
Collaborative Reverse Logistics Network for Infectious Medical Waste Management during the COVID-19 Outbreak


Abstract
:1. Introduction
1.1. IMW Management
1.2. Logistics
- Build a collaborative location and routing optimization model for IMW by introducing MPCs and mobile processing facilities;
- Develop a quantitative method for the estimation of IMW generated in the stage of a pandemic;
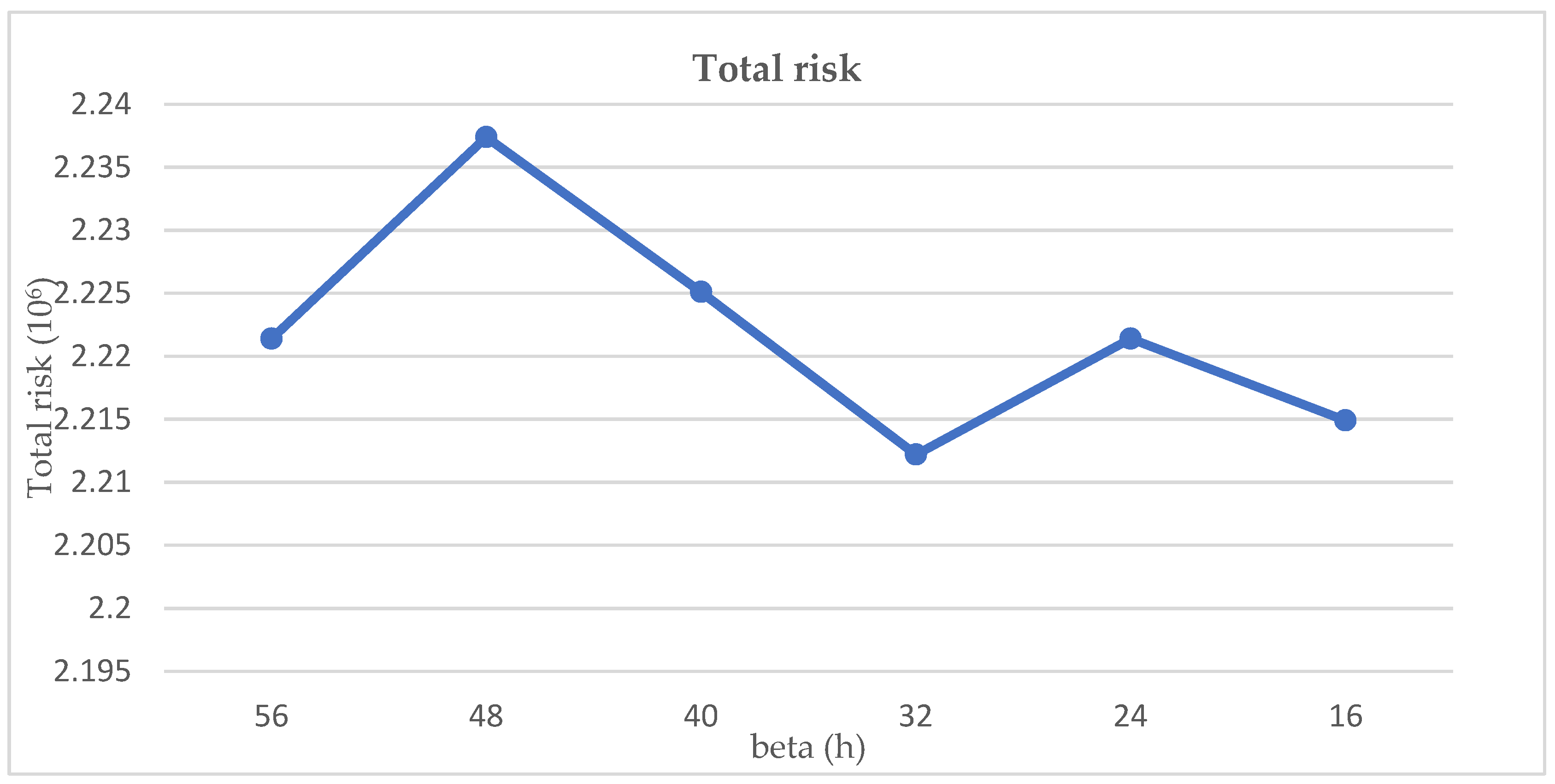
- Consider infection risk and transportation timeliness to meet the requirements of the storage time restriction of IMW treatment (i.e., not exceed 48 h);
- Provide a case study in a real situation to obtain general managerial implications.
