
A Comparative Study on Intention to Use Digital Therapeutics: MZ Generation and Baby Boomers’ Digital Therapeutics Use Intention in Korea


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Digital Literacy
2.2.2. Privacy Concern
2.2.3. Public Perception of Digital Therapeutics
2.2.4. Digital Therapeutics Use Intention
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Reliability and Validity of the Variables
3.2. The Types of Digital Literacy
3.3. Public Perceptions of Digital Therapeutics
3.4. The Difference between the MZ Generation and the Baby Boomers
3.4.1. The Relationship between Digital Literacy, Privacy Concern, DTx Perception, and DTx Use Intention
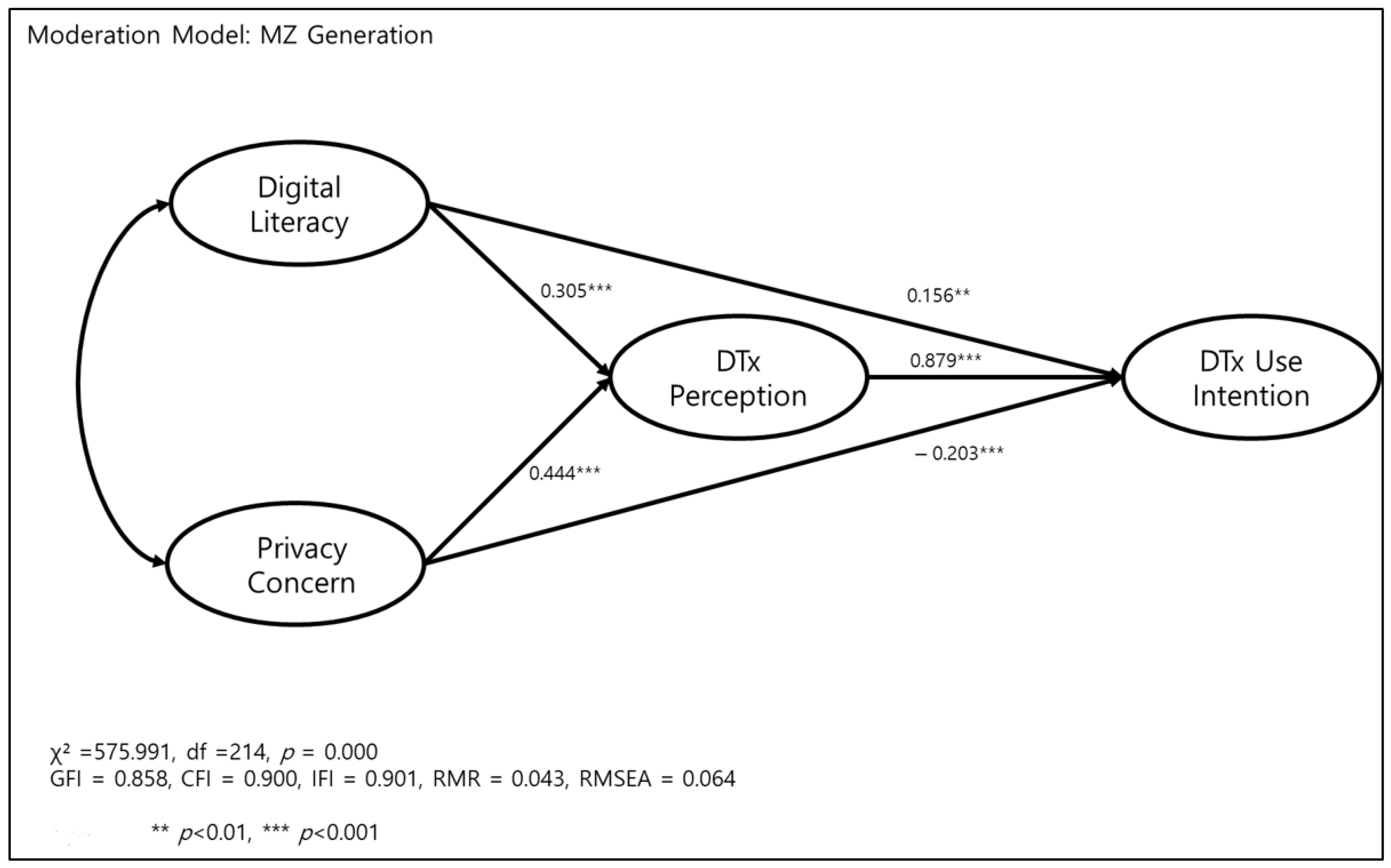
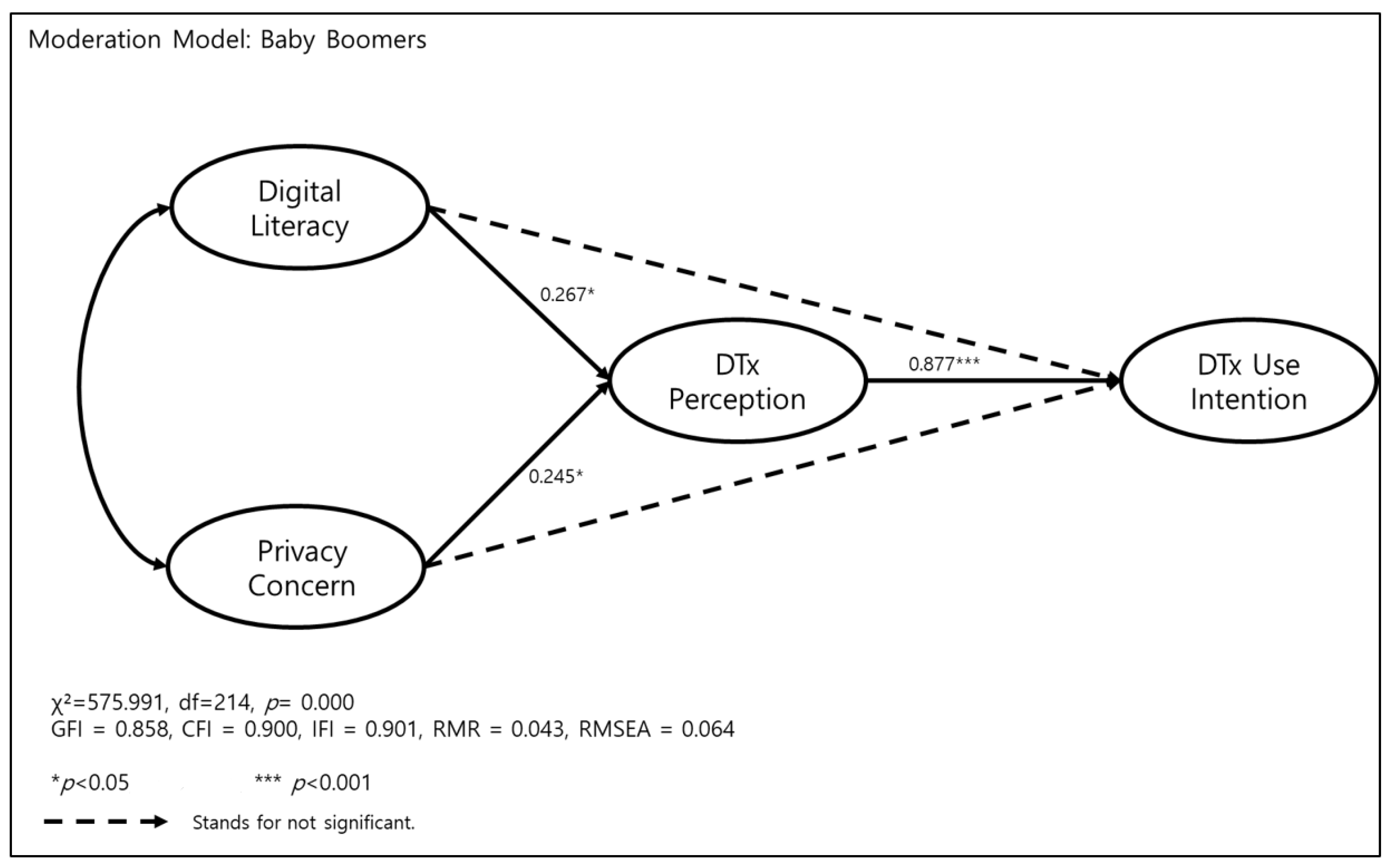
3.4.2. The Path Difference between the MZ Generation and the Baby Boomers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mathews, S.C.; McShea, M.J.; Hanley, C.L.; Ravitz, A.; Labrique, A.B.; Cohen, A.B. Digital health: A path to validation. NPJ Digit. Med. 2019, 2, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, W.H.; Park, J.W. Regulatory reform plans and strategies for the emerging digital healthcare industry. J. Regul. Stud. 2019, 27, 37–39. [Google Scholar]
