
Effects of 90 Min Napping on Fatigue and Associated Environmental Factors among Nurses Working Long Night Shifts: A Longitudinal Observational Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Operational Definition
2.2. Study Design
2.3. Participants
2.4. Work Condition
2.5. Measures
2.5.1. Nurses’ Characteristics
2.5.2. Sleep/Activity
- TIB (min): Time in bed. Duration with a lying posture.
- SL (min): Sleep latency. The interval duration between the time of changing posture from standing to lying and the first sleep-onset time.
- WASO (min): Wake after sleep onset. The total duration one stays awake during the sleep onset to sleep offset interval.
- BOT (min): Bed-out time. The interval duration between the last awakening time and the time of changing posture from lying to standing.
- TND (min): Total nap duration. The TIB from which SL, WASO, and BOT were subtracted; sleeping duration.
- SE (%): Sleep efficiency. The ratio of TND to TIB. This represented napping quality.
2.5.3. Napping Environment
2.5.4. Ways of Spending Breaks
2.5.5. Working Environment
2.5.6. Fatigue
2.6. Statistical Analysis
3. Results
3.1. Nurses’ Characteristics
3.2. Characteristics and Cumulative Fatigue of Nurses Based on the Number of Naps with TND ≥ 90 Min during Four Night Shifts
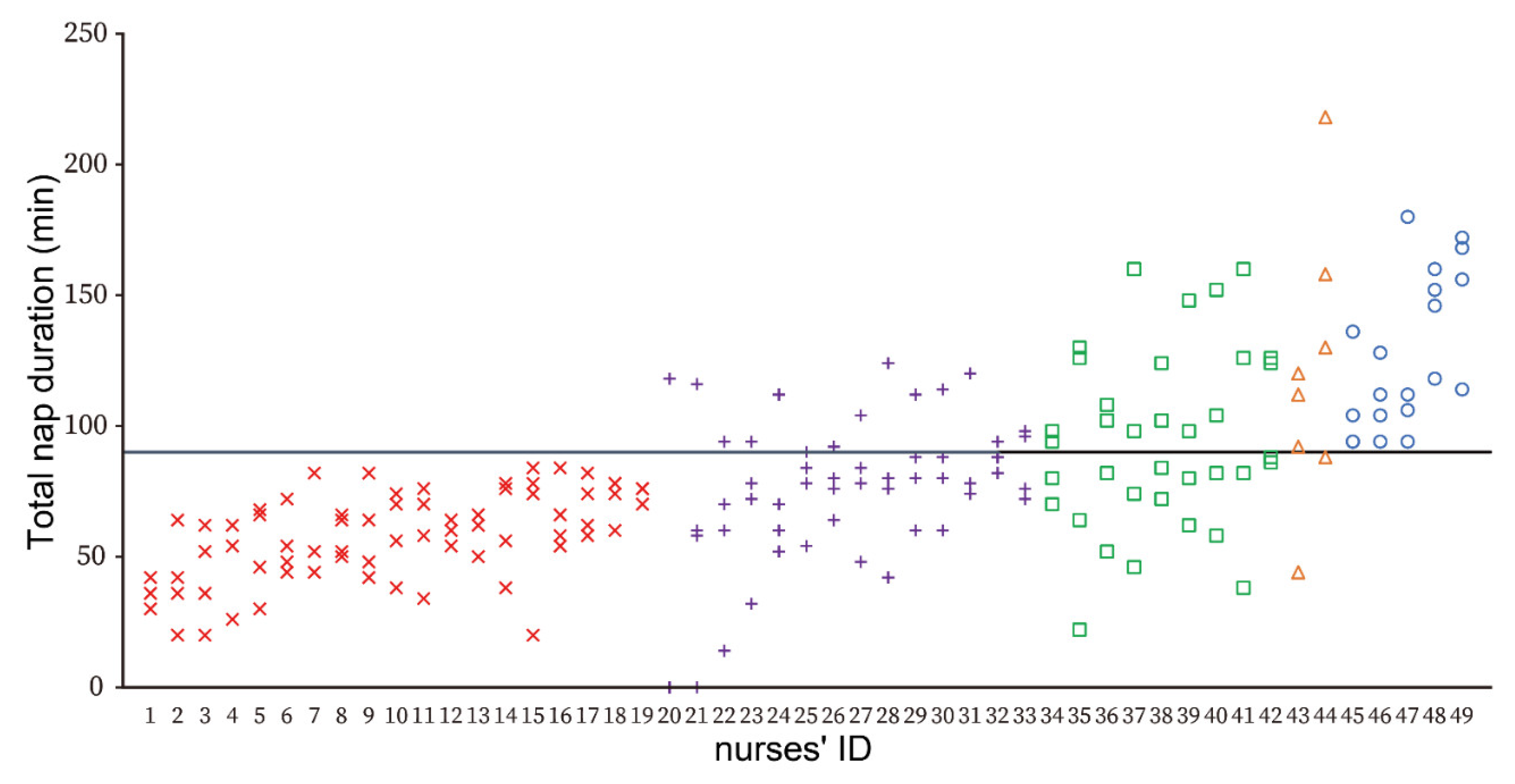
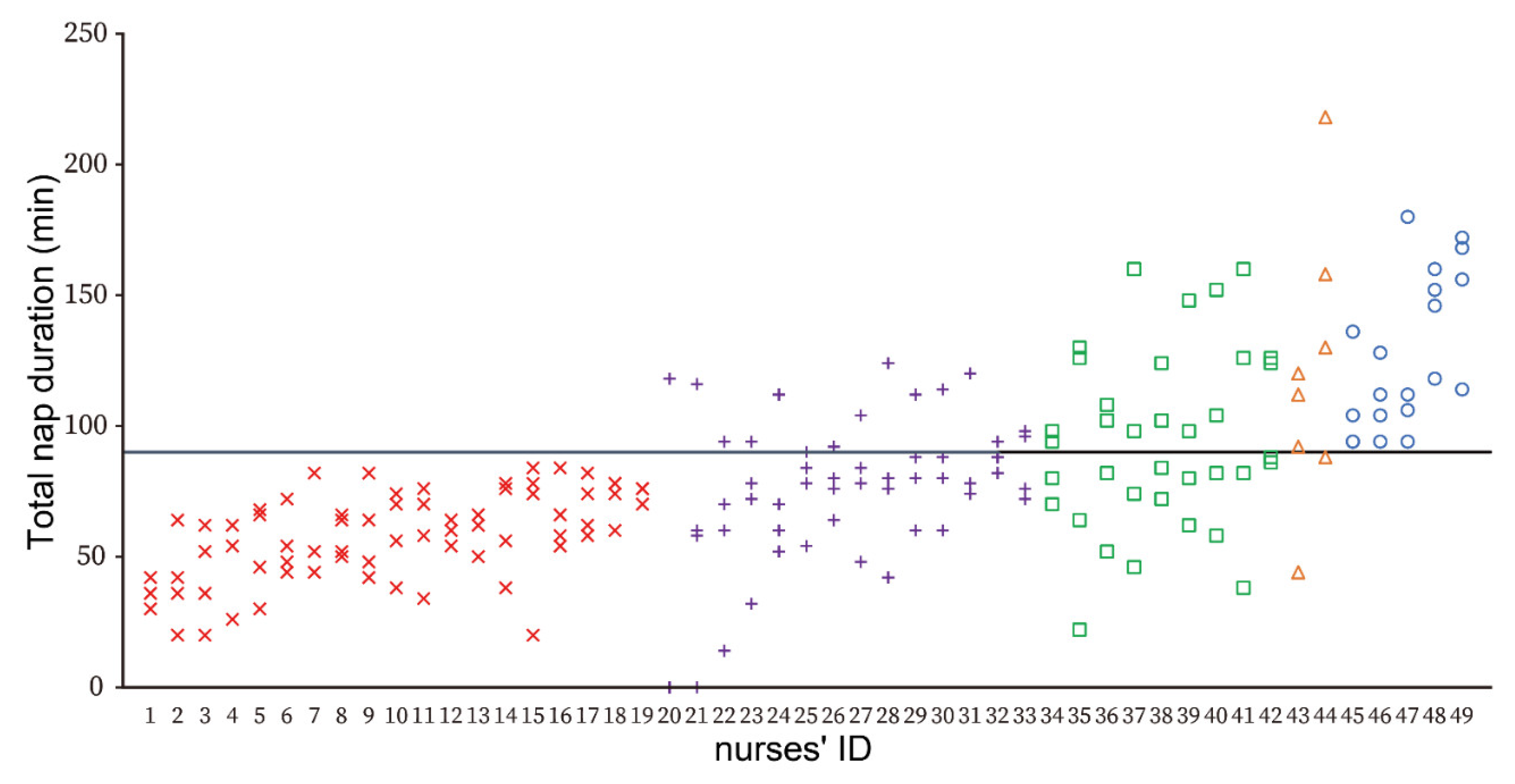
3.3. Characteristics of Napping with TND ≥ 90 Min
3.4. Napping Environment, Ways of Spending Breaks, and Working Environment during Night Shifts
3.5. Environmental Factors Associated with a Night Shift of TND ≥ 90 Min
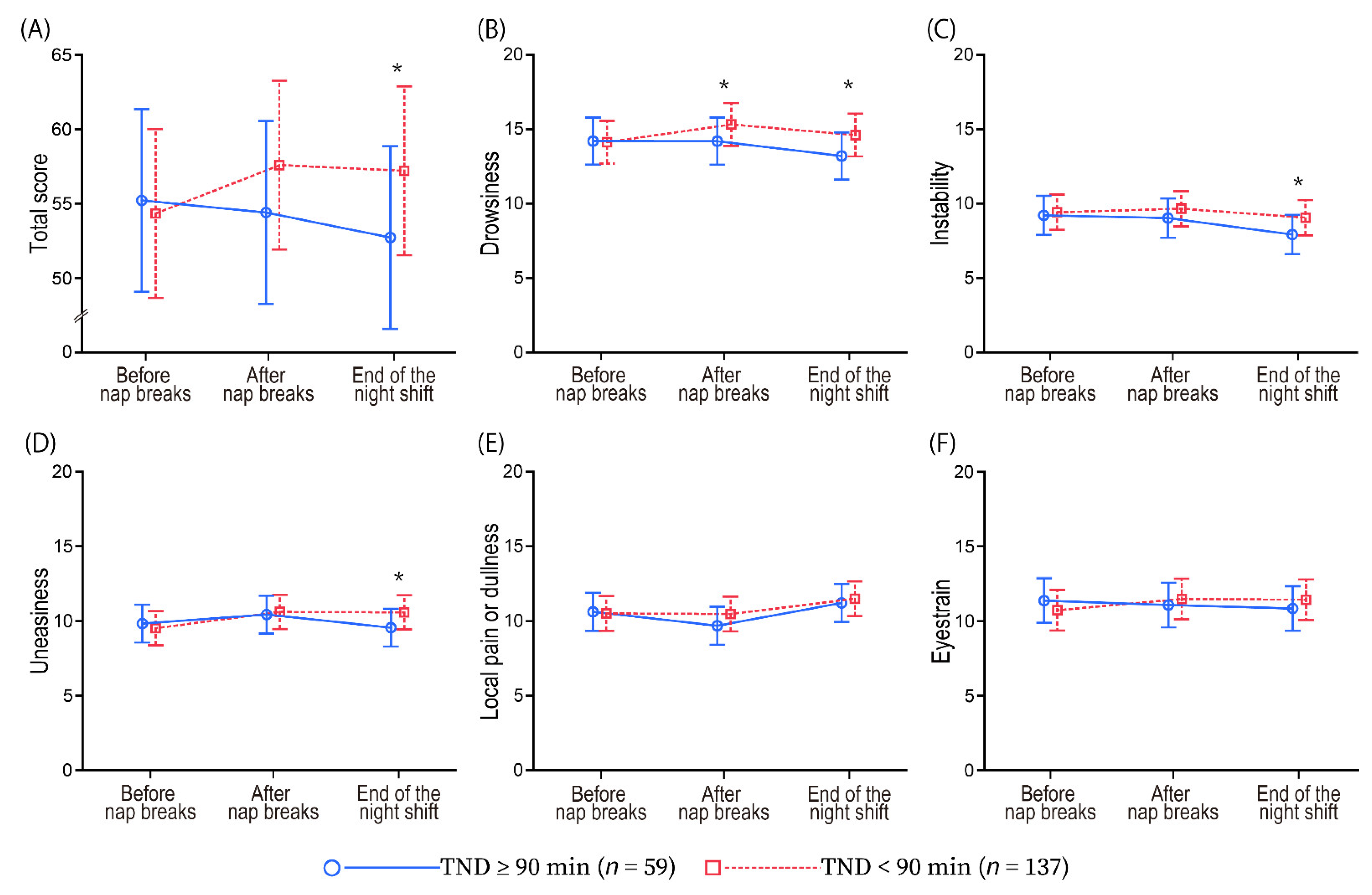
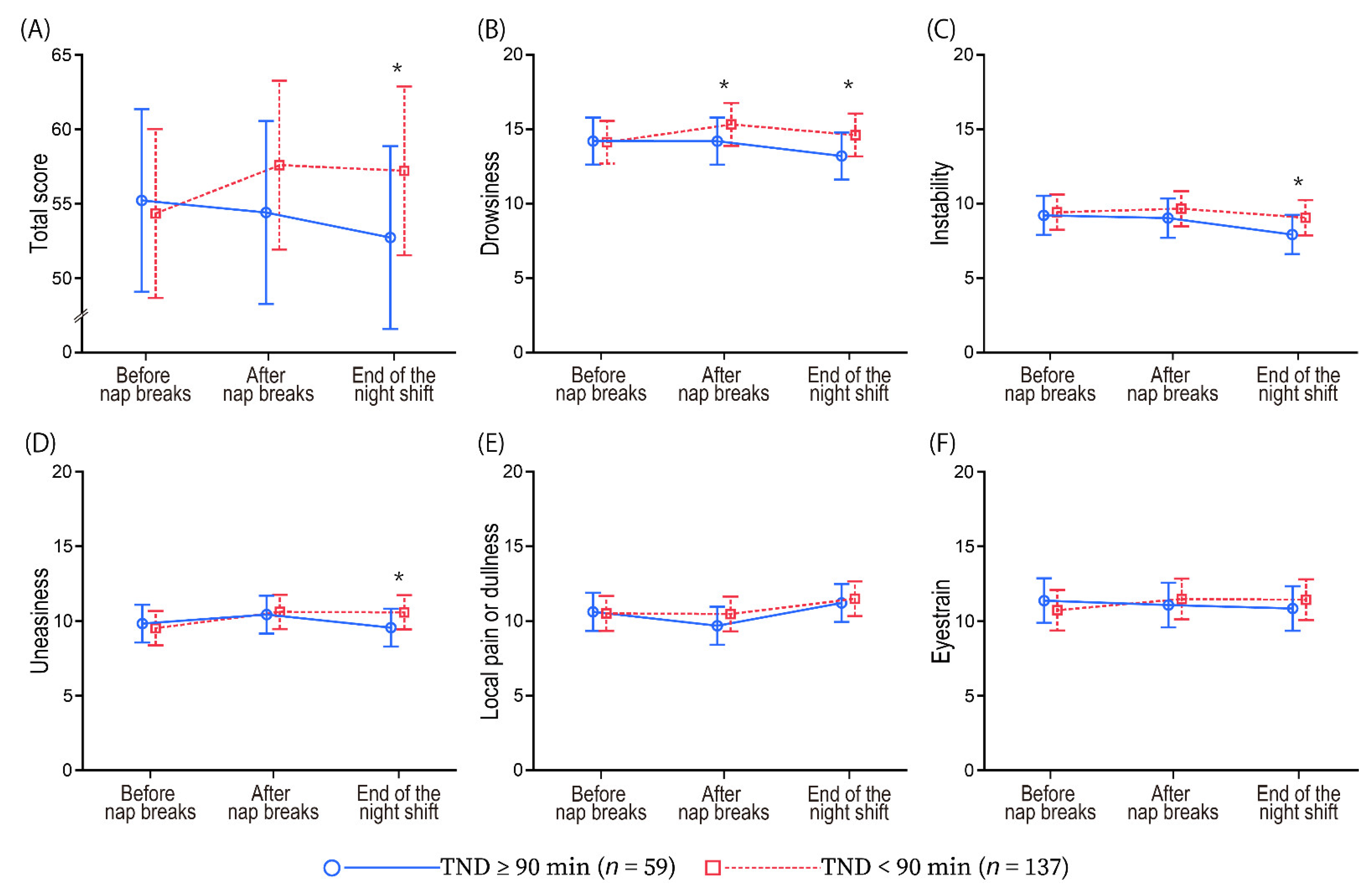
3.6. Relationship between Naps with TND ≥ 90 Min and Feelings of Fatigue
4. Discussion
4.1. Napping with TND ≥ 90 Min and Associated Factors
4.2. Effects of TND ≥ 90 Min on Fatigue
4.3. Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bae, S.-H.; Fabry, D. Assessing the relationships between nurse work hours/overtime and nurse and patient outcomes: Systematic literature review. Nurs. Outlook 2014, 62, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Trinkoff, A.M.; Johantgen, M.; Storr, C.L.; Gurses, A.P.; Liang, Y.; Han, K. Nurses’ Work Schedule Characteristics, Nurse Staffing, and Patient Mortality. Nurs. Res. 2011, 60, 1–8. [Google Scholar] [CrossRef]
- Dall’Ora, C.; Griffiths, P.; Emmanuel, T.; Rafferty, A.M.; Ewings, S.; Sermeus, W.; Heede, K.V.D.; Bruyneel, L.; Lesaffre, E.; Aiken, L.; et al. 12-hr shifts in nursing: Do they remove unproductive time and information loss or do they reduce education and discussion opportunities for nurses? A cross-sectional study in 12 European countries. J. Clin. Nurs. 2020, 29, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Stimpfel, A.W.; Aiken, L.H. Hospital Staff Nurses’ Shift Length Associated with Safety and Quality of Care. J. Nurs. Care Qual. 2013, 28, 122–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Nursing Association. Survey on Hospital Nursing 2020. Available online: https://www.nurse.or.jp/home/publication/pdf/research/96.pdf (accessed on 4 June 2022). (In Japanese).
