
Distrustful, Dissatisfied, and Conspiratorial: A Latent Profile Analysis of COVID-19 Vaccination Rejection


Abstract
:
1. Introduction
1.1. Trust in Scientists, Satisfaction with the Government and Endorsement of Conspiracy Theories about COVID-19 Vaccination
1.2. Latent Profile Analysis in Researching Vaccine Attitudes
- RQ 1: Are there different latent profiles of individuals that quantitatively and qualitatively differ in terms of their trust in scientists, their satisfaction with the national government, and their belief in conspiracy theories?
- RQ 2: Do latent profiles differ by sociodemographic composition (gender, age, education, and political orientation)?
- RQ 3: Do the identified profiles differ in their attitudes toward vaccination against COVID-19?
2. Materials and Methods
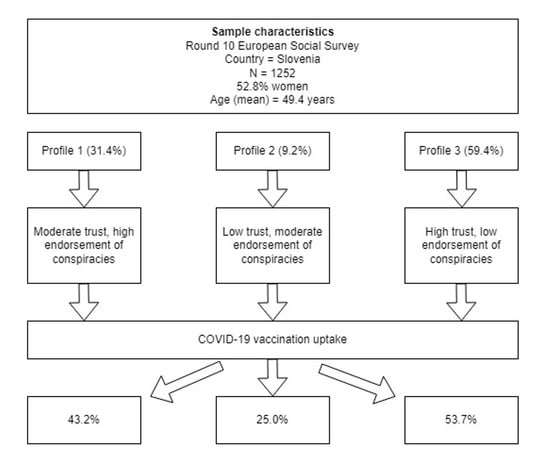
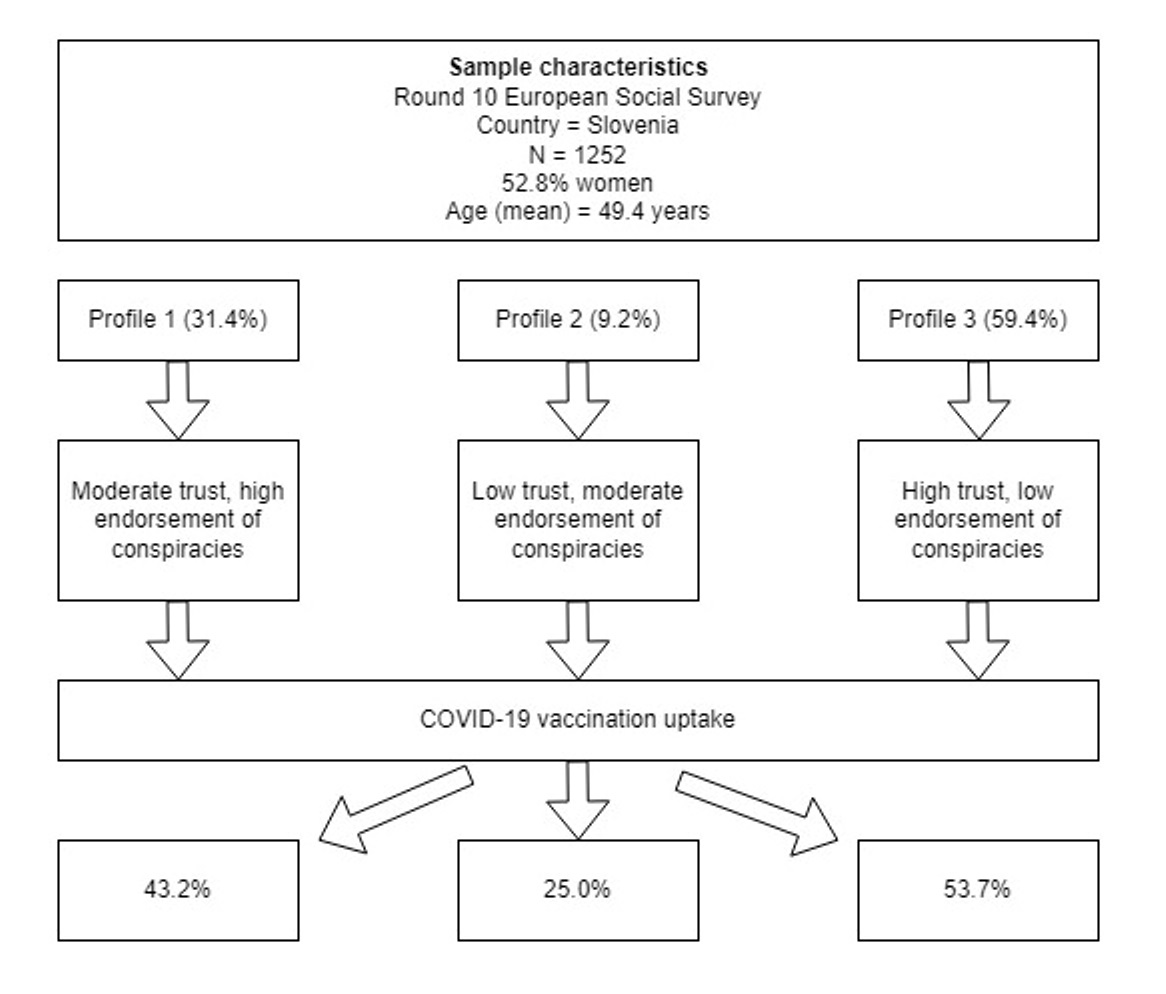
2.1. Participants
2.2. Materials
2.2.1. Latent Indicators
2.2.2. Sociodemographic Variables
2.2.3. Outcome Variables
2.3. Statistical Analyses
3. Results
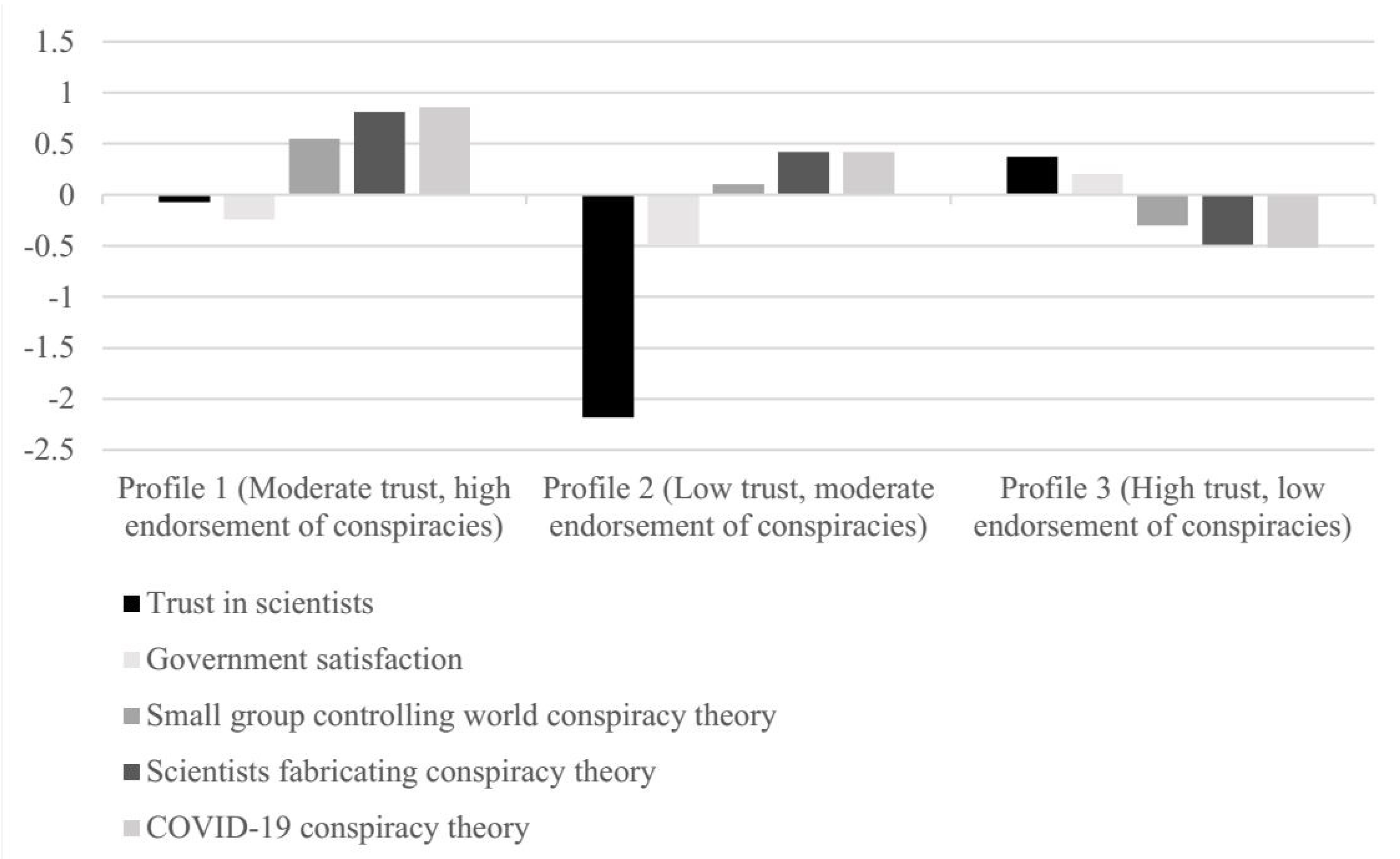
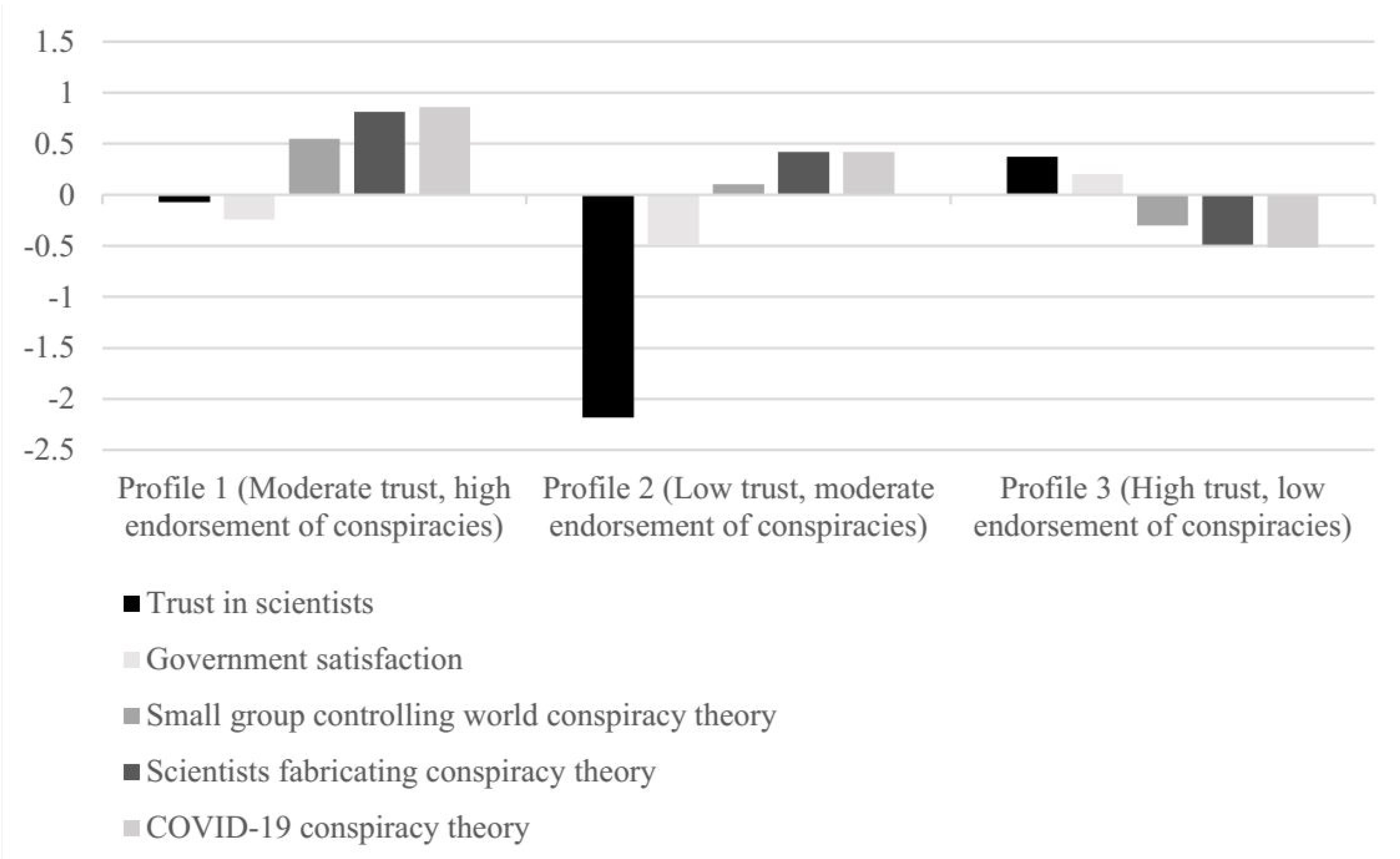
3.1. Latent Profiles of Trust and Conspiracy Theories Endorsement
3.2. Government and COVID-19 Pandemic
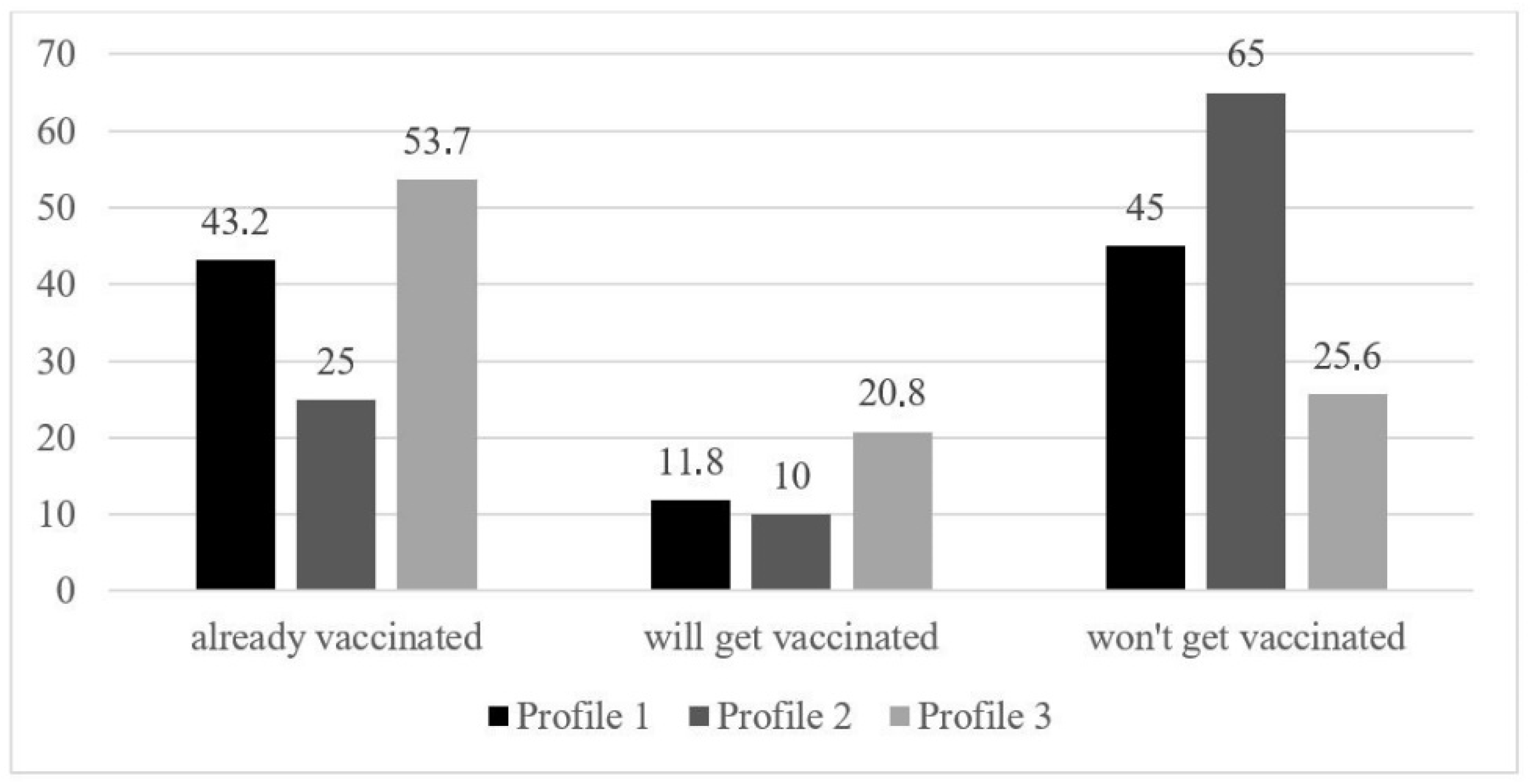