- Lee, J.H. A research on the necessity for telemedicine in the digital healthcare era. Dong-A Law Rev. 2020, 88, 245–256. [Google Scholar] [CrossRef]
- Eom, J.H.; Choi, J.W. Artificial intelligence(AI) in healthcare and research. Future Med. Humanit. 2021, 4, 93–101. [Google Scholar]
- Korea Information Society Development Institute. Development Direction of Domestic Digital Healthcare, AI Trend Watch 2021;4. Available online: https://www.kisdi.re.kr/report/view.do?key=m2101113025339&arrMasterId=4311435&masterId=4311435&artId=555721 (accessed on 28 February 2022).
- Ministry of Health and Welfare. Health Data F.LO.W. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&page=1&CONT_SEQ=365938 (accessed on 28 February 2022).
- Korea Institute for Health and Social affairs. Current Status and Implications of Health Literacy among Korean Adults. Health Welf. Issue Focus 2021, 413, 1–10. Available online: http://repository.kihasa.re.kr/handle/201002/38740 (accessed on 28 February 2022).
- Shon, J.H.; Kim, C.S.; Lee, H.S. A study on the response of each generation to the communication characteristics of the MZ generation-Focusing on Generation, M.Z. Generation X, and Baby Boomers. J. Commun. Des. 2021, 77, 202–215. [Google Scholar]
