
Feasibility of a Social Network-Based Physical Activity Intervention Targeting Vocational School Students: A Pilot Study


Abstract
:1. Introduction
1.1. Background
- Processes for successful implementation of the intervention, which are documented and rated,
- Resources necessary for the implementation of the intervention, which are tracked and quantified,
- Challenges during the development and implementation of the intervention, which are noted,
- Resources and challenges faced during data processing, which are recorded,
- Use and acceptability of the employed intervention (in our case the Web 2.0 platforms), as well as reasons for non-use, which are assessed.
1.2. Objectives
2. Materials and Methods
2.1. Participants and Setting
2.2. Intervention
2.3. Outcomes
2.4. Statistical Methods
2.5. Feasibility Criteria
2.6. Ethical Aspects
3. Results
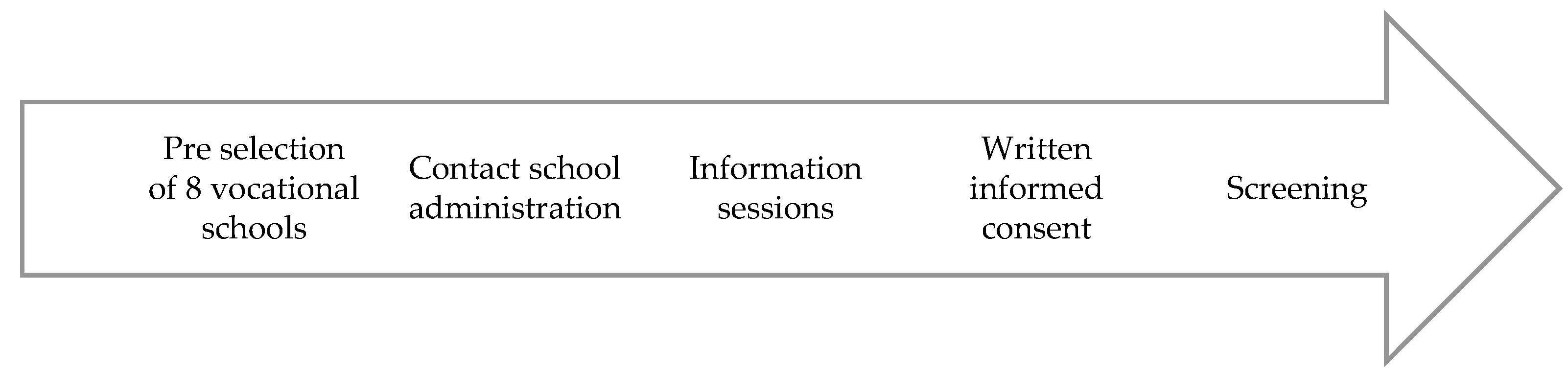
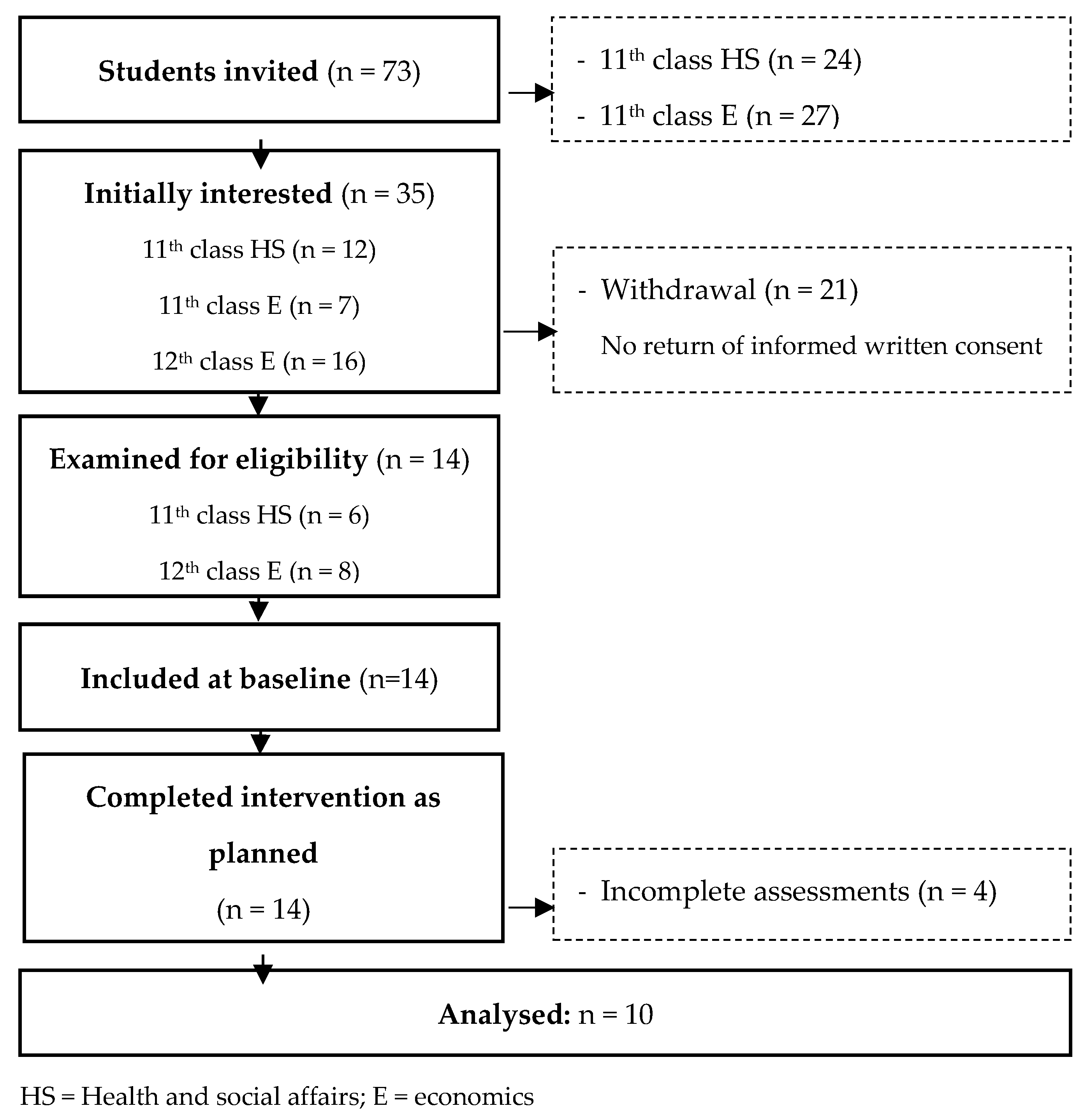
3.1. Recruitment
3.2. Participants
3.3. Feasibility
3.4. Estimation of Potential Effects
3.5. Participants’ Feedback
4. Discussion
5. Conclusions
- Creating a supportive environment, including integration of the program in the daily setting of the target group, e.g., school increasing autonomous motivation via peer relations and social support.
- Providing a social media add-on, including incorporation of an existing social media platform that is frequently and easily used by the target population during their leisure time.
- Addition of BCTs, including complementing the intervention with other effective BCTs, such as feedback and goal setting.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCT | behaviour change technique |