3.3. Differences between the Latent Profiles and Their Attitudes toward COVID-19 Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 18 April 2022).
- Larson, H.J.; de Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Republic of Slovenia. Vaccination|GOV.SI. Available online: https://www.gov.si/en/topics/vaccination/ (accessed on 12 August 2022).
- European Commision. European Citizens’ Knowledge and Attitudes towards Science and Technology—Eurobarometer Survey. Available online: https://europa.eu/eurobarometer/surveys/detail/2237 (accessed on 12 August 2022).
- European Commision. Attitudes on Vaccination against COVID-19—Eurobarometer Survey. Available online: https://europa.eu/eurobarometer/surveys/detail/2512 (accessed on 7 June 2022).
- Rozek, L.S.; Jones, P.; Menon, A.; Hicken, A.; Apsley, S.; King, E.J. Understanding Vaccine Hesitancy in the Context of COVID-19: The Role of Trust and Confidence in a Seventeen-Country Survey. Int. J. Public Health 2021, 66, 636255. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.O.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M.C. Lack of Trust, Conspiracy Beliefs, and Social Media Use Predict COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef] [PubMed]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2021, 51, 1763–1769. [Google Scholar] [CrossRef]
- Chen, X.; Lee, W.; Lin, F. Infodemic, Institutional Trust, and COVID-19 Vaccine Hesitancy: A Cross-National Survey. Int. J. Environ. Res. Public Health 2022, 19, 8033. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Yahaghai, R.; Alimoradi, Z.; Broström, A.; Griffiths, M.D.; Pakpour, A.H. The mediational role of trust in the healthcare system in the association between generalized trust and willingness to get COVID-19 vaccination in Iran. Hum. Vaccin. Immunother. 2022, 18, 1–8. [Google Scholar] [CrossRef]
- Trent, M.; Seale, H.; Chughtai, A.A.; Salmon, D.; MacIntyre, C.R. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: A comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2022, 40, 2498–2505. [Google Scholar] [CrossRef]
- Tagini, S.; Brugnera, A.; Ferrucci, R.; Priori, A.; Compare, A.; Parolin, L.; Pravettoni, G.; Silani, V.; Poletti, B. Behind the Scenes of COVID-19 Vaccine Hesitancy: Psychological Predictors in an Italian Community Sample. Vaccines 2022, 10, 1158. [Google Scholar] [CrossRef]
- Earnshaw, V.A.; Eaton, L.A.; Kalichman, S.C.; Brousseau, N.M.; Hill, E.C.; Fox, A.B. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl. Behav. Med. 2020, 10, 850–856. [Google Scholar] [CrossRef]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef]