- Shin, S.H. A Study on the Effect of IT Service Quality on User Satisfaction and Customer Loyalty: Focusing on the Perception Difference between the MZ Generation and the Existing Generation. Ind. Converg. Res. 2022, 20, 13–21. [Google Scholar]
- Bae, Y.I.; Shin, H.L. A Study on the Consumer Acceptance of Digital Healthcare Service, Gyeonggi Research Institute. 2019. Available online: https://www.gri.re.kr/%EC%97%B0%EA%B5%AC%EB%B3%B4%EA%B3%A0%EC%84%9C/?brno=14411&prno=6490 (accessed on 28 February 2022).
- Survey for Government Policies Regarding Strategies for the Commercialization and Globalization of Digital Therapeutics. Yonsei Med. J. 2022, 63, S56. [CrossRef]
- Yan, K.; Balijepalli, C.; Druyts, E. The Impact of Digital Therapeutics on Current Health Technology Assessment Frameworks. Front. Digit. Health 2021, 3, 667016. [Google Scholar] [CrossRef] [PubMed]
- Guidance Document Software as a Medical Device (SaMD): Definition and Classification. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-devices/application-information/guidance-documents/software-medical-device-guidance-document.html (accessed on 28 February 2022).
- FDA. Software as a Medical Device (SAMD): Clinical Evaluation 2017. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/software-medical-device-samd-clinical-evaluation (accessed on 28 February 2022).
