
Mental Health and Physical Activity of Female Higher Education Students during the COVID-19 Pandemic: A Comparative Cross-Sectional Study from Lithuania




Abstract
1. Introduction
2. Materials and Methods
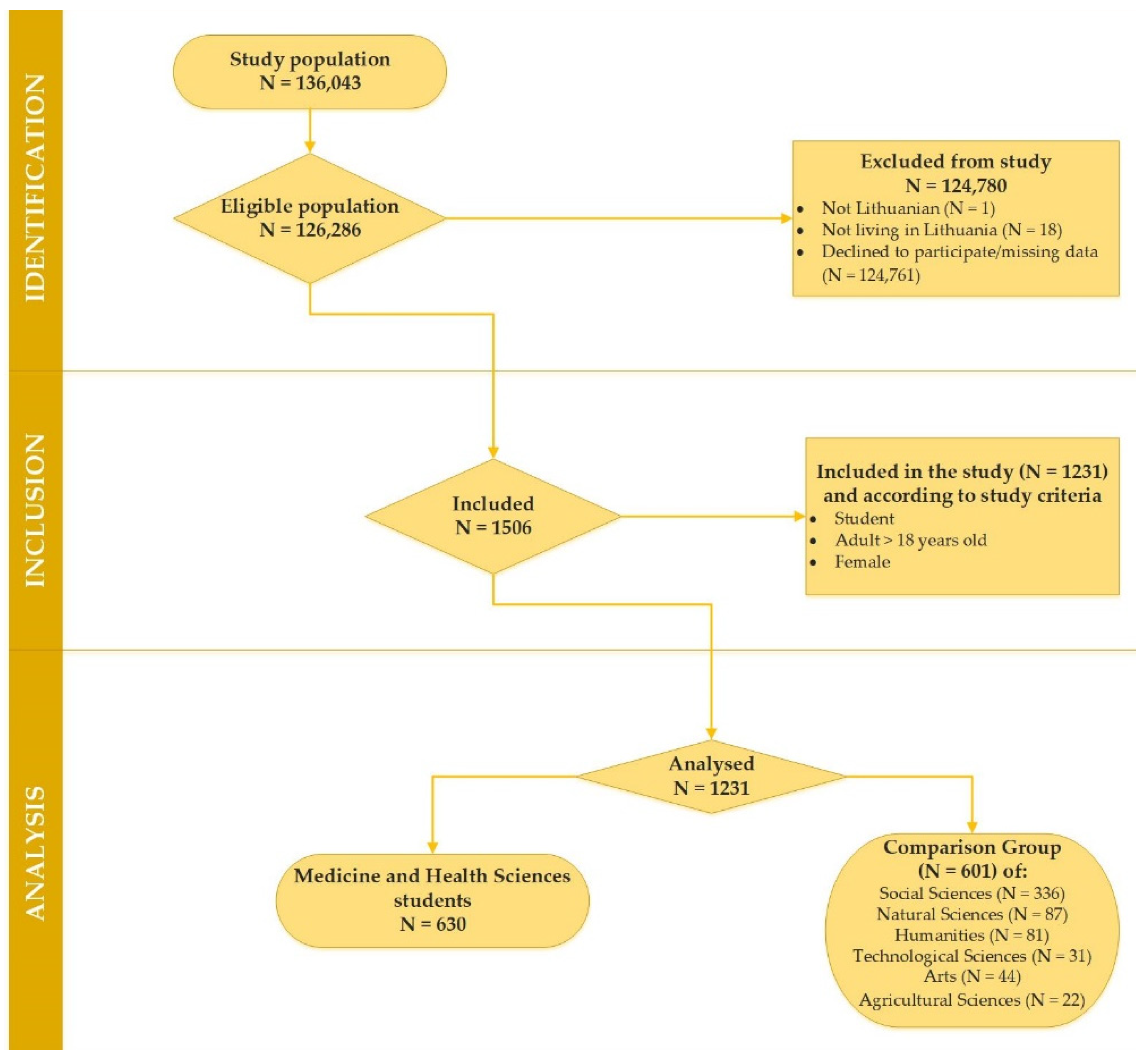
2.1. Study Population, Area and Design
2.2. Measures
2.2.1. The Hospital Anxiety and Depression Scale (HADS)
2.2.2. The Patient Health Questionnaire (PHQ-15)
2.2.3. Baecke Physical Activity Questionnaire (BPAQ)
2.3. Statistical Analysis
3. Results
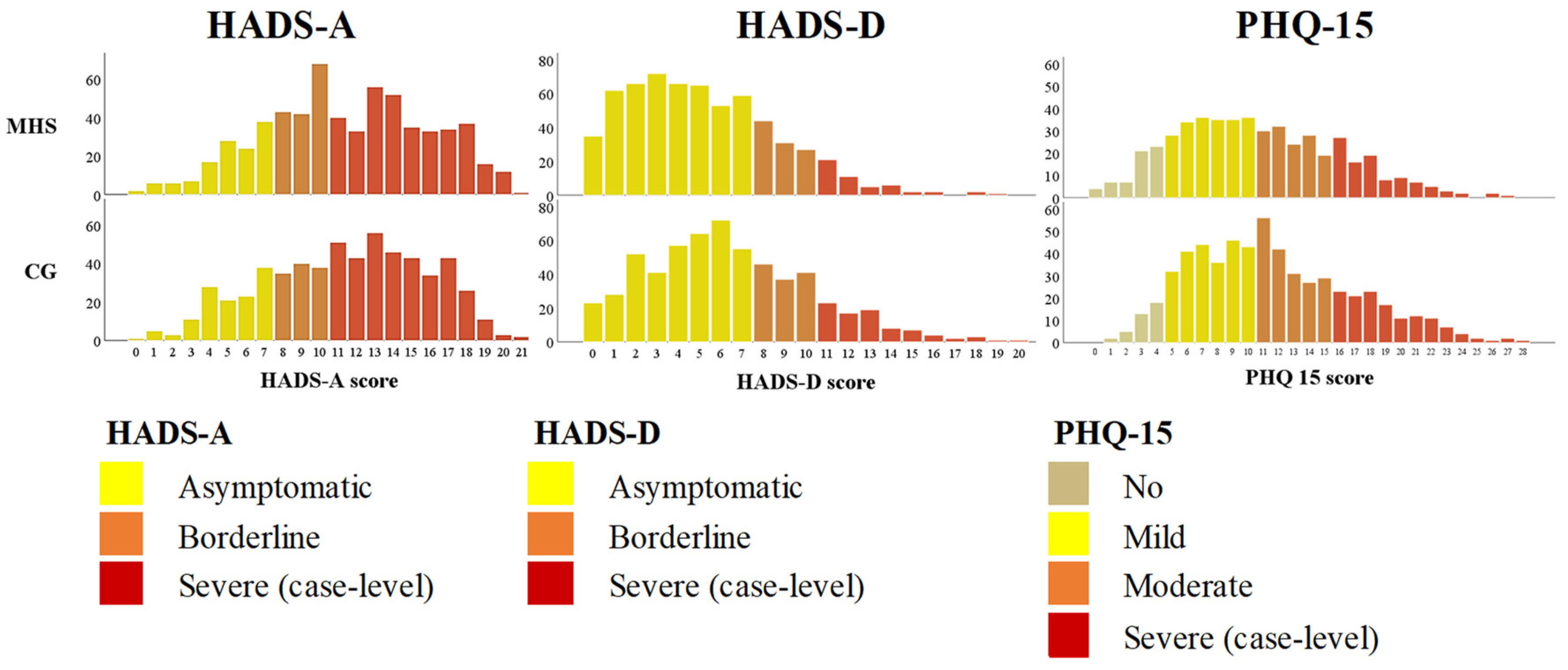
3.1. Descriptive and Frequency Analyses
3.2. Regression Analyses
4. Discussion
4.1. The Incidence for Symptoms of Mental Disorders
4.2. Somatic Complaints and Comorbid Mental Disorders Symptoms
4.3. The Disparities in Mental Health
4.4. Physical Activity for Symptoms of Depression and Anxiety
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed on 1 May 2021).
- World Health Organisation. Depression. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 1 November 2021).
- American Psychiatric Association. Anxiety Disorders. Available online: https://www.psychiatry.org/patients-families/anxiety-disorders (accessed on 13 January 2022).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM–5), 5th ed.; American Psychiatric Publishing: Arlington, VA, USA; Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Humaida, I.A.I. Relationship between stress and psychosomatic complaints among nurses in Tabarjal Hospital. Open J. Med. Psychol. 2012, 1, 15–19. [Google Scholar] [CrossRef][Green Version]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressiveepisode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef] [PubMed]
- WHO World Mental Health Survey Consortium. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization world mental health surveys. J. Am. Med. Assoc. 2004, 291, 2581–2590. [Google Scholar] [CrossRef] [PubMed]