- Cadeddu, C.; Sapienza, M.; Castagna, C.; Regazzi, L.; Paladini, A.; Ricciardi, W.; Rosano, A. Vaccine Hesitancy and Trust in the Scientific Community in Italy: Comparative Analysis from Two Recent Surveys. Vaccines 2021, 9, 1206. [Google Scholar] [CrossRef] [PubMed]
- Thaker, J. The Persistence of Vaccine Hesitancy: COVID-19 Vaccination Intention in New Zealand. J. Health Commun. 2021, 26, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Plohl, N.; Musil, B. Understanding, Trusting, and Applying Scientific Insights to Improve Your Health: A Latent Profile Analysis Approach. Int. J. Environ. Res. Public Health 2022, 19, 9967. [Google Scholar] [CrossRef]
- Douglas, K.M.; Sutton, R.M.; Cichocka, A. The Psychology of Conspiracy Theories. Curr. Dir. Psychol. Sci. 2017, 26, 538–542. [Google Scholar] [CrossRef]
- Goreis, A.; Kothgassner, O.D. Social Media as Vehicle for Conspiracy Beliefs on COVID-19. Digit. Psychol. 2020, 1, 36–39. [Google Scholar] [CrossRef]
- Constantinou, M.; Kagialis, A.; Karekla, M. COVID-19 Scientific Facts vs. Conspiracy Theories: 0–1: Science Fails to Convince Even Highly Educated Individuals. 2020. Available online: https://assets.researchsquare.com/files/rs-33972/v1/79c54352-5aa4-4e54-a82f-14d21069730f.pdf?c=1631842666 (accessed on 7 June 2022).
- Kessels, R.; Luyten, J.; Tubeuf, S. Willingness to get vaccinated against Covid-19 and attitudes toward vaccination in general. Vaccine 2021, 39, 4716–4722. [Google Scholar] [CrossRef]
- Hacquin, A.-S.; Altay, S.; de Araujo, E.; Chevallier, C.; Mercier, H. Sharp Rise in Vaccine Hesitancy in a Large and Representative Sample of the French Population: Reasons for Vaccine Hesitancy. PsyArXiv 2020. [Google Scholar]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Edwards, M.; Lobera, J.; Díaz-Catalán, C.; Barlow, F.K. Resolving the small-pockets problem helps clarify the role of education and political ideology in shaping vaccine scepticism. Br. J. Psychol. 2021, 112, 992–1011. [Google Scholar] [CrossRef]
- Spurk, D.; Hirschi, A.; Wang, M.; Valero, D.; Kauffeld, S. Latent profile analysis: A review and “how to” guide of its application within vocational behavior research. J. Vocat. Behav. 2020, 120, 103445. [Google Scholar] [CrossRef]
