
Organizational Justice and Health: A Survey in Hospital Workers

 ,
,  ,
,  ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Intergroup Comparison
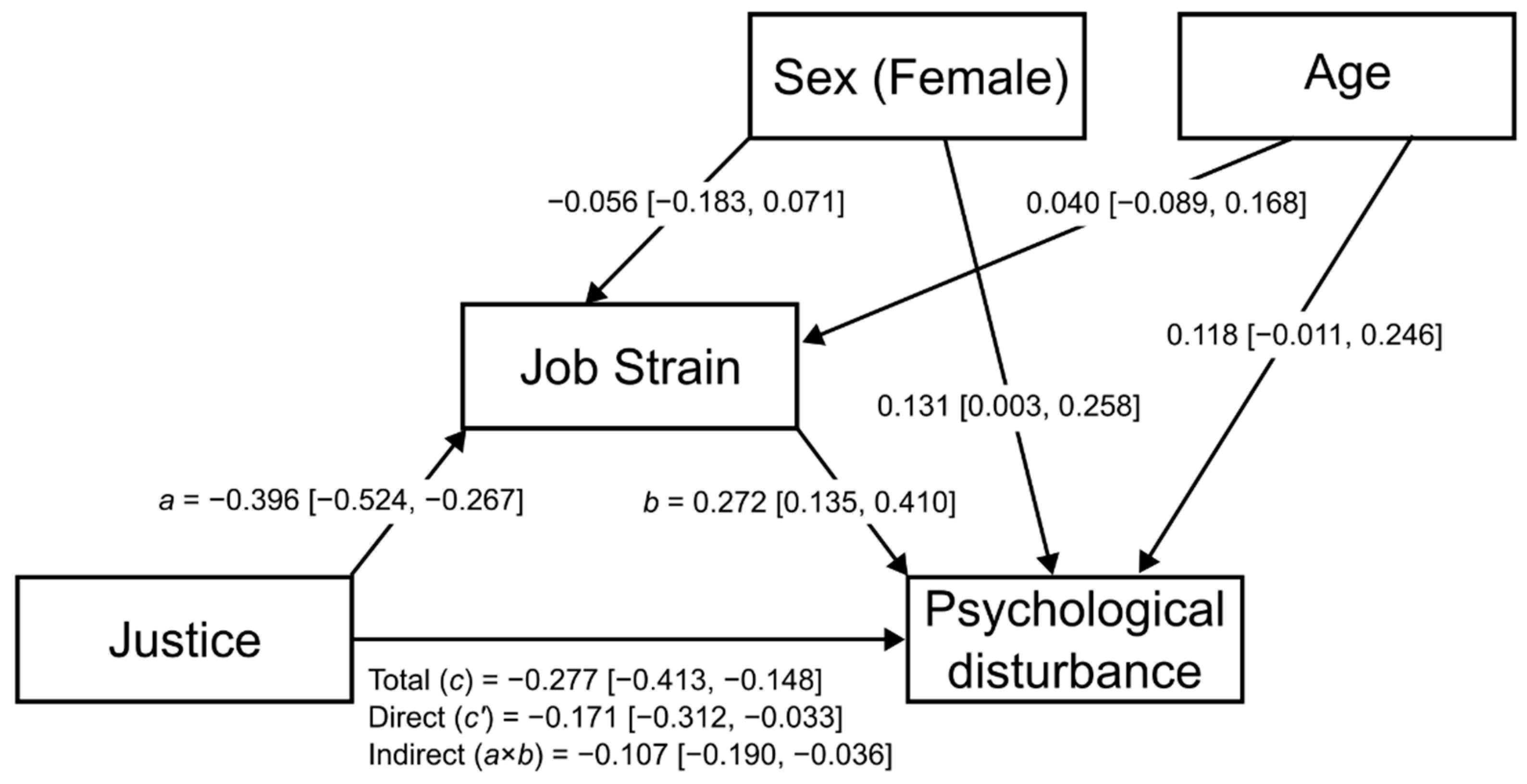
3.3. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elovainio, M.; Heponiemi, T.; Sinervo, T.; Magnavita, N. Organizational justice and health; review of evidence. G. Ital. Med. Lav. Ergon. 2010, 32, 5–9. [Google Scholar]
- Virtanen, M.; Elovainio, M. Justice at the workplace: A review. Camb. Q. Healthc. Ethics 2018, 27, 306–315. [Google Scholar] [CrossRef]
- Global Burden of Disease Study GBD 2016. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259, Erratum in Lancet 2017, 390, e38.