- Khoo, E.M.; Mathers, N.J.; McCarthy, S.A.; Low, W.Y. Somatisation disorder and its associated factors in multiethnic primary care clinic attenders. Int. J. Behav. Med. 2012, 19, 165–173. [Google Scholar] [CrossRef]
- Liu, L.; Bi, B.; Qin, X.; Wei, S.; Wang, W.; Li, Y.; Jin, Q.; Ai, L.; Phillips, M.R.; Dong, G. The prevalence of somatoform disorders in internal medicine outpatient departments of 23 general hospitals in Shenyang, China. Gen. Hosp. Psychiatry 2012, 34, 339–344. [Google Scholar] [CrossRef]
- Zeng, F.; Sun, X.; Yang, B.; Shen, H.; Liu, L. The theoretical construction of a classification of clinical somatic symptoms in psychosomatic medicine theory. PLoS ONE 2016, 11, e0161222. [Google Scholar] [CrossRef]
- Ibrahim, A.K.; Kelly, S.J.; Adams, C.E.; Glazebrook, C. A systematic review of studies of depression prevalence in university students. J Psychiatr Res. 2013, 47, 391–400. [Google Scholar] [CrossRef]
- Veldman, K.; Reijneveld, S.A.; Ortiz, J.A.; Verhulst, F.C.; Bultmann, U. Mental health trajectories from childhood to young adulthood affect the educational and employment status of young adults: Results from the TRAILS study. J. Epidemiol. Community Health 2015, 69, 588–593. [Google Scholar] [CrossRef]
- Global Burden of Disease Study. In Global Health Data Exchange; Institute for Health Metrics and Evaluation: Washington, DC, USA, 2016; Available online: http://ghdx.healthdata.org/gbd-results-tool/ (accessed on 5 September 2021).
- Data and Resources: Prevalence of Mental Health. In Health Topics [Website]; WHO Regional Office for Europe: Copenhagen, Denmark, 2018; Available online: http://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/data-and-statistics/ (accessed on 7 September 2021).