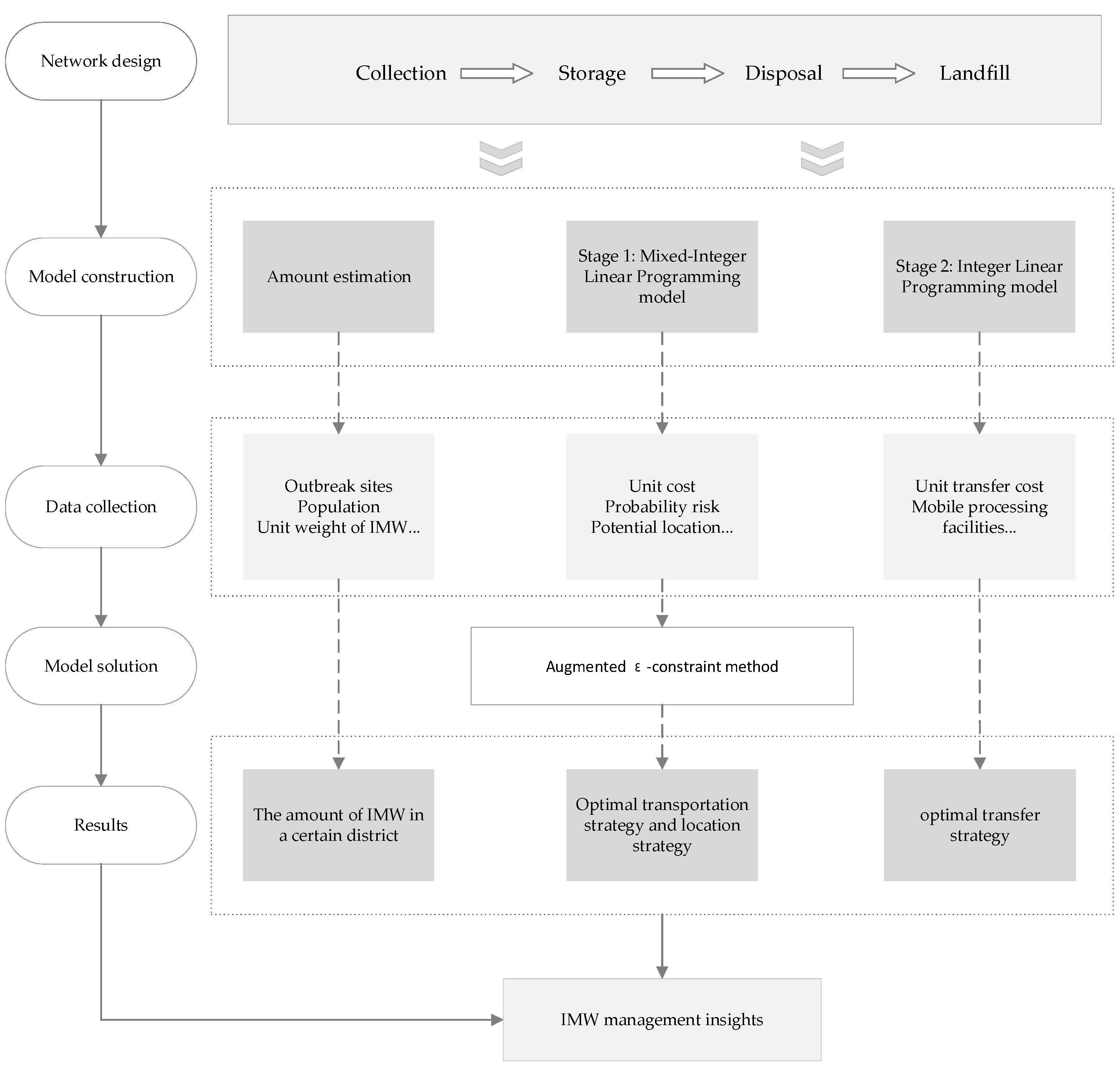
2. Materials and Methods
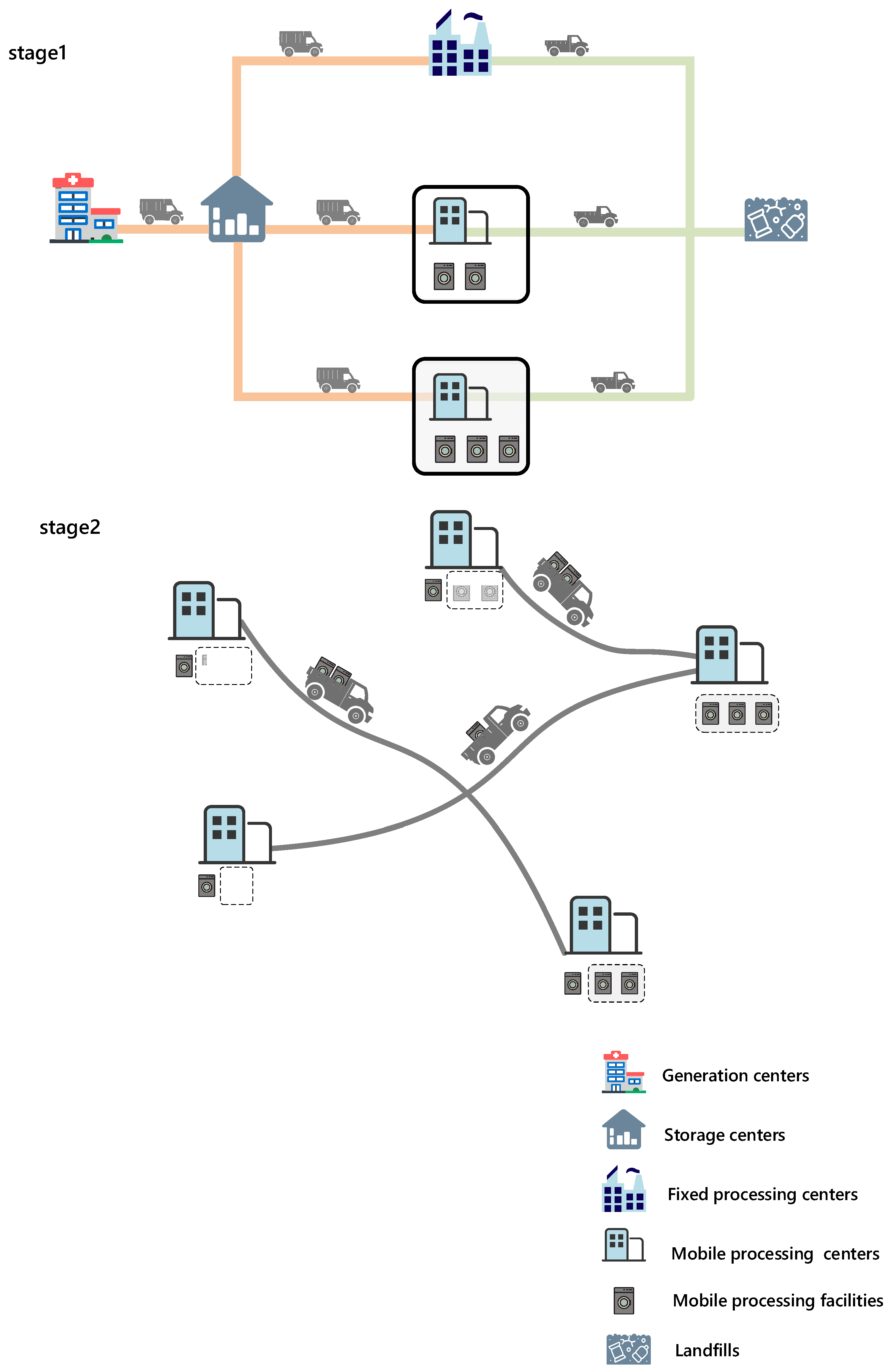
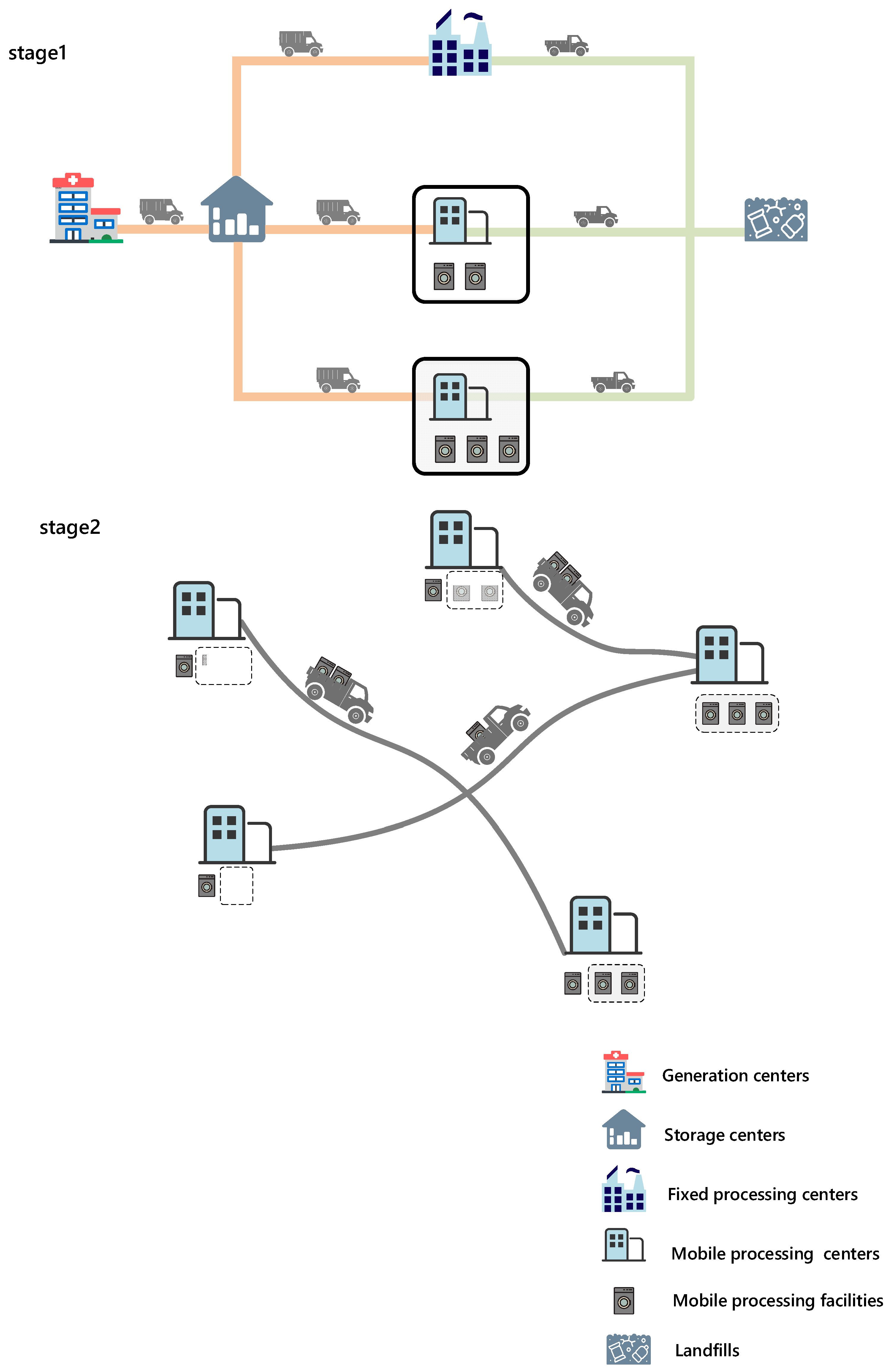
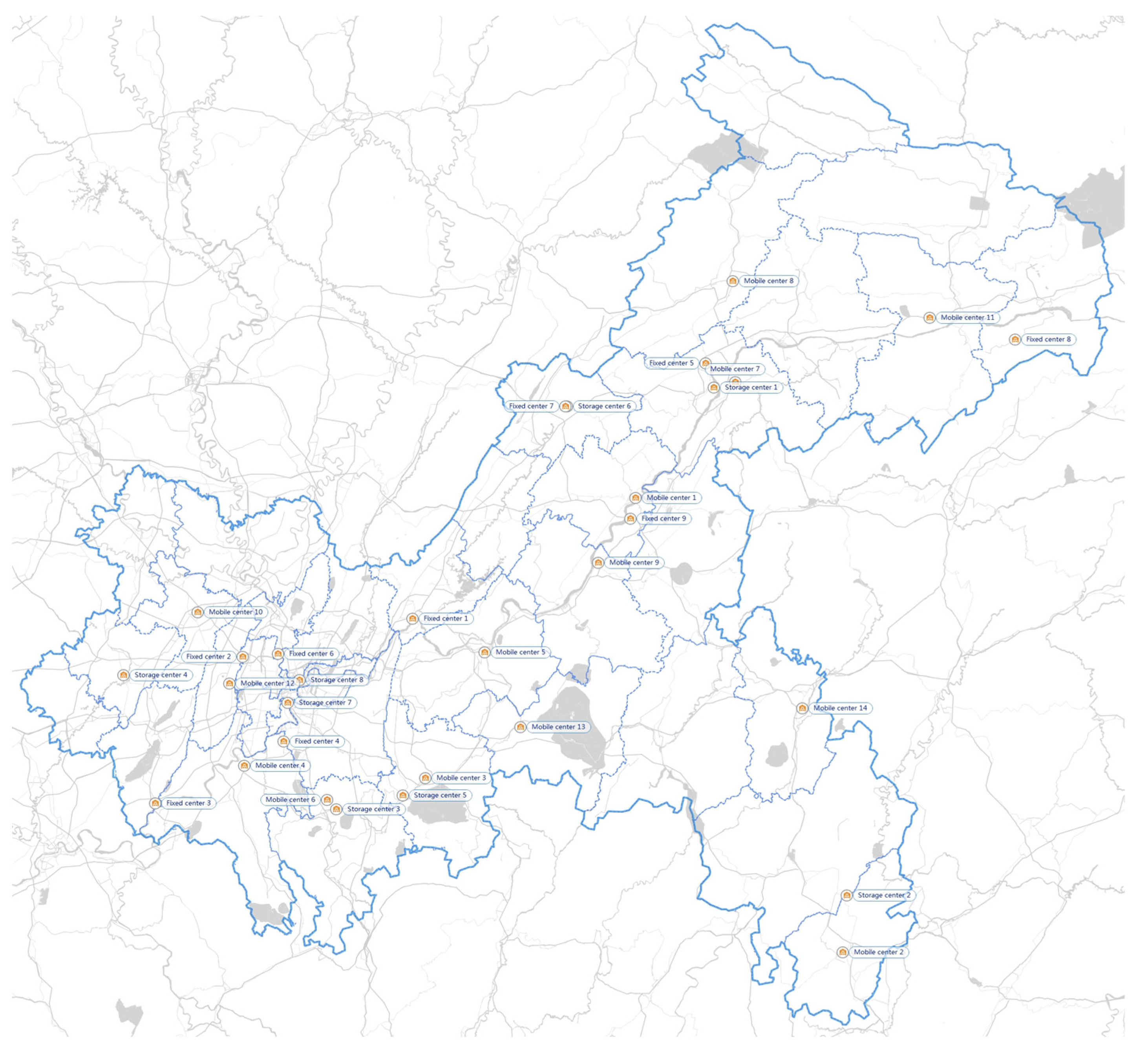
2.1. The Structure of IMW Network
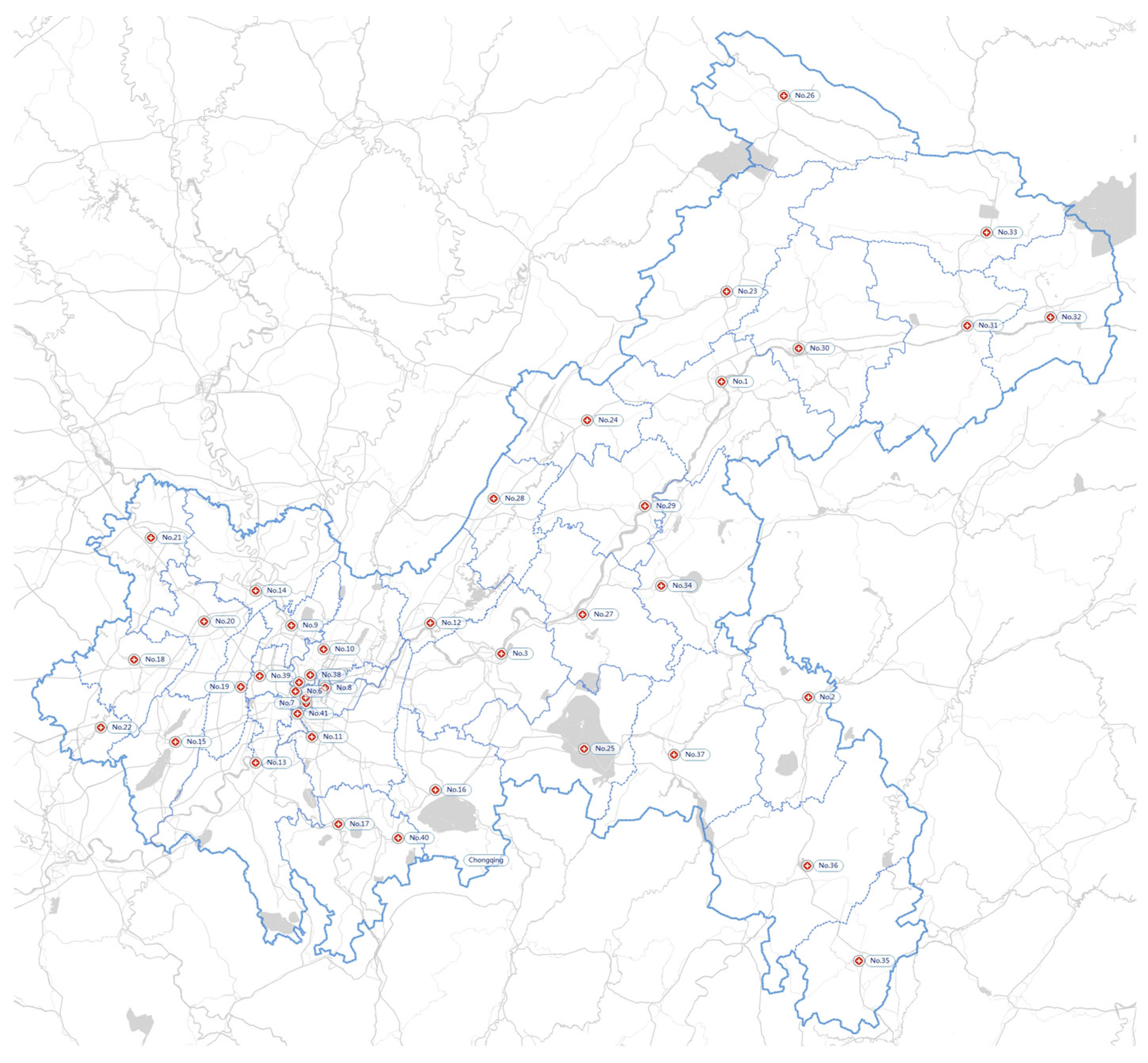
- IMW originates from existing hospitals, temporary hospitals, clinics, laboratories, and residential areas.
- IMW has been collected from all generators to the largest public hospital of the district, so the network starts with the largest public hospitals from all districts.
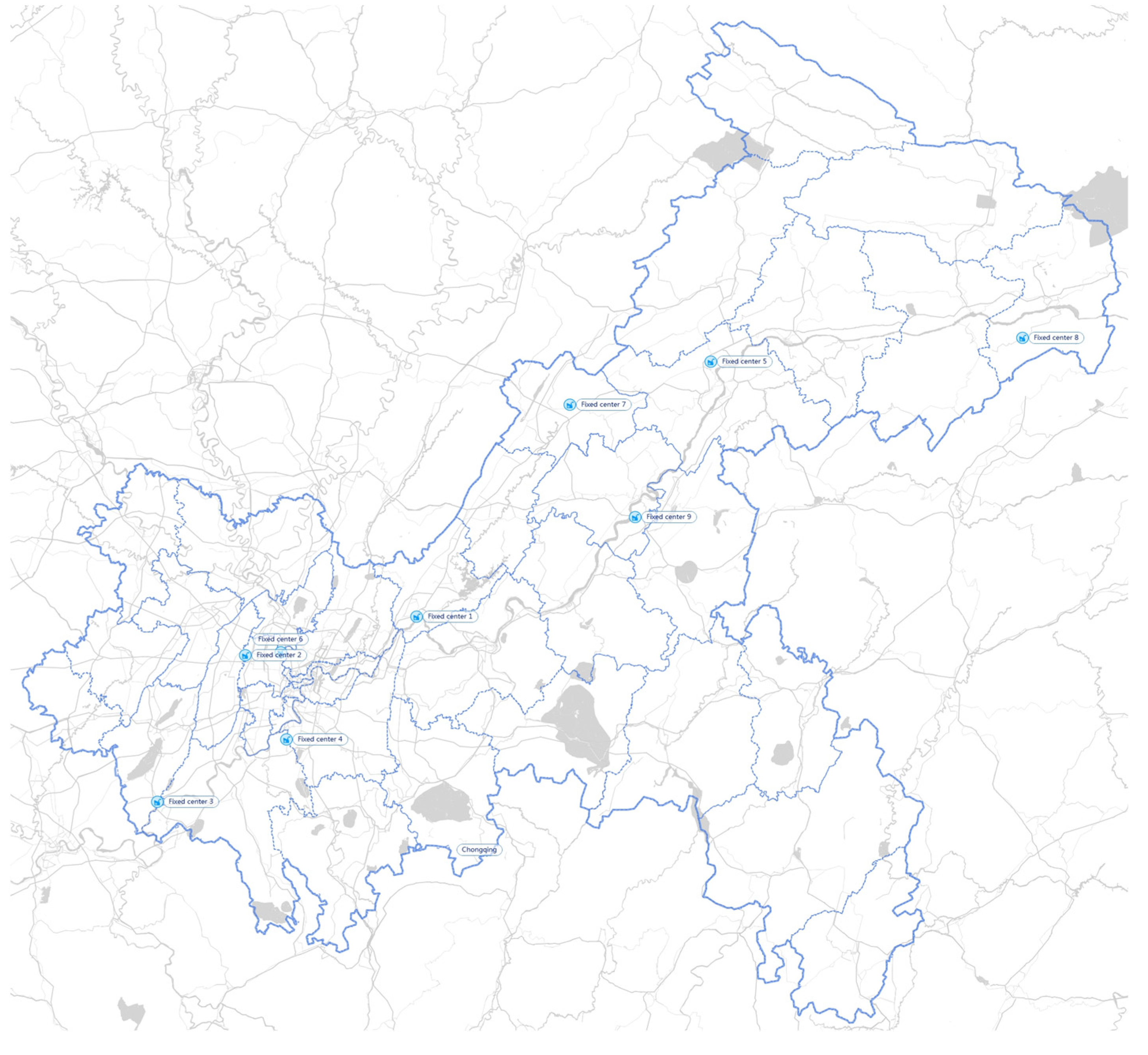
- The processing capacity of FPC is definite. In addition, FPCs and MPCs both have partial storage capability, which is also definite.