- Agency UMaHpR. Guidance: Medical Device Stand-Alone Software Including Apps (Including IVDMDs) 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/999908/Software_flow_chart_Ed_1-08b-IVD.pdf (accessed on 28 February 2022).
- Sverdlov, O.; Dam, J.V.; Hannesdottir, K.; Thornton-Wells, T. Digital therapeutics: An integral component of digital innovation in drug development. Clin. Pharmacol. Ther. 2018, 104, 72–80. [Google Scholar] [CrossRef]
- Lawrence, E.M. Why do college graduates behave more healthfully than those who are less educated? J. Health Soc. Behav. 2017, 58, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.A.; Truman, B.I. Education improves public health and promotes health equity. Int. J. Health Serv. 2015, 45, 657–678. [Google Scholar] [CrossRef]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaportzis, E.; Clausen, M.G.; Gow, A.J. Older adults perceptions of technology and barriers to interacting with tablet computers: A focus group study. Front. Psychol. 2017, 8, 1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, N.P.; Hornbrook, M.C. Older adults’ readiness to engage with eHealth patient education and self-care resources: A cross-sectional survey. BMC Health Serv. Res. 2018, 18, 220. [Google Scholar] [CrossRef] [PubMed]
- Korean Statistical Information Service. Korean Census Data. Available online: https://kosis.kr/index/index.do (accessed on 28 February 2022).
- Eshet, Y. Digital literacy: A conceptual framework for survival skills in the digital era. J. Educ. Multimed. Hypermedia 2004, 13, 93–106. [Google Scholar]
- Eshet-Alkalai, Y.; Eran, C. You can teach old dogs new tricks: The factors that affect changes over time in digital literacy. J. Inf. Educ. Technol. 2010, 9, 173–181. [Google Scholar] [CrossRef]
- Malhotra, N.K.; Sung, S.K.; James, A. Internet users’ information privacy concerns (IUIPC): The construct, the scale, and a causal model. Inf. Syst. Res. 2004, 15, 336–355. [Google Scholar] [CrossRef] [Green Version]
- Williams, S.J.; Seale, C.; Boden, S.; Lowe, P.; Steinberg, D.L. Medicalization and beyond: The social construction of insomnia and snoring in the news. Health 2008, 12, 251–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilton, S.; Hunt, K.; Langan, M.; Bedford, H.; Petticrew, M. Newsprint media representations of the introduction of the HPV vaccination programme for cervical cancer prevention in the UK (2005–2008). Soc. Sci. Med. 2010, 70, 942–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| M | SD | (1) | (2) | (3) | (4) | |
|---|---|---|---|---|---|---|
| (1) Digital literacy | 3.45 | 0.60 | 1 | |||
| (2) Privacy concern | 3.98 | 0.58 | 0.174 ** | 1 | ||
| (3) DTx perception | 3.53 | 0.34 | 0.273 ** | 0.502 ** | 1 | |
| (4) DTx use intention | 3.51 | 0.68 | 0.317 ** | 0.195 ** | 0.435 ** | 1 |
| Factors | |||
|---|---|---|---|
| Information Utilization Ability | Creative Producing Ability | Digital Communication Ability | |
| I can send MP3 files to others. | 0.874 | 0.126 | 0.127 |
| I can upload my files to web-hards on the internet, etc. | 0.851 | 0.218 | 0.054 |
| I can configure the web browser (Explorer, etc.). | 0.848 | 0.161 | 0.133 |
| I use the Internet well for my work/class. | 0.844 | 0.168 | 0.161 |
| I can find the information I need through a search engine. | 0.764 | −0.055 | 0.249 |
