
Integrating Cognitive Dysfunction Accommodation Strategies into an HIV Prevention Session: A 2-Arm Pilot Feasibility Study


Abstract
:1. Introduction
2. Materials and Methods
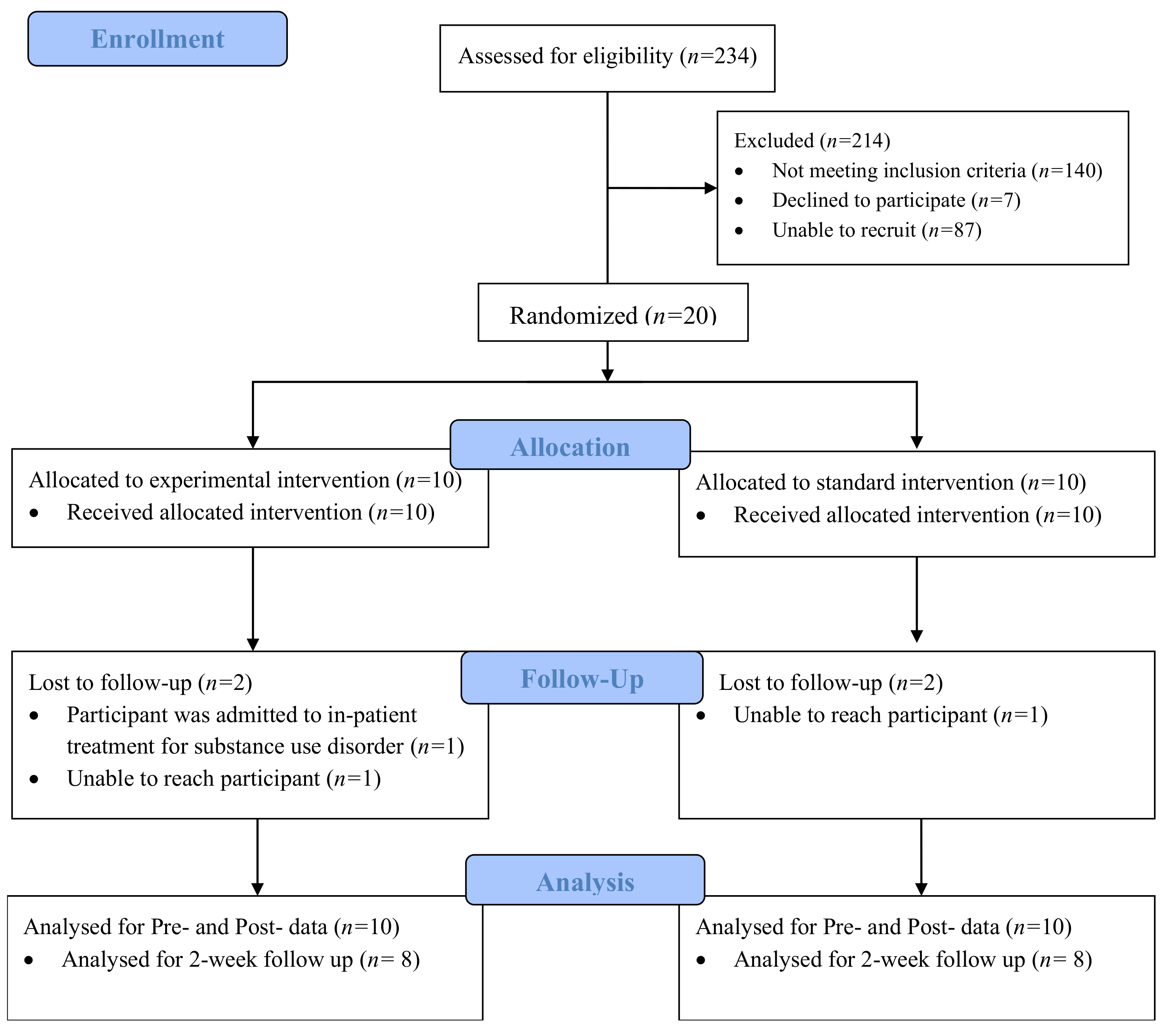
2.1. Study Design and Sample
2.2. Assessment Tools
2.2.1. Demographics
2.2.2. Brief Inventory of Neurocognitive Impairment (BINI)
2.2.3. Accommodation Strategy Acceptability Survey
2.2.4. Skills Assessment
2.3. Data Analysis
3. Results
3.1. Demographics
3.2. Acceptability of Accommodation Strategies
3.3. Impact of Accommodation Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murphy, A.; Barbaro, J.; Martinez-Aguado, P.; Chilunda, V.; Jaureguiberry-Bravo, M.; Berman, J.W. The Effects of Opioids on HIV Neuropathogenesis. Front. Immunol. 2019, 10, 2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanborn, V.; Gunstad, J.; Shrestha, R.; Mistler, C.B.; Copenhaver, M.M. Cognitive profiles in persons with opioid use disorder enrolled in methadone treatment. Appl. Neuropsychol. Adult 2020, 29, 1–7. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Drug Abuse. Drugs, Brains, and Behavior: The Science of Addiction. 2020. Available online: https://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction/drugs-brain (accessed on 13 September 2020).