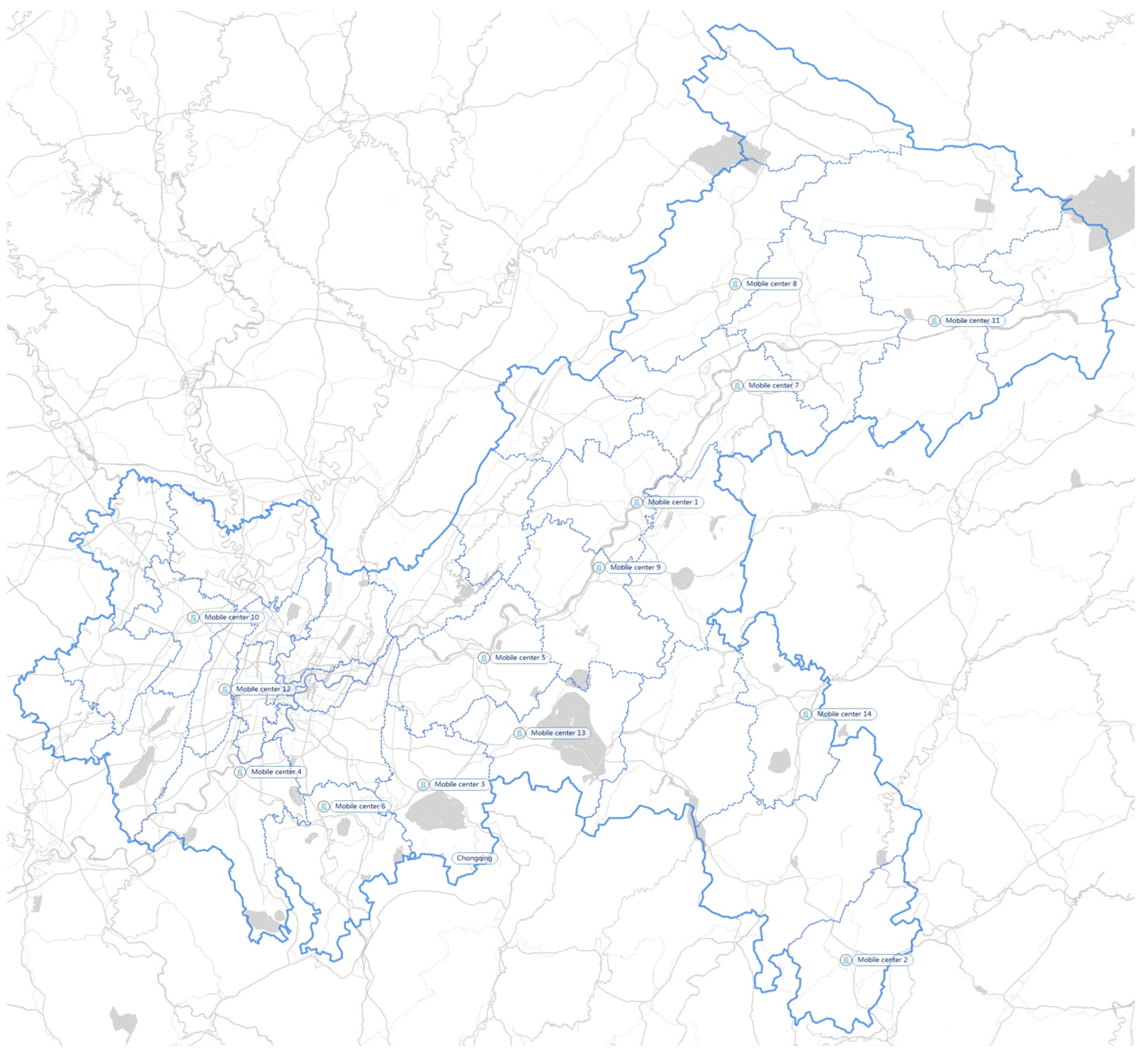
- The processing capacity of MPC is proportional to the number of mobile processing facilities. One MPC can accommodate a definite number of mobile processing facilities.
- To improve efficiency, all IMW are transported to the storage centers with no storage in IMW generation centers.
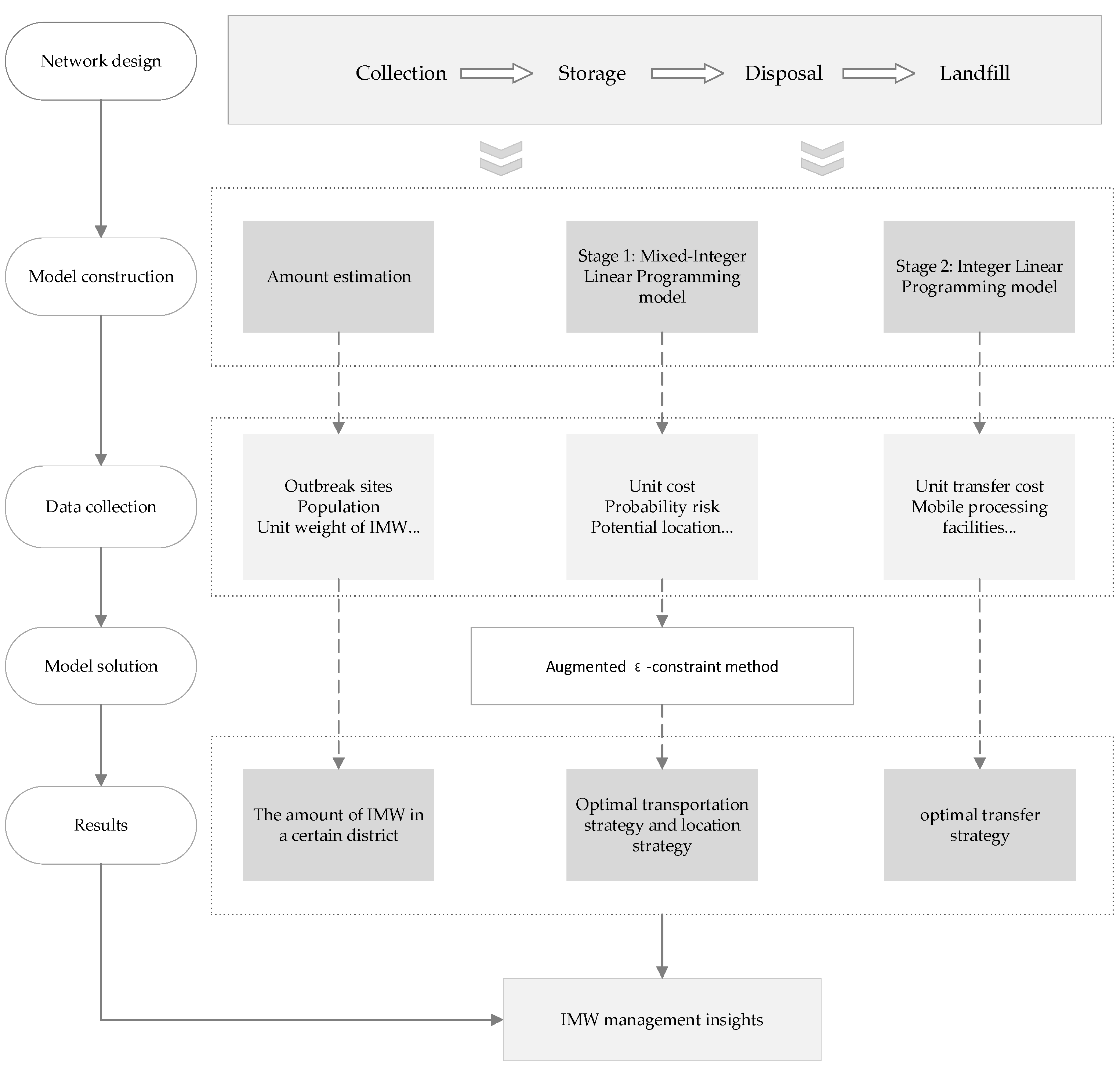
2.2. Model Construction
- First stage: produces demand distribution of different mobile devices.
- The location of storage centers, MPCs, and FPCs;
- The demand flow speed between each center;
- The number of mobile processing facilities in each MPC.
- 2.
- Second stage: generates corresponding mobile scheme, according to demand distribution in different outbreak situations.
- The number of mobile processing facilities transferred between MPCs;
- The path of transferring mobile processing facilities.
| Indices | |
| c | IMW generation center |
| s | IMW storage center |
| i | IMW FPC |
| j | IMW MPC |
| t | outbreaks at different times |
| Parameters | |
| the amount of IMW produced by IMW generation center c in the time t | |
| fixed operating cost for FPC i | |
| fixed operating cost for MPC j | |
| fixed operating cost for storage center s | |
| unit processing cost for FPC i | |
| unit processing cost for MPC j | |
| unit processing cost for storage center s | |
| cost of disassembly and installation for each mobile processing facility | |
| procurement cost for each mobile processing facility | |
| unit transportation cost using IMW transfer vehicle | |
| unit transportation cost for transferring a mobile processing facility | |
| distance from IMW generation center c to storage center s | |
| distance from storage center s to FPC i | |
| distance from storage center s to MPC j | |
| distance from MPC j’ to MPC j | |
| maximum capacity of storage center s | |
| maximum capacity of FPC i | |
| maximum capacity of each mobile processing facility | |
| maximum number of mobile processing facility accommodated in each MPC j | |
| risk of infection around storage centers | |
| risk of infection around FPCs | |
