
The Impact of Signing Do-Not-Resuscitate Orders on the Use of Non-Beneficial Life-Sustaining Treatments for Intensive Care Unit Patients: A Retrospective Study


Abstract

1. Introduction
Objective
2. Methods
2.1. Design
2.2. Sample and Setting
2.3. Ethical Considerations
2.4. Instruments
2.5. Data Collection and Analysis
3. Results
3.1. Patients’ Characteristics with Regard to Signing or Non-Signing of a DNR
3.2. Influence of DNR Signing and Timing on Predeath Resuscitation Practice
3.3. Signing the DNR for Withdrawing Life-Sustaining Treatments
4. Discussion
4.1. DNR Signing Ratio and Timing as an Ethical Dilemma
4.2. Illness Severity Assessment Had a Positive Effect on DNR Signing
4.3. Signing DNR Orders Effectively Reduces Resuscitation Practices before Death
4.4. DNR Signing Did Not Facilitate the Withdrawal of Life-Sustaining Treatments
4.5. Limitations of the Study
4.6. Suggestions
5. Conclusions
Application in Clinical Practice
6. Implications for Clinical Practice
- (1)
- Learn about the current state of life-sustaining therapies in the ICU under the national health insurance support.
- (2)
- Facilitate the patient’s understanding of the benefits of natural death after signing a DNR order in the ICU.
- (3)
- Facilitate learning with regard to the low withdrawal rate of non-beneficial life-sustaining treatments in the ICU.
- (4)
- Provide a reference for considering the timing of DNR decision-making and the discussion of “time-limited trials” for withdrawal from non-beneficial life-sustaining treatments.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ay, E.; Weigand, M.; Röhrig, R.; Gruss, M. Dying in the Intensive Care Unit (ICU): A retrospective descriptive analysis of deaths in the ICU in a communal tertiary Hospital in Germany. Anesthesiol. Res. Pract. 2020, 2020, 2356019. [Google Scholar] [PubMed]
- Dubois, M. Ethical issues at the end of life. Tech. Reg. Anesth. Pain Manag. 2005, 9, 133–138. [Google Scholar]
- Park, Y.R.; Kim, J.A.; Kim, K. Changes in how ICU nurses perceive the DNR decision and their nursing activity after implementing it. Nurs. Ethics 2011, 18, 802–813. [Google Scholar]
- Manalo, M.F.C. End-of-life decisions about withholding or withdrawing therapy: Medical, ethical, and religio-cultural considerations. Palliat. Care Res. Treat. 2013, 7, 1–5. [Google Scholar]
- Tu, M.-S.; Huang, T.-Y.; Chen, R.-Y.; Tzeng, S.-H.; Chung, J.-M.; Lin, M.-Z. Withdrawal of life-sustaining treatment in terminal ill patients: A 2-year experience in a medical center. Taiwan J. Hosp. Palliat. Care 2016, 21, 289–303. [Google Scholar]
