
The Narrative Medicine Approach in the Treatment of Diabetic Macular Edema: An Italian Experience


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Patient Journey Map
2.2. Participants and Recruitment for the Narrative Medicine Phase
2.3. Data Collection and Narrative Analysis
3. Results
3.1. The Patient Journey
3.2. Sociodemographic Characteristics of DME Patients and Caregivers
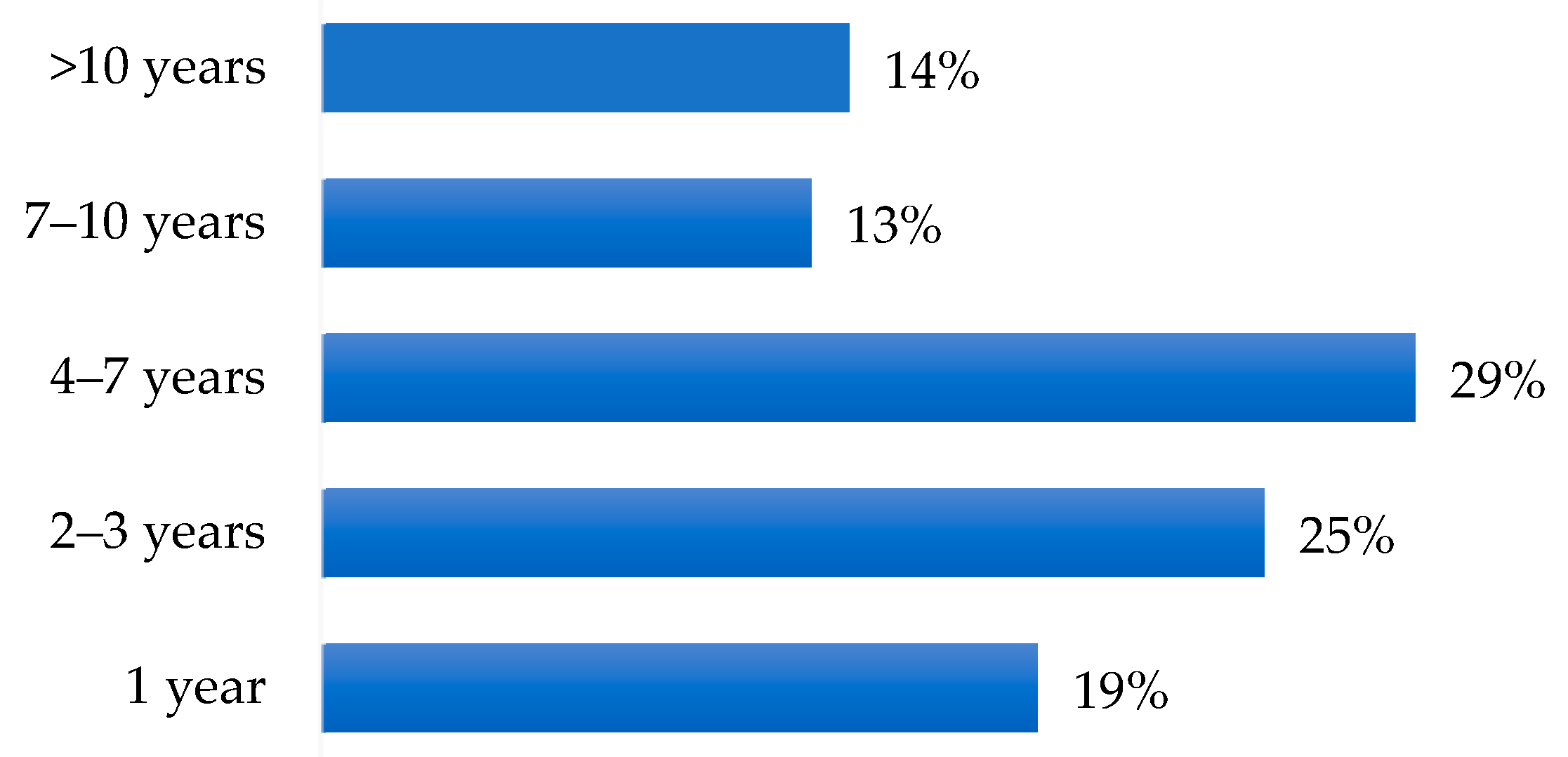
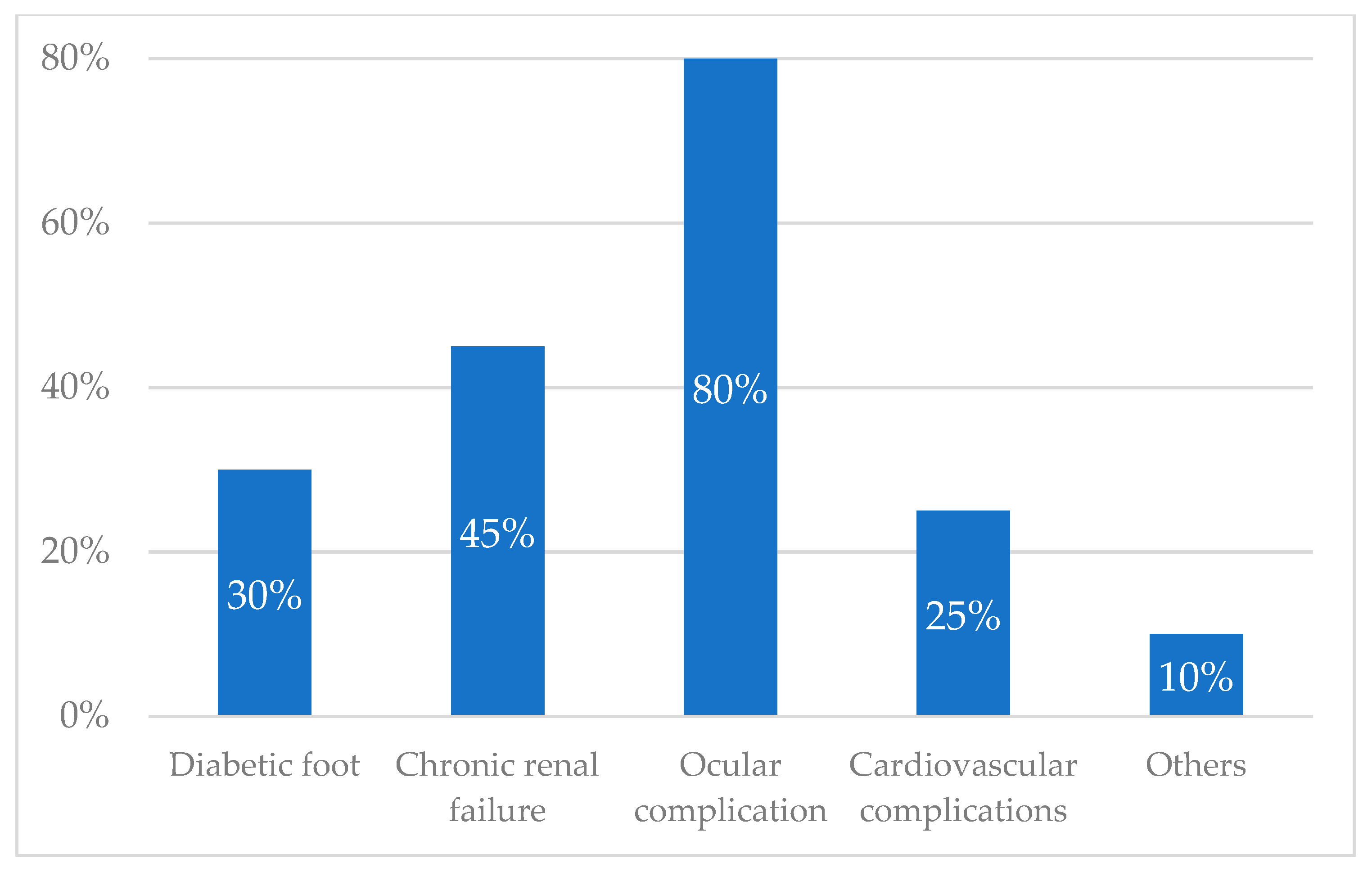
3.3. Diagnosis of Diabetes and Its DME Complication
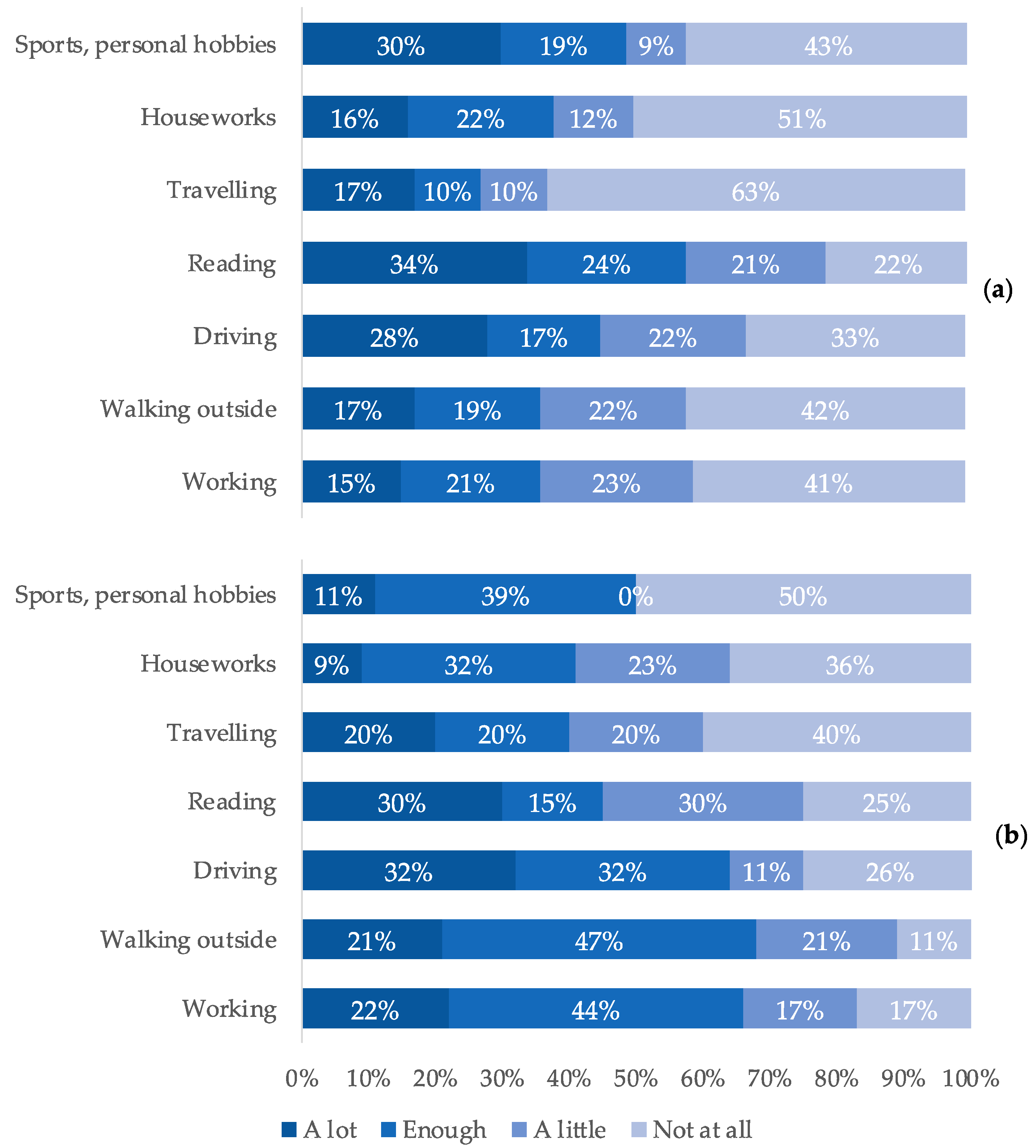