| risk of infection around MPCs | |
| risk of infection during transportation | |
| population exposure on the route from IMW generation center c to storage center s | |
| population exposure on the route from storage center s to FPC i | |
| population exposure on the route from storage center s to MPC j | |
| population exposure around storage center s | |
| population exposure around FPC i | |
| population exposure around MPC j | |
| upper limit for the storage time of IMW in the storage center | |
| Decision Variables | |
| 0/1 variable for selection of MPC j in the time t | |
| 0/1 variable for selection of FPC i in the time t | |
| 0/1 variable for selection of storage center s in the time t | |
| the number of mobile processing facilities in the MPC j in the time t | |
| the number of newly acquired mobile processing facilities in MPC j in the time t | |
| the number of mobile processing facilities that move from MPC j to MPC j’ at the end of the time t | |
| the flow rate of IMW transferred from IMW generation center c to storage center s in the time t | |
| the flow rate of IMW transferred from storage center s to FPC i in the time t | |
| the flow rate of IMW transferred from storage center s to MPC j in the time t | |
2.3. Model Solution
2.3.1. Amount Estimation
- The amount of basic IMW before the outbreak;
- The steep increase in the number of protective suits for health workers, COVID-19 tests, vaccination, and treatment of infected patients after the outbreak.
| Parameters | |
| district where IMW generation center c is located | |
| total population in district d | |
| total population of medical staff in district d | |
| the number of confirmed cases in district d | |
| average PPE’ s weight per worker | |
| the weight of items for one COVID-19 test | |
| the weight of basic IMW, such as masks per person, before outbreak | |
| the weight of IMW produced by treating an infected patient | |
| acceptance rate of PPE before outbreak | |
| acceptance rate of PPE after outbreak | |
| acceptance rate of COVID-19 tests before outbreak | |