- Tembo, A.C.; Higgins, I.; Parker, V. The experience of communication difficulties in critically ill patients in and beyond intensive care: Findings from a larger phenomenological study. Intens. Crit. Care Nur. 2015, 31, 171–178. [Google Scholar]
- Quenot, J.-P.; Ecarnot, F.; Meunier-Beillard, N.; Dargent, A.; Large, A.; Andreu, P.; Rigaud, J.-P. What are the ethical issues in relation to the role of the family in intensive care? Ann. Transl. Med. 2017, 5, S40. [Google Scholar]
- Annadurai, K.; Danasekaran, R.; Mani, G. Euthanasia: Right to die with dignity. J. Fam. Med. Prim. Care 2014, 3, 477–478. [Google Scholar] [CrossRef]
- Khatony, A.; Fallahi, M.; Rezaei, M.; Mahdavikian, S. Comparison of attitude of nurses and nursing students toward euthanasia. Nurs. Ethics 2022, 29, 208–216. [Google Scholar]
- Ministry of Health and Welfare. Hospice Palliative Care Act. In The R.O.C Laws & Regulations Database; Ministry of Health and Welfare: Taipei, Taiwan, 2021. [Google Scholar]
- Chang, Y.; Huang, C.-F.; Lin, C.-C. Do-not-resuscitate orders for critically ill patients in intensive care. Nurs. Ethics 2010, 17, 445–455. [Google Scholar]
- Mercadante, S.; Gregoretti, C.; Cortegiani, A. Palliative care in intensive care units: Why, where, what, who, when, how. BMC Anesthesiol. 2018, 18, 106. [Google Scholar]
- Juang, I.-F.; Huang, C.-F.; Huang, Y.-T. A Comparison of Differences in Medical Treatments Patients with Do-not-resuscitate Orders Received Before Death in the Intensive Care Units in Northern Taiwan and Eastern Taiwan. JTCCT 2015, 24, 1–18. [Google Scholar]
- Flannery, L.; Ramjan, L.M.; Peters, K. End-of-life decisions in the Intensive Care Unit (ICU)—Exploring the experiences of ICU nurses and doctors–A critical literature review. Aust. Crit. Care 2016, 29, 97–103. [Google Scholar] [PubMed]
- Connolly, C.; Miskolci, O.; Phelan, D.; Buggy, D. End-of-life in the ICU: Moving from ‘withdrawal of care’ to a palliative care, patient-centred approach. Brit. J. Anaesth. 2016, 117, 143–145. [Google Scholar] [PubMed]
- Stokes, H.; Vanderspank-Wright, B.; Bourbonnais, F.F.; Wright, D.K. Meaningful experiences and end-of-life care in the intensive care unit: A qualitative study. Intens. Crit. Care Nur. 2019, 53, 1–7. [Google Scholar]
- Ministry of Health and Welfare. Patient Right to Autonomy Act. In The R.O.C Laws & Regulations Database; Ministry of Health and Welfare: Taipei, Taiwan, 2021. [Google Scholar]
- Donaldson, T.M. Harming patients by provision of intensive care treatment: Is it right to provide time-limited trials of intensive care to patients with a low chance of survival? Med. Health Care Philos. 2021, 24, 227–233. [Google Scholar] [CrossRef]