| BMI | body mass index |
| MVPA | moderate to vigorous physical activity |
| PA | physical activity |
| QOL | quality of life |
| SSS | subjective social status |
| WHO | World Health Organization |
References
- 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 7 April 2022).
- World Health Organization. World Health Statistics 2020: Monitoring Health for the Sdgs, Sustainable Development Goals. Available online: https://apps.who.int/iris/bitstream/handle/10665/332070/9789240005105-eng.pdf?sequence=1&isAllowed=y (accessed on 28 May 2022).
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1.6 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- World Health Organization. Germany Physical Activity Factsheet. 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0020/382511/germany-eng.pdf (accessed on 31 May 2022).
- Adimon-Themenblatt: Sportliche Aktivität in der Schule. Available online: https://www.rki.de/adimon (accessed on 31 May 2022).
- Mróz-Gorgoń, B.; Peszko, K. Marketing Analysis of Social Media—Definition Considerations. Eur. J. Serv. Manag. 2016, 20, 33–40. [Google Scholar] [CrossRef]
- Günther, L.; Schleberger, S.; Pischke, C.R. Effectiveness of Social Media-Based Interventions for the Promotion of Physical Activity: Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 13018. [Google Scholar] [CrossRef] [PubMed]
- Teens’ Social Media Usage Is Drastically Increasing. Available online: https://www.statista.com/chart/15720/frequency-of-teenagers-social-media-use/ (accessed on 31 May 2022).
