
Caregivers’ Compliance and Perception of Daycare Centers—A Community-Based Childhood Drowning Prevention Intervention Implemented in Rural Bangladesh

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Setting, Procedure, and Implementation
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Characteristics of the Respondents
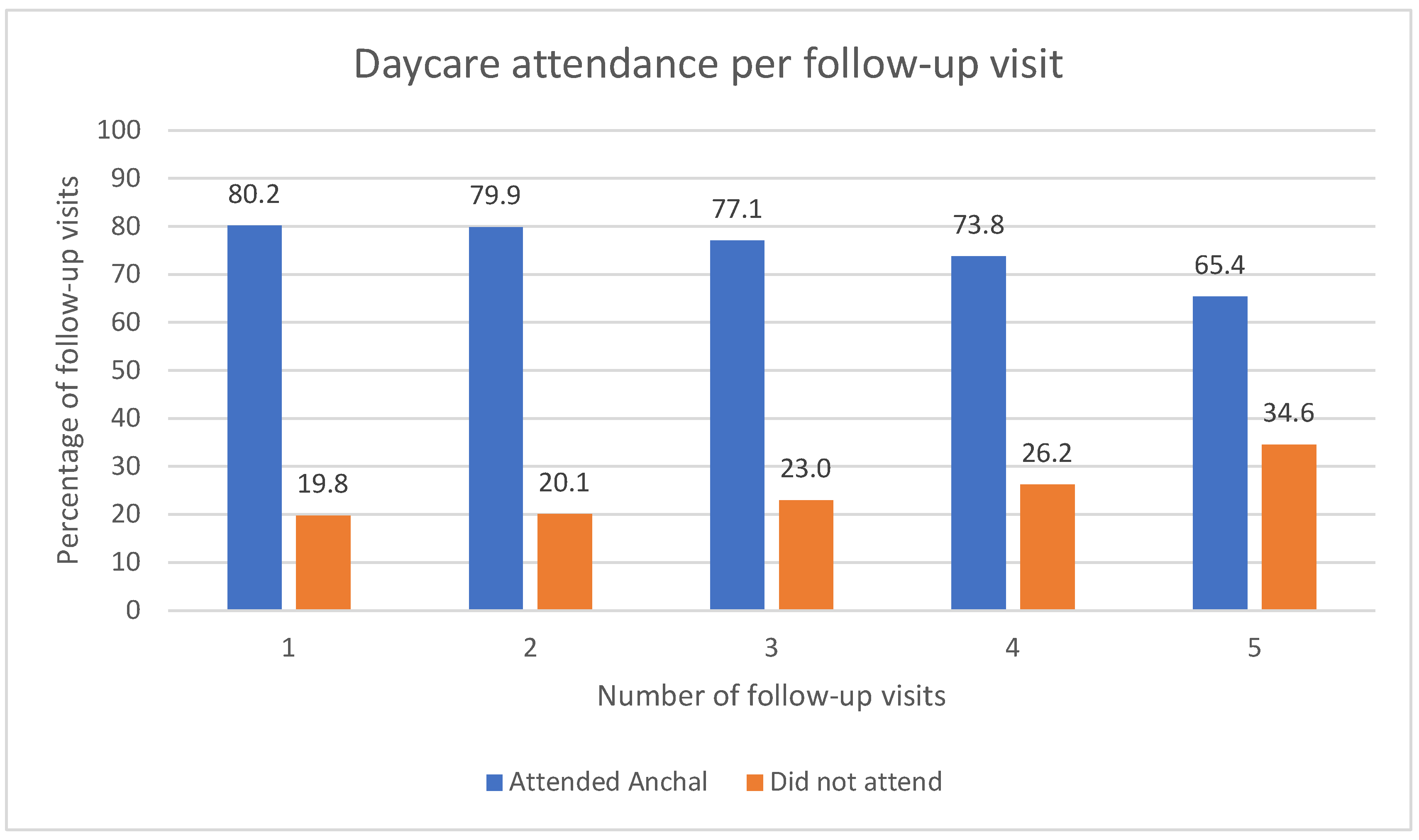
3.2. Daycare Attendance
3.3. General Perception and Satisfaction towards Daycare
3.4. Respondents’ Engagement in Income-Generating Activities and Household Chores
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leavy, J.E.; Crawford, G.; Leaversuch, F.; Nimmo, L.; McCausland, K.; Jancey, J. A review of drowning prevention interventions for children and young people in high-, low- and middle-income countries. J. Community Health 2016, 41, 424–441. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Population Research and Training (NIPORT) and ICF. Bangladesh Demographic and Health Survey 2017–18. Dhaka, Bangladesh, and Rockville, Maryland, USA: NIPORT and ICF. 2020. Available online: https://dhsprogram.com/pubs/pdf/FR344/FR344.pdf (accessed on 1 August 2021).