- Barker, L.M.; Nussbaum, M.A. Fatigue, performance and the work environment: A survey of registered nurses. J. Adv. Nurs. 2011, 67, 1370–1382. [Google Scholar] [CrossRef] [PubMed]
- Smith-Miller, C.A.; Shaw-Kokot, J.; Curro, B.; Jones, C.B. An Integrative Review: Fatigue among Nurses in Acute Care Settings. JONA J. Nurs. Adm. 2014, 44, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.; Permito, R.; English, A.; Albritton, S.; Coogle, C.; Van Dongen, H.P.A. Performance and sleepiness in nurses working 12-h day shifts or night shifts in a community hospital. Accid. Anal. Prev. 2019, 126, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Geiger-Brown, J.; Rogers, V.E.; Trinkoff, A.M.; Kane, R.L.; Bausell, R.B.; Scharf, S.M. Sleep, Sleepiness, Fatigue, and Performance of 12-Hour-Shift Nurses. Chrono. Int. 2012, 29, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Lowe, C.J.; Safati, A.; Hall, P.A. The neurocognitive consequences of sleep restriction: A meta-analytic review. Neurosci. Biobehav. Rev. 2017, 80, 586–604. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.E. Chapter 40: The Effects of Fatigue and Sleepiness on Nurse Performance and Patient Safety. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008; pp. 2-509–2-545. ISBN 9781587633539. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2645/ (accessed on 4 June 2022).
- Caldwell, J.A.; Caldwell, J.L.; Thompson, L.A.; Lieberman, H.R. Fatigue and its management in the workplace. Neurosci. Biobehav. Rev. 2019, 96, 272–289. [Google Scholar] [CrossRef] [PubMed]
- American Nurses Association. Position Statement: Addressing Nurse Fatigue to Promote Safety and Health: Joint Responsibilities of Registered Nurses and Employers to Reduce Risks. Available online: https://www.nursingworld.org/~49de63/globalassets/practiceandpolicy/health-and-safety/nurse-fatigue-position-statement-final.pdf (accessed on 4 June 2022).
- Japanese Nursing Association. Guidelines on Night Shift and Shift Work for Nurses. Available online: https://www.nurse.or.jp/home/publication/pdf/guideline/yakin_guideline.pdf (accessed on 4 June 2022). (In Japanese).
- Li, H.; Shao, Y.; Xing, Z.; Li, Y.; Wang, S.; Zhang, M.; Ying, J.; Shi, Y.; Sun, J. Napping on night-shifts among nursing staff: A mixed-methods systematic review. J. Adv. Nurs. 2019, 75, 291–312. [Google Scholar] [CrossRef] [PubMed]
- Martin-Gill, C.; Barger, L.K.; Moore, C.G.; Higgins, J.S.; Teasley, E.M.; Weiss, P.M.; Condle, J.P.; Flickinger, K.L.; Coppler, P.J.; Sequeira, D.J.; et al. Effects of Napping During Shift Work on Sleepiness and Performance in Emergency Medical Services Personnel and Similar Shift Workers: A Systematic Review and Meta-Analysis. Prehosp. Emerg. Care 2018, 22, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.D.; Liszka, M.K.; Mcilvaine, Q.S.; Nong, L.; Weaver, M.D.; Turner, R.L.; Platt, T.E.; Opitz, S.E.; Guyette, F.X.; Martin-Gill, C.; et al. Does the evidence support brief (≤30-mins), moderate (31–60-mins), or long duration naps (61+ mins) on the night shift? A systematic review. Sleep Med. Rev. 2021, 59, 101509. [Google Scholar] [CrossRef] [PubMed]
- Geiger-Brown, J.; Sagherian, K.; Zhu, S.; Wieroniey, M.A.; Blair, L.; Warren, J.; Hinds, P.S.; Szeles, R. CE: Original Research: Napping on the Night Shift: A Two-Hospital Implementation Project. Am. J. Nurs. 2016, 116, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith-Coggins, R.; Howard, S.K.; Mac, D.T.; Wang, C.; Kwan, S.; Rosekind, M.R.; Sowb, Y.; Balise, R.; Levis, J.; Gaba, D.M. Improving Alertness and Performance in Emergency Department Physicians and Nurses: The Use of Planned Naps. Ann. Emerg. Med. 2006, 48, 596–604.e3. [Google Scholar] [CrossRef]
- Barthe, B.; Tirilly, G.; Gentil, C.; Toupin, C. Job demands and resting and napping opportunities for nurses during night shifts: Impact on sleepiness and self-evaluated quality of healthcare. Ind. Health 2016, 54, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Kagamiyama, H.; Sumi, N.; Yoshida, Y.; Sugimura, N.; Nemoto, F.; Yano, R. Association between sleep and fatigue in nurses who are engaged in 16 h night shifts in Japan: Assessment using actigraphy. Jpn. J. Nurs. Sci. 2019, 16, 373–384. [Google Scholar] [CrossRef]
- Da Borges, F.N.S.; Fischer, F.M.; Rotenberg, L.; Soares, N.S.; Fonseca, M.B.; Smolensky, M.H.; Sackettlundeen, L.; Haus, E.; de Moreno, C.R.C. Effects of Naps at Work on the Sleepiness of 12-Hour Night Shift Nursing Personnel. Sleep Sci. 2009, 2, 24–29. [Google Scholar]
- Ruggiero, J.S.; Redeker, N.S. Effects of Napping on Sleepiness and Sleep-Related Performance Deficits in Night-Shift Workers: A Systematic Review. Biol. Res. Nurs. 2014, 16, 134–142. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Dement, W.C. Chapter 2: Normal Human Sleep: An Overview. In Principles and Practice of Sleep Medicine, 6th ed.; Kryger, M., Roth, T., Dement, W.C., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 15–24. ISBN 9780323242882. [Google Scholar]
- Léger, D.; Debellemaniere, E.; Rabat, A.; Bayon, V.; Benchenane, K.; Chennaoui, M. Slow-wave sleep: From the cell to the clinic. Sleep Med. Rev. 2018, 41, 113–132. [Google Scholar] [CrossRef]