| I can understand exactly what the information conveys. | 0.759 | 0.124 | 0.233 |
| I can express what I want to say through pictures or videos on the Internet. | 0.640 | 0.409 | 0.297 |
| As a fan of celebrities such as stars, sportsmen, politicians, and CEOs, I can produce fan art such as videos, audio, and pictures. | 0.026 | 0.877 | 0.078 |
| I can parody or remix drama music videos, popular songs, and movies with audio and video. | 0.072 | 0.866 | 0.076 |
| I decorate and manage my blog or mini-homepage well. | 0.168 | 0.718 | 0.252 |
| I am good with digital cameras and camcorders. | 0.436 | 0.640 | 0.127 |
| I express my intentions clearly in writing on the Internet. | 0.255 | 0.556 | 0.410 |
| I use the Internet to send group messages or texts to my friends. | 0.117 | 0.213 | 0.795 |
| I use the internet to send my regards to my friends. | 0.170 | 0.242 | 0.795 |
| By using the Internet, I have come to understand myself and others better. | 0.124 | 0.140 | 0.781 |
| I think the Internet provides an important opportunity to get to know a variety of people from different regions. | 0.301 | 0.003 | 0.707 |
| Kaiser–Meyer–Olkin (KMO): 0.894, Bartlett’s Test of Sphericity: 6421.587, df = 120, p = 0.000 | |||
| Eigen Value | 4.927 | 3.181 | 2.899 |
| % of Variance Explained | 30.795 | 19.879 | 18.122 |
| Cumulative Variance Explained | 30.795 | 50.673 | 68.795 |
| Cronbach’s α | 0.927 | 0.845 | 0.825 |
| M | 3.954 | 2.832 | 3.589 |
| Factors | |||||||
|---|---|---|---|---|---|---|---|
| Regulation Need | Cost Efficiency | Health Benefit | Medical Concern | Device credibility | Health Inequality | Uncertain Literacy | |
| To use digital therapeutics, guidelines for cybersecurity permission and examination of medical devices must be prepared. | 0.835 | 0.113 | 0.208 | −0.045 | 0.078 | 0.052 | −0.092 |
| Personal information protection regulations for the use of digital therapeutics should be strengthened. | 0.805 | 0.118 | 0.137 | 0.025 | 0.111 | 0.038 | −0.034 |
| To use digital therapeutics, screening criteria such as permission for medical devices applied with big data, VR, and AI technologies must be clear. | 0.797 | 0.110 | 0.246 | −0.050 | 0.055 | 0.014 | −0.064 |
| For digital therapies, the stability of technology is the most important. | 0.712 | 0.227 | −0.041 | 0.156 | −0.156 | 0.084 | 0.111 |
| Expectations for digital therapeutics are high, but there is still a long way to go in terms of licensing, insurance, and data utilization. | 0.686 | 0.033 | 0.025 | 0.089 | 0.046 | 0.140 | 0.276 |
| The interest and support of the government are essential for the development of digital therapeutics. | 0.589 | 0.380 | 0.123 | 0.129 | −0.091 | 0.081 | 0.129 |
| As we enter an aging society, disease management programs such as digital treatments will be more necessary. | 0.540 | 0.395 | 0.285 | −0.024 | −0.116 | 0.175 | −0.141 |
| For digital therapeutics, the effectiveness of technology (therapeutic effect) is the most important. | 0.513 | 0.274 | 0.122 | 0.183 | −0.141 | 0.059 | 0.206 |
| If it is possible to claim private health insurance, I am willing to use digital therapeutics. | 0.280 | 0.747 | 0.154 | 0.077 | −0.087 | −0.036 | 0.096 |
| If it is digital therapeutics developed by conglomerates, I am willing to use it. | 0.030 | 0.714 | 0.258 | 0.078 | −0.004 | 0.067 | 0.142 |