- Serranheira, F.; Sousa-Uva, M.; Heranz, F.; Kovacs, F.; Sousa-Uva, A. Low Back Pain (LBP), work and absenteeism. Work 2020, 65, 463–469. [Google Scholar] [CrossRef]
- Vernon, H. The Neck Disability Index: State-of-the-art, 1991–2008. J. Manip. Physiol. Ther. 2008, 31, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Vinstrup, J.; Jakobsen, M.D.; Andersen, L.L. Perceived stress and low-back pain among healthcare workers: A multi-center prospective cohort study. Front. Public Health 2020, 8, 297. [Google Scholar] [CrossRef]
- Acquadro Maran, D.; Magnavita, N.; Garbarino, S. Identifying Organizational Stressors That Could Be a Source of Discomfort in Police Officers: A Thematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3720. [Google Scholar] [CrossRef]
- Pimentel, M.A.F.; Redfern, O.C.; Gerry, S.; Collins, G.S.; Malycha, J.; Prytherch, D.; Schmidt, P.E.; Smith, G.B.; Watkinson, P.J. A comparison of the ability of the National Early Warning Score and the National Early Warning Score 2 to identify patients at risk of in-hospital mortality: A multi-centre database study. Resuscitation. 2019, 134, 147–156. [Google Scholar] [CrossRef]
- Moridzadeh, R.S.; Sanaiha, Y.; Madrigal, J.; Antonios, J.; Benharash, P.; Baril, D.T. Nationwide comparison of the medical complexity of patients by surgical specialty. J. Vasc. Surg. 2021, 73, 683–688.e2. [Google Scholar] [CrossRef] [PubMed]
- Dryden-Palmer, K.D.; Parshuram, C.S.; Berta, W.B. Context, complexity and process in the implementation of evidence-based innovation: A realist informed review. BMC Health Serv. Res. 2020, 20, 81. [Google Scholar] [CrossRef] [PubMed]
- Cozijnsen, L.; Levi, M.; Verkerk, M.J. Why industrial methods do not work in healthcare: An analytical approach. Intern. Med. J. 2020, 50, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Sara, J.D.; Prasad, M.; Eleid, M.F.; Zhang, M.; Widmer, R.J.; Lerman, A. Association Between Work-Related Stress and Coronary Heart Disease: A Review of Prospective Studies Through the Job Strain, Effort-Reward Balance, and Organizational Justice Models. J. Am. Heart Assoc. 2018, 7, e008073. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Van der Molen, H.F.; Nieuwenhuijsen, K.; Frings-Dresen, M.H.W.; de Groene, G. Work-related psychosocial risk factors for stress-related mental disorders: An updated systematic review and meta-analysis. BMJ Open 2020, 10, e034849. [Google Scholar] [CrossRef]
- Bastos, A.; Sá, J.C.; Fernandes, S.M. A study on the reality of Portuguese companies about work health and safety. In Occupational Safety and Hygiene, 2nd ed.; Arezes, P., Baptista, J.S., Barroso, M.P., Carneiro, P., Eds.; Taylor & Francis: London, UK, 2014; Volume II, pp. 687–691. Available online: https://www.researchgate.net/publication/300376480_A_study_on_the_reality_of_Portuguese_companies_about_work_health_and_safety (accessed on 7 July 2022).