- Donaldson, T.M. Death during life sustaining treatment must be considered a failure but can be acceptable if the treatment was proportional. Intens. Care Med. 2022, 48, 967–968. [Google Scholar]
- Saha, D.; Moreno, C.; Csete, M.; Perez, E.K.; Cubeddu, L.; Farcy, D.; Henry, S.; Glazer, Z.; Moreno-Walton, L.A.; Goldszer, R.C. Outcomes of patients who have do not resuscitate status prior to being admitted to an intensive care unit. Scientifica 2016, 2016, 1513946. [Google Scholar]
- Ma, J.; Chi, S.; Buettner, B.; Pollard, K.; Muir, M.; Kolekar, C.; Al-Hammadi, N.; Chen, L.; Kollef, M.; Dans, M. Early palliative care consultation in the medical ICU: A cluster randomized crossover trial. Crit. Care Med. 2019, 47, 1707–1715. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Fang, Y.-T.; Chen, H.-C.; Lin, C.-Y.; Chang, Y.-P.; Chen, Y.-M.; Huang, C.-H.; Huang, K.-T.; Chang, H.-C.; Su, M.-C. Effect of do-not-resuscitate orders on patients with sepsis in the medical intensive care unit: A retrospective, observational and propensity score-matched study in a tertiary referral hospital in Taiwan. BMJ Open 2019, 9, e029041. [Google Scholar]
- Ouyang, D.J.; Lief, L.; Russell, D.; Xu, J.; Berlin, D.A.; Gentzler, E.; Su, A.; Cooper, Z.R.; Senglaub, S.S.; Maciejewski, P.K. Timing is everything: Early do-not-resuscitate orders in the intensive care unit and patient outcomes. PLoS ONE 2020, 15, e0227971. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, T.M. When the harms of intensive care treatment outweigh the benefits, the default use of time-limited trials is not ethically justifiable. Intens. Care Med. 2022, 48, 377–378. [Google Scholar] [CrossRef] [PubMed]
- Cheung, E.H.-L.; Cheung, J.C.-H.; Yip, Y.-Y. Time-limited trial of intensive care is more than merely life sustaining. Intens. Care Med. 2022, 48, 507–508. [Google Scholar] [CrossRef]
- Lin, H.-M.; Liu, C.-K.; Huang, Y.-C.; Ho, C.-W.; Chen, M. Investigating Key Factors Related to the Decision of a Do-Not-Resuscitate Consent. Int. J. Environ. Res. Public Health 2021, 19, 428. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.J.; Desai, N.; Pattison, N.; Droney, J.M.; King, A.; Farquhar-Smith, P.; Gruber, P.C. Quality of transition to end-of-life care for cancer patients in the intensive care unit. Ann. Intens. Care 2015, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Godinjak, A.; Iglica, A.; Rama, A.; Tančica, I.; Jusufović, S.; Ajanović, A.; Kukuljac, A. Predictive value of SAPS II and APACHE II scoring systems for patient outcome in a medical intensive care unit. Acta Med. Acad. 2016, 45, 97–103. [Google Scholar] [CrossRef]