- Fallis, W.M.; McMillan, D.E.; Edwards, M.P. Napping During Night Shift: Practices, Preferences, and Perceptions of Critical Care and Emergency Department Nurses. Crit. Care Nurse 2011, 31, e1–e11. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.P.; McMillan, D.E.; Fallis, W.M. Napping during breaks on night shift: Critical care nurse managers’ perceptions. Dynamics 2013, 24, 30–35. [Google Scholar] [PubMed]
- Irish, L.A.; Kline, C.E.; Gunn, H.E.; Buysse, D.J.; Hall, M.H. The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Med. Rev. 2015, 22, 23–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.-S.; Wu, Y.-H.; Lu, M.R.; Hsu, C.-Y.; Liu, C.-K.; Hsu, C. Did a brief nap break have positive benefits on information processing among nurses working on the first 8-h night shift? Appl. Ergon. 2015, 48, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Oriyama, S.; Miyakoshi, Y.; Kobayashi, T. Effects of Two 15-min Naps on the Subjective Sleepiness, Fatigue and Heart Rate Variability of Night Shift Nurses. Ind. Health 2014, 52, 25–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva-Costa, A.; de Araú, M.M.; Nagai, R.; Fischer, F.M. Environmental and Organizational Conditions for Napping during Night Work: A Qualitative Study among Nursing Professionals. Sleep Sci. 2010, 3, 11–15. [Google Scholar]
- Touitou, Y.; Reinberg, A.; Touitou, D. Association between light at night, melatonin secretion, sleep deprivation, and the internal clock: Health impacts and mechanisms of circadian disruption. Life Sci. 2017, 173, 94–106. [Google Scholar] [CrossRef]
- Basner, M.; Müller, U.; Elmenhorst, E.-M. Single and Combined Effects of Air, Road, and Rail Traffic Noise on Sleep and Recuperation. Sleep 2011, 34, 11–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troynikov, O.; Watson, C.G.; Nawaz, N. Sleep environments and sleep physiology: A review. J. Therm. Biol. 2018, 78, 192–203. [Google Scholar] [CrossRef]
- Faraut, B.; Andrillon, T.; Vecchierini, M.-F.; Leger, D. Napping: A public health issue. From epidemiological to laboratory studies. Sleep Med. Rev. 2017, 35, 85–100. [Google Scholar] [CrossRef]
- Caruso, C.C.; Hitchcock, E.M. Strategies for Nurses to Prevent Sleep-Related Injuries and Errors. Rehabilitation Nurs. 2010, 35, 192–197. [Google Scholar] [CrossRef]
- Wendsche, J.; Ghadiri, A.; Bengsch, A.; Wegge, J. Antecedents and outcomes of nurses’ rest break organization: A scoping review. Int. J. Nurs. Stud. 2017, 75, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Japanese Nursing Association. Survey on Hospital Nursing 2018. Available online: https://www.nurse.or.jp/home/publication/pdf/research/94.pdf (accessed on 4 June 2022). (In Japanese).
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National sleep foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Stock, D.; Knight, J.A.; Raboud, J.; Cotterchio, M.; Strohmaier, S.; Willett, W.; Eliassen, A.H.; Rosner, B.; Hankinson, S.E.; Schernhammer, E. Rotating night shift work and menopausal age. Hum. Reprod. 2019, 34, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Gava, G.; Orsili, I.; Alvisi, S.; Mancini, I.; Seracchioli, R.; Meriggiola, M.C. Cognition, Mood and Sleep in Menopausal Transition: The Role of Menopause Hormone Therapy. Medicina 2019, 55, 668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Center for Environmental Therapeutics. Morningness-Eveningness Questionnaire Self-Assessment Version (MEQ-SA). Available online: https://cet.org/wp-content/uploads/2019/11/MEQ-SA-EN.pdf (accessed on 4 June 2022).
- Matsuo, M.; Masuda, F.; Sumi, Y.; Takahashi, M.; Yamada, N.; Ohira, M.H.; Fujiwara, K.; Kanemura, T.; Kadotani, H. Comparisons of Portable Sleep Monitors of Different Modalities: Potential as Naturalistic Sleep Recorders. Front. Neurol. 2016, 7, 110. [Google Scholar] [CrossRef] [PubMed]
- Nakazaki, K.; Kitamura, S.; Motomura, Y.; Hida, A.; Kamei, Y.; Miura, N.; Mishima, K. Validity of an algorithm for determining sleep/wake states using a new actigraph. J. Physiol. Anthropol. 2014, 33, 31. [Google Scholar] [CrossRef] [Green Version]
- Brzozowski, S.L.; Cho, H.; Arsenault Knudsen, É.N.; Steege, L.M. Predicting nurse fatigue from measures of work demands. Appl. Ergon. 2021, 92, 103337. [Google Scholar] [CrossRef]
- Kosugoh, R.; Fujii, H.; Hirata, A. Subjective Assessment of Workload (1): Revision of the Cumulative Fatigue Symptoms Index. J. Sci. Labour 1992, 68, 489–502. (In Japanese) [Google Scholar]
- Sakai, K. Revision of the Jikaku-sho shirabe in 2002. Dig Sci. Labour 2002, 57, 295–298. (In Japanese) [Google Scholar]
- Snijders, T.A.B.; Bosker, R.J. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling, 2nd ed.; SAGE: Thousand Oaks, CA, USA, 2011; ISBN 9781446254332. [Google Scholar]
- Ficca, G.; Axelsson, J.; Mollicone, D.J.; Muto, V.; Vitiello, M.V. Naps, cognition and performance. Sleep Med. Rev. 2010, 14, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Zion, N.; Shochat, T. Let them sleep: The effects of a scheduled nap during the night shift on sleepiness and cognition in hospital nurses. J. Adv. Nurs. 2019, 75, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 15 July 2022).