| acceptance rate of COVID-19 tests after outbreak | |
| 1 if district d breaks out the pandemic, 0 otherwise |
2.3.2. Linearization
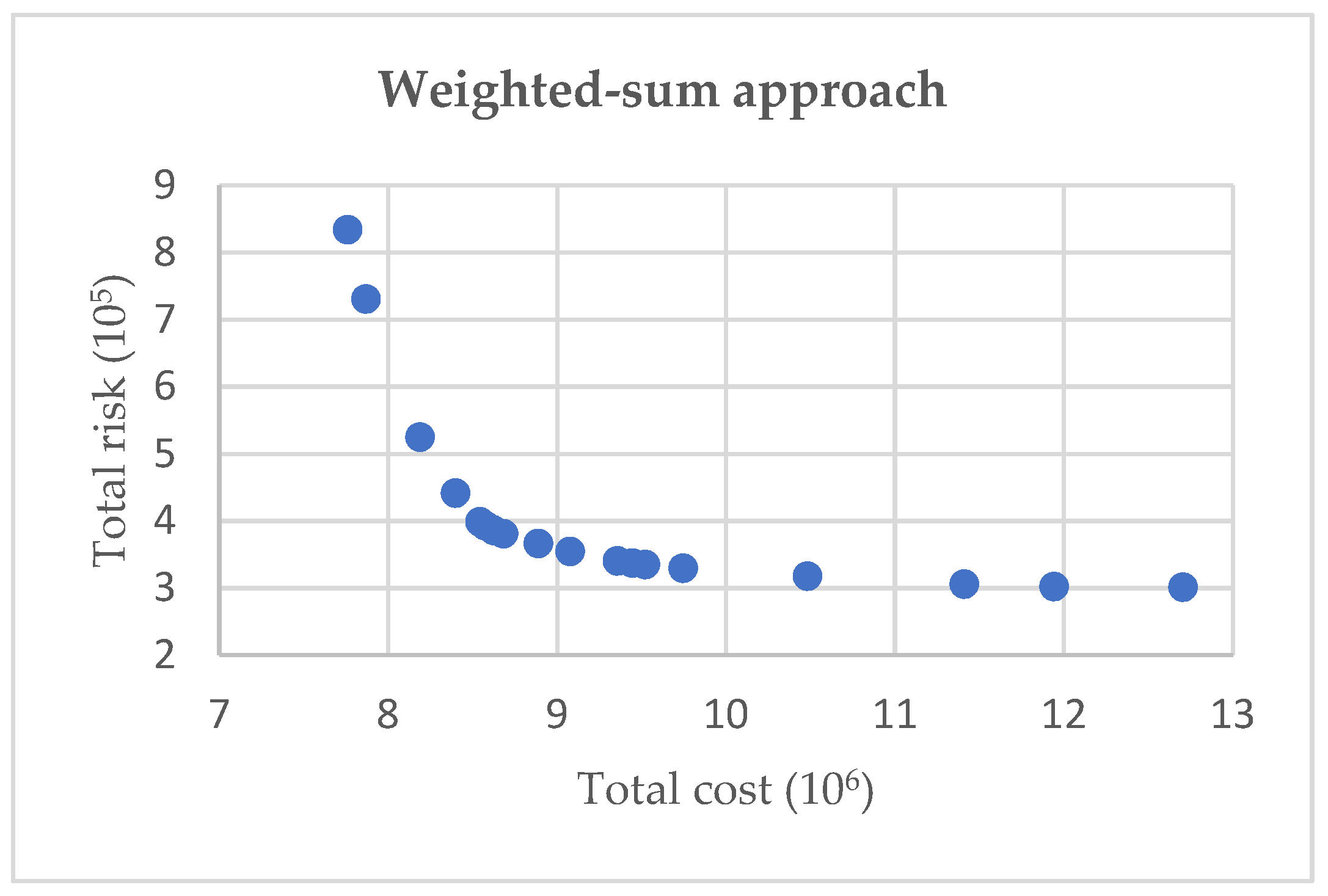
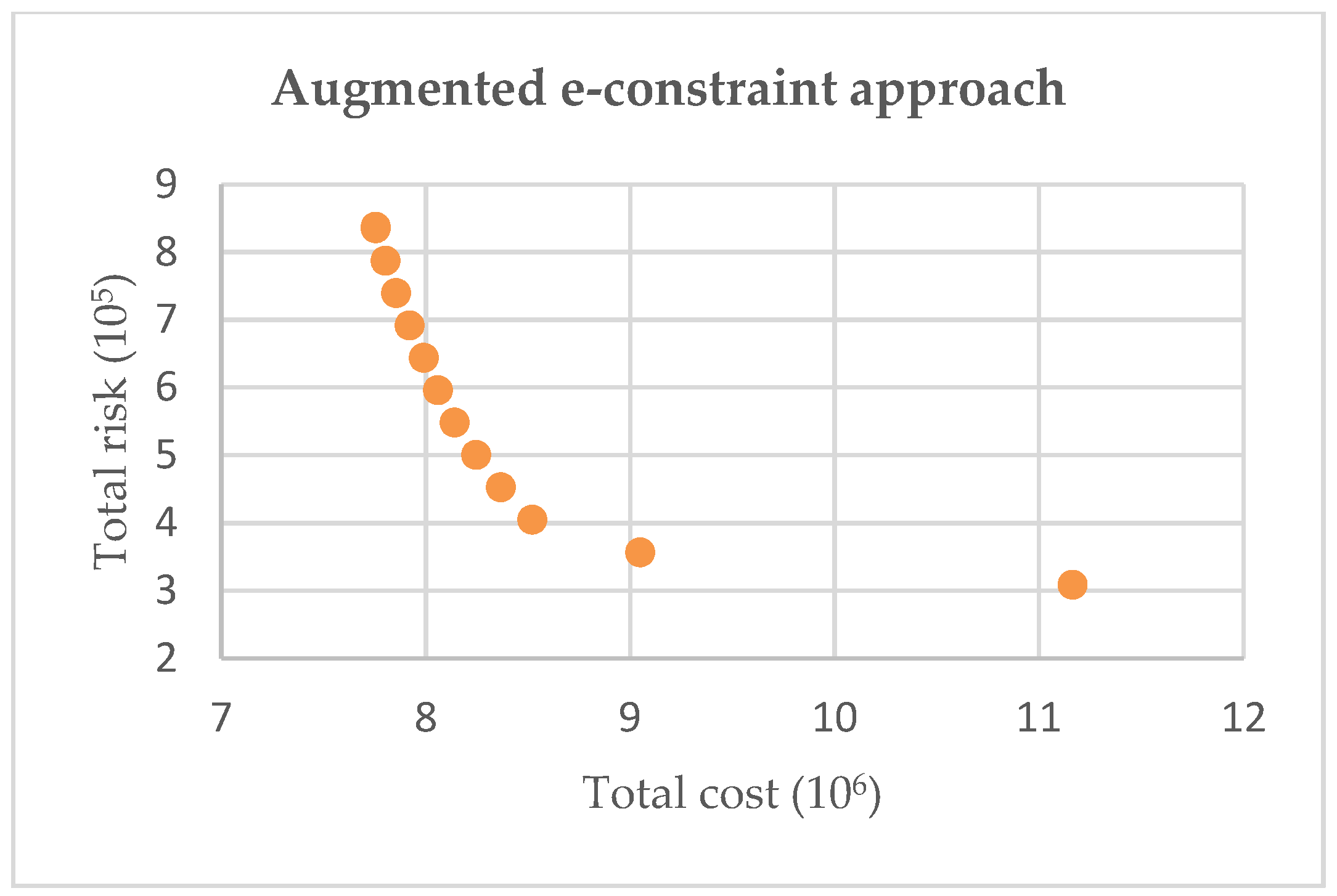
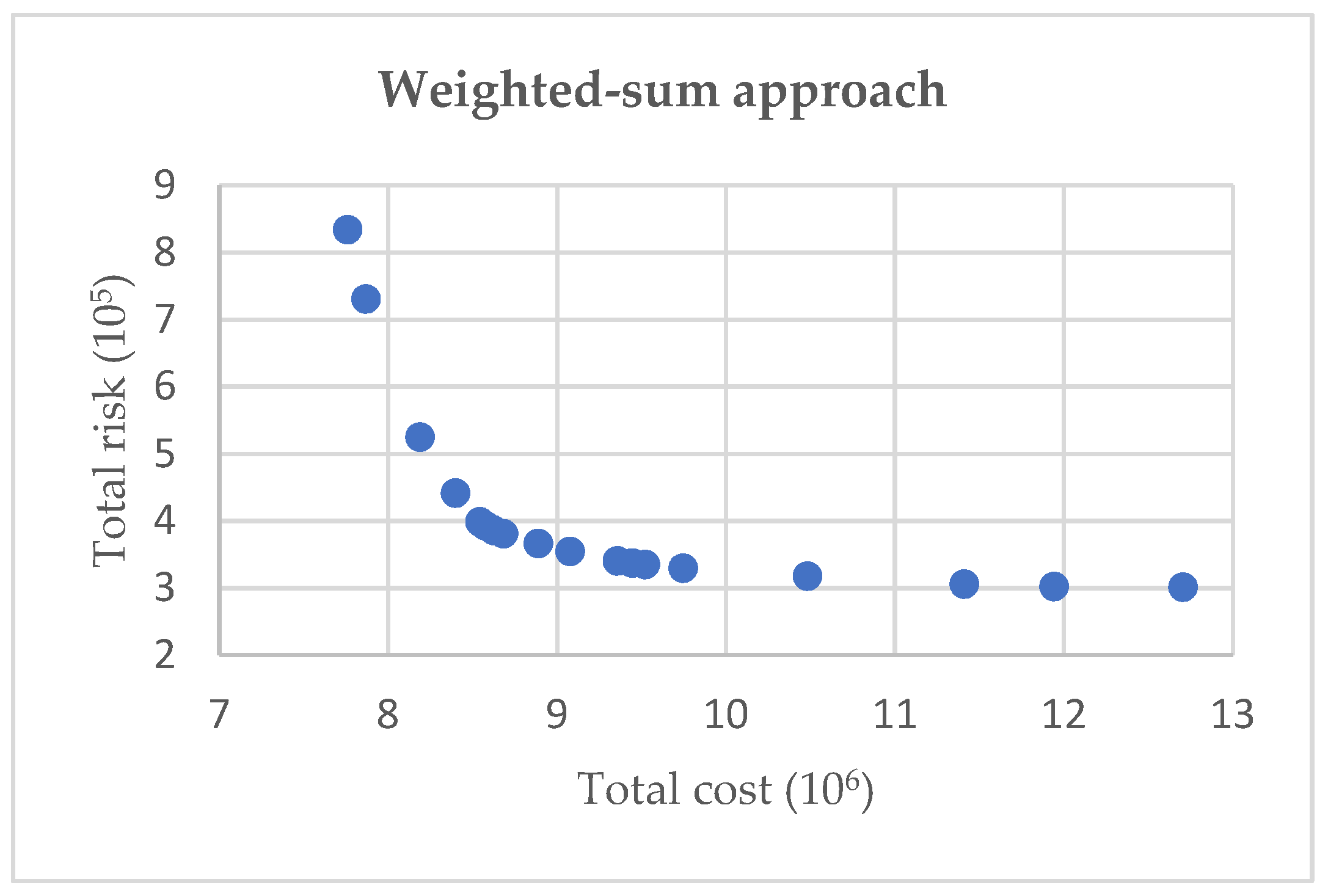
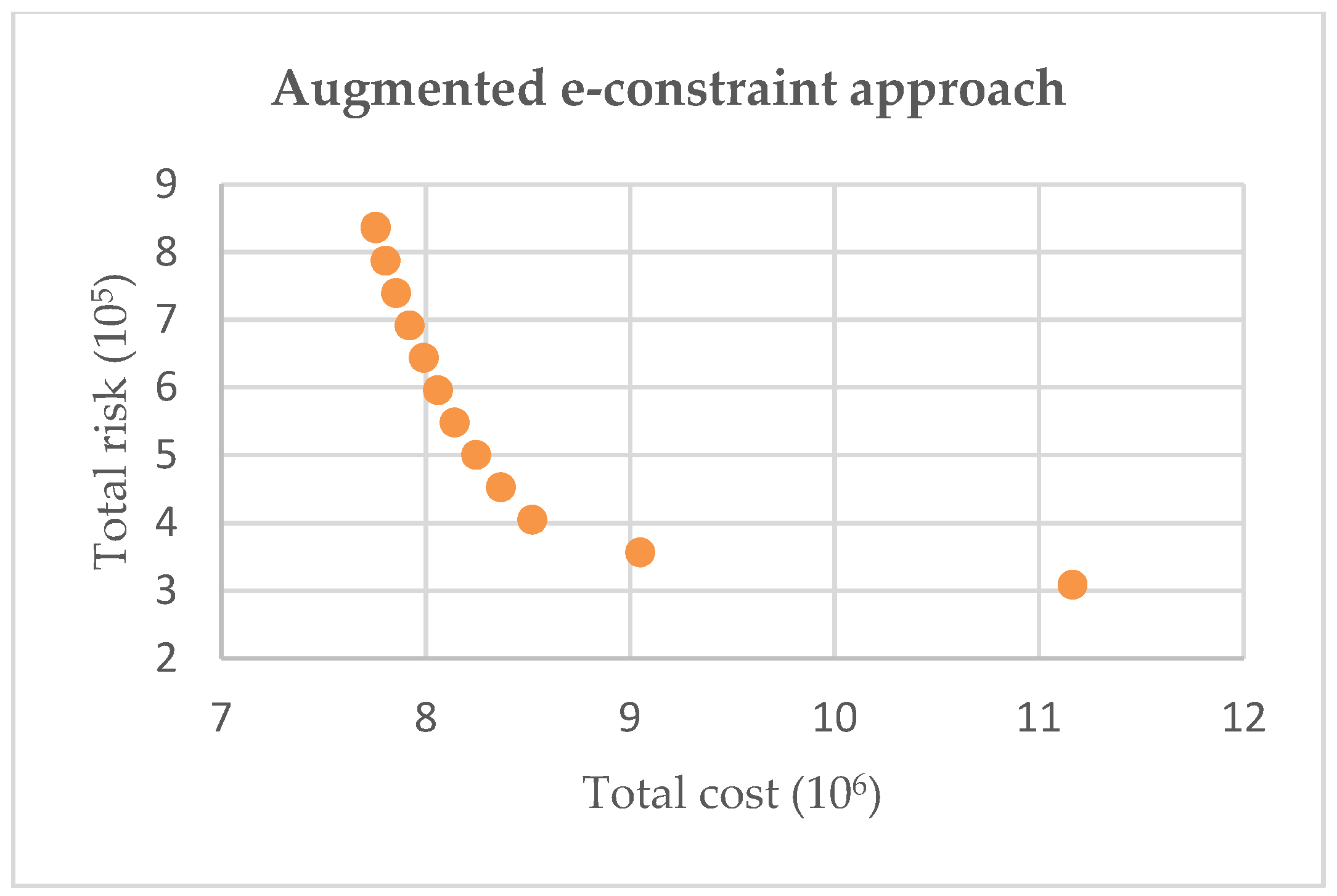
2.3.3. Augmented ε-Constraint Method
2.4. Data Collection
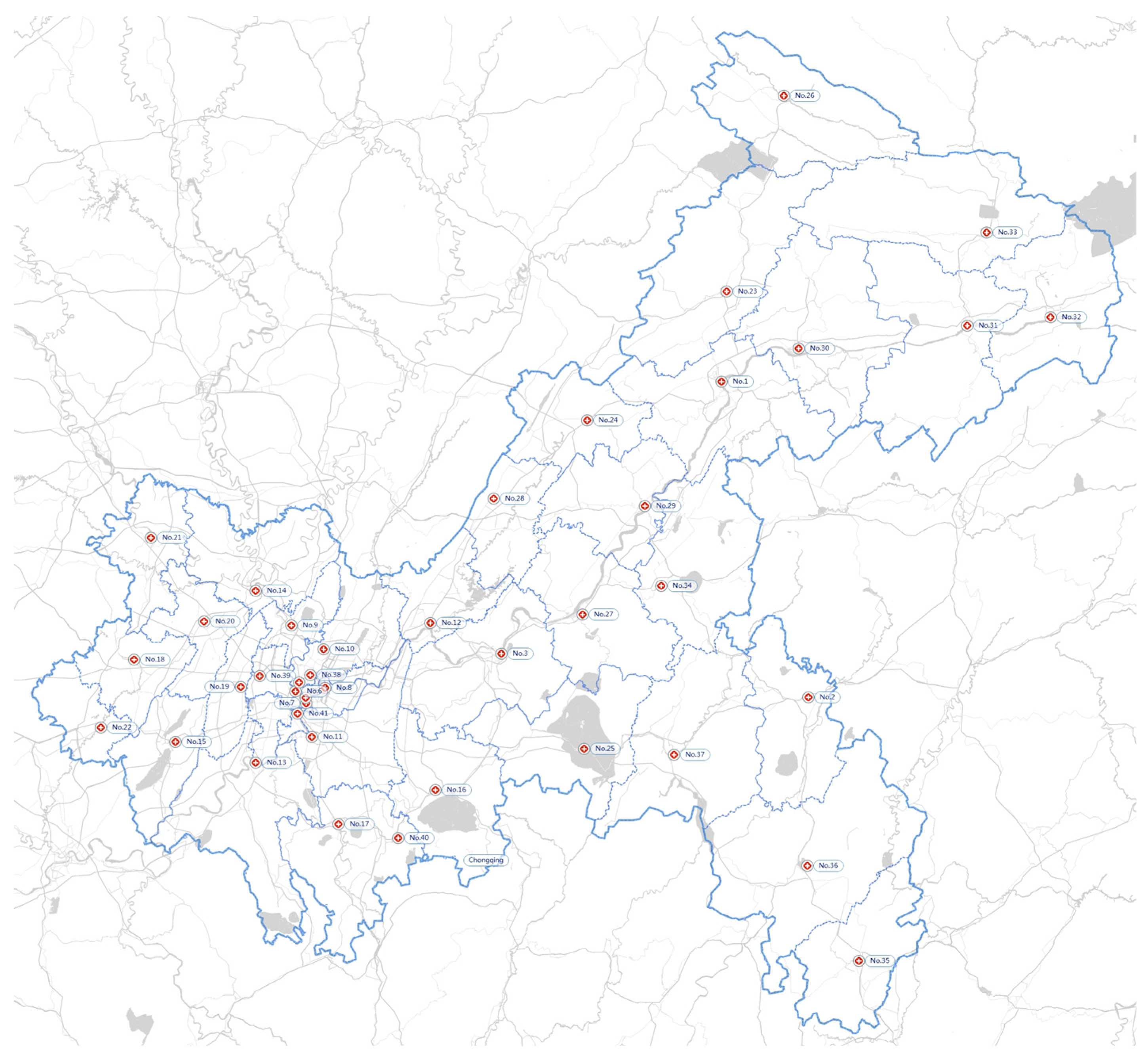
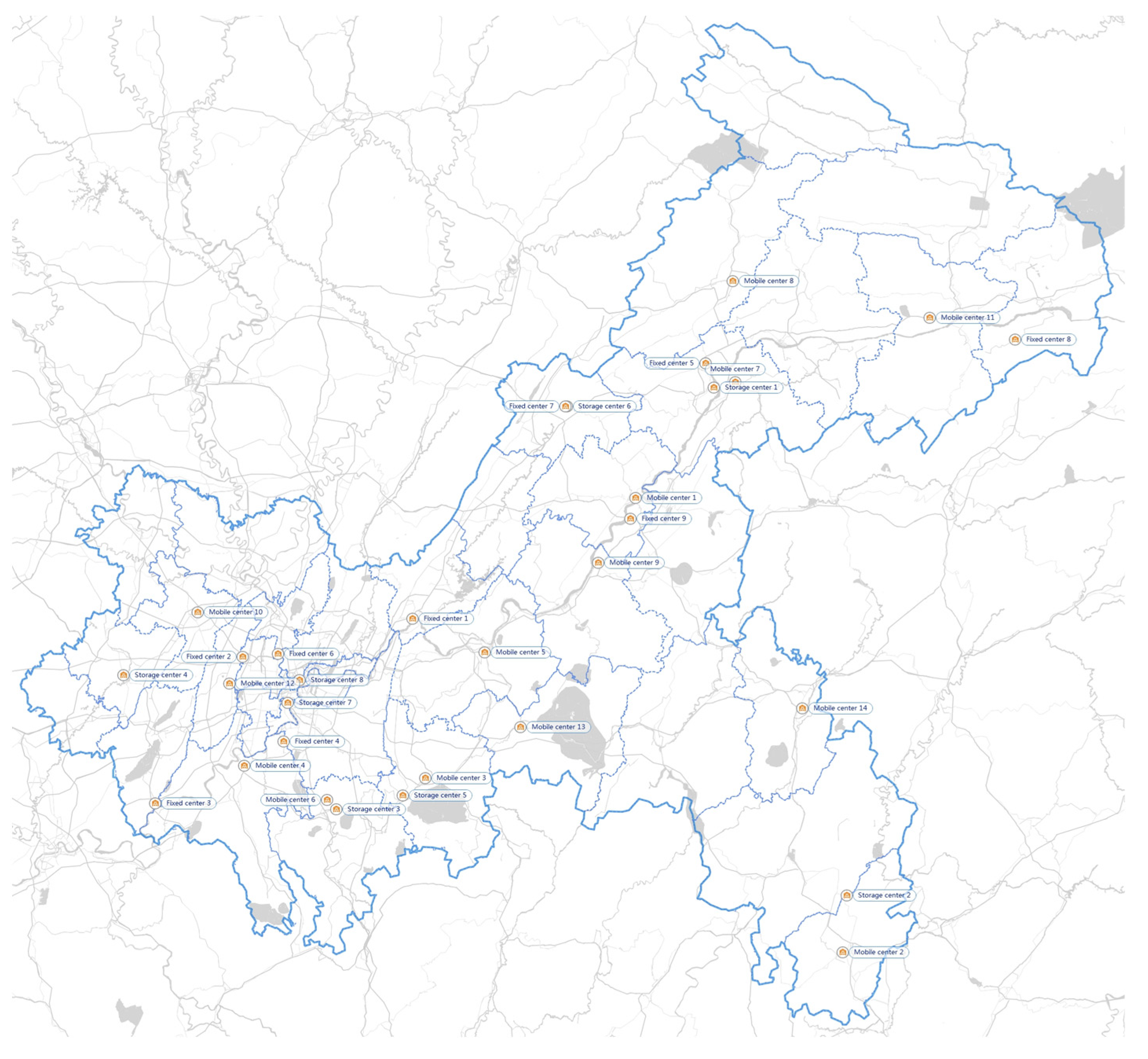
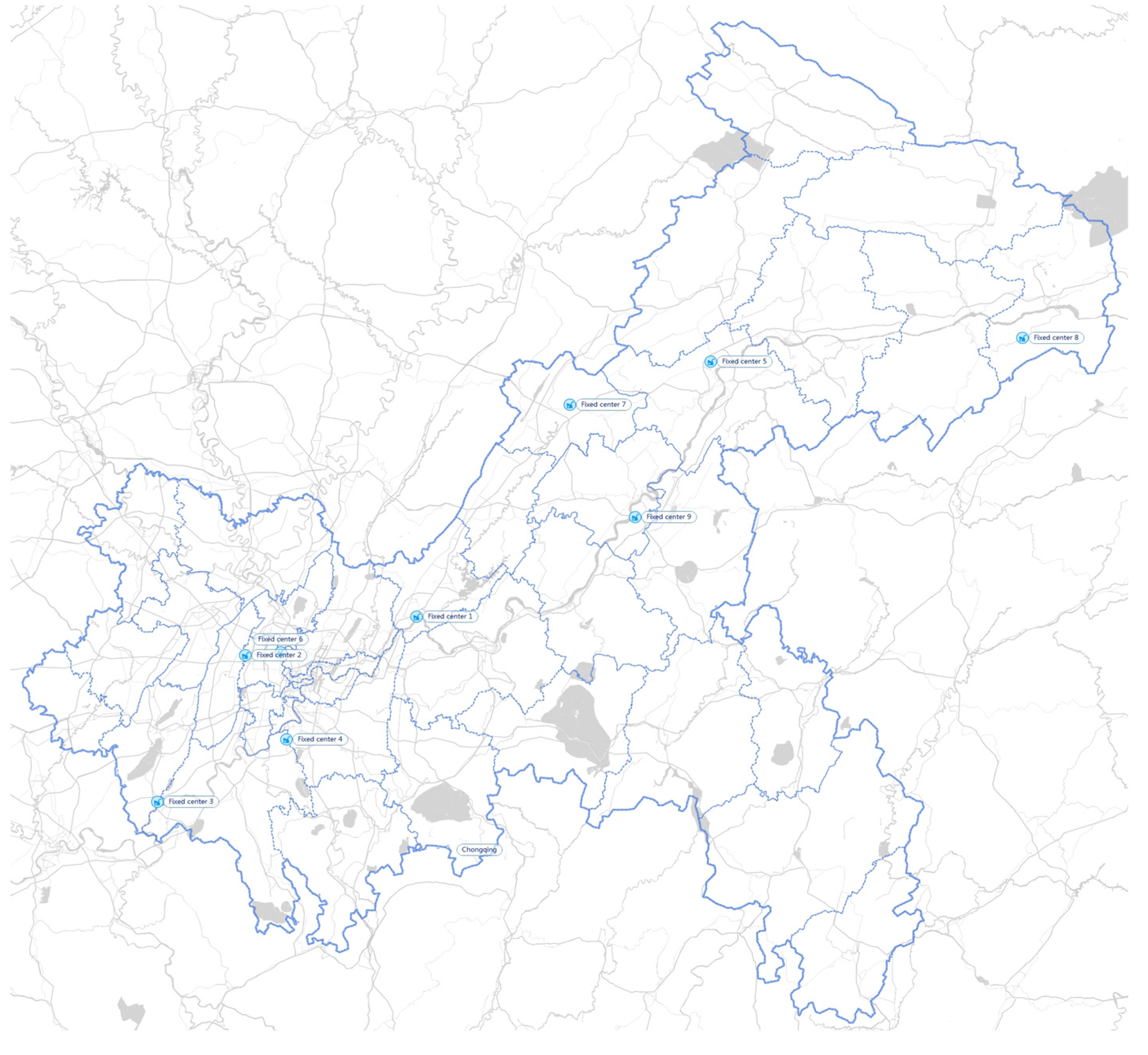
2.4.1. Data on Locations
2.4.2. Data on Estimation of IMW’s Generation
2.4.3. Data on Risks
2.4.4. Data on the Rest Parameters
3. Results and Discussions
3.1. Sensitivity Analysis
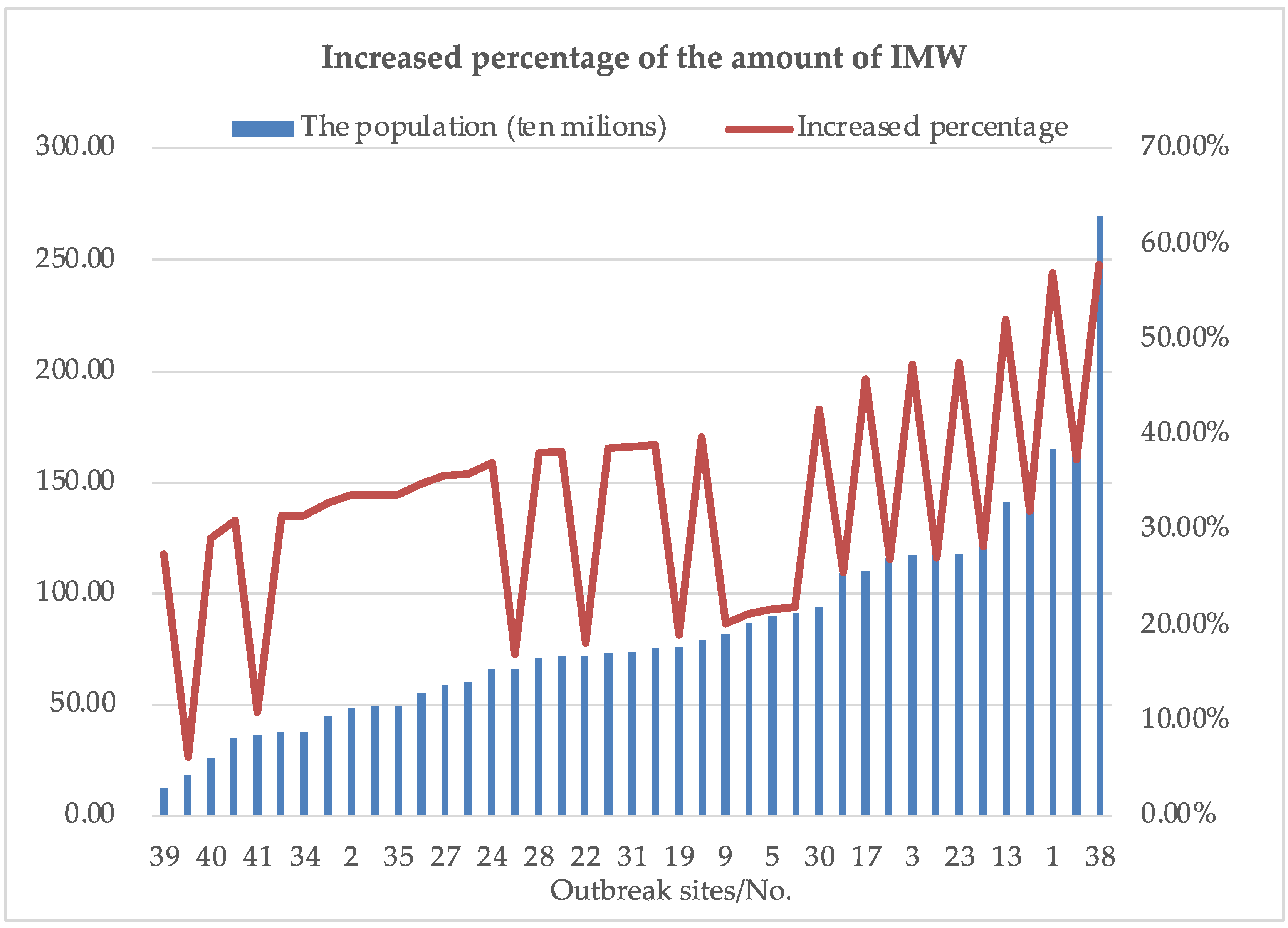
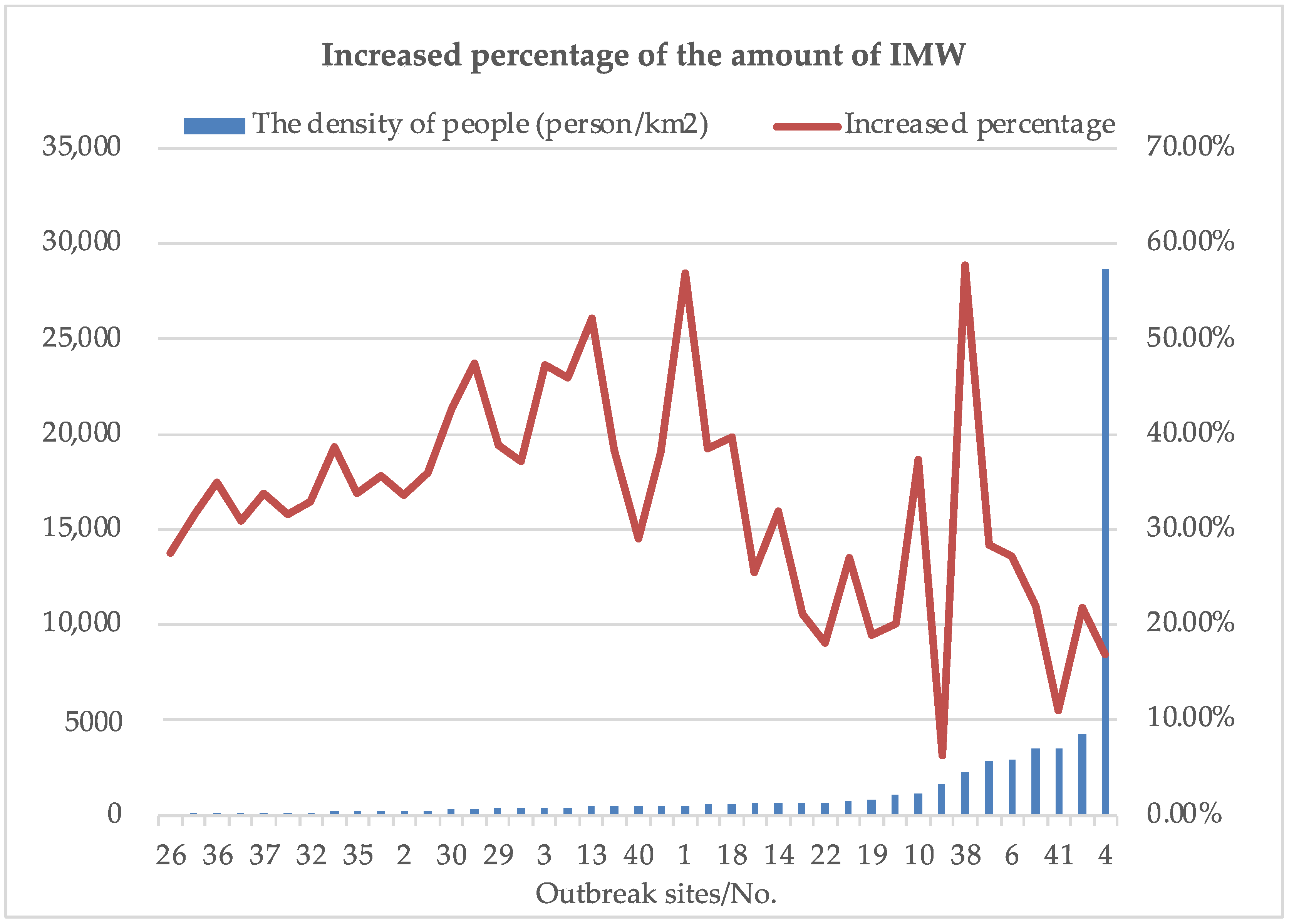
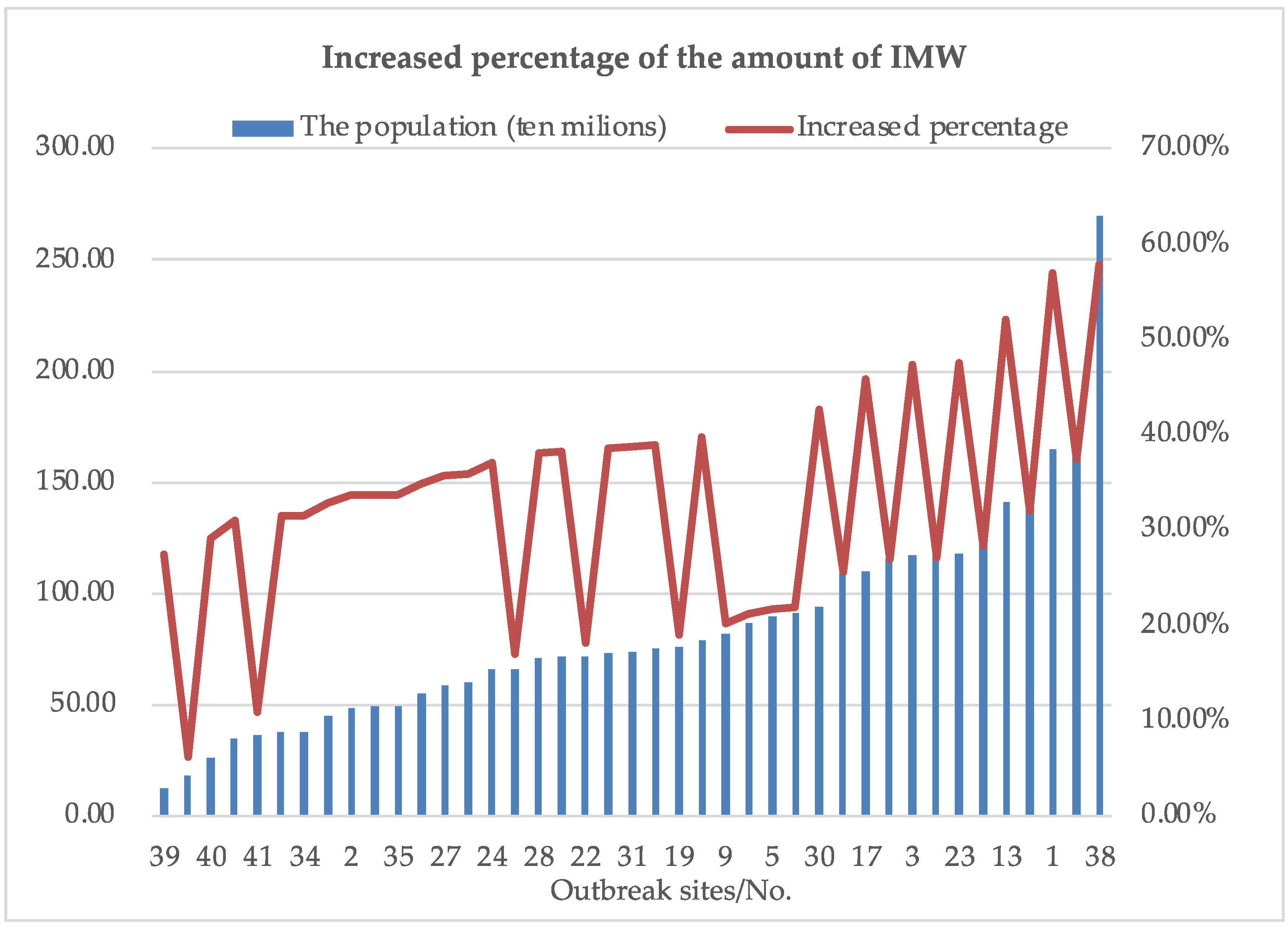
3.1.1. For Outbreak Sites
3.1.2. For Capacity and Cost of Mobile Processing Facility
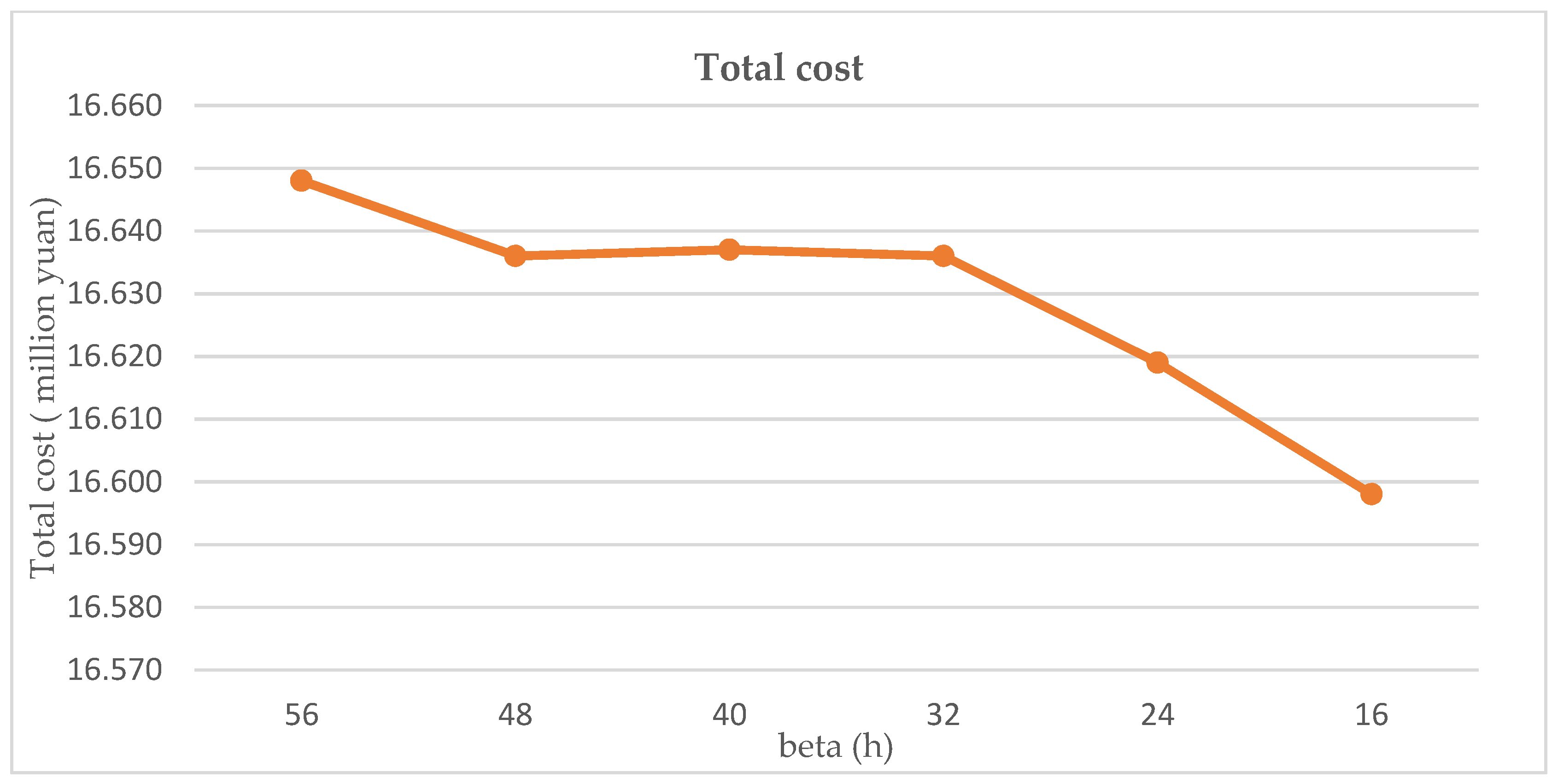
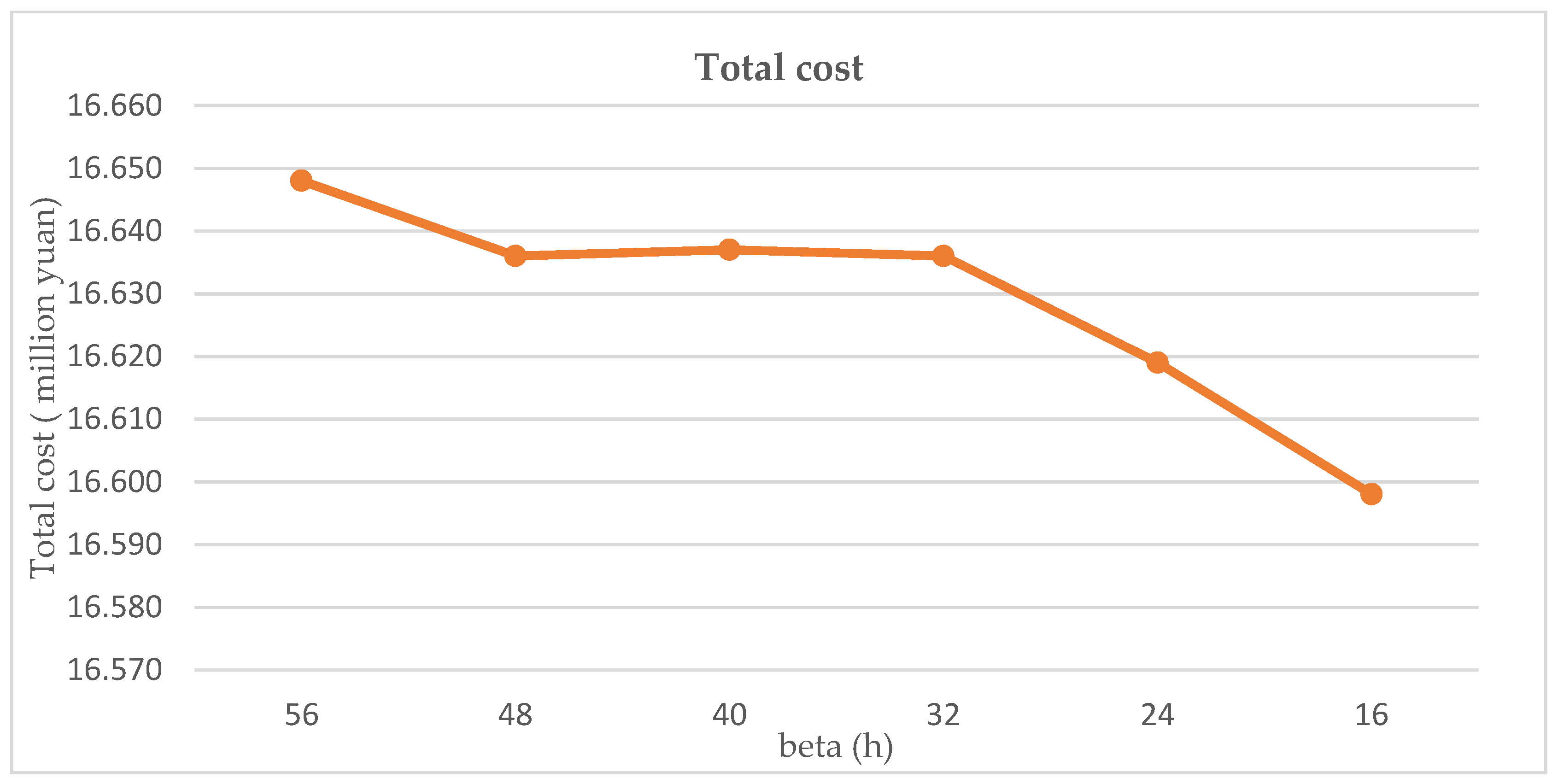
3.1.3. For Time Limit
- The various branches of government need to work together: The public construction department should fully consider the location and function of the processing centers in combination with the actual situation when planning. The financial department should give financial and policy support to the businesses that produce and sell small and mobile processing facilities. The supervision department should supervise the management and treatment of IMW by hospitals and processing institutions, avoiding them disregarding risks for reducing costs. The pandemic prevention and control department should flexibly adjust prevention and control policies, focusing on areas with large populations and high population density.
- The public hospitals are the source of IMW generation and bear the costs and risks in the collection and storage process. Timeliness can greatly reduce the risk of infection. The storage time limit can be set more flexibly. If the storage cost is relatively low, the storage time could be appropriately extended to reduce the total cost. If the processing cost is relatively low, the storage time could be appropriately shortened to reduce the total risk. The public hospitals can flexibly adjust the time limit according to the actual situation of the pandemic to balance the costs and risks.