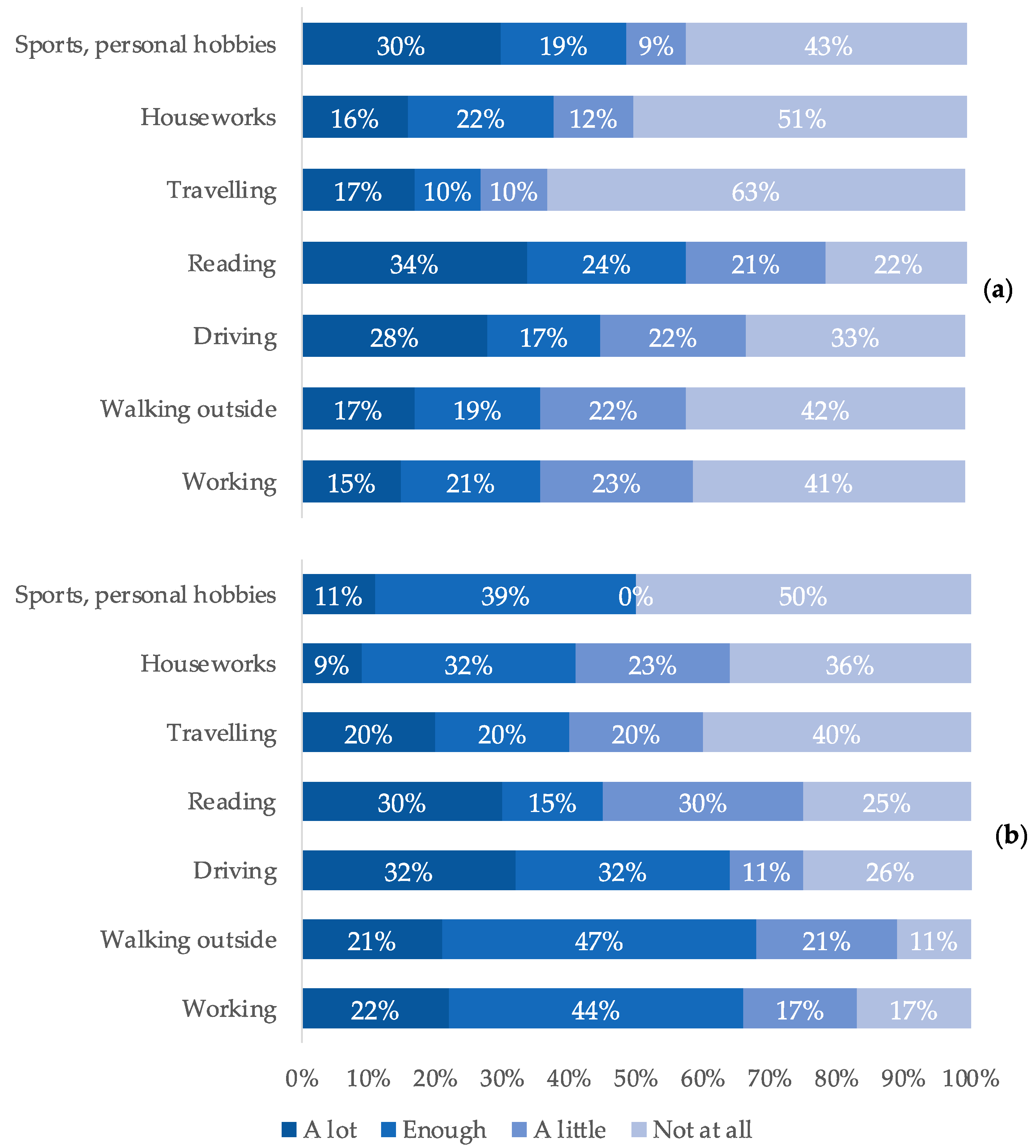
3.4. The Impact of DME on Daily Life
3.5. Treatment of Diabetes and Its Eye Complication
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health Estimates 2019: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2019. World Health Organization. 2020. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 10 June 2022).
- National Institute of Statistics. Italian Statistical Yearbook 2020. National Institute of Statistics. 2020. Available online: http://dati.istat.it/Index.aspx (accessed on 10 June 2022).