- Saksvik, I.B.; Bjorvatn, B.; Hetland, H.; Sandal, G.M.; Pallesen, S. Individual differences in tolerance to shift work–A systematic review. Sleep Med. Rev. 2011, 15, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, A. Methodological Aspects of Shift-Work Research. Chrono-Int. 2004, 21, 1037–1047. [Google Scholar] [CrossRef]
- Purnell, M.T.; Feyer, A.-M.; Herbison, G.P. The impact of a nap opportunity during the night shift on the performance and alertness of 12-h shift workers. J. Sleep Res. 2002, 11, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Loupa, G.; Katikaridis, A.; Karali, D.; Rapsomanikis, S. Mapping the noise in a Greek general hospital. Sci. Total Environ. 2019, 646, 923–929. [Google Scholar] [CrossRef]
- World Health Organization. Night Noise Guidelines for Europe; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2009; ISBN 9789289041737. [Google Scholar]
- Gooley, J.J.; Chamberlain, K.; Smith, K.A.; Khalsa, S.B.S.; Rajaratnam, S.M.W.; Van Reen, E.; Zeitzer, J.M.; Czeisler, C.A.; Lockley, S.W. Exposure to room light before bedtime suppresses melatonin onset and shortens melatonin duration in humans. J. Clin. Endocrinol. Metab. 2011, 96, E463–E472. [Google Scholar] [CrossRef] [Green Version]
- Santhi, N.; Thorne, H.C.; van der Veen, D.R.; Johnsen, S.; Mills, S.L.; Hommes, V.; Schlangen, L.J.M.; Archer, S.N.; Dijk, D.-J. The spectral composition of evening light and individual differences in the suppression of melatonin and delay of sleep in humans. J. Pineal Res. 2012, 53, 47–59. [Google Scholar] [CrossRef]
- Chang, A.-M.; Aeschbach, D.; Duffy, J.F.; Czeisler, C.A. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc. Natl. Acad. Sci. USA 2015, 112, 1232–1237. [Google Scholar] [CrossRef] [Green Version]
- Randjelović, P.; Stojiljković, N.; Radulović, N.; Ilić, I.; Stojanović, N.; Ilić, S. The association of smartphone usage with subjective sleep quality and daytime sleepiness among medical students. Biol. Rhythm Res. 2019, 50, 857–865. [Google Scholar] [CrossRef]
- Xie, X.; Dong, Y.; Wang, J. Sleep quality as a mediator of problematic smartphone use and clinical health symptoms. J. Behav. Addict. 2018, 7, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Takahashi, M.; Takeyama, H.; Matsumoto, S.; Ebara, T.; Murata, K.; Tachi, N.; Itani, T. How do the Timing and Length of a Night-Shift Nap Affect Sleep Inertia? Chronobiol. Int. 2010, 27, 1031–1044. [Google Scholar] [CrossRef] [PubMed]
- Hilditch, C.J.; McHill, A.W. Sleep inertia: Current insights. Nat. Sci. Sleep 2019, 11, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhéaume, A.; Mullen, J. The impact of long work hours and shift work on cognitive errors in nurses. J. Nurs. Manag. 2018, 26, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ji, X.; Zhou, W.; Liu, J. Sleep problems in shift nurses: A brief review and recommendations at both individual and institutional levels. J. Nurs. Manag. 2019, 27, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Arito, H.; Fukuda, H. Nurses’ workload associated with 16-h night shifts. II: Effects of a nap taken during the shifts. Psychiatry Clin. Neurosci. 1999, 53, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Boivin, D.B.; Boudreau, P. Impacts of shift work on sleep and circadian rhythms. Pathol. Biol. 2014, 62, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Di Muzio, M.; Dionisi, S.; Di Simone, E.; Cianfrocca, C.; Di Muzio, F.; Fabbian, F.; Barbiero, G.; Tartaglini, D.; Giannetta, N. Can nurses’ shift work jeopardize the patient safety? A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4507–4519. [Google Scholar] [CrossRef] [PubMed]
- Konya, I.; Watanabe, K.; Shishido, I.; Sugimura, N.; Matsushita, Y.; Yamaguchi, S.; Yano, R. Post-Work Recovery from Fatigue and Sleep Episodes among Nurses Who Are Engaged in 16-Hour Night Shifts: A Prospective Observational Study. Healthcare 2022, 10, 1089. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Mean (SD) |
|---|---|
| Age (years) | 28.8 (4.2) |
| Nursing experience (years) | 7.0 (4.2) |
| Nursing experience in the current ward (years) | 3.4 (2.2) |
| n (%) | |
| Sex | |
| Male | 3 (6.1) |
| Female | 46 (93.9) |
| Marital status (Yes) | 8 (16.3) |
| Child-rearing (Yes) | 5 (10.2) |
| Ward | |
| A (medical) | 12 (24.5) |
| B (medical) | 13 (26.5) |
| C (medical) | 5 (10.2) |
| D (surgical) | 5 (10.2) |
| E (medical) | 4 (8.2) |
| F (surgical) | 10 (20.4) |
| Variables | Mean (SD) |
|---|---|
| Sleep | |
| Subjective mean daily sleep duration (hour) | 6.3 (0.9) |
| n (%) | |
| Take napping before night shift (Yes) | 13 (26.5) |
| Chronotype | |
| Definite morning type | 0 (0.0) |
| Moderate morning type | 6 (12.2) |
| Intermediate type | 34 (69.4) |