- Huedo-Medina, T.B.; Shrestha, R.; Copenhaver, M. Modeling a Theory-Based Approach to Examine the Influence of Neurocognitive Impairment on HIV Risk Reduction Behaviors Among Drug Users in Treatment. AIDS Behav. 2016, 20, 1646–1657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winstanley, E.L.; Mahoney, J.J.; Castillo, F.; Comer, S.D. Neurocognitive impairments and brain abnormalities resulting from opioid-related overdoses: A systematic review. Drug Alcohol Depend. 2021, 226, 108838. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Nonfatal Drug Overdoses. 2020. Available online: https://www.cdc.gov/drugoverdose/data/nonfatal.html (accessed on 1 July 2020).
- Copenhaver, M.M.; Sanborn, V.; Shrestha, R.; Mistler, C.; Gunstad, J. Association between the brief inventory of neurocognitive impairment (BINI) and objective cognitive testing among persons with opioid use disorders in drug treatment. J. Addict. Dis. 2021, 32, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Altice, F.L.; Kamarulzaman, A.; Soriano, V.; Schechter, M.; Friedland, G.H. Treatment of medical, psychiatric, and substance-use comorbidities in people infected with HIV who use drugs. Lancet 2010, 376, 367–387. [Google Scholar] [CrossRef] [Green Version]
- Kamarulzaman, A.; Altice, F.L. Challenges in managing HIV in people who use drugs. Curr. Opin. Infect. Dis. 2015, 28, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Rezapour, T.; Hatami, J.; Farhoudian, A.; Sofuoglu, M.; Noroozi, A.; Daneshmand, R.; Samiei, A.; Ekhtiari, H. Cognitive rehabilitation for individuals with opioid use disorder: A randomized controlled trial. Neuropsychol. Rehabilit. 2017, 29, 1273–1289. [Google Scholar] [CrossRef]
- Anand, P.; Springer, S.A.; Copenhaver, M.M.; Altice, F.L. Neurocognitive Impairment and HIV Risk Factors: A Reciprocal Relationship. AIDS Behav. 2010, 14, 1213–1226. [Google Scholar] [CrossRef] [Green Version]
- Maglione, M.A.; Raaen, L.; Chen, C.; Azhar, G.; Shahidinia, N.; Shen, M.; Maksabedian, E.; Shanman, R.M.; Newberry, S.; Hempel, S. Effects of medication assisted treatment (MAT) for opioid use disorder on functional outcomes: A systematic review. J. Subst. Abus. Treat. 2018, 89, 28–51. [Google Scholar] [CrossRef] [Green Version]
- Jhanjee, S. Evidence Based Psychosocial Interventions in Substance Use. Indian J. Psychol. Med. 2014, 36, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Mistler, C.B.; Shrestha, R.; Gunstad, J.; Sanborn, V.; Copenhaver, M.M. Adapting behavioural interventions to compensate for cognitive dysfunction in persons with opioid use disorder. Gen. Psychiatry 2021, 34, e100412. [Google Scholar] [CrossRef]
- Copenhaver, M.; Avants, S.K.; Warburton, L.A.; Margolin, A. Intervening Effectively with Drug Abusers Infected with HIV: Taking into Account the Potential for Cognitive Impairment. J. Psychoact. Drugs 2003, 35, 209–218. [Google Scholar] [CrossRef]
- Gallagher, M.; McLeod, H.J.; McMillan, T.M. A systematic review of recommended modifications of CBT for people with cognitive impairments following brain injury. Neuropsychol. Rehabil. 2016, 29, 1–21. [Google Scholar] [CrossRef]
- Ramsay, J.R. CBT for Adult ADHD: Adaptations and Hypothesized Mechanisms of Change. J. Cogn. Psychother. 2010, 24, 37–45. [Google Scholar] [CrossRef]
- Shrestha, R.; Didomizio, E.; Kim, R.; Altice, F.L.; Wickersham, J.A.; Copenhaver, M.M. Awareness about and willingness to use long-acting injectable pre-exposure prophylaxis (LAI-PrEP) among people who use drugs. J. Subst. Abus. Treat. 2020, 117, 108058. [Google Scholar] [CrossRef]
- Mistler, C.B.; Idiong, C.I.; Copenhaver, M.M. Integrating Cognitive Dysfunction Accommodation Strategies into Behavioral Interventions for Persons on Medication for Opioid Use Disorder. Front. Public Health 2022, 10, 2296–2565. [Google Scholar] [CrossRef]
- Copenhaver, M.; Shrestha, R.; Wickersham, J.A.; Weikum, D.; Altice, F. An Exploratory Factor Analysis of a Brief Self-Report Scale to Detect Neurocognitive Impairment Among Participants Enrolled in Methadone Maintenance Therapy. J. Subst. Abus. Treat. 2016, 63, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Qualtrics. 2021. Available online: https://qualtrics.com (accessed on 22 June 2021).
