossRef]
- Engel, L.S.; Chow, W.-H.; Vaughan, T.L.; Gammon, M.D.; Risch, H.A.; Stanford, J.L.; Schoenberg, J.B.; Mayne, S.T.; Dubrow, R.; Rotterdam, H.; et al. Population Attributable Risks of Esophageal and Gastric Cancers. J. Natl. Cancer Inst. 2003, 95, 1404–1413. [Google Scholar] [CrossRef]
- Ishiguro, S.; Sasazuki, S.; Inoue, M.; Kurahashi, N.; Iwasaki, M.; Tsugane, S. JPHC Study Group Effect of Alcohol Consumption, Cigarette Smoking and Flushing Response on Esophageal Cancer Risk: A Population-Based Cohort Study (JPHC Study). Cancer Lett. 2009, 275, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Islami, F.; Kamangar, F.; Nasrollahzadeh, D.; Aghcheli, K.; Sotoudeh, M.; Abedi-Ardekani, B.; Merat, S.; Nasseri-Moghaddam, S.; Semnani, S.; Sepehr, A.; et al. Socio-Economic Status and Oesophageal Cancer: Results from a Population-Based Case-Control Study in a High-Risk Area. Int. J. Epidemiol. 2009, 38, 978–988. [Google Scholar] [CrossRef]
- Dar, N.A.; Shah, I.A.; Bhat, G.A.; Makhdoomi, M.A.; Iqbal, B.; Rafiq, R.; Nisar, I.; Bhat, A.B.; Nabi, S.; Masood, A.; et al. Socioeconomic Status and Esophageal Squamous Cell Carcinoma Risk in Kashmir, India. Cancer Sci. 2013, 104, 1231–1236. [Google Scholar] [CrossRef]
- Zhang, L.; Cheng, H.; Zhou, Y.; Yuan, Z.; Chen, T.; Chen, X.; Lü, M. Association between socioeconomic status and esophageal squamous cell carcinoma in the population of Taixing area, Jiangsu province. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 147–150. [Google Scholar]
- Lin, Y.; Totsuka, Y.; He, Y.; Kikuchi, S.; Qiao, Y.; Ueda, J.; Wei, W.; Inoue, M.; Tanaka, H. Epidemiology of Esophageal Cancer in Japan and China. J. Epidemiol. 2013, 23, 233–242. [Google Scholar] [CrossRef]
- Sheikh, M.; Poustchi, H.; Pourshams, A.; Etemadi, A.; Islami, F.; Khoshnia, M.; Gharavi, A.; Hashemian, M.; Roshandel, G.; Khademi, H.; et al. Individual and Combined Effects of Environmental Risk Factors for Esophageal Cancer Based on Results From the Golestan Cohort Study. Gastroenterology 2019, 156, 1416–1427. [Google Scholar] [CrossRef]
- Sapkota, A.; Zaridze, D.; Szeszenia-Dabrowska, N.; Mates, D.; Fabiánová, E.; Rudnai, P.; Janout, V.; Holcatova, I.; Brennan, P.; Boffetta, P.; et al. Indoor Air Pollution from Solid Fuels and Risk of Upper Aerodigestive Tract Cancers in Central and Eastern Europe. Environ. Res. 2013, 120, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Mlombe, Y.B.; Rosenberg, N.E.; Wolf, L.L.; Dzamalala, C.P.; Chalulu, K.; Chisi, J.; Shaheen, N.J.; Hosseinipour, M.C.; Shores, C.G. Environmental Risk Factors for Oesophageal Cancer in Malawi: A Case-Control Study. Malawi Med. J. 2015, 27, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Guan, S.; Wang, J.; Zhao, L.; Jia, Y.; Lu, Z.; Yin, C.; Yang, S.; Song, Q.; Han, L.; et al. The Effects of Air Pollution on Mortality and Clinicopathological Features of Esophageal Cancer. Oncotarget 2017, 8, 58563–58576. [Google Scholar] [CrossRef] [PubMed]