| Moderate evening type | 8 (16.3) |
| Definite evening type | 1 (2.1) |
| Sleep-related habits | |
| Frequency of caffeine intake | |
| Rarely drink (Can’t drink) | 18 (36.7) |
| <2 times/week | 10 (20.4) |
| 3–4 times/week | 6 (12.2) |
| 5–6 times/week | 4 (8.2) |
| Every day | 11 (22.5) |
| Daily time spent on electronic devices | |
| 30–59 min | 1 (2.1) |
| 1–2 h | 18 (36.7) |
| ≥2 h | 30 (61.2) |
| Time spent on electronic devices before bedtime | |
| None | 1 (2.1) |
| <15 min | 7 (14.3) |
| 15–29 min | 8 (16.3) |
| 30–44 min | 17 (34.7) |
| 45–59 min | 9 (18.3) |
| ≥60 min | 7 (14.3) |
| Variables | None | One/Two Night Shifts | Three/Four Night Shifts | p | Post Hoc |
|---|---|---|---|---|---|
| (n = 19) | (n = 23) | (n = 7) | |||
| Median (IQR) | |||||
| Age (years) | 29.0 (26.0, 30.0) | 27.0 (24.0, 31.0) | 33.0 (28.0, 33.0) | 0.097 | |
| Nursing experience (years) | 6.2 (3.3, 8.3) | 5.3 (3.2, 9.0) | 10.2 (7.2, 12.2) | 0.038 | None < Three/Four * |
| Nursing experience in the current ward (years) | 2.7 (1.3, 3.8) | 3.3 (2.2, 5.3) | 4.2 (2.2, 5.0) | 0.497 | |
| Subjective mean daily sleep duration (hour) | 6.0 (5.5, 7.0) | 6.0 (5.5, 7.0) | 6.0 (6.0, 7.5) | 0.964 | |
| n (%) | |||||
| Gender | |||||
| Male | 1 (5.3) | 2 (8.7) | 0 (0.0) | 0.999 | |
| Female | 18 (94.7) | 21 (91.3) | 7 (100.0) | ||
| Marital status | |||||
| Yes | 5 (26.3) | 3 (13.0) | 0 (0.0) | 0.372 | |
| No | 14 (73.7) | 20 (87.0) | 7 (100.0) | ||
| Child-rearing | |||||
| Yes | 3 (15.8) | 2 (8.7) | 0 (0.0) | 0.682 | |
| No | 16 (84.2) | 21 (91.3) | 7 (100.0) | ||
| Take napping before night shift (Yes) | |||||
| Yes | 3 (15.8) | 7 (30.4) | 3 (42.9) | 0.302 | |
| No | 16 (84.2) | 16 (69.6) | 4 (57.1) | ||
| Chronotype | |||||
| Definite morning type | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.370 | |
| Moderate morning type | 2 (10.5) | 3 (13.0) | 1 (14.3) | ||
| Intermediate type | 14 (73.7) | 17 (73.9) | 3 (42.9) | ||
| Moderate evening type | 3 (15.8) | 2 (8.7) | 3 (42.9) | ||
| Definite evening type | 0 (0.0) | 1 (4.4) | 0 (0.0) | ||
| Frequency of caffeine intake | |||||
| Rarely drink (Can’t drink) | 5 (26.3) | 9 (39.1) | 4 (57.1) | 0.328 | |
| <2 times/week | 3 (15.8) | 7 (30.4) | 0 (0.0) | ||
| 3–4 times/week | 3 (15.8) | 2 (8.7) | 1 (14.3) | ||
| 5–6 times/week | 3 (15.8) | 0 (0.0) | 1 (14.3) | ||
| Every day | 5 (26.3) | 5 (21.8) | 1 (14.3) | ||
| Daily time spent on electronic devices | |||||
| 30–59 min | 0 (0.0) | 1 (4.4) | 0 (0.0) | 0.999 | |
| 1–2 h | 7 (36.8) | 8 (34.8) | 3 (42.9) | ||
| ≥2 h | 12 (63.2) | 14 (60.8) | 4 (57.1) | ||
| Time spent on electronic devices before bedtime | |||||
| None | 0 (0.0) | 1 (4.4) | 0 (0.0) | 0.721 | |
| <15 min | 2 (10.5) | 3 (13.0) | 2 (28.6) | ||
| 15–29 min | 4 (21.1) | 2 (8.7) | 2 (28.6) | ||
| 30–44 min | 6 (31.6) | 10 (43.5) | 1 (14.3) | ||
| 45–59 min | 5 (26.3) | 3 (13.0) | 1 (14.3) | ||
| ≥60 min | 2 (10.5) | 4 (17.4) | 1 (14.3) | ||
| Variables | TND < 90 min (n = 137) | TND ≥ 90 min (n = 59) | t | p |
|---|---|---|---|---|
| Sleep or Nap before the night shifts | ||||
| Last awakening time (h:m) | 10:52 (2:10) | 11:39 (1:57) | 2.42 | 0.016 |
| Last sleep or nap duration (hour) | 7.3 (3.2) | 6.8 (3.6) | −0.93 | 0.355 |
| Awakening duration until nap breaks (hour) | 13.9 (3.0) | 13.5 (2.5) | −0.76 | 0.450 |
| Nap breaks and napping during night shifts | ||||
| Start time of nap breaks (h:m) | 0:45 (1:53) | 1:12 (1:58) | 1.53 | 0.128 |
| TIB (min) | 104.6 (27.7) | 160.2 (32.3) | 12.24 | <0.001 |
| Start time of lying (h:m) | 1:02 (1:53) | 1:23 (1:57) | 1.19 | 0.235 |
| Start time of napping (h:m) | 1:30 (1:50) a | 1:40 (1:54) | 0.58 | 0.563 |
| SL (min) | 23.2 (18.9) a | 17.2 (12.3) | −2.23 | 0.027 |
| TND (min) | 60.5 (20.4) | 120.9 (27.1) | 17.15 | <0.001 |
| SE (%) | 59.6 (18.2) | 75.9 (9.7) | 6.48 | <0.001 |
| WASO (min) | 11.8 (13.6) a | 16.3 (14.4) | 2.07 | 0.040 |
| Frequency of awakenings during napping (Times) | 1.7 (1.4) a | 2.9 (1.8) | 5.04 | <0.001 |
| Frequency of postural changes (Times) | 2.5 (2.4) a | 4.3 (2.9) | 4.32 | <0.001 |
| End time of napping (h:m) | 2:44 (1:46) a | 3:58 (1:50) | 4.36 | <0.001 |
| BOT (min) | 6.4 (4.6) a | 5.9 (2.8) | −0.80 | 0.426 |
| End time of lying (h:m) | 2:47 (1:48) | 4:03 (1:50) | 4.54 | <0.001 |
| End time of nap breaks (h:m) | 2:58 (1:46) | 4:13 (1:50) | 4.45 | <0.001 |
| Subjective evaluation (%) | 47.1 (21.5) b | 65.9 (22.0) | 5.46 | <0.001 |
| Variables | Mean (SD) or n (%) | t | p | |
|---|---|---|---|---|
| TND < 90 min (n = 137) | TND ≥ 90 min (n = 59) | |||
| Napping environment | ||||
| Illuminance (lux) | 18.6 (89.3) | 11.0 (58.5) a | −0.59 | 0.556 |
| Noise level (dB LAeq, napping) | 42.3 (4.7) | 39.3 (4.8) | −4.11 | <0.001 |