- Midena, E.; Frizziero, L.; Midena, G.; Pilotto, E. Intraocular fluid biomarkers (liquid biopsy) in human diabetic retinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 3549–3560. [Google Scholar] [CrossRef] [PubMed]
- Porta, M.; Tomalino, M.G.; Santoro, F.; Ghigo, L.D.; Cairo, M.; Aimone, M.; Pietragalla, G.B.; Passera, P.; Montanaro, M.; Molinatti, G.M. Diabetic retinopathy as a cause of blindness in the province of Turin, north-west Italy, in 1967–1991. Diabet. Med. 1995, 12, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zeng, H.; Bao, S.; Wang, N.; Gillies, M.C. Diabetic macular edema: New concepts in patho-physiology and treatment. Cell Biosci. 2014, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barham, R.; El Rami, H.; Sun, J.K.; Silva, P.S. Evidence-Based Treatment of Diabetic Macular Edema. Semin. Ophthalmol. 2017, 32, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Lally, D.R.; Shah, C.P.; Heier, J.S. Vascular endothelial growth factor and diabetic macular edema. Surv. Ophthalmol. 2016, 61, 759–768. [Google Scholar] [CrossRef]
- Marini, M.G.; Reale, L.; Cappuccio, A.; Spizzichino, M.; Zini, P.; Amato, F.; Mameli, S.; Raffaeli, W. Narrative medicine to highlight values of Italian pain therapists in a changing healthcare system. Pain Manag. 2014, 4, 351–362. [Google Scholar] [CrossRef]
- Midena, E.; Varano, M.; Pilotto, E.; Staurenghi, G.; Camparini, M.; Pece, A.; Battaglia Parodi, M.; Vadalà, M.; Donati, S.; Frizziero, L.; et al. Real-life patient journey in neovascular age-related macular degeneration: A narrative medicine analysis in the Italian setting. Eye 2022, 36, 182–192. [Google Scholar] [CrossRef]
- Davies, E.L.; Pollock, D.; Graham, A.; Laing, R.E.; Langton, V.; Bulto, L.; Kelly, J. Reporting of patient journey mapping in current literature: A scoping review protocol. JBI Evid. Synth. 2021, 20, 1361–1368. [Google Scholar] [CrossRef]
- Fioretti, C.; Mazzocco, K.; Riva, S.; Oliveri, S.; Masiero, M.; Pravettoni, G. Research studies on patients’ illness experience using the Narrative Medicine approach: A systematic review. BMJ Open 2016, 6, e011220. [Google Scholar] [CrossRef]
- Chapman, A.L.; Hadfield, M.; Chapman, C.J. Qualitative research in healthcare: An introduction to grounded theory using thematic analysis. J. R Coll. Physicians Edinb. 2015, 45, 201–205. [Google Scholar] [CrossRef]
- QSR International. Available online: https://www.qsrinternational.com (accessed on 19 June 2022).
- Frizziero, L.; Calciati, A.; Midena, G.; Torresin, T.; Parrozzani, R.; Pilotto, E.; Midena, E. Subthreshold Micropulse Laser Modulates Retinal Neuroinflammatory Biomarkers in Diabetic Macular Edema. J. Clin. Med. 2021, 10, 3134. [Google Scholar] [CrossRef]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rothschild, P.R.; Omri, S.; Gélizé, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef]
- Eramudugolla, R.; Wood, J.; Anstey, K.J. Co-morbidity of depression and anxiety in common age-related eye diseases: A population-based study of 662 adults. Front. Aging Neurosci. 2013, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Ulhaq, Z.S.; Soraya, G.V.; Dewi, N.A.; Wulandari, L.R. The prevalence of anxiety symptoms and disorders among ophthalmic disease patients. Ther. Adv. Ophthalmol. 2022, 14, 25158414221090100. [Google Scholar] [CrossRef]
- Association of Diabetologists and Italian Society of Diabetology. Standard Italiani per la Cura del Diabete Mellito 2016. AMD-SID. 2016. Available online: http://www.standarditaliani.it/home.php (accessed on 10 June 2022).