- Small and mobile processing facilities can greatly respond to emergencies. IMW can be managed more efficiently. The disposal institution can develop new businesses, build MPCs with smaller unit scale and wider distribution, and purchase mobile processing facilities for decentralized processing. Since the capacity and cost of mobile processing facilities have a greater impact on the total cost of the network, disposal institutions should choose mobile processing facilities with appropriate capacity according to their own business conditions and pandemic situation. Multiple disposal institutions can also collaborate to flexibly move facilities based on actual outbreaks to improve facility utilization.
- In addition to just-in-time transportation of IMW, the third-party logistics providers can also operate the transfer business of mobile processing facilities. Some third-party logistics providers can even combine transshipment and processing operations to operate mobile IMW incinerators. In these transportation links, the choice of the route is the key to saving costs, and the third-party logistics provider should choose the globally optimal route.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hao, X.; Cheng, S.; Wu, D.; Wu, T.; Lin, X.; Wang, C. Reconstruction of the full transmission dynamics of COVID-19 in Wuhan. Nature 2020, 584, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Adeloye, D.; Elneima, O.; Daines, L.; Poinasamy, K.; Quint, J.K.; Walker, S.; Brightling, C.E.; Siddiqui, S.; Hurst, J.R.; Chalmers, J.D.; et al. The long-term sequelae of COVID-19: An international consensus on research priorities for patients with pre-existing and new-onset airways disease. Lancet Respir. Med. 2021, 9, 1467–1478. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 24 December 2020).
- WHO. WHO COVID-19 Dashboard. 2021. Available online: https://covid19.who.int (accessed on 24 December 2020).