- Anderson, G.S.; Di Nota, P.M.; Groll, D.; Carleton, R.N. Peer Supportand Crisis-Focused Psychological Interventions Designed to Mitigate Post-Traumatic Stress Injuries among Public Safety and Frontline Healthcare Personnel: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7645. [Google Scholar] [CrossRef] [PubMed]
- Di Nota, P.M.; Kasurak, E.; Bahji, A.; Groll, D.; Anderson, G.S. Coping among public safety personnel: A systematic review and meta-analysis. Stress Health 2021, 37, 613–630. [Google Scholar] [CrossRef]
- Finney, C.; Stergiopoulos, E.; Hensel, J.; Bonato, S.; Dewa, C.S. Organizational stressors associated with job stress and burnout in correctional officers: A systematic review. BMC Public Health 2013, 13, 82. [Google Scholar] [CrossRef]
- Colquitt, J.A.; Conlon, D.E.; Wesson, M.J.; Porter, C.O.; Ng, K.Y. Justice at the millennium: A meta-analytic review of 25 years of organizational justice research. J. Appl. Psychol. 2001, 86, 425–445. [Google Scholar] [CrossRef]
- Magnavita, N.; Bergamaschi, A. Justice at the workplace. Validation of the Italian version of Colquitt’s justice measurement questionnaire (JM20). G. Ital. Med. Lav. Ergon. 2008, 30, 449–450. [Google Scholar]
- Enoksen, E. Examining the dimensionality of Colquitt’s Organizational Justice Scale in a public health sector context. Psychol. Rep. 2015, 116, 723–737. [Google Scholar] [CrossRef] [PubMed]
- Baka, Ł. Development and validation of the Polish version of Colquitt’s organizational justice measure. Int. J. Occup. Med. Environ. Health 2018, 31, 415–427. [Google Scholar] [CrossRef]
- Karasek, R.A. Job demands, job decision latitude, and mental strain: Implications for job redesign. Admin. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Theorell, T.; Perski, A.; Åkerstedt, T.; Sigala, F.; Ahlberg-Hultén, G.; Svensson, J.; Eneroth, P. Changes in job strain in relation to changes in physiological state: A longitudinal study. Scand. J. Work. Environ. Health 1988, 14, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N. Two tools for health surveillance of job stress: The Karasek Job Content Questionnaire and the Siegrist Effort Reward Imbalance Questionnaire. G. Ital. Med. Lav. Ergon. 2007, 29, 667–670. [Google Scholar] [PubMed]
- Karasek, R.; Choi, B.; Ostergren, P.O.; Ferrario, M.; Smet, P.D. Testing two methods to create comparable scale scores between the Job Content Questionnaire (JCQ) and JCQ-like questionnaires in the European JACE Study. Int. J. Behav. Med. 2007, 14, 189–201. [Google Scholar] [CrossRef]
- Goldberg, P. The Detection of Psychiatric Illness by Questionnaire; Oxford University Press: Oxford, UK, 1972. [Google Scholar]
- Piccinelli, M.; Bisoffi, G.; Bon, M.G.; Cunico, L.; Tansella, M. Validity and test-retest reliability of the Italian version of the 12-item General Health Questionnaire in general practice: A comparison between three scoring methods. Compr. Psychiatry 1993, 34, 198–205. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- PROCESS Vers. 4.1 © 2012–2022 by Andrew F. Hayes. Available online: https://uedufy.com/data-analysis/spss/ (accessed on 7 July 2022).
- Ministry of Health. Staff of the National Health Service 2020. Available online: https://www.salute.gov.it/portale/temi/p2_6.jsp?id=5237&area=statisticheSSN&menu=personaleSSN (accessed on 7 July 2022).