- Avants, S.; Margolin, A.; Usubiaga, M.H.; Doebrick, C. Targeting HIV-related outcomes with intravenous drug users maintained on methadone: A randomized clinical trial of a harm reduction group therapy. J. Subst. Abus. Treat. 2004, 26, 67–78. [Google Scholar] [CrossRef]
- Margolin, A.; Avants, S.K.; Warburton, L.A.; Hawkins, K.A.; Shi, J. A randomized clinical trial of a manual-guided risk reduction intervention for HIV-positive injection drug users. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2003, 22, 223–228. [Google Scholar] [CrossRef]
- Copenhaver, M.M.; Lee, I.-C.; Baldwin, P. A randomized controlled trial of the community-friendly health recovery program (CHRP) among high-risk drug users in treatment. AIDS Behav. 2013, 17, 2902–2913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM Corporation, IBM SPSS Statistics for Windows; IBM Corp: Armonk, NY, USA, 2017.
- Wilde, E.A.; Whiteneck, G.G.; Bogner, J.; Bushnik, T.; Cifu, D.X.; Dikmen, S.; French, L.; Giacino, J.T.; Hart, T.; Malec, J.F.; et al. Recommendations for the Use of Common Outcome Measures in Traumatic Brain Injury Research. Arch. Phys. Med. Rehabil. 2010, 91, 1650–1660.e17. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health. Cognition Measures. 2020. Available online: https://www.healthmeasures.net/explore-measurement-systems/nih-toolbox/intro-to-nih-toolbox/cognition (accessed on 9 December 2020).
- Substance Abuse and Mental Health Services Administration. TIP 29: Substance Use Disorder Treatment for People with Physical and Cognitive Disabilities. 2012. Available online: https://store.samhsa.gov/product/TIP-29-Substance-Use-Disorder-Treatment-for-People-With-Physical-and-Cognitive-Disabilities/SMA12-4078 (accessed on 13 September 2020).
- Mayer, K.H.; Safren, S.A.; Elsesser, S.; Psaros, C.; Tinsley, J.P.; Marzinke, M.; Clarke, W.; Hendrix, C.; Taylor, S.W.; Haberer, J.; et al. Optimizing Pre-Exposure Antiretroviral Prophylaxis Adherence in Men Who Have Sex with Men: Results of a Pilot Randomized Controlled Trial of “Life-Steps for PrEP”. AIDS Behav. 2016, 21, 1350–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biello, K.B.; Psaros, C.; Krakower, D.S.; Marrow, E.; Safren, S.A.; Mimiaga, M.J.; Hightow-Weidman, L.; Sullivan, P.; Mayer, K.H. A Pre-Exposure Prophylaxis Adherence Intervention (LifeSteps) for Young Men Who Have Sex with Men: Protocol for a Pilot Randomized Controlled Trial. JMIR Res. Protoc. 2019, 8, e10661. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, R.; Altice, F.L.; Karki, P.; Copenhaver, M.M. Integrated Bio-behavioral Approach to Improve Adherence to Pre-exposure Prophylaxis and Reduce HIV Risk in People Who Use Drugs: A Pilot Feasibility Study. AIDS Behav. 2018, 22, 2640–2649. [Google Scholar] [CrossRef]
- Rass, O.; Kleykamp, B.A.; Vandrey, R.G.; Bigelow, G.E.; Leoutsakos, J.M.; Stitzer, M.L.; Strain, E.C.; Copersino, M.L.; Mintzer, M.Z. Cognitive performance in methadone maintenance patients: Effects of time relative to dosing and maintenance dose level. Exp. Clin. Psychopharmacol. 2014, 22, 248–256. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Drug Overdose Deaths in the U.S. Top 100,000 Annually; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. [Google Scholar]
- Centers for Disease Control and Prevention. HIV and People Who Inject Drugs. 2020. Available online: https://www.cdc.gov/hiv/group/hiv-idu.html (accessed on 29 September 2020).