- Abnet, C.C.; Arnold, M.; Wei, W.-Q. Epidemiology of Esophageal Squamous Cell Carcinoma. Gastroenterology 2018, 154, 360–373. [Google Scholar] [CrossRef]
- Okui, T. Age-Period-Cohort Analysis of Healthy Lifestyle Behaviors Using the National Health and Nutrition Survey in Japan. J. Prev. Med. Public Health 2020, 53, 409–418. [Google Scholar] [CrossRef]
- Wang, M.; Luo, X.; Xu, S.; Liu, W.; Ding, F.; Zhang, X.; Wang, L.; Liu, J.; Hu, J.; Wang, W. Trends in Smoking Prevalence and Implication for Chronic Diseases in China: Serial National Cross-Sectional Surveys from 2003 to 2013. Lancet Respir. Med. 2019, 7, 35–45. [Google Scholar] [CrossRef]
- Pan, X.-F.; Wang, L.; Pan, A. Epidemiology and Determinants of Obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Hoyo, C.; Cook, M.B.; Kamangar, F.; Freedman, N.D.; Whiteman, D.C.; Bernstein, L.; Brown, L.M.; Risch, H.A.; Ye, W.; Sharp, L.; et al. Body Mass Index in Relation to Oesophageal and Oesophagogastric Junction Adenocarcinomas: A Pooled Analysis from the International BEACON Consortium. Int. J. Epidemiol. 2012, 41, 1706–1718. [Google Scholar] [CrossRef]
- Kamangar, F.; Chow, W.-H.; Abnet, C.C.; Dawsey, S.M. Environmental Causes of Esophageal Cancer. Gastroenterol. Clin. N. Am. 2009, 38, 27–57. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| China | Japan | |||
|---|---|---|---|---|
| 1990 | 2019 | 1990 | 2019 | |
| Both | ||||
| ASMR a, per 100,000 | 22.08263 | 13.14883 | 4.931302 | 3.911883 |
| Deaths, ×1000 | 176.6016 | 257.3158 | 8.37199 | 13.99966 |
| Relative proportion in all causes of death, % | 2.11% | 2.41% | 1.03% | 1.00% |
| Men | ||||
| ASMR, per 100,000 | 30.52923 | 21.6905 | 9.356257 | 7.264125 |
| Deaths, ×1000 | 117.0849 | 197.7159 | 6.861007 | 11.55804 |
| Relative proportion in all causes of death, % | 2.55% | 3.17% | 1.56% | 1.62% |
| Women | ||||
| ASMR, per 100,000 | 14.69056 | 5.916205 | 1.570562 | 1.091518 |
| Deaths, ×1000 | 59.51674 | 59.59982 | 1.510983 | 2.441627 |
| Relative proportion in all causes of death, % | 1.58% | 1.35% | 0.41% | 0.35% |
| Drift | China | Japan | ||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| Local Drift a (95%CI) | ||||
| Age | ||||
| 25–29 | −1.69 (−4.42 to 1.12) | −5.71 (−10.58 to −0.57) | −1.09 (−4.40 to 2.34) | −0.77 (−5.16 to 3.83) |
| 30–34 | −2.13 (−3.42 to −0.81) | −5.91 (−8.85 to −2.87) | −1.66 (−3.20 to −0.08) | −0.45 (−2.94 to 2.11) |
| 35−39 | −2.86 (−3.62 to −2.10) | −6.32 (−8.30 to −4.30) | −2.47 (−3.30 to −1.64) | −0.21 (−1.58 to 1.19) |
| 40–44 | −3.21 (−3.64 to −2.77) | −6.65 (−7.88 to −5.41) | −3.12 (−3.53 to −2.71) | −0.10 (−0.85 to 0.64) |
| 45−49 | −2.84 (−3.12 to −2.56) | −6.57 (−7.37 to −5.77) | −3.40 (−3.62 to −3.17) | −0.18 (−0.66 to 0.30) |
| 50−54 | −2.23 (−2.43 to −2.02) | −6.11 (−6.67 to −5.54) | −2.85 (−3.00 to −2.71) | −0.10 (−0.43 to 0.24) |