- Bangladesh Bureau of Statistics. Report on Bangladesh Sample Vital Statistics. 2020. Available online: http://bbs.portal.gov.bd/sites/default/files/files/bbs.portal.gov.bd/page/b343a8b4_956b_45ca_872f_4cf9b2f1a6e0/2021-06-28-07-11-c1784c6fe700cf52ff934e8dd7cf9147.pdf (accessed on 9 September 2021).
- Peden, A.E.; Franklin, R.C.; Leggat, P.A. Developing drowning prevention strategies for rivers through the use of a modified Delphi process. Inj. Prev. 2019, 26, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyder, A.A.; Borse, N.N.; Blum, L.; Khan, R.; El Arifeen, S.; Baqui, A.H. Childhood drowning in low- and middle-income countries: Urgent need for intervention trials. J. Paediatr. Child Health 2008, 44, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Szpilman, D. Drowning. In The Science of Beach Lifeguarding; CRC Press: Boca Raton, FL, USA, 2018; pp. 143–160. [Google Scholar]
- Leavy, J.E.; Crawford, G.; Portsmouth, L.; Jancey, J.; Leaversuch, F.; Nimmo, L.; Hunt, K. Recreational drown-ing prevention interventions for adults, 1990–2012: A review. J. Community Health 2015, 40, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Alonge, O.; Bhuiyan, A.A.; Agrawal, P.; Salam, S.S.; Talab, A.; Rahman, Q.S.; Hyder, A.A. Epide-miology of drowning in Bangladesh: An update. Int. J. Environ. Res. Public Health 2017, 14, 488. [Google Scholar] [CrossRef] [PubMed]
- Alonge, O.; Bishai, D.; Wadhwaniya, S.; Agrawal, P.; Rahman, A.; Hoque, E.M.D.; Baset, K.U.; Salam, S.S.; Bhuiyan, A.-A.; Islam, I.; et al. Large-scale evaluation of interventions designed to reduce childhood Drownings in rural Bangladesh: A before and after cohort study. Inj. Epidemiol. 2020, 7, 1–12. [Google Scholar] [CrossRef]
- Nair, D.; Alonge, O.; Hamadani, J.D.; Salam, S.S.; Islam, I.; Hyder, A.A. Developmental Assessments during Injury Research: Is Enrollment of Very Young Children in Crèches Associated with Better Scores? Int. J. Environ. Res. Public Health 2017, 14, 1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, P.S. Project to Prevent Drowning Deaths. Prothom Alo. 21 September 2021. Available online: https://www.prothomalo.com/bangladesh/%E0%A6%AA%E0%A6%BE%E0%A6%A8%E0%A6%BF%E0%A6%A4%E0%A7%87-%E0%A6%A1%E0%A7%81%E0%A6%AC%E0%A7%87-%E0%A6%AE%E0%A7%83%E0%A6%A4%E0%A7%8D%E0%A6%AF%E0%A7%81-%E0%A6%B0%E0%A7%87%E0%A6%BE%E0%A6%A7%E0%A7%87-%E0%A6%AA%E0%A7%8D%E0%A6%B0%E0%A6%95%E0%A6%B2%E0%A7%8D%E0%A6%AA (accessed on 10 July 2021).
- Mazumder, S.H. Development of Daycare Facility: The Inimitable Solution to Reduce Child Drowning. The Independent, Bangladesh. 3 May 2019. Available online: https://m.theindependentbd.com/home/printnews/198026 (accessed on 21 July 2021).