- Kostoglou, A.; Kotanidou, A.; Marvaki, C.; Orfanos, S. Mortality rate of ICU patients according to APACHE II and SAPS II score. Health Res. J. 2018, 4, 219–233. [Google Scholar] [CrossRef]
- Ma, J.-C.; Li, C.-H.; Lin, P.-X.; Hsiao, C.-Y.; Su, M.-I. Early Mortality Rate Prediction Recognition of End-stage Non-cancer Patients in the Emergency Room. J. Intern. Med. Taiwan 2020, 31, 417–424. [Google Scholar]
- Brennan, P.M.; Murray, G.D.; Teasdale, G.M. A practical method for dealing with missing Glasgow Coma Scale verbal component scores. J. Neurosurg. 2020, 1, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Baek, M.S.; Koh, Y.; Hong, S.-B.; Lim, C.-M.; Huh, J.W. Effect of timing of do-not-resuscitate orders on the clinical outcome of critically ill patients. Korean J. Crit. Care Med. 2016, 31, 229–235. [Google Scholar] [CrossRef]
- Dignam, C.; Brown, M.; Thompson, C.H. Moving from “Do Not Resuscitate” Orders to Standardized Resuscitation Plans and Shared-Decision Making in Hospital Inpatients. Gerontol. Geriatr. Med. 2021, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.-C.; Lin, P.-X.; Yeh, S.-S.; Cheng, W.-J.; Chen, Y.-Z.; Li, C.-H.; Su, M.-I.; Hsiao, C.-Y. A Retrospective Study on Life Sustaining Treatment After the Withdrawal of Endotracheal Tube from ICU Patients with Terminal Illness. J. Intern. Med. Taiwan 2019, 30, 388–395. [Google Scholar]
- Mehta, S.; Spies, C.; Shehabi, Y. Ten tips for ICU sedation. Intens. Care Med. 2018, 44, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Riker, R.R.; Fraser, G.L.; Therapy, D. Adverse events associated with sedatives, analgesics, and other drugs that provide patient comfort in the intensive care unit. Pharmacotherapy 2005, 25, 8S–18S. [Google Scholar] [CrossRef]
- Shepherd, S.J. Criteria for intensive care unit admission and the assessment of illness severity. Surgery 2018, 36, 171–179. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Total n = 386 | Non-DNR n = 67 | DNR n = 319 | p |
|---|---|---|---|---|
| Age | 65.6 ± 17.8 | 63.1 ± 18.8 | 66.2 ± 17.5 | 0.418 |
| Number of ICU admissions in one year | 1.13 ± 0.49 | 1.15 ± 0.66 | 1.13 ± 0.44 | 0.788 |
| Number of hospitalisations in one year | 3.02 ± 3.32 | 3.34 ± 3.63 | 2.95 ± 3.25 | 0.41 |
| Number of emergency room visits in one year | 2.01 ± 2.39 | 1.76 ± 1.84 | 2.07 ± 2.49 | 0.344 |
| Length of the last stay in ICU (days) | 7.2 ± 9.16 | 4.79 ± 7.85 | 7.7 ± 9.34 | 0.018 * |
| Sex | 0.266 | |||
| Female | 144 (37.3%) | 29 (20.1%) | 115 (79.9%) | |
| Male | 242 (62.7%) | 38 (15.7%) | 204 (84.3%) | |
| Marital status | 0.016 * | |||
| Married | 249 (64.5%) | 47 (70.1%) | 202 (63.3%) | |
| Unmarried | 56 (14.5%) | 14 (20.9%) | 42 (13.2%) | |
| Widowed/Divorced | 81 (21%) | 6 (9%) | 75 (23.5%) | |