- Ndjaboué, R.; Brisson, C.; Vézina, M. Organisational justice and mental health: A systematic review of prospective studies. Occup. Environ. Med. 2012, 69, 694–700. [Google Scholar] [CrossRef]
- Haghighinezhad, G.; Atashzadeh-Shoorideh, F.; Ashktorab, T.; Mohtashami, J.; Barkhordari-Sharifabad, M. Relationship between perceived organizational justice and moral distress in intensive care unit nurses. Nurs. Ethics 2019, 26, 460–470. [Google Scholar] [CrossRef]
- Top, M.; Tekingunduz, S. The effect of organizational justice and trust on job stress in hospital organizations. J. Nurs. Scholarsh. 2018, 50, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N. Is there a gender gap in Italian radiology? A cross-sectional study. Eur. J. Radiol. 2013, 82, e502–e507. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Odagiri, Y.; Takamiya, T.; Ohya, Y.; Inoue, S. Organizational justice and insomnia: A prospective cohort study examining insomnia onset and persistence. Int. Arch. Occup. Environ. Health 2017, 90, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Kondo, N. Organizational justice, psychological distress, and stress-related behaviors by occupational class in female Japanese employees. PLoS ONE 2019, 14, e0214393. [Google Scholar] [CrossRef]
- Kakemam, E.; Torkzadeh, L.; Rouzbahani, M.; Zahedi, H.; Chegini, Z. The relationship between workplace deviant behaviors and organizational justice among nurses: A cross-sectional survey. Nurs. Forum. 2021, 56, 889–896. [Google Scholar] [CrossRef]
- Hashish, E.A.A. Nurses’ perception of organizational justice and its relationship to their workplace deviance. Nurs. Ethics 2020, 27, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Mengstie, M.M. Perceived organizational justice and turnover intention among hospital healthcare workers. BMC Psychol. 2020, 8, 19. [Google Scholar] [CrossRef]
- Choi, H.; Shin, S. The Factors That Affect Turnover Intention According to Clinical Experience: A Focus on Organizational Justice and Nursing Core Competency. Int. J. Environ. Res. Public Health 2022, 19, 3515. [Google Scholar] [CrossRef]
- Shimamura, M.; Fukutake, M.; Namba, M.; Ogino, T. The relationship among factors of organizational justice, organizational citizenship behavior, job satisfaction, and ease of work among Japanese nurses. Appl. Nurs. Res. 2021, 61, 151479. [Google Scholar] [CrossRef]
- Chen, D.; Lin, Q.; Yang, T.; Shi, L.; Bao, X.; Wang, D. Distributive Justice and Turnover Intention Among Medical Staff in Shenzhen, China: The Mediating Effects of Organizational Commitment and Work Engagement. Risk Manag. Healthc. Policy 2022, 15, 665–676. [Google Scholar] [CrossRef]
- Chen, S.Y.; Wu, W.C.; Chang, C.S.; Lin, C.T.; Kung, J.Y.; Weng, H.C.; Lin, Y.T.; Lee, S.I. Organizational justice, trust, and identification and their effects on organizational commitment in hospital nursing staff. BMC Health Serv. Res. 2015, 15, 363. [Google Scholar] [CrossRef] [PubMed]
- Ybema, J.F.; van der Meer, L.; Leijten, F.R. Longitudinal relationships between organizational justice, productivity loss, and sickness absence among older employees. Int. J. Behav. Med. 2016, 23, 645–654. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Correia, I.; Almeida, A.E. Organizational justice, professional identification, empathy, and meaningful work during COVID-19 pandemic: Are they burnout protectors in physicians and nurses? Front. Psychol. 2020, 11, 566139. [Google Scholar] [CrossRef]