- Shen, R.; Guan, X.; Huang, Y.; Liu, Z.; Chen, H.; Zhang, T.; Ma, C. A descriptive epidemiological study of disability prevalence attributed to neurotic disorders in China. Psychiatry Res. 2019, 272, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, H. Briquets syndrome in association with depression and panic: A reconceptualization of Briquets syndrome. Am. J. Psychiatr. 1989, 146, 334–338. [Google Scholar] [PubMed]
- Silva, M.; Loureiro, A.; Cardoso, G. Social determinants of mental health: A review of the evidence. Eur. J. Psychiatry 2016, 30, 259–292. [Google Scholar]
- Srivastava, K. Women and mental health: Psychosocial perspective. Ind. Psychiatry J. 2012, 21, 1. [Google Scholar] [CrossRef]
- Springs, F.E.; Friedrich, W.N. Health risk behaviors and medical sequelae of childhood sexual abuse. Mayo Clinic. Proc. 1992, 67, 527–532. [Google Scholar] [CrossRef]
- Drossman, D.A.; Talley, M.J.; Leserman, J.; Olden, K.W.; Barreiro, M.A. Sexual and physical abuse and gastrointestinal illness: Review and recommendations. Ann. Intern. Med. 1995, 123, 782–794. [Google Scholar] [CrossRef]
- McCauley, J.; Kern, D.E.; Kolodner, K.; Dill, L.; Sckroeder, A.F.; DeChant, H.K.; Ryden, J.; Bass, E.B. “The battering syndrome”: Prevalence and clinical characteristics of domestic violence in primary care internal medicinepractices. Ann. Intern. Med. 1995, 123, 737–746. [Google Scholar] [CrossRef]
- Mezey, G.; Bacchus, L.; Bewley, S.; White, S. Domestic violence, lifetime trauma and psychological health of childbearing women. BJOG 2005, 112, 197–204. [Google Scholar] [CrossRef]
- Valentine, S.E.; Marques, L.; Wang, Y.; Ahles, E.M.; Dixon De Silva, L.; Alegría, M. Gender differences in exposure to potentially traumatic events and diagnosis of posttraumatic stress disorder (PTSD) by racial and ethnic group. Gen. Hosp. Psychiatry 2019, 61, 60–68. [Google Scholar] [CrossRef]
- Myklestad, I.; Straiton, M. The relationship between self-harm and bullying behaviour: Results from a population based study of adolescents. BMC Public Health 2021, 21, 524. [Google Scholar] [CrossRef]
- Wilson, M.L.; Viswanathan, B.; Rousson, V.; Bovet, P. Weight status, body image and bullying among adolescents in the Seychelles. Int. J. Environ. Res. Public Health 2013, 10, 1763–1774. [Google Scholar] [CrossRef] [PubMed]
- Charoenwanit, S. The relationship of cyber-bullying and academic achievement, general health, and depression in adolescents in Thailand. Walailak J. Sci. Technol. 2019, 16, 231–241. [Google Scholar] [CrossRef]
- Craig, W.; Boniel-Nissim, M.; King, N.; Walsh, S.D.; Boer, M.; Donnelly, P.D.; Harel-Fisch, Y.; Malinowska-Cieślik, M.; de Matos, M.G.; Cosma, A.; et al. Social media use and cyber-bullying: A cross-national analysis of young people in 42 countries. J. Adolesc. Health 2020, 66, S100–S108. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Yang, X.; Yang, Y.; Chen, L.; Qiu, X.; Qiao, Z.; Zhou, J.; Pan, H.; Ban, B.; Zhu, X.; et al. The role of family environment in depressive symptoms among university students: A large sample survey in china. PLoS ONE 2015, 10, e0143612. [Google Scholar] [CrossRef]
- Guerrero-Muñoz, D.; Salazar, D.; Constain, V.; Perez, A.; Pineda-Cañar, C.A.; García-Perdomo, H.A. Association between family functionality and depression: A systematic review and meta-analysis. Korean J. Fam. Med. 2021, 42, 172–180. [Google Scholar] [CrossRef]
- John, J.; Miller, M.D. Clinical implications of gender differences in schizophrenia. Psychiatr. Times 2018, 35, 9–11. [Google Scholar]
- Arnett, J.J.; Žukauskienė, R.; Sugimura, K. The new life stage of emerging adulthood at ages 18–29 years: Implications for mental health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood. A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Arias-de la Torre, J.; Ronaldson, A.; Prina, M.; Matcham, F.; Pereira, S.M.P.; Hatch, S.L.; Armstrong, D.; Pickles, A.; Hotopf, M.; Dregan, A. Depressive symptoms during early adulthood and the development of physical multimorbidity in the UK: An observational cohort study. Lancet Healthy Longev. 2021, 2, e801–e810. [Google Scholar] [CrossRef]
- Gustavson, K.; Knudsen, A.K.; Nesvåg, R.; Knudsen, G.P.; Vollset, S.E.; Reichborn-Kjennerud, T. Prevalence and stability of mental disorders among young adults: Findings from a longitudinal study. BMC Psychiatry 2018, 18, 65. [Google Scholar] [CrossRef]
- Beesdo, K.; Knappe, S.; Pine, D.S. Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM-V. Psychiatr. Clin. N. Am. 2009, 32, 483–524. [Google Scholar] [CrossRef] [PubMed]
- Bains, N.; Abdijadid, S. Major Depressive Disorder. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kalin, N.H. The critical relationship between anxiety and depression. Am. J. Psychiatry 2020, 177, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Copeland, W.E.; Adair, C.E.; Smetanin, P.; Stiff, D.; Briante, C.; Colman, I.; Fergusson, D.; Horwood, L.; Poulton, R.; Costello, E.J.; et al. Diagnostic transitions from childhood to adolescence to early adulthood. J. Child. Psychol. Psychiatry 2013, 54, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.J.; Copeland, W.; Angold, A. The great Smoky Mountains study: Developmental epidemiology in the southeastern United States. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 639–646. [Google Scholar] [CrossRef]
- Johnson, J.G.; Cohen, P.; Kasen, S. Minor depression during adolescence and mental health outcomes during adulthood. Br. J. Psychiatry 2009, 195, 264–265. [Google Scholar] [CrossRef]
- Tanner, J.L. Mental health in emerging adulthood. In The Oxford Handbook of Emerging Adulthood; Arnett, J.J., Ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Barlett, C.P.; Barlett, N.D. The young and the restless: Examining the relationships between age, emerging adulthood variables, and the dark triad. Pers. Individ. Dif. 2015, 86, 20–24. [Google Scholar] [CrossRef]
- Mirza, A.A.; Baig, M.; Beyari, G.M.; Halawani, M.A.; Mirza, A.A. Depression and anxiety among medical students: A brief overview. Adv. Med. Educ. Pract. 2021, 12, 393–398. [Google Scholar] [CrossRef]
- Brazeau, C.M.; Shanafelt, T.M.; Durning, S.J.; Massie, F.S.; Eacker, A.; Moutier, C.; Dyrbye, L.N.; Satele, D.; Sloan, J.A. Distress among matriculating medical students relative to the general population. Acad. Med. 2014, 89, 1520–1525. [Google Scholar] [CrossRef]
- Hope, V.; Henderson, M. Medical student depression, anxiety and distress outside North America: A systematic review. Med. Educ. 2014, 48, 963–979. [Google Scholar] [CrossRef]
- Quek, T.T.C.; Tam, W.W.S.; Tran, B.X.; Zhang, M.; Zhang, Z.; Ho, C.S.H.; Ho, R.C.M. The global prevalence of anxiety among medical students: A meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 2735. [Google Scholar] [CrossRef]
- Mao, Y.; Zhang, N.; Liu, J.; Zhu, B.; He, R.; Wang, X. A systematic review of depression and anxiety in medical students in China. BMC Med. Educ. 2019, 19, 327. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, M.; Joneborg, N.; Runeson, B. Stress and depression among medical students: A cross-sectional study. Med. Educ. 2005, 39, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad. Med. 2006, 81, 354–373. [Google Scholar] [CrossRef] [PubMed]
- Rotenstein, L.S.; Ramos, M.A.; Torre, M.; Segal, J.B.; Peluso, M.J.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students a systematic review and meta-analysis. J. Am. Med. Assoc. 2016, 316, 2214–2236. [Google Scholar] [CrossRef]
- Prinz, P.; Hertrich, K.; Hirschfelder, U.; de Zwaan, M. Burnout, depression and depersonalisation–psychological factors and coping strategies in dental and medical students. GMS Z. Med. Ausbild. 2012, 29, Doc10. [Google Scholar]
- World Health Organisation. COVID-2019 Situation Reports-171. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200709-covid-19-sitrep-171.pdf?sfvrsn=9aba7ec7_2 (accessed on 9 August 2020).
- Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 3 August 2022).
- World Health Organisation. Available online: https://covid19.who.int/region/euro/country/lt (accessed on 2 August 2022).
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Vindegaard, N.; Eriksen Benros, M. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Žilinskas, E.; Žulpaitė, G.; Puteikis, K.; Viliūnienė, R. Mental health among higher education students during the COVID-19 pandemic: A cross-sectional survey from Lithuania. Int. J. Environ. Res. Public Health 2021, 18, 12737. [Google Scholar] [CrossRef]
- Biwer, F.; Wiradhany, W.; Egbrink, M.O.; Hospers, H.; Wasenitz, S.; Jansen, W.; de Bruin, A. Changes and adaptations: How university students self-regulate their online learning during the COVID-19 pandemic. Front. Psychol. 2021, 12, 642593. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Du, X. Addressing collegiate mental health amid COVID-19 pandemic. Psychiatry Res. 2020, 288, 113003. [Google Scholar] [CrossRef] [PubMed]
- Kwong, A.S.F.; Pearson, R.M.; Adams, M.J.; Northstone, K.; Tilling, K.; Smith, D.; Fawns-Ritchie, C.; Bould, H.; Warne, N.; Zammit, S.; et al. Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. Br. J. Psychiatry 2021, 218, 334–343. [Google Scholar] [CrossRef]
- Hawes, M.T.; Szenczy, A.K.; Klein, D.N.; Hajcak, G.; Nelson, B.D. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Varga, T.V.; Bu, F.; Dissing, A.S.; Elsenburg, L.K.; Bustamante, J.J.H.; Matta, J.; van Zon, S.K.; Brouwer, S.; Bültmann, U.; Fancourt, D.; et al. Loneliness, worries, anxiety, and precautionary behaviours in response to the COVID-19 pandemic: A longitudinal analysis of 200,000 Western and Northern Europeans. Lancet Reg. Health-Eur. 2021, 2, 100020. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Bullmore, E.; Ballard, C.; Christensen, H.; Silver, R.C.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Tomé, T.H.; Valentini, N.C. Benefits of systematic physical activities on individual’s psychological parameters: A study about anxiety and aggression. J. Physic. Educ. 2008, 17, 123–130. [Google Scholar]
- De Moor, M.H.; Boomsma, D.I.; Stubbe, J.H.; Willemsen, G.; de Geus, E.J. Testing causality in the association between regular exercise and symptoms of anxiety and depression. Arch. Gen. Psychiatry 2008, 65, 897–905. [Google Scholar] [CrossRef]
- Salmon, P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: A unifying theory. Clin. Psychol. Rev. 2001, 21, 33–61. [Google Scholar] [CrossRef]
- Bauer, L.L.; Seiffer, B.; Deinhart, C.; Atrott, B.; Sudeck, G.; Hautzinger, M.; Rösel, I.; Wolf, S. Associations of exercise and social support with mental health during quarantine and social-distancing measures during the COVID-19 pandemic: A cross-sectional survey in Germany. medRxiv 2020, 20144105. [Google Scholar] [CrossRef]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; López-Sánchez, G.F.; Grabovac, I.; Willeit, P.; Vancampfort, D.; Caperchione, C.M.; Sadarangani, K.P.; Werneck, A.O.; et al. Moderate to vigorous physical activity and sedentary behavior changes in self-isolating adults during the COVID-19 pandemic in Brazil: A cross-sectional survey exploring correlates. Sport. Sci. Health 2022, 18, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef] [PubMed]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Sarchiapone, M.; Apter, A.; et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2017, 26, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; MacIntosh, L.; O’Neill, C.; D’Silva, C.; Shearer, H.; Smith, K.; Côtéa, P. The association of physical activity with depression and stress among post-secondary school students: A systematic review. Ment. Health Phys. Act. 2018, 14, 146–156. [Google Scholar] [CrossRef]
- Puthran, R.; Zhang, M.W.B.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef]
- Honney, K.; Buszewicz, M.; Coppola, W.; Griffin, M. Comparison of levels of depression in medical and non-medical students. Clin. Teach. 2010, 7, 180–184. [Google Scholar] [CrossRef]
- Moreira de Sousa, J.; Moreira, C.A.; Telles-Correia, D. Anxiety, depression and academic performance: A study amongst Portuguese medical students versus non-medical students. Acta Med. Port. 2018, 31, 454–462. [Google Scholar] [CrossRef]
- Al-Dabal, B.K.; Koura, M.R.; Rasheed, P.; Al-Sowielem, L.; Makki, S.M.; Comparative, A. Study of perceived stress among female medical and non-medical university students in Dammam, Saudi Arabia. Sultan Qaboos Univ. Med. J. 2010, 10, 231–240. [Google Scholar]
- Evans-Lacko, S.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Benjet, C.; Bruffaerts, R.; Chiu, W.T.; Florescu, S.; de Girolamo, G.; Gureje, O.; et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO World Mental Health (WMH) surveys. Psychol Med. 2018, 48, 1560–1571. [Google Scholar] [CrossRef]
- Venkatarao, E.; Iqbal, S.; Gupta, S. Stress, anxiety and depression among medical undergraduate students and their socio-demographic correlates. Indian J. Med. Res. Suppl. 2015, 141, 354–357. [Google Scholar] [CrossRef]
- Steptoe, A.; Tsuda, A.; Tanaka, Y.; Wardle, J. Depressive symptoms, socio-economic background, sense of control, and cultural factors in university students from 23 countries. Int. J. Behav. Med. 2007, 14, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Ghodasara, S.L.; Davidson, M.A.; Reich, M.S.; Savoie, C.V.; Rodgers, S.M. Assessing student mental health at the Vanderbilt University School of Medicine. Acad. Med. 2011, 86, 116–121. [Google Scholar] [CrossRef]
- Bassols, A.M.; Okabayashi, L.S.; da Silva, A.B.; Carneiro, B.B.; Feijó, F.; Guimarães, G.C.; Cortes, G.N.; Rohde, L.A.; Eizirik, C.L. First- and last-year medical students: Is there a difference in the prevalence and intensity of anxiety and depressive symptoms? Braz. J. Psychiatry 2014, 36, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Inam, S.B. Anxiety and depression among students of a Medical College in Saudi Arabia. Int. J. Health Sci. 2007, 1, 295–300. [Google Scholar]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/directorgeneral/speeches/detail/who-director-general-s-opening-remarks-at-themedia-briefing-on-covid-19---11-march-2020/ (accessed on 1 September 2021).