| Employed | 0.315 | |||
| Yes | 135 (34.9%) | 27 (40.3%) | 108 (33.9%) | |
| No | 251 (65%) | 40 (59.7%) | 211 (66.1%) | |
| Religion | 0.781 | |||
| None | 151 (39.1%) | 23 (33.4%) | 128 (40.1%) | |
| Buddhism | 139 (36%) | 26 (39.4%) | 113 (35.4%) | |
| Taoism | 74 (19.2%) | 16 (24.2%) | 58 (18.2%) | |
| Others | 22 (5.7%) | 2 (3%) | 20 (6.3%) | |
| Living style | 0.251 | |||
| Living with family | 343 (88.9%) | 60 (89.6%) | 283 (88.7%) | |
| Living alone | 23 (6%) | 2 (3%) | 21 (6.6%) | |
| Living in a nursing home | 20 (5.2%) | 5 (7.4%) | 15 (4.7%) | |
| Specialty | 0.231 | |||
| Haematology and Oncology | 109 (28.2%) | 21 (31.3%) | 88 (27.6%) | |
| Gastroenterology | 79 (20.5%) | 10 (14.9%) | 69 (21.6%) | |
| Infectious diseases | 63 (16.3%) | 15 (22.4%) | 48 (15%) | |
| Nephrology | 37 (9.6%) | 3 (4.5%) | 34 (10.6%) | |
| Others | 98 (25.4%) | 18 (26.9%) | 80 (25.1%) | |
| Palliative care consultation | 101 (26.2%) | 3 (4.5%) | 98 (30.7%) | <0.001 *** |
| Death place | 0.057 | |||
| Died in ICU | 294 (76.2%) | 45 (67.2%) | 249 (78.1%) | |
| Predeath discharged | 92 (23.8%) | 22 (32.8%) | 70 (21.9%) |
| Items | Total n = 386 | Non-DNR n = 67 | DNR n = 319 | p |
|---|---|---|---|---|
| Worst physical conditions within 24 h of ICU admission | ||||
| GCS score | 7.8 ± 3.9 | 7.5 ± 4.1 | 7.9 ± 3.9 | 0.425 |
| SAPS II score | 73 ± 26 | 66.6 ± 28.2 | 74.4 ± 25.4 | 0.028 * |
| APACHE II score | 29.9 ± 9.2 | 27.5 ± 10.6 | 30.4 ± 8.8 | 0.037 * |
| Care needs for ICU admission | 0.996 | |||
| Respiratory failure | 266 (68.9%) | 47 (70.1%) | 219 (68.7%) | |
| Severe septic shock | 49 (12.7%) | 9 (13.4%) | 40 (12.5%) | |
| Massive haemorrhage | 14 (3.6%) | 2 (3%) | 12 (3.8%) | |
| Post-resuscitation | 30 (7.8%) | 5 (7.5%) | 25 (7.8%) | |
| Diabetic ketoacidosis | 1 (0.3%) | 0 (0%) | 1 (0.3%) | |
| Severe heart failure and acute pulmonary oedema | 8 (2.1%) | 1 (1.5%) | 7 (2.2%) | |
| Drug toxicity with organ failure | 3 (0.8%) | 0 | 3 (0.9%) | |
| Electrolyte imbalance of body fluids associated with renal failure | 4 (1%) | 1 (1.5%) | 3 (0.9%) | |
| Others | 11 (2.8%) | 2 (3%) | 9 (2.8%) | |
| Comfort care | ||||
| Sedatives | 166 (43%) | 25 (37.3%) | 141 (44.2%) | 0.301 |
| Muscle relaxants | 68 (17.6%) | 9 (13.4%) | 59 (18.5%) | 0.323 |
| Analgesics | 173 (44.8%) | 20 (29.9%) | 153 (48%) | 0.007 ** |
| Vascular line | ||||
| An intra-arterial catheter (A-line) | 367 (95.1%) | 63 (94%) | 304 (95.3%) | 0.663 |
| Central venous catheter (CVC) | 277 (71.7%) | 43 (64.2%) | 234 (73.4%) | 0.129 |
| Item | Non-DNR n = 67 | DNR n = 319 | p | Time of DNR Signed | Resuscitations after DNR n = 75 | ||