- Arakelian, E.; Paulsson, S.; Molin, F.; Svartengren, M. How Human Resources Index, Relational Justice, and Perceived Productivity Change after Reorganization at a Hospital in Sweden That Uses a Structured Support Model for Systematic Work Environment Management. Int. J. Environ. Res. Public Health 2021, 18, 11611. [Google Scholar] [CrossRef] [PubMed]
- Luger, T.; Maher, C.G.; Rieger, M.A.; Steinhilber, B. Work-break schedules for preventing musculoskeletal symptoms and disorders in healthy workers. Cochrane Database Syst. Rev. 2019, 7, CD012886. [Google Scholar] [CrossRef]
- Lo, J.; Chan, L.; Flynn, S. A Systematic Review of the Incidence, Prevalence, Costs, and Activity and Work Limitations of Amputation, Osteoarthritis, Rheumatoid Arthritis, Back Pain, Multiple Sclerosis, Spinal Cord Injury, Stroke, and Traumatic Brain Injury in the United States: A 2019 Update. Arch. Phys. Med. Rehabil. 2021, 102, 115–131. [Google Scholar] [CrossRef]
- Sahar, T.; Cohen, M.J.; Ne’eman, V.; Kandel, L.; Odebiyi, D.O.; Lev, I.; Brezis, M.; Lahad, A. Insoles for prevention and treatment of back pain. Cochrane Database Syst. Rev. 2007, 4, CD005275. [Google Scholar] [CrossRef]
- Huang, R.; Ning, J.; Chuter, V.H.; Taylor, J.B.; Christophe, D.; Meng, Z.; Xu, Y.; Jiang, L. Exercise alone and exercise combined with education both prevent episodes of low back pain and related absenteeism: Systematic review and network meta-analysis of randomised controlled trials (RCTs) aimed at preventing back pain. Br. J. Sports Med. 2020, 54, 766–770. [Google Scholar] [CrossRef]
- Maciel, R.R.B.T.; Dos Santos, N.C.; Portella, D.D.A.; Alves, P.G.J.M.; Martinez, B.P. Effects of physical exercise at the workplace for treatment of low back pain: A systematic review with meta-analysis. Rev. Bras. Med. Trab. 2018, 16, 225–235. [Google Scholar] [CrossRef]
- Chirico, F.; Nucera, G.; Magnavita, N. COVID-19: Protecting Healthcare Workers is a priority. Infect. Control Hosp. Epidemiol. 2020, 41, 1117. [Google Scholar] [CrossRef]


{kind=link}
| Sex | N | % |
|---|---|---|
| Male | 83 | 38.1 |
| Female | 135 | 61.9 |
| Age | ||
| <25 | 9 | 4.1 |
| 30–34 | 13 | 6.0 |
| 35–39 | 43 | 19.7 |
| 40–44 | 36 | 16.5 |
| 45–49 | 41 | 18.8 |
| 50–59 | 68 | 31.2 |
| >60 | 8 | 3.7 |
| Category | ||
| Physician | 50 | 22.9 |
| Nurse | 112 | 51.4 |
| Support staff | 56 | 25.7 |
| Physician (N = 50) | Nurse (N = 107) | Auxiliary Staff (N = 55) | p Value * | |
|---|---|---|---|---|
| Organizational Justice | 61.64 ± 16.61 | 63.09 ± 17.75 | 66.91 ± 15.98 | 0.206 |
| Procedural Justice | 19.44 ± 6.28 | 20.08 ± 6.39 | 20.87 ± 6.26 | 0.509 |
| Distributive Justice | 11.12 ± 3.62 | 11.84 ± 3.94 | 13.05 ± 4.04 | 0.036 1 vs. 3 = 0.035 |
| Interpersonal Justice | 14.74 ± 4.82 | 14.30 ± 3.95 | 15.47 ± 4.10 | 0.245 |
| Informational Justice | 16.34 ± 5.63 | 16.78 ± 4.38 | 17.51 ± 4.53 | 0.436 |
| Younger (<40 years) (N = 65) | Middle (40–49 years) (N = 77) | Older (>50 years) (N = 76) | ||