- Pandey, R.M. Approaches to sample size calculation in comparative studies. Indian J. Pediatr. 1999, 66, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Baecke, J.A.H.; Burema, J.; Frijters, E.R. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bunevicius, A.; Peceliuniene, J.; Mickuviene, N.; Valius, L.; Bunevicius, R. Screening for depression and anxiety disorders in primary care patients. Depress. Anxiety 2007, 24, 455–460. [Google Scholar] [CrossRef]
- Bunevicius, R.; Peceliuniene, J.; Mickuviene, N.; Bunevicius, A.; Pop, V.J.; Girdler, S.S. Mood and thyroid immunity assessed by ultrasonographic imaging in a primary health care. J. Affect. Disord. 2007, 97, 85–90. [Google Scholar] [CrossRef][Green Version]
- Bunevicius, A.; Katkute, A.; Bunevicius, R. Symptoms of anxiety and depression in medical students and in humanities students: Relationship with big-five personality dimensions and vulnerability to stress. Int. J. Soc. Psychiatry 2008, 54, 494–501. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. J. Am. Med. Assoc. 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Zarankė, S. The Effect of Progressive Muscle Relaxation Exercises in Reducing Perceived Stress and Somatic Symptoms of Conscripts Performing Military Service in Unit X. Master’s Thesis, Vytautas Magnus University, Faculty of Social Sciences, Department of Psychology, Kaunas, Lithuania, 2021. [Google Scholar]
- Kocalevent, R.D.; Hinz, A.; Brähler, E. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry 2013, 13, 91. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; deGruy, F.V.; Swindle, R. A symptom checklist to screen for somatoform disorders in primary care. Psychosomatics 1998, 39, 263–272. [Google Scholar] [CrossRef]
- Barsky, A.J.; Orav, E.J.; Bates, D.W. Somatization increases medical utilization and costs independent of psychiatric and medical co-morbidity. Arch. Gen. Psychiatry 2005, 62, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-15: Validity of a new measure for evaluating the severity of somatic symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef]
- Philippaerts, R.M.; Westerterp, K.R.; Lefevre, J. Doubly labeled water validation of three physical activity questionnaires. Int. J. Sports Med. 1999, 20, 284–289. [Google Scholar] [CrossRef]
- Sadeghisani, M.; Manshadi, F.D.; Azimi, H.; Montazeri, A. Validity and reliability of the Persian version of Baecke habitual physical activity questionnaire in healthy subjects. Asian J. Sports Med. 2016, 7, e31778. [Google Scholar] [CrossRef]
- Khosravi, M. Burnout among Iranian medical students: Prevalence and its relationship to personality dimensions and physical activity. Eur. J. Transl. Myol. 2021, 31, 9411. [Google Scholar]
- Miežienė, B.; Šiupšinskas, L.; Jankauskienė, R. Relationships between sport, work and leisure-time physical activity among Lithuanian university students. Education. Physical Training. Sport 2011, 2, 24–30. [Google Scholar] [CrossRef]
- Ribikauskaitė, D. Links among physical activity, mental health and anthropometric data applying physical education program. Wellness Educ. Manag. 2016, 1, 18–24. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Kardangusheva, A.M.; Dzakhmysheva, D.A.; Kardanova, M.A.; Chanaeva, A.Y.; Makoeva, M.A.; Khagabanova, I.S. Prevalence of anxiety and depression disorders among medical students one year after the start of the COVID-19 pandemic. Cardiometry 2022, 21, 111–118. [Google Scholar] [CrossRef]
- Basheti, I.A.; Mhaidat, Q.N.; Mhaidat, H.N. Prevalence of anxiety and depression during COVID-19 pandemic among healthcare students in Jordan and its effect on their learning process: A national survey. PLoS ONE 2021, 16, e0249716. [Google Scholar] [CrossRef] [PubMed]
- Sazakli, E.; Leotsinidis, M.; Bakola, M.; Kitsou, K.S.; Katsifara, A.; Konstantopoulou, A.; Jelastopulu, E. Prevalence and associated factors of anxiety and depression in students at a Greek university during COVID-19 lockdown. J. Public Health Res. 2021, 10, 2089. [Google Scholar] [CrossRef] [PubMed]
- Rolland, F.; Hadouiri, N.; Haas-Jordache, A.; Gouy, E.; Mathieu, L.; Goulard, A.; Morvan, Y.; Frajerman, A. Mental health and working conditions among French medical students: A nationwide study. J. Affect. Disord. 2022, 306, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Shawahna, R.; Hattab, S.; Al-Shafei, R.; Tab’ouni, M. Prevalence and factors associated with depressive and anxiety symptoms among Palestinian medical students. BMC Psychiatry 2020, 20, 244. [Google Scholar] [CrossRef]