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef]
- Vujosevic, S.; Midena, E. Diabetic Retinopathy in Italy: Epidemiology Data and Telemedicine Screening Programs. J. Diabetes Res. 2016, 2016, 3627465. [Google Scholar] [CrossRef]
- Scanlon, P.H. Update on Screening for Sight-Threatening Diabetic Retinopathy. Ophthalmic Res. 2019, 62, 218–224. [Google Scholar] [CrossRef]
- Kashim, R.M.; Newton, P.; Ojo, O. Diabetic Retinopathy Screening: A Systematic Review on Patients’ Non-Attendance. Int. J. Environ. Res. Public Health 2018, 15, 157. [Google Scholar] [CrossRef] [Green Version]
- Manchaiah, V.K.; Stephens, D.; Meredith, R. The patient journey of adults with hearing impairment: The patients’ views. Clin. Otolaryngol. 2011, 36, 227–234. [Google Scholar] [CrossRef]
- Trebble, T.M.; Hansi, N.; Hydes, T.; Smith, M.A.; Baker, M. Process mapping the patient journey: An introduction. BMJ 2010, 341, c4078. [Google Scholar] [CrossRef]
- Salana, K.; Maty, S.; Hage, R. A Whole Other Story: Interpreting Narrative Medicine. Glob. Adv. Health Med. 2021, 10, 21649561211031880. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Participants | DME Patients N = 82 | Caregivers N = 24 |
|---|---|---|
| Male | 57% | 39% |
| Female | 43% | 61% |
| Age (years) | ||
| Average | 65 | 55 |
| Range | 30–82 | 22–80 |
| Type of diabetes | ||
| DM I | 17% | |
| DM II | 83% | |
| Duration of diabetes (years) | ||
| Mean | 19 | |
| Range | 0–58 | |
| <10 years 10–20 years >20 years | 24% 40% 36% | |
| Age at diagnosis of diabetes (years) | ||
| DM I | ||
| Average Range | 31 11–50 | |
| DM II | ||
| Average Range | 48 22–73 | |
| Marital status | ||
| Married | 88% | 75% |
| Unmarried | 12% | 25% |
| Instruction level | ||
| Obligatory education | 65% | 57% |
| Diploma/degree/master | 35% | 43% |
| Occupational status | ||
| Employed | 40% | 56% |
| Retired/unoccupied | 60% | 44% |
| Population of interviewees’ hometown (amount of people) | ||
| <25,000 | 40% | |
| 25,000–250,000 | 20% | |
| >250,000 | 40% | |
| Relationship | ||
| Partner | 42% | |
| Son/daughter | 39% | |
| Others | 19% | |
| DM: diabetes mellitus | ||
| Driving | “In everyday life I have problems driving at night: when I drive, I look fixed on the strips, otherwise I have the flash in my eyes“ “I think about the driving license, it expires on the 23rd and I am very worried, that is a thought unfortunately” “I’m just sorry that I had to abandon the car both for the problem that I do not see there and for the foot that I no longer have the reflex ready” “The only problem I have right now is that I have everything expiring. The driving license, the carrying of weapons and I must redo everything and with the problems that there are in Italy it becomes difficult. I’m 59 years old and if they take away my driving license, I’m in trouble” “Yes, I am sad because I am afraid of losing my autonomy, I do not want to depend on anyone. If I had to know that tomorrow, they take away my car (crying) because it’s like dying” |
| Reading | “Reading I struggle because closely I can’t, it’s a still image, I can’t adjust, focus” “Before I read a lot, the grandchildren gave me books to read the stories but now I can no longer read” |
| Walking | “I no longer feel safe walking, I stumble often, the doctor said it is a beginning of diabetic neuropathy” “I don’t have the confidence to walk quietly alone, balance, being able to visualize people’s faces. The biggest thing is that you can’t take two steps on your own” |
| Hobbies | “First I sewed with crochet, now not” “I used to play bowls and I don’t see the ball far away anymore” “The eye problem affects my day, I loved sewing, knitting, reading…now I struggle if there is a long word I struggle and so I go to the meaning of the sentence but maybe I understood in one way and instead there was written another thing, and everything changes. I can’t stick the needle even with the needle thread and then I get angry and cry there” |
| “Diabetologists and ophthalmologists do not know each other, I am the one who acts as an intermediary. It would be necessary that on the same day that you visit here, you could do an hour even with the diabetologist, it would be very important“ “Diabetologist and ophthalmologist do not dialogue, I had to report to the diabetologist, and he verifies everything. They are two worlds that do not talk to each other“ “Having a fixed point of reference would be appropriate. We are the means to make cardiology, diabetology, and ophthalmology talk to each other. We always bring the reports, for example, we brought to the diabetologist what we did with the cardiologist. Everyone looks at his specialty, there is no real coordination point, he updates the computer” “However, diabetologist and ophthalmologist do not talk to each other, nor does one ask about the other… they are a number for both. Perhaps the doctors have lost sight of the patient but not through his fault but because he is overloaded” “The problem is all a whole. Diabetes itself is not disabling but it is the problem that creates you” |