- Leung, C.L.K.; Li, K.-K.; Wei, V.W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S.; Kwok, K.O. Profiling vaccine believers and skeptics in nurses: A latent profile analysis. Int. J. Nurs. Stud. 2022, 126, 104142. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-L.; Lin, Y.-J.; Chang, Y.-P.; Chou, W.-J.; Yen, C.-F. Differences in Sources of Information, Risk Perception, and Cognitive Appraisals between People with Various Latent Classes of Motivation to Get Vaccinated against COVID-19 and Previous Seasonal Influenza Vaccination: Facebook Survey Study with Latent Profile Analysis in Taiwan. Vaccines 2021, 9, 1203. [Google Scholar] [CrossRef]
- Stahl, J.-P.; Cohen, R.; Denis, F.; Gaudelus, J.; Martinot, A.; Lery, T.; Lepetit, H. The impact of the web and social networks on vaccination. New challenges and opportunities offered to fight against vaccine hesitancy. Med. Mal. Infect. 2016, 46, 117–122. [Google Scholar] [CrossRef]
- Charron, J.; Gautier, A.; Jestin, C. Influence of information sources on vaccine hesitancy and practices. Med. Mal. Infect. 2020, 50, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccin. Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- European Social Survey ERIC. European Social Survey (ESS), Round 10—2020. 2022. Available online: https://ess-search.nsd.no/en/study/172ac431-2a06-41df-9dab-c1fd8f3877e7 (accessed on 12 August 2022).