- Waqas, A.; Naveed, S.; Aedma, K.K.; Tariq, M.; Afzaal, T. Exploring clusters of defense styles, psychiatric symptoms and academic achievements among medical students: A cross-sectional study in Pakistan. BMC Res. Notes 2018, 11, 782. [Google Scholar] [CrossRef]
- Gan, G.G.; Yuen Ling, H. Anxiety, depression and quality of life of medical students in Malaysia. Med. J. Malays. 2019, 74, 57–61. [Google Scholar]
- Bogowicz, P.; Ferguson, J.; Gilvarry, E.; Kamali, F.; Kaner, E.; Newbury-Birch, D. Alcohol and other substance use among medical and law students at a UK university: A cross-sectional questionnaire survey. Postgrad. Med. J. 2018, 94, 131–136. [Google Scholar] [CrossRef]
- Safa, F.; Anjum, A.; Hossain, S.; Trisa, T.I.; Alam, S.F.; Rafi, M.A.; Podder, V.; Koly, K.N.; Azad, D.T.; Ahmad, W.U.; et al. Immediate psychological responses during the initial period of the COVID-19 pandemic among Bangladeshi medical students. Child. Youth Serv. Rev. 2021, 122, 105912. [Google Scholar] [CrossRef]
- Dayeh, A.; Mustafa, A.N. The Relations among Internet Use Habits and Severity of Depressive-Anxiety Symptoms among University Students. Master’s Thesis, Lithuanian University of Health Sciences, Department of Psychiatry, Kaunas, Lithuania, 2021. [Google Scholar]
- Gavurova, B.; Ivankova, V.; Rigelsky, M.; Mudarri, T.; Miovsky, M. Somatic symptoms, anxiety, and depression among college students in the Czech Republic and Slovakia: A cross-sectional study. Front. Public Health 2022, 10, 859107. [Google Scholar] [CrossRef] [PubMed]
- Anan, C.; Chunfeng, X.; Shuxin, L.; Lirui, K.; Jingjing, Y.; Chang, L. Investigation on the mental health status and risk factors among Chinese overseas students under COVID-19 outbreak. Res. Sq. 2020, 1–7. [Google Scholar] [CrossRef]
- Kapfhammer, H.P. Somatic symptoms in depression. Dialogues Clin. Neurosci. 2006, 8, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Bohman, H.; Jonsson, U.; Päären, A.; von Knorring, L.; Olsson, G.; von Knorring, A.-L. Prognostic significance of functional somatic symptoms in adolescence: A 15-year community-based follow-up study of adolescents with depression compared with healthy peers. BMC Psychiatry 2012, 12, 90. [Google Scholar] [CrossRef] [PubMed]
- Larsson, B.S. Somatic complaints and their relationship to depressive symptoms in Swedish adolescents. J. Child. Psychol. Psychiatry 1991, 32, 821–832. [Google Scholar] [CrossRef]
- Tylee, A.; Gandhi, P. The importance of somatic symptoms in depression in primary care. Prim. Care Companion J. Clin. Psychiatry 2005, 7, 167–176. [Google Scholar] [CrossRef]
- Halpern, C.T.; Tucker, C.M.; Bengtson, A.; Kupper, L.L.; McLean, S.A.; Martin, S.L. Somatic symptoms among US adolescent females: Associations with sexual and physical violence exposure. Matern. Child Health J. 2013, 17, 1951–1960. [Google Scholar] [CrossRef]
- McLean, S.A.; Diatchenko, L.; Lee, Y.M.; Swor, R.A.; Domeier, R.M.; Jones, J.S.; Jones, C.W.; Reed, C.; Harris, R.E.; Maixner, W.; et al. Catechol O-methyltransferase haplotype predicts immediate musculoskeletal neck pain and psychological symptoms after motor vehicle collision. J. Pain 2011, 12, 101–107. [Google Scholar] [CrossRef]
- Raj, A.; Saleem, T.K.; Vidyadharan, V. Somatic complaints and their relationship with depressive symptoms among adolescent girls: A descriptive study. Kerala J. Psychiatry 2018, 31, 10–17. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Harper, W.; Durning, S.J.; Moutier, C.; Thomas, M.R.; Massie, F.S., Jr.; Eacker, A.; Power, D.V.; Szydlo, D.W.; Sloan, J.A.; et al. Patterns of distress in US medical students. Med. Teach. 2011, 33, 834–839. [Google Scholar] [CrossRef]
- Shaikh, B.T.; Kahloon, A.; Kazmi, M.; Khalid, H.; Nawaz, K.; Khan, N.; Khan, S. Students, stress and coping strategies: A case of Pakistani medical school. Educ. Health 2004, 17, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Abdulghani, H.M.; AlKanhal, A.A.; Mahmoud, E.S.; Ponnamperuma, G.G.; Alfaris, E.A. Stress and its effects on medical students: A cross-sectional study at a college of medicine in Saudi Arabia. J. Health Popul. Nutr. 2011, 29, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Hilger-Kolb, J.; Diehl, K.; Herr, R.; Loerbroks, A. Effort-reward imbalance among students at German universities: Associations with self-rated health and mental health. Int. Arch. Occup. Environ. Health 2018, 91, 1011–1020. [Google Scholar] [CrossRef]
- Lupo, M.K.; Strous, R.D. Religiosity, anxiety and depression among Israeli medical students. Isr. Med. Assoc. J. 2011, 13, 613–618. [Google Scholar] [PubMed]
- Samaranayake, C.B.; Fernando, A.T. Satisfaction with life and depression among medical students in Auckland, New Zealand. N. Z. Med. J. 2011, 124, 12–17. [Google Scholar]