| 55−59 | −1.83 (−2.00 to −1.65) | −5.42 (−5.85 to −4.98) | −2.06 (−2.16 to −1.96) | −0.06 (−0.32 to 0.20) |
| 60−64 | −1.43 (−1.59 to −1.28) | −4.60 (−4.93 to −4.28) | −1.38 (−1.46 to −1.31) | 0.00 (−0.21 to 0.21) |
| 65–69 | −1.38 (−1.52 to −1.23) | −4.15 (−4.43 to −3.88) | −0.77 (−0.83 to −0.71) | −0.27 (−0.45 to −0.09) |
| 70–74 | −1.36 (−1.52 to −1.20) | −3.68 (−3.95 to −3.41) | −0.36 (−0.43 to −0.30) | −1.01 (−1.17 to −0.84) |
| 75–79 | −1.20 (−1.41 to −1.00) | −3.09 (−3.40 to −2.78) | −0.34 (−0.42 to −0.26) | −2.01 (−2.18 to −1.85) |
| 80–84 | −0.71 (−1.05 to −0.36) | −2.28 (−2.74 to −1.81) | −0.42 (−0.54 to −0.30) | −2.86 (−3.07 to −2.66) |
| Net Drift a (95%CI) | ||||
| −1.98 (−2.22 to −1.74) | −5.22 (−5.77 to −4.68) | −1.86 (−2.12 to −1.59) | −0.50 (−0.91 to −0.08) | |
| Factor | China | Japan | ||||||
|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | |||||
| RR a | 95%CI b | RR | 95%CI | RR | 95%CI | RR | 95%CI | |
| Age | ||||||||
| 25–29 | 0.41 | 0.29 to 0.58 | 0.81 | 0.48 to 1.35 | 0.05 | 0.04 to 0.08 | 0.02 | 0.01 to 0.03 |
| 30–34 | 1.44 | 1.20 to 1.73 | 1.21 | 0.85 to 1.74 | 0.16 | 0.13 to 0.20 | 0.03 | 0.02 to 0.04 |
| 35–39 | 4.05 | 3.65 to 4.50 | 1.68 | 1.29 to 2.20 | 0.41 | 0.36 to 0.46 | 0.09 | 0.07 to 0.11 |
| 40–44 | 12.17 | 11.44 to 12.95 | 3.51 | 2.97 to 4.14 | 1.60 | 1.51 to 1.69 | 0.29 | 0.26 to 0.32 |
| 45–49 | 22.31 | 21.28 to 23.40 | 5.95 | 5.28 to 6.70 | 4.86 | 4.71 to 5.01 | 0.68 | 0.63 to 0.73 |
| 50–54 | 39.67 | 38.22 to 41.18 | 9.97 | 9.11 to 10.91 | 10.99 | 10.77 to 11.22 | 1.57 | 1.48 to 1.66 |
| 55–59 | 61.68 | 59.69 to 63.73 | 14.70 | 13.61 to 15.89 | 20.49 | 20.15 to 20.82 | 2.58 | 2.46 to 2.70 |
| 60–64 | 85.95 | 83.32 to 88.66 | 22.24 | 20.70 to 23.90 | 30.87 | 30.42 to 31.33 | 3.69 | 3.54 to 3.85 |
| 65–69 | 113.14 | 109.62 to 116.77 | 30.34 | 28.27 to 32.57 | 41.21 | 40.62 to 41.80 | 4.74 | 4.55 to 4.94 |
| 70–74 | 150.47 | 145.06 to 156.08 | 39.08 | 36.16 to 42.25 | 50.19 | 49.37 to 51.02 | 6.38 | 6.09 to 6.69 |
| 75–79 | 176.38 | 169.50 to 183.54 | 43.99 | 40.56 to 47.71 | 58.53 | 57.52 to 59.56 | 8.57 | 8.17 to 8.99 |
| 80–84 | 200.88 | 191.80 to 210.39 | 47.11 | 43.17 to 51.41 | 65.02 | 63.79 to 66.28 | 11.36 | 10.81 to 11.93 |
| Period | ||||||||
| 1990–1994 | 1.00 | 0.96 to 1.04 | 1.30 | 1.20 to 1.41 | 1.16 | 1.12 to 1.19 | 1.01 | 0.95 to 1.07 |
| 1995–1999 | 0.93 | 0.90 to 0.96 | 1.06 | 1.00 to 1.13 | 1.09 | 1.07 to 1.11 | 1.00 | 0.96 to 1.05 |
| 2000–2004 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| 2005–2009 | 0.90 | 0.87 to 0.93 | 0.74 | 0.70 to 0.79 | 0.91 | 0.89 to 0.92 | 0.97 | 0.94 to 1.01 |
| 2010–2014 | 0.71 | 0.68 to 0.73 | 0.46 | 0.43 to 0.50 | 0.81 | 0.79 to 0.83 | 0.94 | 0.89 to 0.99 |
| 2015–2019 | 0.60 | 0.58 to 0.63 | 0.35 | 0.32 to 0.38 | 0.73 | 0.70 to 0.76 | 0.89 | 0.83 to 0.95 |
| Cohort | ||||||||