| Didn’t know | “I did not know the complications of diabetes, I realized it 5 years ago that I began to see badly, so I had a visit” “I did not know about the visual complication, they told me that diabetes brings complications on other organs, but I found out only after that I could get to this” “I didn’t know the complications of diabetes. For me, my only knowledge was not to eat sweets, stop” “When I was diagnosed with diabetes I did not know about the complications, I found out a few weeks later. Surely the one that scares me the most is not seeing us anymore“ “When I was diagnosed with diabetes, I didn’t know the complications, I discovered them as we went on, eye complications are the ones that scare me the most” |
| Underestimated | “I knew the complications of diabetes, but I honestly ignored the visual ones, I didn’t think they were so invasive” “I did not believe that diabetes could do all this damage to vision, to the eyes, … I am especially concerned about those” |
| Average km to reach the Diabetic Eye Clinic | 102 km |
| Average time taken to reach the Diabetic Eye Clinic | 50 min |
| Average monthly cost of reaching the Diabetic Eye Clinic | 34 euros |
| Average time taken to perform the ophthalmological evaluation at the hospital (including the travel) | 5.8 h |
| Economic burden | “This disease impacts economically: I take 860 euros from the government: total 860 euros and eye complication costs a lot to me, so it impacts” “Economically the management of diabetes and vision has affected economically, I manage everything privately. Fixing a visit and an OCT is impossible and therefore you are forced to this” |
| Distance to the diabetic eye clinic | “Not having nearby clinics, I must move here in the mayor diabetic clinic., the trips impact” “To come here I come by car and my son takes me” “To come here, most of the time I come by public transport: I have the bus under the house, then I take the train” “If I do not have to do the eye examination I come by car, it takes 30 min (20 min if I come by car)” “It’s 50 km each time to come here” |
| Time spent for the visits | “When I leave the house to when we leave here passes a long time, es Friday that they did not do the injections I arrived at 8 and I left here at noon and a half” “Today it was a bit longer, but I usually stay here two or two and a half hours” “It takes half a day for an examination that lasts 3 min. It is from one that I am here, now that I am out of here it will be 4 and a half. Now that you go to the acceptance that even if you arrive well in advance, however, you lose 3⁄4 of an hour, then go upstairs, you must wait for them to call you, make another line an hour and a half …“ |
| Difficulties in reservations | “For reservations I have a lot of difficulty because the waits are long” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Midena, E.; Polo, C.; Frizziero, L.; Marini, M.G.; Lattanzio, R.; Vadalà, M.; Pilotto, E.; Varano, M. The Narrative Medicine Approach in the Treatment of Diabetic Macular Edema: An Italian Experience. Int. J. Environ. Res. Public Health 2022, 19, 9367. https://doi.org/10.3390/ijerph19159367
Midena E, Polo C, Frizziero L, Marini MG, Lattanzio R, Vadalà M, Pilotto E, Varano M. The Narrative Medicine Approach in the Treatment of Diabetic Macular Edema: An Italian Experience. International Journal of Environmental Research and Public Health. 2022; 19(15):9367. https://doi.org/10.3390/ijerph19159367
Chicago/Turabian StyleMidena, Edoardo, Chiara Polo, Luisa Frizziero, Maria Giulia Marini, Rosangela Lattanzio, Maria Vadalà, Elisabetta Pilotto, and Monica Varano. 2022. "The Narrative Medicine Approach in the Treatment of Diabetic Macular Edema: An Italian Experience" International Journal of Environmental Research and Public Health 19, no. 15: 9367. https://doi.org/10.3390/ijerph19159367
APA StyleMidena, E., Polo, C., Frizziero, L., Marini, M. G., Lattanzio, R., Vadalà, M., Pilotto, E., & Varano, M. (2022). The Narrative Medicine Approach in the Treatment of Diabetic Macular Edema: An Italian Experience. International Journal of Environmental Research and Public Health, 19(15), 9367. https://doi.org/10.3390/ijerph19159367