- Hemphill, N.M.; Kuan, M.T.Y.; Harris, K.C. Reduced physical activity during COVID-19 pandemic in children with congenital heart disease. Can. J. Cardiol. 2020, 36, 1130–1134. [Google Scholar] [CrossRef]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef]
- Xiang, M.Q.; Tan, X.M.; Sun, J.; Yang, H.Y.; Zhao, X.P.; Liu, L.; Hou, X.; Hu, M. Relationship of physical activity with anxiety and depression symptoms in Chinese college students during the COVID-19 outbreak. Front. Psychol. 2020, 11, 582436. [Google Scholar] [CrossRef]
- Legey, S.; Aquino, F.; Lamego, M.K.; Paes, F.; Nardi, A.E.; Neto, G.M.; Mura, G.; Sancassiani, F.; Rocha, N.; Murillo-Rodriguez, E.; et al. Relationship among physical activity level, mood and anxiety states and quality of life in physical education students. Clin. Pract. Epidemiol. Ment. Health 2017, 13, 82–91. [Google Scholar] [CrossRef]
- Murray, A.; Marenus, M.; Cahuas, A.; Friedman, K.; Ottensoser, H.; Kumaravel, V.; Sanowski, J.; Chen, W. The impact of web-based physical activity interventions on depression and anxiety among college students: Randomized experimental trial. JMIR Form. Res. 2022, 6, e31839. [Google Scholar] [CrossRef]
- Kayani, S.; Wang, J.; Kayani, S.; Kiyani, T.; Qiao, Z.; Zou, X.; Imran, M. Self-system mediates the effect of physical activity on students’ anxiety: A study from Canada. Asia Pac. Educ. Res. 2020, 30, 443–457. [Google Scholar] [CrossRef]
- Larun, L.; Nordheim, L.V.; Ekeland, E.; Hagen, K.B.; Heian, F. Exercise in prevention and treatment of anxiety and depression among children and young people. Cochrane Database Syst. Rev. 2006, 3, CD004691. [Google Scholar] [CrossRef]
- Wipfli, B.M.; Rethorst, C.D.; Landers, D.M. The anxiolytic effects of exercise: A meta-analysis of randomized trials and dose-response analysis. J. Sport Exerc. Psychol. 2008, 30, 392–410. [Google Scholar] [CrossRef]
- Carek, P.J.; Laibstain, S.E.; Carek, S.M. Exercise for the treatment of depression and anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [Google Scholar] [CrossRef]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prevent. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; de Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–796. [Google Scholar] [CrossRef]
- Bennie, J.A.; Teychenne, M.J.; De Cocker, K.; Biddle, S.J.H. Associations between aerobic and muscle-strengthening exercise with depressive symptom severity among 17,839 U.S. adults. Prevent. Med. 2019, 121, 121–127. [Google Scholar] [CrossRef]
- Ibrahim, N.; Amit, N.; Shahar, S.; Wee, L.H.; Ismail, R.; Khairuddin, R.; Siau, C.S.; Safien, A.M. Do depression literacy, mental illness beliefs and stigma influence mental health help-seeking attitude? A cross-sectional study of secondary school and university students from B40 households in Malaysia. BMC Public Health 2019, 19, 544. [Google Scholar] [CrossRef]
- Reavley, N.J.; McCann, T.V.; Jorm, A.F. Mental health literacy in higher education students. Early Interv. Psychiatry 2012, 6, 45–52. [Google Scholar] [CrossRef]
- McLafferty, M.; Armour, C.; Bunting, B.; Ennis, E.; Lapsley, C.; Murray, E.; O’Neill, S. Coping, stress, and negative childhood experiences: The link to psychopathology, self-harm, and suicidal behavior. PsyCh J. 2019, 8, 293–306. [Google Scholar] [CrossRef]
- Che Rahimi, A.; Bakar, R.S.; Mohd Yasin, M.A. Psychological well-being of Malaysian university students during COVID-19 pandemic: Do religiosity and religious coping matter? Healthcare 2021, 9, 1535. [Google Scholar] [CrossRef]
- Roviello, V.; Gilhen-Baker, M.; Vicidomini, C.; Roviello, G.N. Forest-bathing and physical activity as weapons against COVID-19: A review. Environ. Chem. Lett. 2022, 20, 131–140. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Branch of Science | Eligible (N = 85,024) | Analysed (N = 1231) | ||
|---|---|---|---|---|
| N | % | N | % | |
| Medicine and Health Sciences (MHS) | 12,930 | 15.2 | 630 | 51.1 |
| Comparison group (CG) | 72,094 | 84.8 | 601 | 49.9 |
| Social and Natural Sciences | 53,048 | 73.5 | 423 | 70.3 |
| Humanities and Arts | 9304 | 12.9 | 125 | 20.8 |
| Technological and Agricultural Sciences | 9742 | 13.5 | 53 | 9 |
| Variables | Medicine and Health Sciences (N = 630) | Comparison Group † (N = 601) | V a/d b | Total (N = 1231) | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Age (yr), mean ± SD | 21.8 ± 3.8 | 21.4 ± 3.5 | 0.1 b | 21.6 ± 3.7 | |||
| Year of study | |||||||
| 1st | 226 | 48.4 | 241 | 51.6 | 0.2 b,*** | 467 | 37.9 |
| 2nd | 140 | 46.7 | 160 | 53.3 | 300 | 24.4 | |
| 3rd | 82 | 45.8 | 97 | 54.2 | 179 | 14.5 | |