| Temperature (°C) | 25.1 (1.3) | 24.9 (1.0) a | −1.05 | 0.294 |
| Humidity (%) | 66.2 (7.5) | 64.3 (6.3) a | −1.70 | 0.091 |
| Unpleasant smells (Yes) | 2 (1.5) | 0 (0.0) | 0.999 | |
| Japanese futons (Yes) | 40 (29.2) | 31 (52.5) | 0.002 | |
| Folding beds (Yes) | 36 (26.3) | 1 (1.7) | <0.001 | |
| Beds in vacant hospital room (Yes) | 23 (16.8) | 14 (23.7) | 0.320 | |
| Sofa beds (Yes) | 14 (10.2) | 7 (11.9) | 0.802 | |
| Stretchers (Yes) | 20 (14.6) | 0 (0.0) | 0.001 | |
| Examination tables (Yes) | 4 (2.9) | 6 (10.2) | 0.069 | |
| Bed sheets (Yes) | 124 (90.5) | 54 (91.5) | 0.999 | |
| Quilt (Yes) | 125 (91.2) | 55 (93.2) | 0.781 | |
| Toweling blankets (Yes) | 9 (6.6) | 10 (17.0) | 0.034 | |
| Pillow (Yes) | 117 (85.4) | 52 (88.1) | 0.822 | |
| Ways of spending breaks | ||||
| Caffeine consumption before nap breaks (Yes) | 67 (48.9) | 23 (40.4) b | 0.343 | |
| Carrying a PHS with the nurse call system (Yes) | 8 (5.8) | 10 (17.0) | 0.028 | |
| Time spent on electronic devices (min) | 29.8 (26.8) | 23.6 (26.5) | −1.50 | 0.136 |
| Changing clothes (Yes) | 8 (5.8) | 3 (5.1) | 0.999 | |
| Using a sleep mask (Yes) | 6 (4.4) | 4 (6.8) | 0.492 | |
| Using earplugs (Yes) | 2 (1.5) | 0 (0.0) | 0.999 | |
| Watching television (Yes) | 4 (2.9) | 4 (6.8) | 0.245 | |
| Listening to music (Yes) | 9 (6.6) | 1 (1.7) | 0.287 | |
| Doing remaining work (Yes) | 17 (12.4) | 3 (5.1) | 0.196 | |
| Eating (Yes) | 27 (19.7) | 21 (35.6) | 0.029 | |
| Working Environment | ||||
| Number of nurses | 3.0 (0.6) | 3.1 (0.7) | 0.14 | 0.886 |
| Number of care workers | 0.2 (0.4) | 0.4 (0.5) | 1.54 | 0.125 |
| Number of hospitalized patients | 22.1 (4.3) | 21.0 (4.1) | −1.68 | 0.095 |
| Number of patients each nurse responsible for | 8.2 (4.4) | 7.4 (3.0) | −1.25 | 0.213 |
| Supper breaks (Yes) | 137 (100.0) | 59 (100.0) | 0.999 | |
| Nap break duration (min) | 138.3 (27.7) | 182.2 (39.6) | 8.88 | <0.001 |
| Steps | 10,367.2 (2652.9) c | 8918.6 (2199.9) d | −3.23 | 0.002 |
| Steps before napping per hour | 736.5 (204.3) c | 648.6 (193.7) d | −2.47 | 0.014 |
| Steps after napping per hour | 752.7 (229.7) e | 769.5 (238.6) b | 0.46 | 0.648 |
| Variables | aOR [95% CIs] | p |
|---|---|---|
| Napping Environment | ||
| Noise level (dB LAeq, napping) | 0.88 [0.78, 0.98] | 0.022 |
| Humidity (%) | 0.94 [0.87, 1.02] | 0.152 |
| Japanese futons | ||
| Yes | 1.19 [0.34, 4.14] | 0.787 |
| No | 1.00 [Ref] | |
| Folding beds | ||
| Yes | 0.73 [0.06, 9.48] | 0.807 |
| No | 1.00 [Ref] | |
| Examination tables | ||
| Yes | 15.02 [0.80, 283.19] | 0.071 |
| No | 1.00 [Ref] | |
| Toweling blankets | ||
| Yes | 1.44 [0.29, 7.07] | 0.655 |
| No | 1.00 [Ref] | |
| Ways of spending breaks | ||
| Carrying a PHS with nurse call system | ||
| Yes | 1.71 [0.13, 22.86] | 0.686 |
| No | 1.00 [Ref] | |
| Time spent on electronic devices (min) | 0.97 [0.94, 0.99] | 0.009 |
| Doing remaining work | ||
| Yes | 0.24 [0.03, 2.01] | 0.188 |
| No | 1.00 [Ref] | |
| Eating | ||
| Yes | 1.78 [0.57, 5.54] | 0.319 |
| No | 1.00 [Ref] | |
| Working Environment | ||
| Number of care workers (person) | 1.17 [0.22, 6.30] | 0.854 |
| Number of hospitalized patients (person) | 0.87 [0.74, 1.04] | 0.124 |
| Nap break duration (min) | 1.04 [1.02, 1.07] | <0.001 |
| Steps before napping (100 steps/hour) | 0.75 [0.55, 1.03] | 0.078 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, K.; Sugimura, N.; Shishido, I.; Konya, I.; Yamaguchi, S.; Yano, R. Effects of 90 Min Napping on Fatigue and Associated Environmental Factors among Nurses Working Long Night Shifts: A Longitudinal Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 9429. https://doi.org/10.3390/ijerph19159429
Watanabe K, Sugimura N, Shishido I, Konya I, Yamaguchi S, Yano R. Effects of 90 Min Napping on Fatigue and Associated Environmental Factors among Nurses Working Long Night Shifts: A Longitudinal Observational Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9429. https://doi.org/10.3390/ijerph19159429
Chicago/Turabian StyleWatanabe, Kazuhiro, Naotaka Sugimura, Inaho Shishido, Issei Konya, Shinya Yamaguchi, and Rika Yano. 2022. "Effects of 90 Min Napping on Fatigue and Associated Environmental Factors among Nurses Working Long Night Shifts: A Longitudinal Observational Study" International Journal of Environmental Research and Public Health 19, no. 15: 9429. https://doi.org/10.3390/ijerph19159429
APA StyleWatanabe, K., Sugimura, N., Shishido, I., Konya, I., Yamaguchi, S., & Yano, R. (2022). Effects of 90 Min Napping on Fatigue and Associated Environmental Factors among Nurses Working Long Night Shifts: A Longitudinal Observational Study. International Journal of Environmental Research and Public Health, 19(15), 9429. https://doi.org/10.3390/ijerph19159429