- Hosseinpour, M.; Terlutter, R. Your Personal Motivator Is with You: A Systematic Review of Mobile Phone Applications Aiming at Increasing Physical Activity. Sports Med. 2019, 49, 1425–1447. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Brackbill, D.; Yang, S.; Becker, J.; Herbert, N.; Centola, D. Support or Competition? How Online Social Networks Increase Physical Activity: A Randomized Controlled Trial. Prev. Med. Rep. 2016, 4, 453–458. [Google Scholar] [CrossRef] [Green Version]
- Reik, R.; Woll, A.; Gröben, F.; Berndt, E.D. Betriebliche Gesundheitsförderung in der Ausbildung. Wie verändert Sich der Lebensstil der Jugendlichen über einen zweijährigen Ausbildungszeitraum und welchen Beitrag kann ein Azubi-Fit Programm leisten? Arbeitsmed. Sozialmed. Umweltmed. 2010, 45, 640–646. [Google Scholar]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A Tutorial on Pilot Studies: The What, Why and How. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.; Ferguson, M.; Vandelanotte, C.; Plotnikoff, R.; De Bourdeaudhuij, I.; Thomas, S.; Nelson-Field, K.; Olds, T. A Web-Based, Social Networking Physical Activity Intervention for Insufficiently Active Adults Delivered Via Facebook App: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e174. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (V1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of Accelerometer Wear and Nonwear Time Classification Algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. Accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- International Physical Activity Questionnaire. Downloadable Questionnaires. Available online: https://sites.google.com/site/theipaq/questionnaire_links (accessed on 7 May 2022).
- International Physical Activity Questionnaire. Ipaq Scoring Protocol. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 7 May 2022).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Health Interview Surveys: Towards International Harmonization of Methods and Instruments. Available online: https://apps.who.int/iris/bitstream/handle/10665/107328/E72841.pdf?sequence=1&isAllowed=y (accessed on 7 May 2022).
- WHOQOL Group. Development of the World Health Organization Whoqol-Bref Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Whoqol: Measuring Quality of Life. Available online: https://www.who.int/tools/whoqol/whoqol-bref/docs/default-source/publishing-policies/whoqol-bref/german-whoqol-bref (accessed on 7 May 2022).
- Angermeyer, M.C.; Kilian, R.; Matschinger, H. Handbuch für die deutschsprachigen Versionen der WHO Instrumente zur Erfassung von Lebensqualität, 1st ed.; Hogrefe: Göttingen, Germany, 2000. [Google Scholar]
- Emi-2 in German. Available online: http://exercise-motivation.bangor.ac.uk/emi/german.php (accessed on 7 May 2022).
- Messner, E.M.; Terhorst, Y.; Barke, A.; Baumeister, H.; Stoyanov, S.; Hides, L.; Kavanagh, D.; Pryss, R.; Sander, L.; Probst, T. The German Version of the Mobile App Rating Scale (Mars-G): Development and Validation Study. JMIR Mhealth Uhealth 2020, 8, e14479. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 31 May 2022).