| 4–6th | 182 | 63.9 | 103 | 36.1 | 285 | 23.2 | |
| Income (euros (€) per month) | |||||||
| <200 | 213 | 46.6 | 243 | 53.4 | 0.04 b | 456 | 37 |
| 200–500 | 201 | 44.5 | 250 | 55.5 | 451 | 36.6 | |
| >500 | 146 | 45 | 178 | 55 | 324 | 26.3 | |
| Marital status | |||||||
| Married | 31 | 54.4 | 26 | 45.6 | 0.03 a | 57 | 4.6 |
| Single | 591 | 50.9 | 571 | 49.1 | 1162 | 94.4 | |
| Divorced | 8 | 66.7 | 4 | 33.3 | 12 | 1 | |
| Housing | |||||||
| In one‘s own apartment | 76 | 58.9 | 53 | 41.1 | 0.1 a | 129 | 10.5 |
| In a rented apartment | 157 | 47.4 | 174 | 52.6 | 331 | 26.9 | |
| With parents | 247 | 54.6 | 205 | 45.4 | 452 | 36.7 | |
| With friends | 34 | 58.6 | 24 | 41.4 | 58 | 4.7 | |
| With relatives | 10 | 58.8 | 7 | 41.2 | 17 | 1.4 | |
| In a dormitory | 106 | 43.4 | 138 | 56.6 | 244 | 19.8 | |
| HADS-A score, mean ± SD | 9.6 ± 4.5 | 11.7 ± 4.4 | 10.4 ± 4.5 | ||||
| Asymptomatic (score ≤ 7) | 220 | 62.9 | 130 | 37.1 | 0.4 b,*** | 350 | 28.4 |
| Borderline (score: 8–10) | 129 | 53.3 | 113 | 46.7 | 242 | 19.7 | |
| Severe (case) (score ≥ 11) | 281 | 44 | 358 | 56 | 639 | 51.9 | |
| HADS-D score, mean ± SD | 5.2 ± 3.5 | 6.4 ± 3.8 | 5.8 ± 3.7 | ||||
| Asymptomatic (score ≤ 7) | 478 | 54.9 | 392 | 45.1 | 0.3 b,*** | 870 | 70.7 |
| Borderline (score: 8–10) | 102 | 45.1 | 124 | 54.9 | 226 | 18.4 | |
| Severe (case) (score ≥ 11) | 50 | 37 | 85 | 63 | 135 | 11 | |
| PHQ-15 score, mean ± SD | 10.6 ± 5.3 | 11.5 ± 5.3 | 11.1 ± 5.3 | ||||
| Asymptomatic (score < 7) | 101 | 56.3 | 78 | 43.8 | 0.2 b,*** | 179 | 14.6 |
| Mild (score: 5–10) | 198 | 45.6 | 235 | 54.4 | 433 | 35.2 | |
| Moderate (score: 11–14) | 149 | 41.8 | 208 | 58.2 | 357 | 29 | |
| Severe (case) (score ≥ 15) | 101 | 42.3 | 151 | 57.7 | 262 | 21.3 | |
| Baecke total score, mean ± SD | 7.9 ± 1.3 | 7.4 ± 1.3 | 0.4 b,*** | 7.7 ± 1.3 | |||
| Sport index score, mean ± SD | 2.6 ± 0.7 | 2.3 ± 0.7 | 0.4 b,*** | 2.5 ± 0.7 | |||
| Leisure index score, mean ± SD | 2.8 ± 0.6 | 2.7 ± 0.6 | 0.2 b,*** | 2.7 ± 0.6 | |||
| Work index score, mean ± SD | 2.6 ± 0.6 | 2.4 ± 0.6 | 0.3 b,*** | 2.5 ± 0.6 | |||
| PHQ-15 Score | Medicine and Health Sciences 1 | Comparison Group 2,† | ||||
|---|---|---|---|---|---|---|
| Β | 95% CI | p | β | 95% CI | p | |
| HADS-A score | 0.6 | (0.5; 0.7) | <0.0001 | 0.5 | (0.4; 0.6) | <0.0001 |
| HADS-D score | 0.3 | (0.2; 0.4) | <0.0001 | 0.2 | (0.04; 0.3) | 0.007 |
| Variables | Baecke Index (Score) | Sport Index (Score) | Work Index (Score) | Leisure Index (Score) | ||||
|---|---|---|---|---|---|---|---|---|
| β (SE) | ORadj (95% CI) | β (SE) | ORadj (95% CI) | β (SE) | ORadj (95% CI) | β (SE) | ORadj (95% CI) | |
| Medicine and Health Sciences | ||||||||
| HADS-A score ≥ 11 1,a | 0.2 (0.3) | 1.2 (0.6–2.4) | 0.02 (0.3) | 0.9 (0.6–1.7) | 0.5 (0.3) | 1.6 (1–2.6) | –0.4 (0.3) | 0.7 (0.4–1.1) |
| HADS-D score ≥ 11 2,b | –0.4 (0.6) | 0.9 (0.2–3.1) | –1.1 (0.5) * | 0.4 (0.1–1) | 0.2 (0.4) | 1.2 (0.5–2.8) | –0.1 (0.4) | 0.9 (0.4–2) |
| Comparison group † | ||||||||
| HADS-A score ≥ 11 3,c | 0.2 (0.3) | 1.2 (0.6–2.2) | –0.1 (0.2) | 0.9 (0.5–1.5) | 0.2 (0.2) | 1.2 (0.8–1.9) | 0.1 (0.2) | 1.1 (0.7–1.8) |
| HADS-D score ≥ 11 4,d | –0.4 (0.4) | 0.7 (0.3–1.6) | –0.9 (0.4) * | 0.4 (0.2–0.9) | 0.2 (0.4) | 1.2 (0.6–2.4) | 0.4 (0.3) | 1.5 (0.8–2.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baranauskas, M.; Kupčiūnaitė, I.; Stukas, R. Mental Health and Physical Activity of Female Higher Education Students during the COVID-19 Pandemic: A Comparative Cross-Sectional Study from Lithuania. Int. J. Environ. Res. Public Health 2022, 19, 9725. https://doi.org/10.3390/ijerph19159725
Baranauskas M, Kupčiūnaitė I, Stukas R. Mental Health and Physical Activity of Female Higher Education Students during the COVID-19 Pandemic: A Comparative Cross-Sectional Study from Lithuania. International Journal of Environmental Research and Public Health. 2022; 19(15):9725. https://doi.org/10.3390/ijerph19159725
Chicago/Turabian StyleBaranauskas, Marius, Ingrida Kupčiūnaitė, and Rimantas Stukas. 2022. "Mental Health and Physical Activity of Female Higher Education Students during the COVID-19 Pandemic: A Comparative Cross-Sectional Study from Lithuania" International Journal of Environmental Research and Public Health 19, no. 15: 9725. https://doi.org/10.3390/ijerph19159725
APA StyleBaranauskas, M., Kupčiūnaitė, I., & Stukas, R. (2022). Mental Health and Physical Activity of Female Higher Education Students during the COVID-19 Pandemic: A Comparative Cross-Sectional Study from Lithuania. International Journal of Environmental Research and Public Health, 19(15), 9725. https://doi.org/10.3390/ijerph19159725