{kind=link}
| Time | Control Condition | Experimental Condition |
|---|---|---|
| 0:00 | Begin Group—Introduce topics to be discussed Facilitator introduces purpose of group: HIV prevention and Harm Reduction | Begin Group—Introduce topics to be discussed Facilitator introduces purpose of group: HIV prevention and Harm Reduction Accommodation strategy: Mention of group etiquette, use of agenda on the board for patients to refer to throughout the session and mindfulness meditation Pre-recorded breathing exercise |
| 0:05 | Engaging in healthcare/advocacy/ resources available Distribute handout with list of local healthcare resources available | Engaging in healthcare/advocacy/resources available Distribute handout with list of local healthcare resources available Accommodation strategy: Have patients discuss resources they have used/resources they need |
| 0:10 | Harm Reduction Explain the concept of harm reduction with example strategies, Pyramid of Harms/types of Harm, ABC’s of harm reduction | Harm Reduction Explain the concept of harm reduction with example strategies, Pyramid of Harms/types of Harm, ABC’s of harm reduction Accommodation strategy: Use of projector and use of whiteboard to relay info |
| 0:20 | HIV infection risk/Risk behaviors/ Risk perception Review how HIV is transmitted, Bodily Fluids: Injection Drug Use and Sex, PrEP | HIV infection risk/Risk behaviors/Risk perception Review how HIV is transmitted, Bodily Fluids: Injection Drug Use and Sex, PrEP Accommodation strategy: True or False Activity, Use of Visuals, Use of Catch Phrases, Case Study Scenarios |
| 0:25 | HIV prevention skills Distribute handout with the steps of how to apply a condom and how to clean a needle | HIV prevention skills Distribute handout with the steps of how to apply a condom and how to clean a needle Accommodation strategy: Facilitator demonstration of how to apply a condom and how to clean a needle, followed by participant demonstrations |
| 0:35 | Communication skills/refusal skills Group discussion on how to talk to a partner about safe sex, negotiating partner support | Communication skills/refusal skills Group discussion on how to talk to a partner about safe sex, negotiating partner support Accommodation strategy: Video on partner communication, debrief on video, practice communication skills |
| 0:40 | Closure Ask the group to share personal experiences and if they have any questions | Closure Ask the group to share personal experiences and if they have any questions Accommodation strategy: Goal setting with patients, SMART goals |
| 0:45 | End session | End session |
| Demographic | Standard Condition (Mean, S.D.) (n, %) | Experimental Condition (Mean, S.D.) (n, %) | Total (Mean, S.D.) (n, %) | p-Value |
|---|---|---|---|---|
| Age | 43 (11.05) | 48 (11.52) | 44.7 (11.49) | 0.335 |
| BINI score | 125 (50.48) | 135 (35.63) | 130 (43.29) | 0.608 |
| Methadone dosage (mg) | 98.1 (11.81) | 63.5 (32.58) | 80.8 (22.19) | 0.005 * |
| Length of substance use (years) | 18.1 (12.19) | 23.3 (10.86) | 20.7 (11.53) | 0.327 |
| Gender | ||||
| Male | 5 (50) | 4 (40) | 9 (45) | 0.653 |
| Female | 5 (50) | 6 (60) | 11 (55) | |
| Ethnicity | ||||
| Caucasian | 4 (40) | 5 (50) | 9 (45) | 0.302 |
| African American | 5 (50) | 2 (20) | 7 (35) | |
| Hispanic or Latinx | 1 (10) | 3 (30) | 4 (20) | |
| Education level | ||||
| Some high school, no degree | 1 (10) | 2 (20) | 3 (15) | 0.663 |
| High school degree | 6 (60) | 4 (40) | 10 (50) | |
| 2-year college degree | 1 (10) | 0 (0.0) | 1 (5) | |
| Trade school degree | 1 (10) | 2 (20) | 3 (15) | |
| Some college, no degree | 1 (10) | 2 (20) | 3 (15) | |
| Psychiatric visit in past 12 months | ||||
| No | 5 (50) | 4 (40) | 9 (45) | 0.653 |