- Lubke, G.; Neale, M.C. Distinguishing Between Latent Classes and Continuous Factors: Resolution by Maximum Likelihood? Multivar. Behav. Res. 2006, 41, 499–532. [Google Scholar] [CrossRef] [PubMed]
- Muthen, B.; Muthen, L.K. Integrating Person-Centered and Variable-Centered Analyses: Growth Mixture Modeling With Latent Trajectory Classes. Alcohol. Clin. Exp. Res. 2000, 24, 882–891. [Google Scholar] [CrossRef]
- Ferguson, S.L.; Moore, E.W.G.; Hull, D.M. Finding latent groups in observed data: A primer on latent profile analysis in Mplus for applied researchers. Int. J. Behav. Dev. 2020, 44, 458–468. [Google Scholar] [CrossRef]
- Tein, J.-Y.; Coxe, S.; Cham, H. Statistical Power to Detect the Correct Number of Classes in Latent Profile Analysis. Struct. Equ. Model. 2013, 20, 640–657. [Google Scholar] [CrossRef]
- Miller, J.M. Do COVID-19 Conspiracy Theory Beliefs Form a Monological Belief System? Can. J. Pol. Sci. 2020, 53, 319–326. [Google Scholar] [CrossRef]
- Wood, M.J.; Douglas, K.M.; Sutton, R.M. Dead and Alive. Soc. Psychol. Personal. Sci. 2012, 3, 767–773. [Google Scholar] [CrossRef]
- Meyer, S.B.; Violette, R.; Aggarwal, R.; Simeoni, M.; MacDougall, H.; Waite, N. Vaccine hesitancy and Web 2.0: Exploring how attitudes and beliefs about influenza vaccination are exchanged in online threaded user comments. Vaccine 2019, 37, 1769–1774. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Profile | LL | AIC | BIC | SABIC | Entropy | BLRT-p | LMR-p | Smallest Class % |
|---|---|---|---|---|---|---|---|---|
| 1 | −11966.490 | 23952.981 | 24004.306 | 23972.541 | / | / | / | / |
| 2 | −11731.906 | 23495.812 | 23577.932 | 23527.109 | 0.60 | <0.001 | <0.001 | 36.2 |
| 3 | −11664.573 | 23373.146 | 23486.061 | 23416.179 | 0.67 | <0.001 | 0.0196 | 9.1 |
| 4 | −11615.361 | 23286.721 | 23430.431 | 23341.490 | 0.70 | <0.001 | 0.1532 | 4.8 |
| 5 | −11558.414 | 23184.827 | 23359.332 | 23251.333 | 0.82 | <0.001 | 0.0016 | 2.9 |
| 6 | −11529.057 | 23138.113 | 23343.413 | 23216.355 | 0.84 | <0.001 | 0.1868 | 2.0 |
| Profile 1 (31.4%) (a) | Profile 2 (9.2%) (b) | Profile 3 (59.4%) (c) | F | η2 | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||
| Trust in scientists | 6.99 b,c | 1.56 | 2.42 c | 1.36 | 7.96 | 1.49 | 674.737 *** | 0.52 |
| Satisfaction with government | 3.08 b,c | 2.79 | 2.36 c | 2.73 | 4.35 | 2.84 | 40.997 *** | 0.06 |
| Small group controlling world conspiracy theory | 4.11b,c | 1.11 | 3.57 c | 1.32 | 3.07 | 1.11 | 113.601 *** | 0.15 |
| Scientists fabricating conspiracy theory | 4.18 b,c | 0.96 | 3.71 c | 1.17 | 2.59 | 0.95 | 364.604 *** | 0.36 |
| COVID-19 conspiracy theory | 4.38 b,c | 1.10 | 3.78 c | 1.20 | 2.50 | 0.98 | 421.600 *** | 0.41 |