- Lampert, T.; Hoebel, J.; Kuntz, B.; Müters, S.; Kroll, L.E. Messung Des sozioökonomischen Status und des subjektiven sozialen Status in KIGGS Welle. J. Health Monit. 2018, 3, 114–133. [Google Scholar] [CrossRef]
- Hankonen, N.; Heino, M.T.; Hynynen, S.T.; Laine, H.; Araújo-Soares, V.; Sniehotta, F.F.; Vasankari, T.; Sund, R.; Haukkala, A. Randomised Controlled Feasibility Study of a School-Based Multi-Level Intervention to Increase Physical Activity and Decrease Sedentary Behaviour among Vocational School Students. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuipers, A.; Kloek, G.C.; de Vries, S.I. Understanding Vocational Students’ Motivation for Dietary and Physical Activity Behaviors. Int. J. Environ. Res. Public Health 2021, 18, 1381. [Google Scholar] [CrossRef]
- Van Dyck, D.; D’Haese, S.; Plaete, J.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. Opinions Towards Physical Activity Interventions Using Facebook or Text Messaging: Focus Group Interviews with Vocational School-Aged Adolescents. Health Soc. Care Communit. 2019, 27, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Saez, L.; Langlois, J.; Legrand, K.; Quinet, M.; Lecomte, E.; Omorou, A.; Briançon, S. PRALIMAP-INÈS Trial Group Reach and Acceptability of a Mobile Reminder Strategy and Facebook Group Intervention for Weight Management in Less Advantaged Adolescents: Insights From the PRALIMAP-INÈS Trial. JMIR Mhealth Uhealth 2018, 6, e110. [Google Scholar] [CrossRef] [PubMed]
- Ellis, W.E.; Dumas, T.M.; Forbes, L.M. Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can. J. Behav. Sci. /Rev. Can. Des Sci. Du Comport. 2020, 52, 177–187. [Google Scholar] [CrossRef]
- Fernandes, S.; Caperchione, C.M.; Thornton, L.E.; Timperio, A. A qualitative exploration of perspectives of physical activity and sedentary behaviour among Indian migrants in Melbourne, Australia: How are they defined and what can we learn? BMC Public Health 2021, 21, 2085. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| What | Content | Intervention Week |
|---|---|---|
| Tutorials app usage | Screen recording on how to use Facebook and Pacer | 1 |
| Post team ranking | Screenshot of team leader board of each group | 2 |
| Spotify podcast | “Quarks Daily” episode with scientific background information about the PA recommendation of 10,000 steps | 3 |
| YouTube clip | Video with tips on how to implement steady walking routines in everyday life | 5 |
| Parameter | Measurement Tool | Measurement Time | |
|---|---|---|---|
| Process | Recruitment rate | Documentation | Implementation |
| Withdrawal | Implementation | ||
| Drop outs/completion rate | Implementation | ||
| Attendance on Facebook | Implementation | ||
| Adequacy eligibility criteria | Implementation | ||
| Adequacy assessments | Implementation | ||
| Ressources | Study staff | Documentation | Entire study |
| Time expenditure | Entire study | ||
| Material | Entire study | ||
| Costs | Entire study | ||
| Management | Challenges | Documentation | Entire study |
| Solution strategies | Entire study | ||
| Preliminary effects | Objective PA | Accelerometer, activity diary | T0, T1 |
| Subjective PA | IPAQ-SF | T0, T1 | |
| BMI | Stadiometer + Scale | T0, T1 | |
| Subjective health | Questionnaire | T0, T1 | |
| Quality of Life | WHOQOL-BREF | T0, T1 | |
| Exercise motives | EMI-2 | T0, T1 | |
| Feedback | Usage and acceptability | Questionnaire | T1 |
| Facebook and Pacer | |||
| Quality Pacer | MARS-G | T1 |
| Total (n = 14) | Male (n = 7) | Female (n = 7) | |