- Kristoffersen, A.E.; van der Werf, E.T.; Stub, T.; Musial, F.; Wider, B.; Jong, M.C.; Wode, K.; Danell, J.-A.B.; Busch, M.; Hoenders, H.R.; et al. Consultations with health care providers and use of self-management strategies for prevention and treatment of COVID-19 related symptoms. A population based cross-sectional study in Norway, Sweden and the Netherlands. Complement. Ther. Med. 2021, 64, 102792. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.Z. Thoughts on the outbreak phases of the COVID-19 changed from emergency response to the combination of emergent response and regular prevention and control activities. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 806–808. [Google Scholar]
- Central People’s Government of the People’s Republic of China. Guiding Opinions of the State Council’s Joint Prevention and Control Mechanism for Novel Coronavirus Pneumonia Epidemic. Available online: http://www.gov.cn/zhengce/content/2020-05/08/content_5509896.htm (accessed on 8 May 2020).
- Al-Omran, K.; Khan, E.; Ali, N.; Bilal, M. Estimation of COVID-19 generated medical waste in the Kingdom of Bahrain. Sci. Total Environ. 2021, 801, 149642. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chen, J.; Fang, R.; Ye, F.; Yang, Z.; Wang, Z.; Shi, F.; Tan, W. What medical waste management system may cope With COVID-19 pandemic: Lessons from Wuhan. Resour. Conserv. Recycl. 2021, 170, 105600. [Google Scholar] [CrossRef]
- Cutler, D.M.; Nikpay, S.; Huckman, R.S. The Business of Medicine in the Era of COVID-19. JAMA 2020, 323, 2003. [Google Scholar] [CrossRef]
- Chang, W.-H. The influences of the COVID-19 pandemic on medical service behaviors. Taiwan J. Obstet. Gynecol. 2020, 59, 821–827. [Google Scholar] [CrossRef]
- EPA. Medical Waste. Available online: https://www.epa.gov/rcra/medical-waste (accessed on 14 May 2022).
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251, Corrigendum in J. Hosp. Infect. 2020, 105, 587. [Google Scholar] [CrossRef] [Green Version]
- Saadat, S.; Rawtani, D.; Hussain, C.M. Environmental perspective of COVID-19. Sci. Total Environ. 2020, 728, 138870. [Google Scholar] [CrossRef]
- Sangkham, S. Face mask and medical waste disposal during the novel COVID-19 pandemic in Asia. Case Stud. Chem. Environ. Eng. 2020, 2, 100052. [Google Scholar] [CrossRef]
- Mol, M.P.G.; Caldas, S. Can the human coronavirus epidemic also spread through solid waste? Waste Manag. Res. 2020, 38, 485–486. [Google Scholar] [CrossRef] [PubMed]
- Windfeld, E.S.; Brooks, M.S.-L. Medical waste management—A review. J. Environ. Manag. 2015, 163, 98–108. [Google Scholar] [CrossRef]
- Bening, C.R.; Kahlert, S.; Asiedu, E. The true cost of solving the plastic waste challenge in developing countries: The case of Ghana. J. Clean. Prod. 2021, 330, 129649. [Google Scholar] [CrossRef]
- Thind, P.S.; Sareen, A.; Singh, D.D.; Singh, S.; John, S. Compromising situation of India’s bio-medical waste incineration units during pandemic outbreak of COVID-19: Associated environmental-health impacts and mitigation measures. Environ. Pollut. 2021, 276, 116621. [Google Scholar] [CrossRef] [PubMed]
- Lemma, H.; Asefa, L.; Gemeda, T.; Dhengesu, D. Infectious medical waste management during the COVID-19 pandemic in public hospitals of West Guji zone, southern Ethiopia. Clin. Epidemiol. Glob. Health 2022, 15, 101037. [Google Scholar] [CrossRef]
- Singh, D.; Aryan, Y.; Chavan, D.; Tembhare, M.; Dikshit, A.K.; Kumar, S. Mask consumption and biomedical waste generation rate during COVID-19 pandemic: A case study of central India. Environ. Res. 2022, 212 Pt C, 113363. [Google Scholar] [CrossRef]
- Shukor, F.S.A.; Mohammed, A.H.; Sani, S.I.A.; Awang, M. A review on the success factors for community participation in solid waste management. In Proceedings of the International Conference on Management, Athens, Greece, 12–16 June 2011. [Google Scholar]
- Bamakan, S.M.H.; Malekinejad, P.; Ziaeian, M. Towards blockchain-based hospital waste management systems; applications and future trends. J. Clean. Prod. 2022, 349, 131440. [Google Scholar] [CrossRef]
- Eydi, A.; Rastgar, S. A DEA model with dual-role factors and fuzzy data for selecting third-party reverse logistics provider, case study: Hospital waste collection. Ain Shams Eng. J. 2021, 13, 101561. [Google Scholar] [CrossRef]
- Zhao, H.; Liu, H.; Wei, G.; Zhang, N.; Qiao, H.; Gong, Y.; Yu, X.; Zhou, J.; Wu, Y. A review on emergency disposal and management of medical waste during the COVID-19 pandemic in China. Sci. Total Environ. 2021, 810, 152302. [Google Scholar] [CrossRef]
- Fernando, R.L.S. Solid waste management of local governments in the Western Province of Sri Lanka: An implementation analysis. Waste Manag. 2018, 84, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Dharmaraj, S.; Ashokkumar, V.; Pandiyan, R.; Munawaroh, H.S.H.; Chew, K.W.; Chen, W.-H.; Ngamcharussrivichai, C. Pyrolysis: An effective technique for degradation of COVID-19 medical wastes. Chemosphere 2021, 275, 130092. [Google Scholar] [CrossRef] [PubMed]
- UN Environment Program (UNEP). Practical Guidelines for the Handling, Storage and Disposal of COVID-19 Infected Wastes, Including Personnel Protective Equipment. [Guidelines]. Available online: https://www.humanitarianlibrary.org/sites/default/files/2020/06/UNEP_PRACTICAL%20GUIDELINE%20FOR%20COVID%2019%20WASTE%20MANAGEMENT%20UNEP-GSC-DOS.pdf (accessed on 3 April 2020).
- Wang, M.; Wood, L.C.; Wang, B. Transportation capacity shortage influence on logistics performance: Evidence from the driver shortage. Heliyon 2022, 8, e09423. [Google Scholar] [CrossRef]
- Kang, X.; Pang, H. City selection for fresh produce e-commerce’s market entry strategy: Based on the perspective of urban logistics competitiveness. Transp. Res. Interdiscip. Perspect. 2022, 13, 100537. [Google Scholar] [CrossRef]
- Wang, F.; Yang, X.; Zhuo, X.; Xiong, M. Joint logistics and financial services by a 3PL firm: Effects of risk preference and demand volatility. Transp. Res. Part E Logist. Transp. Rev. 2019, 130, 312–328. [Google Scholar] [CrossRef]
- Rześny-Cieplińska, J.; Szmelter-Jarosz, A.; Moslem, S. Priority-based stakeholders analysis in the view of sustainable city logistics: Evidence for Tricity, Poland. Sustain. Cities Soc. 2021, 67, 102751. [Google Scholar] [CrossRef]
- Kundu, T.; Sheu, J.-B.; Kuo, H.-T. Emergency logistics management—Review and propositions for future research. Transp. Res. Part E Logist. Transp. Rev. 2022, 164, 102789. [Google Scholar] [CrossRef]
- Maghfiroh, M.F.; Hanaoka, S. Dynamic truck and trailer routing problem for last mile distribution in disaster response. J. Humanit. Logist. Supply Chain Manag. 2018, 8, 252–278. [Google Scholar] [CrossRef]
- Nezhadroshan, A.M.; Fathollahi-Fard, A.M.; Hajiaghaei-Keshteli, M. A scenario-based possibilistic-stochastic programming approach to address resilient humanitarian logistics considering travel time and resilience levels of facilities. Int. J. Syst. Sci. Oper. Logist. 2020, 8, 321–347. [Google Scholar] [CrossRef]
- Yáñez-Sandivari, L.; Cortés, C.E.; Rey, P.A. Humanitarian logistics and emergencies management: New perspectives to a sociotechnical problem and its optimization approach management. Int. J. Disaster Risk Reduct. 2020, 52, 101952. [Google Scholar] [CrossRef]
- Wang, Y.; Ran, L.; Guan, X.; Fan, J.; Sun, Y.; Wang, H. Collaborative multicenter vehicle routing problem with time windows and mixed deliveries and pickups. Expert Syst. Appl. 2022, 197, 116690. [Google Scholar] [CrossRef]
- Kafiabad, S.T.; Zanjani, M.K.; Nourelfath, M. Robust collaborative maintenance logistics network design and planning. Int. J. Prod. Econ. 2021, 244, 108370. [Google Scholar] [CrossRef]
- Hribernik, M.; Zero, K.; Kummer, S.; Herold, D.M. City logistics: Towards a blockchain decision framework for collaborative parcel deliveries in micro-hubs. Transp. Res. Interdiscip. Perspect. 2020, 8, 100274. [Google Scholar] [CrossRef]
- Rogers, D.S.; Tibben-Lembke, R.S. Going Backwards: Reverse Logistics Trends and Practices; Reverse Logistics Executive Council: Pittsburgh, PA, USA, 1999. [Google Scholar]
- Qiu, Y.; Ni, M.; Wang, L.; Li, Q.; Fang, X.; Pardalos, P.M. Production routing problems with reverse logistics and remanufacturing. Transp. Res. Part E Logist. Transp. Rev. 2018, 111, 87–100. [Google Scholar] [CrossRef]
- Rahimi, M.; Ghezavati, V. Sustainable multi-period reverse logistics network design and planning under uncertainty utilizing conditional value at risk (CVaR) for recycling construction and demolition waste. J. Clean. Prod. 2018, 172, 1567–1581. [Google Scholar] [CrossRef]
- Govindan, K.; Gholizadeh, H. Robust network design for sustainable-resilient reverse logistics network using big data: A case study of end-of-life vehicles. Transp. Res. Part E Logist. Transp. Rev. 2021, 149, 102279. [Google Scholar] [CrossRef]
- Budak, A.; Ustundag, A. Reverse logistics optimisation for waste collection and disposal in health institutions: The case of Turkey. Int. J. Logist. Res. Appl. 2016, 20, 322–341. [Google Scholar] [CrossRef]
- Yu, H.; Sun, X.; Solvang, W.D.; Zhao, X. Reverse Logistics Network Design for Effective Management of Medical Waste in Epidemic Outbreaks: Insights from the Coronavirus Disease 2019 (COVID-19) Outbreak in Wuhan (China). Int. J. Environ. Res. Public Health 2020, 17, 1770. [Google Scholar] [CrossRef] [Green Version]
- Kargar, S.; Pourmehdi, M.; Paydar, M.M. Reverse logistics network design for medical waste management in the epidemic outbreak of the novel coronavirus (COVID-19). Sci. Total Environ. 2020, 746, 141183. [Google Scholar] [CrossRef]
- Eren, E.; Tuzkaya, U.R. Safe distance-based vehicle routing problem: Medical waste collection case study in COVID-19 pandemic. Comput. Ind. Eng. 2021, 157, 107328. [Google Scholar] [CrossRef]
- Govindan, K.; Nasr, A.K.; Mostafazadeh, P.; Mina, H. Medical waste management during coronavirus disease 2019 (COVID-19) outbreak: A mathematical programming model. Comput. Ind. Eng. 2021, 162, 107668. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.-L.; Liang, K.-C. Fuzzy logic programming and adaptable design of medical products for the COVID-19 anti-epidemic normalization. Comput. Methods Programs Biomed. 2020, 197, 105762. [Google Scholar] [CrossRef] [PubMed]
- P.R.C. Regulation on Administration of Medical Waste. Available online: http://www.gov.cn/gongbao/content/2011/content_1860802.htm (accessed on 8 January 2011).
- Yong, Z.; Gang, X.; Guanxing, W.; Tao, Z.; Dawei, J. Medical waste management in China: A case study of Nanjing. Waste Manag. 2009, 29, 1376–1382. [Google Scholar] [CrossRef]
- Insa, E.; Zamorano, M.; López, R. Critical review of medical waste legislation in Spain. Resour. Conserv. Recycl. 2010, 54, 1048–1059. [Google Scholar] [CrossRef]
- Lee, B.-K.; Ellenbecker, M.J.; Moure-Ersaso, R. Alternatives for treatment and disposal cost reduction of regulated medical wastes. Waste Manag. 2004, 24, 143–151. [Google Scholar] [CrossRef] [PubMed]
- He, Z.-G.; Li, Q.; Fang, J. The Solutions and Recommendations for Logistics Problems in the Collection of Medical Waste in China. Procedia Environ. Sci. 2016, 31, 447–456. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.C.; Taskin, Z.C. Tutorial Guide to Mixed-Integer Programming Models and Solution Techniques. Optim. Med. Biol. 2008, 521–548. [Google Scholar] [CrossRef] [Green Version]
- Aalaei, A.; Davoudpour, H. Revised multi-choice goal programming for incorporated dynamic virtual cellular manufacturing into supply chain management: A case study. Eng. Appl. Artif. Intell. 2016, 47, 3–15. [Google Scholar] [CrossRef]
- Haimes, Y.Y.; Lasdon, L.S.; Wismer, D.A. On a Bicriterion Formulation of the Problems of Integrated System Identification and System Optimization. IEEE Trans. Syst. Man Cybern. 1971, 1, 296–297. [Google Scholar]
- Mavrotas, G.; Florios, K. An improved version of the augmented ε-constraint method (AUGMECON2) for finding the exact pareto set in multi-objective integer programming problems. Appl. Math. Comput. 2013, 219, 9652–9669. [Google Scholar] [CrossRef]
- Bao, H.X.H.; Li, L.; Lizieri, C. City profile: Chongqing (1997–2017). CITIES 2019, 94, 161–171. [Google Scholar] [CrossRef]
- Zhuang, T.; Qian, Q.K.; Visscher, H.J.; Elsinga, M.G. An analysis of urban renewal decision-making in China from the perspective of transaction costs theory: The case of Chongqing. Neth. J. Hous. Built Environ. 2020, 35, 1177–1199. [Google Scholar] [CrossRef] [Green Version]
- National Health Commission of the People’s Republic of China. National Medical Institution Inquiry. Available online: http://zgcx.nhc.gov.cn:9090/unit (accessed on 31 July 2022).
- Chongqing Municipal Bureau of Ecology, People’s Republic of China. The Issuance of Hazardous Waste Business Licenses in Chongqing. Available online: http://sthjj.cq.gov.cn/zwgk_249/gszx/wxfwjyxkzgs/202110/t20211015_9809345.html (accessed on 30 September 2021).
- Chongqing Municipal Bureau of Statistics of the People’s Republic of China. Chongqing Statistical Yearbook Calendar Year Download (In Chinese). Available online: http://tjj.cq.gov.cn/zwgk_233/tjnj/202012/t20201214_8606164.html (accessed on 4 September 2021).