| I am willing to use digital therapeutics if they are not expensive. | 0.266 | 0.710 | 0.225 | 0.010 | −0.150 | 0.017 | 0.018 |
| If digital treatment is successful in treating obesity, I am willing to use digital therapeutics. | 0.227 | 0.677 | 0.089 | 0.098 | 0.059 | 0.205 | −0.101 |
| If medical efficacy has been proven, I am quite positive about digital therapeutics. | 0.343 | 0.536 | 0.371 | −0.008 | −0.121 | 0.051 | −0.131 |
| People who know how to use digital therapeutics will be healthier. | −0.014 | 0.516 | 0.196 | −0.027 | 0.019 | 0.504 | −0.085 |
| Digital therapeutics can treat medical diseases and disability. | 0.003 | 0.188 | 0.818 | 0.065 | −0.127 | 0.079 | 0.039 |
| Digital therapeutics can treat medical disorders. | 0.057 | 0.139 | 0.797 | 0.081 | −0.091 | 0.029 | 0.038 |
| You can see your health condition through digital therapeutics. | 0.260 | 0.299 | 0.639 | −0.003 | −0.033 | 0.066 | 0.009 |
| Digital therapeutics help manage and prevent chronic diseases. | 0.431 | 0.186 | 0.579 | −0.051 | −0.061 | 0.026 | −0.131 |
| Digital therapies can get help optimizing medication (taking your medication) through digital treatment. | 0.376 | 0.273 | 0.578 | −0.023 | −0.008 | 0.025 | −0.132 |
| If doctors are reluctant to prescribe digital therapeutics, it may be because they are concerned about the side effects of using digital devices themselves. | 0.155 | 0.029 | 0.025 | 0.742 | 0.103 | 0.027 | 0.033 |
| If doctors are reluctant to prescribe digital therapeutics, the reason may be that the treatment effect has not been sufficiently proven. | 0.223 | 0.053 | −0.078 | 0.709 | 0.049 | −0.184 | 0.110 |
| If doctors are reluctant to prescribe digital therapeutics, the reason may be that they do not expect patients to use digital devices well. | −0.031 | 0.045 | 0.086 | 0.643 | 0.115 | 0.237 | 0.097 |
| If doctors are reluctant to prescribe digital therapeutics, it is probably because they are not used to using digital devices. | −0.062 | 0.120 | −0.016 | 0.510 | 0.112 | 0.397 | 0.020 |
| If doctors are reluctant to prescribe digital therapeutics, it may be because they are not yet covered by health insurance or indemnity insurance. | 0.071 | 0.131 | 0.035 | 0.447 | 0.034 | 0.404 | −0.278 |
| If doctors are reluctant to prescribe digital therapeutics, it may be because they think it is inhumane or unethical to use digital devices for treatment. | −0.231 | −0.101 | 0.195 | 0.445 | 0.351 | 0.158 | 0.280 |
| Digital therapeutics are unlikely to be as effective as those using conventional drugs and medical devices. | 0.077 | 0.045 | −0.136 | 0.063 | 0.796 | −0.071 | −0.020 |
| I do not trust the use of digital therapeutics without seeing a doctor or using digital therapeutics without a doctor’s prescription. | 0.126 | −0.124 | −0.195 | 0.148 | 0.713 | 0.029 | 0.107 |
| I think it is inhumane to treat people through digital devices without seeing a doctor. | −0.261 | −0.145 | 0.041 | 0.253 | 0.626 | 0.031 | 0.212 |
| If the use of digital therapeutics become active, there will be a health gap between those who can use them and those who don’t. | 0.138 | −0.007 | 0.091 | 0.154 | 0.007 | 0.736 | 0.194 |
| If the use of digital therapeutics become active, there will be differences in patient preferences between hospitals that prescribe digital therapeutics and those that do not. | 0.343 | 0.191 | 0.000 | 0.095 | −0.105 | 0.651 | 0.166 |