|---|---|---|---|
| Age, years | 17.4 ± 1.2 | 18 ± 1.5 | 17.1 ± 0.7 |
| Body mass index, kg/m2 | 23.5 ± 4.8 | 21.3 ± 5.4 | 25.4 ± 2.3 |
| Subjective social status | 5.7 ± 1.7 | 5.3 ± 2.4 | 6 ± 0.8 |
| Migration background | 78.6 | 28.6 | 50 |
| Graduation (O-levels) | 100 | 50 | 50 |
| MVPA/day < 60 min | 71.4 | 21.4 | 50 |
| What | Time (h) | Study Staff (n) | |
|---|---|---|---|
| Recruitment | 14.5 | 1–2 | |
| Assessments | Organization | 33 | 3 |
| Implementation | 15 | 2–3 | |
| Intervention | Design | 14 | 1–2 |
| Implementation | 1 | 1 | |
| Data management | 15 | 1 | |
| T0 | T1 | SMD (95%CI) | p | |
|---|---|---|---|---|
| Subjective PA | ||||
| MVPA (min/day) | 42.1 ± 55.6 | 59.7 ± 52.9 | −17.6 (−67.1, 31.8) | 0.440 |
| MVPA walking (min/day) | 112.6 ± 113.4 | 125.1 ± 92.6 | −12.5 (−122.4, 97.4) | 0.803 |
| Sedentary time (min/day) * | 360 ± 49 | 381.4 ± 94.4 | −21.4 (−117.2, 74.3) | 0.604 |
| Subjective health | 2.1 ± 0.9 | 2.2 ± 1.1 | 0.1 (−0.5, 0.7) | 0.726 |
| BMI | 23.5 ± 4.8 | 23.5 ± 4.5 | 0 (−0.4, 0.5) | 0.887 |
| QOL (4–20) | ||||
| General | 14.4 ± 3.1 | 14.4 ± 3 | 0 (−1.8, 1.8) | 1.0 |
| Physical health | 15.7 ± 2.8 | 15.3 ± 2.2 | 0.4 (−1.5, 2.2) | 0.663 |
| Psychological health | 13.7 ± 3.7 | 14 ± 3.5 | −0.2 (−3, 2.5) | 0.846 |
| Social relations | 14.7 ± 2.2 | 14.9 ± 2.9 | −0.3 (−2.8, 2.2) | 0.814 |
| Environment | 14.7 ± 3.5 | 15.9 ± 2.8 | −1.2 (−4.5, 2.1) | 0.427 |
| Exercise motives (0–5) | ||||
| Affiliation | 2.2 ± 0.9 | 1.9 ± 1.5 | 0.3 (−1, 1.6) | 0.582 |
| Appearance | 3.6 ± 1 | 3.3 ± 1 | 0.3 (−0.4, 0.9) | 0.401 |
| Challenge | 3.3 ± 1.1 | 3.7 ± 1.1 | −0.4 (−1.4, 0.6) | 0.395 |
| Competition | 2.2 ± 1.5 | 2.2 ± 1.5 | −0.1 (−1.5, 1.4) | 0.940 |
| Enjoyment | 3 ± 1.3 | 3.4 ± 0.8 | −0.4 (−1.4, 0.6) | 0.404 |
| Ill-health-avoidance | 3.5 ± 1.2 | 4.2 ± 0.5 | −0.7 (−1.7, 0.2) | 0.109 |
| Nimbleness | 3.3 ± 1.1 | 3.4 ± 0.8 | −0.1 (−0.9, 0.7) | 0.787 |
| Positive health | 4.3 ± 0.8 | 4.2 ± 0.5 | 0.1 (−0.6, 0.8) | 0.714 |
| Revitalization | 3.6 ± 1.1 | 3.8 ± 0.8 | −0.2 (−1, 0.6) | 0.604 |
| Social pressure | 0.7 ± 1.0 | 0.5 ± 0.8 | 0.1 (−0.6, 0.9) | 0.701 |
| Social recognition | 1.4 ± 1.2 | 1.4 ± 1.0 | −0.1 (−1, 0.8) | 0.856 |
| Strength and endurance | 3.9 ± 1.5 | 3.6 ± 1 | 0.3 (−1, 1.6) | 0.608 |
| Stress nanagement | 2.7 ± 1.2 | 2.8 ± 1.3 | −0.1 (−0.7, 0.6) | 0.806 |
| Weight nanagement | 2.2 ± 1.7 | 2.4 ± 1.7 | −0.2 (−1.3, 1) | 0.727 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Günther, L.; Schleberger, S.; Pischke, C.R. Feasibility of a Social Network-Based Physical Activity Intervention Targeting Vocational School Students: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 9474. https://doi.org/10.3390/ijerph19159474
Günther L, Schleberger S, Pischke CR. Feasibility of a Social Network-Based Physical Activity Intervention Targeting Vocational School Students: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9474. https://doi.org/10.3390/ijerph19159474
Chicago/Turabian StyleGünther, Liane, Sarah Schleberger, and Claudia R. Pischke. 2022. "Feasibility of a Social Network-Based Physical Activity Intervention Targeting Vocational School Students: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 15: 9474. https://doi.org/10.3390/ijerph19159474
APA StyleGünther, L., Schleberger, S., & Pischke, C. R. (2022). Feasibility of a Social Network-Based Physical Activity Intervention Targeting Vocational School Students: A Pilot Study. International Journal of Environmental Research and Public Health, 19(15), 9474. https://doi.org/10.3390/ijerph19159474