| Profile 1 | Profile 2 | Profile 3 | |||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||
| Age | 51.12 | 19.4 | 47.89 | 15.36 | 48.73 | 19.22 | |
| f | % | f | % | f | % | ||
| Gender | Male | 197 | 50 | 52 | 45.6 | 342 | 46 |
| Female | 197 | 50 | 62 | 54.4 | 402 | 54 | |
| Education | Elementary or < | 75 | 19.3 | 27 | 23.7 | 104 | 14 |
| Secondary | 236 | 60.7 | 67 | 58.8 | 363 | 48.9 | |
| Tertiary (BA or similar) | 67 | 17.2 | 19 | 16.7 | 229 | 30.8 | |
| Tertiary (MA, PhD) | 11 | 2.8 | 1 | 0.9 | 47 | 6.3 | |
| Political orientation | Extreme left | 28 | 9 | 10 | 11.5 | 40 | 5.9 |
| Left-leaning | 70 | 22.5 | 17 | 19.5 | 147 | 21.6 | |
| Centrist | 139 | 44.7 | 42 | 48.3 | 305 | 44.8 | |
| Right-leaning | 55 | 17.7 | 14 | 16.1 | 143 | 21 | |
| Extreme right | 19 | 6.1 | 4 | 4.6 | 46 | 6.8 | |
| Profile 1 (a) | Profile 2 (b) | Profile 3 (c) | F | η2 | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||
| Satisfaction with government’s dealing with pandemic | 4.13 c | 2.88 | 3.41 c | 3.06 | 5.15 | 2.59 | 28.301 *** | 0.04 |
| Trusting government dealing with pandemic’s impact | 4.06 b,c | 2.87 | 2.93 c | 2.88 | 5.13 | 2.63 | 40.253 *** | 0.07 |
| Following government rules vs. own decisions when fighting pandemic | 5.78 c | 3.16 | 6.39 c | 3.25 | 4.87 | 3.04 | 18.716 *** | 0.03 |
| Profile 1 “Moderate Trust, High Endorsement of Conspiracies” | Profile 2 “Low Trust, Moderate Endorsement of Conspiracies” | |||
|---|---|---|---|---|
| β (SE) | Wald | β (SE) | Wald | |
| already have | −0.78 (0.21) *** | 13.504 | −1.70 (0.33) *** | 26.014 |
| will have a | −1.13 (0.30) *** | 13.960 | −1.66 (0.47) *** | 12.577 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamot, M.; Kerman, K.; Kirbiš, A. Distrustful, Dissatisfied, and Conspiratorial: A Latent Profile Analysis of COVID-19 Vaccination Rejection. Int. J. Environ. Res. Public Health 2022, 19, 10096. https://doi.org/10.3390/ijerph191610096
Lamot M, Kerman K, Kirbiš A. Distrustful, Dissatisfied, and Conspiratorial: A Latent Profile Analysis of COVID-19 Vaccination Rejection. International Journal of Environmental Research and Public Health. 2022; 19(16):10096. https://doi.org/10.3390/ijerph191610096
Chicago/Turabian StyleLamot, Monika, Katja Kerman, and Andrej Kirbiš. 2022. "Distrustful, Dissatisfied, and Conspiratorial: A Latent Profile Analysis of COVID-19 Vaccination Rejection" International Journal of Environmental Research and Public Health 19, no. 16: 10096. https://doi.org/10.3390/ijerph191610096
APA StyleLamot, M., Kerman, K., & Kirbiš, A. (2022). Distrustful, Dissatisfied, and Conspiratorial: A Latent Profile Analysis of COVID-19 Vaccination Rejection. International Journal of Environmental Research and Public Health, 19(16), 10096. https://doi.org/10.3390/ijerph191610096