- Vecino-Ortiz, A.I.; Jafri, A.; Hyder, A.A. Effective interventions for unintentional injuries: A systematic re-view and mortality impact assessment among the poorest billion. Lancet Glob. Health 2018, 6, e523–e534. [Google Scholar] [CrossRef]
- Crawford, B.R.; Siahainenia, A.; Rotinsulu, C.; Sukmara, A. Compliance and Enforcement of Community-Based Coastal Resource Management Regulations in North Sulawesi, Indonesia. Coast. Manag. 2004, 32, 39–50. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomeroy, R.; Parks, J.; Reaugh-Flower, K.; Guidote, M.; Govan, H.; Atkinson, S. Status and Priority Capacity Needs for Local Compliance and Community-Supported Enforcement of Marine Resource Rules and Regulations in the Coral Triangle Region. Coast. Manag. 2015, 43, 301–328. [Google Scholar] [CrossRef]
- Hyder, A.A.; Alonge, O.; He, S.; Wadhwaniya, S.; Rahman, F.; Rahman, A.; Arifeen, S. Saving of Children’s Lives from Drowning Project in Bangladesh. Am. J. Prev. Med. 2014, 47, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Hyder, A.A.; Alonge, O.; He, S.; Wadhwaniya, S.; Rahman, F.; Rahman, A.; El Arifeen, S. A Framework for Addressing Implementation Gap in Global Drowning Prevention Interventions: Experiences from Bangladesh. J. Heal. Popul. Nutr. 2014, 32, 564–576. [Google Scholar]
- Alonge, O.; Agrawal, P.; Talab, A.; Rahman, Q.S.; Rahman, A.F.; Arifeen, S.; Hyder, A.A. Fatal and non-fatal injury outcomes: Results from a purposively sampled census of seven rural subdistricts in Bangladesh. Lancet Glob. Health 2017, 5, e818–e827. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- De Buck, E.; Vanhove, A.C.; Dorien, O.; Veys, K.; Lang, E.; Vandekerckhove, P. Daycare as a strategy for drowning prevention in children under 6 years of age in low-and middle-income countries. Cochrane Datab. Syst. Rev. 2021, 4, CD014955. [Google Scholar] [CrossRef]
- Rahman, A.; Shafinaz, S.; Linnan, M.; Rahman, F. Community perception of childhood drowning and its pre-vention measures in rural Bangladesh: A qualitative study. Aust. J. Rural Health 2008, 16, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Rahman, A.; Dutta, N.C.; Saha, A.K.; Zwi, A.; Ivers, R.Q.; Jagnoor, J. Implementing a crèche-based community drowning programme in rural Bangladesh: A process evaluation. Inj. Prev. 2021, 28, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Miah, A.H.; Mashreky, S.; Shafinaz, S.; Linnan, M.; Rahman, F. Initial community response to a childhood drowning prevention programme in a rural setting in Bangladesh. Inj. Prev. 2010, 16, 21–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klassen, T.P.; MacKay, J.M.; Moher, D.; Walker, A.; Jones, A.L. Community-based injury prevention interventions. Future Child. 2000, 10, 83–110. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Khanam, M.; Bhuiyan, M.A.-A.; Rahman, A.F. PW 2181 Effectiveness of adolescent brigade in enhancing child drowning prevention programme in bangladesh. Abstracts 2018, 24, A160. [Google Scholar] [CrossRef]
- Survey Analysis Using Likert Scale. 2016. Available online: https://www.manuscriptedit.com/scholar-hangout/survey-analysis-likert-scale/ (accessed on 17 August 2021).
- World Health Organization. WHO Guideline on the Prevention of Drowning through Provision of Day-Care and Basic Swimming and Water Safety Skills. 2021. Available online: https://www.who.int/publications/i/item/9789240030008 (accessed on 9 September 2021).

{kind=link}
| Characteristics of Respondents in Each Follow-up Visit | ||||||
|---|---|---|---|---|---|---|
| Number of Respondents, n (%) | ||||||
| 1st N = 67,232 | 2nd N = 59,806 | 3rd N = 48,058 | 4th N = 34,824 | 5th N = 16,645 | Total | |
| Relation with child | ||||||
| Mother | 64,734 (96.7) | 57,893 (97.2) | 46,740 (97.6) | 33,981 (98.0) | 16,316 (98.3) | 219,664 (97.3) |
| Father | 444 (0.7) | 328 (0.6) | 196 (0.4) | 133 (0.4) | 42 (0.3) | 1143 (0.5) |
| Sibling | 112 (0.2) | 83 (0.1) | 66(0.1) | 40 (0.1) | 21 (0.1) | 322 (0.1) |
| Other | 1673 (2.5) | 1264 (2.1) | 873 (1.8) | 529 (1.5) | 218 (1.3) | 4557(2.0) |
| Occupation | ||||||
| Agriculture | 485 (0.7) | 387 (0.7) | 245 (0.5) | 150 (0.4) | 38 (0.2) | 1305 (0.6) |