| It is not an easy task to learn and use the use of digital therapeutics. | 0.090 | 0.046 | −0.042 | 0.114 | 0.204 | 0.172 | 0.762 |
| There are many problems to be solved before getting used to digital therapeutics. | 0.535 | 0.069 | −0.083 | 0.162 | 0.073 | 0.076 | 0.553 |
| Kaiser–Meyer–Olkin (KMO): 0.870, Bartlett’s Test of Sphericity: 3685.262, df = 55, p = 0.000 | |||||||
| Eigen Value | 5.234 | 3.431 | 3.072 | 2.410 | 1.922 | 1.834 | 1.470 |
| % of Variance Explained | 16.356 | 10.721 | 9.600 | 7.532 | 6.007 | 5.731 | 4.595 |
| Cumulative Variance Explained | 16.356 | 27.078 | 36.677 | 44.209 | 50.216 | 55.947 | 60.542 |
| Cronbach’s α | 0.890 | 0.826 | 0.826 | 0.699 | 0.645 | 0.664 | 0.642 |
| Mean | 4.07 | 3.64 | 3.49 | 3.33 | 3.00 | 3.58 | 3.60 |
| Variables | Dimensions | Groups | M | SD |
|---|---|---|---|---|
| Health Literacy | Information utilization ability | MZ | 4.14 | 0.71 |
| Baby boomers | 3.81 | 0.69 | ||
| Creative production ability | MZ | 3.04 | 0.86 | |
| Baby boomers | 2.67 | 0.76 | ||
| Digital communication ability | MZ | 3.62 | 0.76 | |
| Baby boomers | 3.56 | 0.68 | ||
| Privacy Concern | Collection | MZ | 3.85 | 0.69 |
| Baby boomers | 3.92 | 0.62 | ||
| Control | MZ | 3.93 | 0.66 | |
| Baby boomers | 3.93 | 0.61 | ||
| Awareness | MZ | 4.09 | 0.74 | |
| Baby boomers | 4.15 | 0.66 | ||
| DTx Perception | Regulation need (dtxF1) | MZ | 4.04 | 0.62 |
| Baby boomers | 4.09 | 0.54 | ||
| Cost efficiency (dtxF2) | MZ | 3.66 | 0.60 | |
| Baby boomers | 3.62 | 0.55 | ||
| Health benefit (dtxF3) | MZ | 3.46 | 0.58 | |
| Baby boomers | 3.50 | 0.55 | ||
| Medical concern (dtxF4) | MZ | 3.33 | 0.60 | |
| Baby boomers | 3.33 | 0.54 | ||
| Device credibility (dtxF5) | MZ | 30.08 | 0.70 | |
| Baby boomers | 2.94 | 0.63 | ||
| Health inequality (dtxF6) | MZ | 3.62 | 0.70 | |
| Baby boomers | 3.55 | 0.65 | ||
| Uncertain literacy (dtxF7) | MZ | 3.64 | 0.66 | |
| Baby boomers | 3.57 | 0.63 | ||
| DTx Use Intention | MZ | 3.50 | 0.70 | |
| Baby boomers | 3.52 | 0.67 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Eom, J.; Shim, J. A Comparative Study on Intention to Use Digital Therapeutics: MZ Generation and Baby Boomers’ Digital Therapeutics Use Intention in Korea. Int. J. Environ. Res. Public Health 2022, 19, 9556. https://doi.org/10.3390/ijerph19159556
Kim S, Eom J, Shim J. A Comparative Study on Intention to Use Digital Therapeutics: MZ Generation and Baby Boomers’ Digital Therapeutics Use Intention in Korea. International Journal of Environmental Research and Public Health. 2022; 19(15):9556. https://doi.org/10.3390/ijerph19159556
Chicago/Turabian StyleKim, Soojin, Juhee Eom, and Jiwon Shim. 2022. "A Comparative Study on Intention to Use Digital Therapeutics: MZ Generation and Baby Boomers’ Digital Therapeutics Use Intention in Korea" International Journal of Environmental Research and Public Health 19, no. 15: 9556. https://doi.org/10.3390/ijerph19159556
APA StyleKim, S., Eom, J., & Shim, J. (2022). A Comparative Study on Intention to Use Digital Therapeutics: MZ Generation and Baby Boomers’ Digital Therapeutics Use Intention in Korea. International Journal of Environmental Research and Public Health, 19(15), 9556. https://doi.org/10.3390/ijerph19159556