| Organizational Justice | 65.87 ± 14.41 | 65.55 ± 16.91 | 60.11 ± 16.02 | 0.053 |
| Procedural Justice | 20.33 ± 5.82 | 21.27 ± 6.74 | 18.80 ± 6.12 | 0.052 |
| Distributive Justice | 12.40 ± 3.60 | 12.38 ± 4.15 | 11.23 ± 3.94 | 0.124 |
| Interpersonal Justice | 15.35 ± 3.91 | 14.71 ± 4.13 | 14.16 ± 4.51 | 0.257 |
| Informational Justice | 17.76 ± 4.65 | 17.18 ± 4.49 | 15.80 ± 4.90 | 0.041 1 vs. 3 = 0.047 |
| Male (N = 83) | Female (N = 129) | |||
| Organizational Justice | 66.57 ± 14.45 | 61.92 ± 16.82 | 0.040 | |
| Procedural Justice | 21.06 ± 6.09 | 19.55 ± 6.42 | 0.089 | |
| Distributive Justice | 12.47 ± 3.53 | 11.68 ± 4.16 | 0.153 | |
| Interpersonal Justice | 15.49 ± 3.58 | 14.21 ± 4.51 | 0.029 | |
| Informational Justice | 17.54 ± 4.70 | 16.44 ± 4.72 | 0.096 |
| 1 | 2 | 3 | |
|---|---|---|---|
| 1. Justice | 1 | −0.389 *** | −0.279 *** |
| 2. Job Strain | −0.393 *** | 1 | 0.342 *** |
| 3. Mental disturbance | −0.304 *** | 0.350 *** | 1 |
| Measure | Unstandardized Coefficients | Standard Error | t | p Value | Standardized Coefficients |
|---|---|---|---|---|---|
| Total association | −0.094 (−0.138, −0.049) | 0.022 | −4.162 | <0.001 | −0.277 (−0.413, −0.148) |
| Direct association | −0.058 (−0.104, −0.011) | 0.024 | −2.441 | 0.015 | −0.171 (−0.312, −0.033) |
| Indirect association mediated via Job strain | −0.036 (−0.069, −0.011) | 0.015 | −0.107 (−0.190, −0.036) | ||
| R2 | 0.183 |
| Variable | Model I (Unadjusted) OR (95% CI) | p Value | Model II (Adjusted) OR (95%CI) | p Value | R2 |
|---|---|---|---|---|---|
| Organizational Justice | 0.963 (0.943, 0.984) | <0.001 | 0.961 (0.939, 0.984) | <0.001 | 0.200 |
| Job Strain | 6.122 (2.009, 18.659) | <0.001 | 8.077 (2.385, 27.356) | <0.001 | 0.206 |
| Social Support | 0.843 (0.760, 0.936) | <0.001 | 0.816 (0.726, 0.918) | <0.001 | 0.209 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magnavita, N.; Chiorri, C.; Acquadro Maran, D.; Garbarino, S.; Di Prinzio, R.R.; Gasbarri, M.; Matera, C.; Cerrina, A.; Gabriele, M.; Labella, M. Organizational Justice and Health: A Survey in Hospital Workers. Int. J. Environ. Res. Public Health 2022, 19, 9739. https://doi.org/10.3390/ijerph19159739
Magnavita N, Chiorri C, Acquadro Maran D, Garbarino S, Di Prinzio RR, Gasbarri M, Matera C, Cerrina A, Gabriele M, Labella M. Organizational Justice and Health: A Survey in Hospital Workers. International Journal of Environmental Research and Public Health. 2022; 19(15):9739. https://doi.org/10.3390/ijerph19159739
Chicago/Turabian StyleMagnavita, Nicola, Carlo Chiorri, Daniela Acquadro Maran, Sergio Garbarino, Reparata Rosa Di Prinzio, Martina Gasbarri, Carmela Matera, Anna Cerrina, Maddalena Gabriele, and Marcella Labella. 2022. "Organizational Justice and Health: A Survey in Hospital Workers" International Journal of Environmental Research and Public Health 19, no. 15: 9739. https://doi.org/10.3390/ijerph19159739
APA StyleMagnavita, N., Chiorri, C., Acquadro Maran, D., Garbarino, S., Di Prinzio, R. R., Gasbarri, M., Matera, C., Cerrina, A., Gabriele, M., & Labella, M. (2022). Organizational Justice and Health: A Survey in Hospital Workers. International Journal of Environmental Research and Public Health, 19(15), 9739. https://doi.org/10.3390/ijerph19159739