| Business | 248 (0.4) | 173 (0.3) | 114 (0.2) | 85 (0.3) | 16 (0.1) | 636 (0.3) |
| Student | 68 (0.1) | 49 (0.1) | 38 (0.1) | 17 (0.1) | 6 (0.0) | 178 (0.1) |
| Housewives 1 | 64,562 (97.0) | 57,741 (97.2) | 46,496 (97.4) | 33,805 (97.8) | 16,310 (99.1) | 218,914 (97.4) |
| Service | 806 (1.2) | 678 (1.1) | 534 (1.1) | 342 (1.0) | 80 (0.5) | 2440 (1.1) |
| Skilled labor | 167 (0.3) | 140 (0.2) | 111 (0.2) | 65 (0.2) | 10 (0.1) | 493 (0.2) |
| Unskilled labor/Domestic worker | 169 (0.3) | 143 (0.2) | 126 (0.3) | 56 (0.2) | 4 (0.0) | 498 (0.2) |
| Transport workers | 8 (0.0) | 7 (0.0) | 3 (0.0) | 3 (0.0) | 0 (0.0) | 21 (0.0) |
| Others | 80 (0.1) | 60 (0.1) | 47 (0.1) | 43 (0.1) | 3 (0.0) | 233 (0.1) |
| Across All Follow-ups | ||
|---|---|---|
| Reason for Sending Child to Daycare 1 | Frequency (n) n = 175,321 | Percentage |
| Child can stay safe | 142,846 | 81.5% |
| Remain tension free | 116,307 | 66.3% |
| Can learn reading/writing | 112,973 | 64.4% |
| Can do household chores | 108,489 | 61.9% |
| Can play | 95,237 | 54.3% |
| Can learn to dance/sing/recite/rhymes | 91,573 | 52.2% |
| Can learn cleanliness from daycare | 49,237 | 28.1% |
| Can learn manners and etiquette | 48,470 | 27.7% |
| Nobody else to supervise the child | 7394 | 4.2% |
| Other children attended | 4709 | 2.7% |
| Request from daycare supervisor | 3831 | 2.2% |
| Mother can work outside for money | 3404 | 1.9% |
| Neighbor’s suggestion | 2871 | 1.6% |
| Reasons | Frequency (n = 12,124) | Percentage (%) |
|---|---|---|
| Factors related to children | ||
| Child does not like being without family members | 1377 | 11.4 |
| Child terrified of attending daycare | 342 | 2.8 |
| Child remains sick | 281 | 2.3 |
| Child becomes tired | 137 | 1.1 |
| Child is too young to go to daycare | 95 | 0.8 |
| Child remains hungry at daycare | 80 | 0.7 |
| Child was injured at daycare | 43 | 0.4 |
| Child is disabled | 26 | 0.2 |
| Factors related to daycare | ||
| Too far | 5243 | 43.2 |
| Daycare shut down/opens irregularly/creche mother dropped out | 2502 | 20.6 |
| Creche mother/assistant could not manage/hit the child | 127 | 1.1 |
| Daycare is beside a pond | 37 | 0.3 |
| Factors related to families | ||
| No one available to take child to daycare (due to illness, family problems, etc.) | 3496 | 28.8 |
| Temporarily staying/visiting or moving out from the area | 358 | 3.0 |
| Conflict with work | 234 | 1.9 |
| No benefits to attending daycare | 107 | 0.9 |
| Stay at home mother can supervise | 38 | 0.3 |
| Miscellaneous factors | ||
| Alternative nearby a | 801 | 6.6 |
| Problem with transport during rainy season | 798 | 6.6 |
| Weather: cold/rain | 199 | 1.6 |
| Others b | 258 | 2.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashraf, L.; Agrawal, P.; Rahman, A.; Bhuiyan, M.A.A.; Salam, S.S.; Li, Q.; Bachani, A.M. Caregivers’ Compliance and Perception of Daycare Centers—A Community-Based Childhood Drowning Prevention Intervention Implemented in Rural Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 9537. https://doi.org/10.3390/ijerph19159537
Ashraf L, Agrawal P, Rahman A, Bhuiyan MAA, Salam SS, Li Q, Bachani AM. Caregivers’ Compliance and Perception of Daycare Centers—A Community-Based Childhood Drowning Prevention Intervention Implemented in Rural Bangladesh. International Journal of Environmental Research and Public Health. 2022; 19(15):9537. https://doi.org/10.3390/ijerph19159537
Chicago/Turabian StyleAshraf, Lamisa, Priyanka Agrawal, Aminur Rahman, Md. Al Amin Bhuiyan, Shumona Sharmin Salam, Qingfeng Li, and Abdulgafoor M. Bachani. 2022. "Caregivers’ Compliance and Perception of Daycare Centers—A Community-Based Childhood Drowning Prevention Intervention Implemented in Rural Bangladesh" International Journal of Environmental Research and Public Health 19, no. 15: 9537. https://doi.org/10.3390/ijerph19159537
APA StyleAshraf, L., Agrawal, P., Rahman, A., Bhuiyan, M. A. A., Salam, S. S., Li, Q., & Bachani, A. M. (2022). Caregivers’ Compliance and Perception of Daycare Centers—A Community-Based Childhood Drowning Prevention Intervention Implemented in Rural Bangladesh. International Journal of Environmental Research and Public Health, 19(15), 9537. https://doi.org/10.3390/ijerph19159537