|---|---|---|---|---|---|---|---|
| Before ICU Admission n = 26 | Within 24 h of ICU Admission n = 105 | 48 h after ICU Admission n = 188 | |||||
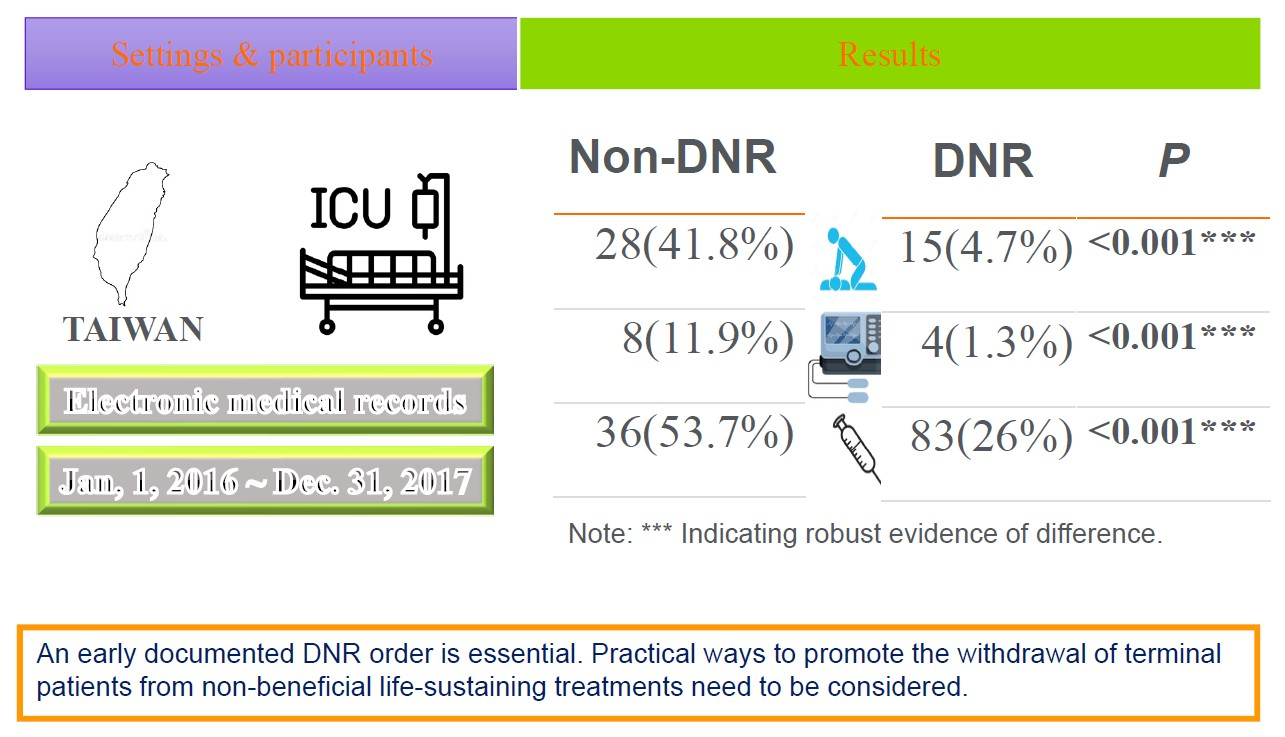
| Chest compressions | 28 (41.8%) | 15 (4.7%) | <0.001 *** | 1 (3.8%) | 6 (5.7%) | 8 (4.3%) | 4 (5.3%) |
| Electric shock | 8 (11.9%) | 4 (1.3%) | <0.001 *** | 1 (3.8%) | 2 (1.9%) | 1 (0.5%) | 1 (1.3%) |
| Cardiotonic drugs injection | 36 (53.7%) | 83 (26%) | <0.001 *** | 9 (34.6%) | 37 (35.2%) | 37 (19.7%) | 73 (97.3%) |
| Total n = 386 | Non-DNR n = 67 | DNR n = 319 | p | Withdrawal after DNR n = 319 | |
|---|---|---|---|---|---|
| Endotracheal tube & ventilator (ET) | 363 (94%) | 64 (95.5%) | 299 (93.7%) | 0.355 | 20 (6.27%) |
| Vasopressors | 344 (89.1%) | 64 (95.5%) | 280 (87.8%) | 0.064 | 4 (1.25%) |
| ECMO | 18 (4.7%) | 4 (6%) | 14 (4.4%) | 0.577 | 2 (0.63%) |
| Continuous venovenous haemofiltration (CVVH) | 126 (32.6%) | 15 (22.4%) | 111 (34.8%) | 0.049 * | 2 (0.63%) |
| Haemodialysis | 37 (9.6%) | 5 (7.5%) | 32 (10%) | 0.516 | 0 |
| Antibiotics | 372 (96.4%) | 61 (91%) | 311 (97.5%) | 0.01 * | 0 |
| Blood transfusion | 281 (72.8%) | 44 (65.7%) | 237 (74.3%) | 0.149 | 0 |
| Intra-aortic balloon pump (IABP) | 4 (1%) | 2 (3%) | 2 (0.6%) | 0.083 | 1 (0.31%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiu, S.-S.; Lee, T.-T.; Yeh, M.-C.; Chen, Y.-C.; Huang, S.-H. The Impact of Signing Do-Not-Resuscitate Orders on the Use of Non-Beneficial Life-Sustaining Treatments for Intensive Care Unit Patients: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 9521. https://doi.org/10.3390/ijerph19159521
Shiu S-S, Lee T-T, Yeh M-C, Chen Y-C, Huang S-H. The Impact of Signing Do-Not-Resuscitate Orders on the Use of Non-Beneficial Life-Sustaining Treatments for Intensive Care Unit Patients: A Retrospective Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9521. https://doi.org/10.3390/ijerph19159521
Chicago/Turabian StyleShiu, Shang-Sin, Ting-Ting Lee, Ming-Chen Yeh, Yu-Chi Chen, and Shu-He Huang. 2022. "The Impact of Signing Do-Not-Resuscitate Orders on the Use of Non-Beneficial Life-Sustaining Treatments for Intensive Care Unit Patients: A Retrospective Study" International Journal of Environmental Research and Public Health 19, no. 15: 9521. https://doi.org/10.3390/ijerph19159521
APA StyleShiu, S.-S., Lee, T.-T., Yeh, M.-C., Chen, Y.-C., & Huang, S.-H. (2022). The Impact of Signing Do-Not-Resuscitate Orders on the Use of Non-Beneficial Life-Sustaining Treatments for Intensive Care Unit Patients: A Retrospective Study. International Journal of Environmental Research and Public Health, 19(15), 9521. https://doi.org/10.3390/ijerph19159521