- Purnomo, C.W.; Kurniawan, W.; Aziz, M. Technological review on thermochemical conversion of COVID-19-related medical wastes. Resour. Conserv. Recycl. 2021, 167, 105429. [Google Scholar] [CrossRef] [PubMed]
- Celis, J.E.; Espejo, W.; Paredes-Osses, E.; Contreras, S.A.; Chiang, G.; Bahamonde, P. Plastic residues produced with confirmatory testing for COVID-19: Classification, quantification, fate, and impacts on human health. Sci. Total Environ. 2020, 760, 144167. [Google Scholar] [CrossRef] [PubMed]
- ADB. Managing Infectious Medical Waste during the COVID-19 Pandemic.2. Available online: https://www.adb.org/publications/managing-medical-waste-covid19 (accessed on 7 April 2020).
- Korkut, E.N. Estimations and analysis of medical waste amounts in the city of Istanbul and proposing a new approach for the estimation of future medical waste amounts. Waste Manag. 2018, 81, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Huang, L.; Lee, D.-H.; Peng, Q. Improved approaches to the network design problem in regional hazardous waste management systems. Transp. Res. Part E Logist. Transp. Rev. 2016, 88, 52–75. [Google Scholar] [CrossRef]
- Chen, Y.; Guo, C. Handbook of Emergency Disposal and Management of Medical Waste in China; Basel Convention Regional Centre for Asia and the Pacific: Beijing, China, 2020. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Generation Center | Population | Population Density (People/km2) | Medical Staff (People) |
|---|---|---|---|---|
| 1 | Wanzhou | 165 | 477.8 | 11,429 |
| 2 | Qianjiang | 49 | 205 | 3359 |
| 3 | Fuling | 117 | 397.8 | 8104 |
| 4 | Yuzhong | 66 | 28,695.7 | 4572 |
| 5 | Jiangbei | 90 | 4306.2 | 6234 |
| 6 | Shapingba | 117 | 2954.5 | 8104 |
| 7 | Jiulongpo | 123 | 2853.8 | 8520 |
| 8 | Nanan | 91 | 3475.2 | 6303 |
| 9 | Beibei | 82 | 1091.9 | 5680 |
| 10 | Yubei | 168 | 1153.1 | 11,637 |
| 11 | Banan | 109 | 597.9 | 7550 |
| 12 | Changshou | 87 | 612.2 | 6026 |
| 13 | Jiangjing | 141 | 438.4 | 9767 |
| 14 | Hechuan | 141 | 601.8 | 9767 |
| 15 | Yongchuan | 116 | 734.6 | 8035 |
| 16 | Nanchuan | 60 | 231.7 | 4156 |
| 17 | Qijiang | 110 | 400.4 | 7619 |
| 18 | Dazu | 79 | 550.9 | 5472 |
| 19 | Bishan | 76 | 830.6 | 5264 |
| 20 | TongLiang | 73 | 544.4 | 5057 |
| 21 | Tongnan | 72 | 454.3 | 4987 |
| 22 | Rongchang | 72 | 668.5 | 4987 |
| 23 | Kaizhou | 118 | 297.7 | 8174 |
| 24 | Liangping | 66 | 349.6 | 4572 |
| 25 | Wulong | 35 | 121 | 2424 |
| 26 | Chengkou | 18 | 54.7 | 1247 |
| 27 | Fengdu | 59 | 203.5 | 4087 |
| 28 | Dianjiang | 71 | 468 | 4918 |
| 29 | Zhong | 75 | 342.9 | 5195 |
| 30 | Yunyang | 94 | 258.5 | 6511 |
| 31 | Fengjie | 74 | 180.6 | 5126 |
| 32 | Wushan | 45 | 152.3 | 3117 |
| 33 | Wuxi | 38 | 94.6 | 2632 |
| 34 | Shizhu | 38 | 126.1 | 2632 |
| 35 | XiuShan | 49 | 199.8 | 3394 |
| 36 | YouYang | 55 | 106.4 | 3810 |
| 37 | Pengshui | 49 | 125.7 | 3394 |
| 38 | Liangjiang | 270 | 2250.0 | 18,702 |
| 39 | High-tech | 13 | 1689.2 | 866 |
| 40 | Wansheng | 26 | 459.4 | 1801 |
| 41 | Dadukou | 36 | 3495.1 | 2494 |
| Operating Cost (Yuan/d) | Processing Cost (Yuan/kg) | Transportation Cost (Yuan/km·kg) | |
|---|---|---|---|
| FPC | 70 | 1 | 0.35 |
| MPC | 50 | 2 | |
| Storage center | 20 | 0.5 |
| No. | Processing Capacity (kg/d) | Storage Capacity (kg/d) |
|---|---|---|
| Fixed center1 | 30,000 | 5000 |
| Fixed center2 | 30,000 | 5000 |
| Fixed center3 | 10,000 | 5000 |
| Fixed center4 | 30,000 | 5000 |
| Fixed center5 | 10,000 | 5000 |
| Fixed center6 | 20,000 | 5000 |
| Fixed center7 | 10,000 | 5000 |
| Fixed center8 | 10,000 | 5000 |
| Fixed center9 | 10,000 | 5000 |
| Mobile center1 | 1500 × Z1 | 2000 |
| Mobile center2 | 1500 × Z2 | 2000 |
| Mobile center3 | 1500 × Z3 | 2000 |
| Mobile center4 | 1500 × Z4 | 2000 |
| Mobile center5 | 1500 × Z5 | 2000 |
| Mobile center6 | 1500 × Z6 | 2000 |
| Mobile center7 | 1500 × Z7 | 2000 |
| Mobile center8 | 1500 × Z8 | 2000 |
| Mobile center9 | 1500 × Z9 | 2000 |
| Mobile center10 | 1500 × Z10 | 2000 |
| Mobile center11 | 1500 × Z11 | 2000 |
| Mobile center12 | 1500 × Z12 | 2000 |
| Mobile center13 | 1500 × Z13 | 2000 |
| Mobile center14 | 1500 × Z14 | 2000 |
| Storage center1 | 4000 | |
| Storage center2 | 4000 | |
| Storage center3 | 4000 | |
| Storage center4 | 4000 | |
| Storage center5 | 4000 | |
| Storage center6 | 4000 | |
| Storage center7 | 4000 | |
| Storage center8 | 4000 |
| No. | Generation Center | The Amount of IMW (kg/d) | ||
|---|---|---|---|---|
| t = 1 | t = 2 | t = 3 | ||
| 1 | Wanzhou | 4341.10 | 4341.10 | 37,519.92 |
| 2 | Qianjiang | 1276.02 | 1276.02 | 1276.02 |
| 3 | Fuling | 3078.24 | 3078.24 | 3078.24 |
| 4 | Yuzhong | 1736.44 | 1736.44 | 1736.44 |
| 5 | Jiangbei | 2367.87 | 2367.87 | 2367.87 |
| 6 | Shapingba | 3078.24 | 27,594.13 | 3078.24 |
| 7 | Jiulongpo | 3236.09 | 3236.09 | 3236.09 |
| 8 | Nanan | 2394.18 | 2394.18 | 2394.18 |
| 9 | Beibei | 2157.40 | 2157.40 | 2157.40 |
| 10 | Yubei | 4420.03 | 4420.03 | 4420.03 |
| 11 | Banan | 2867.76 | 2867.76 | 2867.76 |
| 12 | Changshou | 2288.94 | 2288.94 | 2288.94 |
| 13 | Jiangjing | 3709.67 | 3709.67 | 3709.67 |
| 14 | Hechuan | 3709.67 | 3709.67 | 3709.67 |
| 15 | Yongchuan | 3051.93 | 27,387.34 | 3051.93 |
| 16 | Nanchuan | 1578.58 | 1578.58 | 1578.58 |
| 17 | Qijiang | 2894.07 | 2894.07 | 2894.07 |
| 18 | Dazu | 2078.47 | 19,736.20 | 2078.47 |
| 19 | Bishan | 1999.54 | 19,115.84 | 1999.54 |
| 20 | TongLiang | 1920.61 | 18,495.48 | 1920.61 |
| 21 | Tongnan | 1894.30 | 1894.30 | 1894.30 |
| 22 | Rongchang | 1894.30 | 1894.30 | 1894.30 |
| 23 | Kaizhou | 3104.55 | 3104.55 | 27,800.91 |
| 24 | Liangping | 1736.44 | 1736.44 | 1736.44 |
| 25 | Wulong | 920.84 | 920.84 | 920.84 |
| 26 | Chengkou | 473.57 | 473.57 | 7122.17 |
| 27 | Fengdu | 1552.27 | 1552.27 | 1552.27 |
| 28 | Dianjiang | 1867.99 | 1867.99 | 1867.99 |
| 29 | Zhong | 1973.23 | 1973.23 | 1973.23 |
| 30 | Yunyang | 2473.11 | 2473.11 | 22,838.02 |
| 31 | Fengjie | 1946.92 | 1946.92 | 1946.92 |
| 32 | Wushan | 1183.94 | 1183.94 | 1183.94 |
| 33 | Wuxi | 999.77 | 999.77 | 11,257.92 |
| 34 | Shizhu | 999.77 | 999.77 | 999.77 |
| 35 | XiuShan | 1289.18 | 1289.18 | 1289.18 |
| 36 | YouYang | 1447.03 | 1447.03 | 1447.03 |
| 37 | Pengshui | 1289.18 | 1289.18 | 1289.18 |
| 38 | Liangjiang | 7103.62 | 7103.62 | 7103.62 |
| 39 | High-tech | 328.87 | 328.87 | 328.87 |
| 40 | Wansheng | 684.05 | 684.05 | 684.05 |
| 41 | Dadukou | 947.15 | 947.15 | 947.15 |
| Total | 90,294.93 | 190,495.15 | 185,441.77 | |
| t | Outbreak Sites | Storage Centers | FPCs | MPCs (the Amount of Mobile Processing Facilities) |
|---|---|---|---|---|
| 1 | Sites No. 0 | 1, 2, 4, 6, 7, 13, 15, 16, 19, 22, 23, 26, 28, 30, 31 | 1, 4, 7, 8, 9 | |
| 2 | Sites No. 6, 15, 18, 19, 20 | 1, 2, 4, 6, 7, 8, 10, 11, 13, 14, 15, 16, 19, 20, 22, 23, 26, 28, 29, 30, 31 | 1, 2, 3, 4, 5, 6, 7, 8, 9 | 1 (3), 2 (3), 4 (3), 6 (3) |
| 3 | Sites No. 1, 23, 26, 30, 33 | 1, 2, 4, 6, 7, 8, 10, 11, 13, 14, 15, 16, 19, 20, 22, 23, 26, 28, 29, 30, 31 | 1, 2, 3, 4, 5, 6, 7, 8, 9 | 1 (3), 2 (2), 7 (3), 8 (3) |
| t | Single Objective | Multi-Objective | ||||
|---|---|---|---|---|---|---|
| z1min (Million Yuan) | z1max (Million Yuan) | z2min | z2max | z1 (Million Yuan) | z2 | |
| 1 | 7.7559 | 1.2006 | 0.14115 | 1.2174 | ||
| 2 | 16.476 | 22.237 | 1.1231 | 2.6882 | 16.636 | 2.2374 |
| 3 | 15.985 | 23.997 | 1.0041 | 2.7628 | 16.165 | 2.2496 |
| If No MPC | Single Objective | Multi-Objective | ||||
|---|---|---|---|---|---|---|
| t | z1min (Million Yuan) | z1max (Million Yuan) | z2min | z2max | z1 (Million Yuan) | z2 |
| 3 | 15.943 | 21.515 | 2.1061 | 2.6217 | 16.178 | 2.4670 |
| MPC | The Demand of Mobile Processing Facilities in MPC | ||||
| t = 1 | The Number and Path of Transfer | t = 2 | the Number and Path of Transfer | t = 3 | |
| 1 | 1 | 3 | 3 | ||
| 2 | 1 | 3 | 1facility→7 | 2 | |
| 3 | 1 | 1 | 1 | ||
| 4 | 1 | 3 | 3facilities→8 | 0 | |
| 5 | 1 | 1facility→4 | 0 | 0 | |
| 6 | 1 | 3 | 0 | ||
| 7 | 1 | 1facility→2 | 0 | adding 2 facilities | 3 |
| 8 | 1 | 1facility→4 | 0 | 3 | |
| 9 | 1 | 1facility→1 | 0 | 0 | |
| 10 | 1 | 1facility→6 | 0 | 0 | |
| 11 | 1 | 1facility→6 | 0 | 0 | |
| 12 | 1 | 1facility→2 | 0 | 0 | |
| 13 | 1 | 0 | 0 | ||
| 14 | 1 | 1facility→1 | 1 | 1 | |
| Stage 2 | z3 (Thousand Yuan) | |
|---|---|---|
| Mobile Processing Facilities | No Mobile Processing Facilities | |
| t = 1~t = 2 | 564.12 | 1920 |
| t = 2~t = 3 | 502.16 | 1440 |
| Total | 1066.28 | 3360 |
| MCA | PRC (Million Yuan) | Sites No. 6, 15, 18, 19, 20 | z3 (Million Yuan) | New Devices | ||
|---|---|---|---|---|---|---|
| z1 (Million Yuan) | z2 | Distribution 1–2 | Distribution 2–3 | |||
| 1600 | 0.16 | 16.611 | 2.2879 | 0.6267 | 0.7018 | 2 |
| 1800 | 0.18 | 16.634 | 2.2422 | 0.5368 | 0.4834 | 1 |
| 2000 | 0.2 | 16.636 | 2.2374 | 0.4851 | 0.5483 | 2 |
| 2200 | 0.22 | 16.65 | 2.2085 | 0.4851 | 0.4248 | 0 |
| 2400 | 0.24 | 16.656 | 2.1957 | 0.4023 | 0.4248 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, X.; Liao, W. Collaborative Reverse Logistics Network for Infectious Medical Waste Management during the COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2022, 19, 9735. https://doi.org/10.3390/ijerph19159735
Luo X, Liao W. Collaborative Reverse Logistics Network for Infectious Medical Waste Management during the COVID-19 Outbreak. International Journal of Environmental Research and Public Health. 2022; 19(15):9735. https://doi.org/10.3390/ijerph19159735
Chicago/Turabian StyleLuo, Xuan, and Wenzhu Liao. 2022. "Collaborative Reverse Logistics Network for Infectious Medical Waste Management during the COVID-19 Outbreak" International Journal of Environmental Research and Public Health 19, no. 15: 9735. https://doi.org/10.3390/ijerph19159735
APA StyleLuo, X., & Liao, W. (2022). Collaborative Reverse Logistics Network for Infectious Medical Waste Management during the COVID-19 Outbreak. International Journal of Environmental Research and Public Health, 19(15), 9735. https://doi.org/10.3390/ijerph19159735