| 1910–1914 | 1.43 | 1.28 to 1.61 | 3.53 | 3.00 to 4.15 | 1.36 | 1.31 to 1.42 | 1.94 | 1.80 to 2.09 |
| 1915–1919 | 1.48 | 1.38 to 1.58 | 3.38 | 3.02 to 3.77 | 1.29 | 1.26 to 1.33 | 1.64 | 1.54 to 1.74 |
| 1920–1924 | 1.48 | 1.41 to 1.56 | 3.16 | 2.88 to 3.46 | 1.23 | 1.21 to 1.26 | 1.33 | 1.26 to 1.40 |
| 1925–1930 | 1.42 | 1.36 to 1.48 | 2.88 | 2.65 to 3.13 | 1.23 | 1.20 to 1.25 | 1.10 | 1.05 to 1.16 |
| 1931–1934 | 1.31 | 1.26 to 1.36 | 2.42 | 2.24 to 2.62 | 1.25 | 1.22 to 1.27 | 1.00 | 0.95 to 1.05 |
| 1935–1939 | 1.21 | 1.17 to 1.26 | 1.96 | 1.82 to 2.12 | 1.21 | 1.19 to 1.23 | 0.98 | 0.94 to 1.03 |
| 1940–1944 | 1.11 | 1.07 to 1.15 | 1.55 | 1.43 to 1.67 | 1.16 | 1.14 to 1.18 | 0.98 | 0.94 to 1.03 |
| 1945–1949 | 1.08 | 1.04 to 1.12 | 1.28 | 1.19 to 1.39 | 1.13 | 1.11 to 1.15 | 1.00 | 0.96 to 1.05 |
| 1950–1954 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| 1955–1959 | 0.89 | 0.86 to 0.93 | 0.72 | 0.66 to 0.80 | 0.86 | 0.84 to 0.88 | 0.98 | 0.92 to 1.04 |
| 1960–1964 | 0.74 | 0.70 to 0.77 | 0.46 | 0.40 to 0.53 | 0.71 | 0.69 to 0.74 | 0.96 | 0.89 to 1.04 |
| 1965–1969 | 0.65 | 0.61 to 0.69 | 0.34 | 0.28 to 0.40 | 0.57 | 0.55 to 0.60 | 0.98 | 0.88 to 1.08 |
| 1970–1974 | 0.53 | 0.49 to 0.58 | 0.25 | 0.19 to 0.32 | 0.49 | 0.45 to 0.53 | 0.96 | 0.83 to 1.11 |
| 1975–1979 | 0.45 | 0.39 to 0.51 | 0.18 | 0.12 to 0.27 | 0.48 | 0.42 to 0.55 | 0.98 | 0.77 to 1.23 |
| 1980–1984 | 0.45 | 0.35 to 0.58 | 0.14 | 0.07 to 0.27 | 0.47 | 0.35 to 0.62 | 0.91 | 0.58 to 1.41 |
| 1985–1989 | 0.45 | 0.29 to 0.68 | 0.10 | 0.04 to 0.27 | 0.45 | 0.27 to 0.75 | 0.86 | 0.38 to 1.93 |
| 1990–1994 | 0.40 | 0.16 to 1.00 | 0.08 | 0.01 to 0.44 | 0.41 | 0.13 to 1.27 | 0.81 | 0.19 to 3.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, R.; Sun, J.; Wang, T.; Huang, L.; Wang, S.; Sun, P.; Yu, C. Comparison of Secular Trends in Esophageal Cancer Mortality in China and Japan during 1990–2019: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10302. https://doi.org/10.3390/ijerph191610302
Li R, Sun J, Wang T, Huang L, Wang S, Sun P, Yu C. Comparison of Secular Trends in Esophageal Cancer Mortality in China and Japan during 1990–2019: An Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health. 2022; 19(16):10302. https://doi.org/10.3390/ijerph191610302
Chicago/Turabian StyleLi, Ruiqing, Jinyi Sun, Tong Wang, Lihong Huang, Shuwen Wang, Panglin Sun, and Chuanhua Yu. 2022. "Comparison of Secular Trends in Esophageal Cancer Mortality in China and Japan during 1990–2019: An Age-Period-Cohort Analysis" International Journal of Environmental Research and Public Health 19, no. 16: 10302. https://doi.org/10.3390/ijerph191610302
APA StyleLi, R., Sun, J., Wang, T., Huang, L., Wang, S., Sun, P., & Yu, C. (2022). Comparison of Secular Trends in Esophageal Cancer Mortality in China and Japan during 1990–2019: An Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health, 19(16), 10302. https://doi.org/10.3390/ijerph191610302