| Yes | 5 (50) | 6 (60) | 11 (55) | |
| History of injection drug use | ||||
| No | 1 (10) | 1 (10) | 2 (10) | 1.00 |
| Yes | 9 (90) | 9 (90) | 18 (90) | |
| Acceptability of Accommodation Strategies | n | % |
|---|---|---|
| Was today’s session covered verbally, visually, and with hands-on practice? | 10 | 100% |
| Was it helpful to use different ways of learning? | 10 | 100% |
| What method helped the most? (Check all that apply) | ||
| Verbal | 0 | 0% |
| Visual | 1 | 10% |
| Hands on | 1 | 10% |
| All the Above | 9 | 90% |
| Was mindfulness meditation used at the start of today’s session? | 10 | 100% |
| Was the mindfulness meditation helpful? | 8 | 80% |
| How did mindfulness meditation help? (Check all that apply) | ||
| Helped me focus on learning the material | 4 | 40% |
| Helped calm my mind so I could learn | 6 | 60% |
| Was a specific set of topics presented with an agenda at the start of today’s session? | 10 | 100% |
| Was this agenda of topics helpful? | 10 | 100% |
| How did this agenda help? (Check all that apply) | ||
| Kept the group organized | 3 | 30% |
| Helped me pay attention better | 5 | 50% |
| Helped me know what was coming up next | 5 | 50% |
| Did you discuss risk scenarios in today’s session? | 10 | 100% |
| Were those discussions helpful? | 10 | 100% |
| What was helpful about that discussion? (Check all that apply) | ||
| Helped me plan for risky situations | 6 | 60% |
| Helped me learn from others | 1 | 10% |
| Helped me think about to handle things in the future | 6 | 60% |
| Did you get feedback from other group members in today’s session? | 10 | 100% |
| Did that feedback help you learn the information? | 10 | 100% |
| What was useful about getting feedback (Check all that apply) | ||
| Helped me understand the information better | 6 | 60% |
| Helped me learn from others | 4 | 40% |
| Did the leader close today’s group with a summary of what was covered? | 10 | 100% |
| How was that summary useful? (Check all that apply) | ||
| Helped me recall what was learned | 6 | 60% |
| Helped me keep the information organized before ending | 8 | 80% |
| Helped me pay attention to the overall message | 1 | 10% |
| Helped me pay attention to the overall message | 1 | 10% |
| Time | Condition | Mean Difference | Std. Error | p-Value | 95% C.I. | Observed Power |
|---|---|---|---|---|---|---|
| Pre-post | experimental | 4.875 | 1.700 | 0.012 * | (1.228–8.522) | 0.760 |
| standard | −4.875 | 1.700 | ||||
| Pre-follow up | experimental | 5.875 | 2.218 | 0.019 * | (1.119–10.631) | 0.693 |
| standard | −5.975 | 2.218 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mistler, C.; Copenhaver, M. Integrating Cognitive Dysfunction Accommodation Strategies into an HIV Prevention Session: A 2-Arm Pilot Feasibility Study. Int. J. Environ. Res. Public Health 2022, 19, 9430. https://doi.org/10.3390/ijerph19159430
Mistler C, Copenhaver M. Integrating Cognitive Dysfunction Accommodation Strategies into an HIV Prevention Session: A 2-Arm Pilot Feasibility Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9430. https://doi.org/10.3390/ijerph19159430
Chicago/Turabian StyleMistler, Colleen, and Michael Copenhaver. 2022. "Integrating Cognitive Dysfunction Accommodation Strategies into an HIV Prevention Session: A 2-Arm Pilot Feasibility Study" International Journal of Environmental Research and Public Health 19, no. 15: 9430. https://doi.org/10.3390/ijerph19159430
APA StyleMistler, C., & Copenhaver, M. (2022). Integrating Cognitive Dysfunction Accommodation Strategies into an HIV Prevention Session: A 2-Arm Pilot Feasibility Study. International Journal of Environmental Research and Public Health, 19(15), 9430. https://doi.org/10.3390/ijerph19159430