1. Introduction
Mental health issues have become more prevalent among institutionalised adolescents compared to non-institutionalised adolescents over the years. Delinquency and mental health issues pose a substantial risk to public health comparable to other risks, such as non-communicable and infectious diseases, among institutionalised adolescents [
1]. In particular, adolescent institutionalisation within the juvenile justice system is of concern as mental disorders are found to be very common among juveniles [
2]. Worldwide, 70–100% of institutionalised adolescents had at least one mental disorder classified in the Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) [
3]. In Malaysia, 93% of detained juveniles experienced one or more diagnosable mental disorders, including anxiety and stress [
4]. According to the National Health and Morbidity Survey, 20% of institutionalised adolescents aged 10–17 years old suffered from depression, while 10% attempted suicide due to depression [
5]. It is found that institutionalisation had a negative impact on their mental wellbeing and personal protective skills, such as resilience. They tend to become more emotional and less resilient as a result of institutionalisation [
6]. Besides, institutionalisation also has a significant effect on the adolescents’ interpersonal and social developmental domains. They tend to have impaired cognitive development and are unable to form emotional attachment with their caregivers, which results in low social support received from family and friends [
7]. Moreover, institutionalised adolescents also have higher risk of developing low self-esteem due to emotional abuse [
8]. Due to all these mental health issues, institutionalised adolescents are unable to contribute to the community once they are released.
Despite the implementation of rehabilitative programmes in correctional institutions, the prevalence of mental health issues and recidivism is still rising among institutionalised adolescents [
9]. For instance, the cases of juvenile offence in Malaysia had increased by 10.5% from 4833 cases in 2019 to 5342 cases in 2020 [
10]. This creates a drive for the research of a more effective intervention programme to empower institutionalised adolescents so that they can reintegrate into the community after their release from custody. Cognitive behavioural therapy (CBT) based intervention, such as the Super Skills for Life (SSL) programme, may be an effective solution to this problem. The SSL programme is a targeted prevention programme with multi-component intervention strategies consisting of cognitive preparation, social skills and behavioural activation. It aims to cultivate socially competent adolescents by training them in social skills and by improving their mental wellbeing through the instillation of positive self-perceptions [
11]. Evidence has shown the effectiveness of the SSL programme intervention in improving adolescents’ mental wellbeing and personal protective skills, such as self-esteem and coping skills [
11,
12,
13,
14]. For example, the SSL intervention has shown improvements to the symptoms of generalised anxiety and social phobia among institutionalised youth [
12]. Furthermore, the self-esteem and coping skills of adolescents to deal with behavioural issues were also significantly improved after the SSL intervention [
11,
13,
14].
However, there has not been any study in Malaysia available to explore the effectiveness of the SSL programme among institutionalised adolescents in a more robust manner. Therefore, this study aims to evaluate the effectiveness of the SSL programme in improving the mental wellbeing of institutionalised adolescents in the aspects of mental health status (depression, anxiety and stress) and personal protective skills (resilience, perceived social support and self-esteem). Moreover, factors associated with the mental wellbeing of institutionalised adolescents are also identified so that they can be mitigated to help with the success of the programme.
2. Materials and Methods
2.1. Study Design
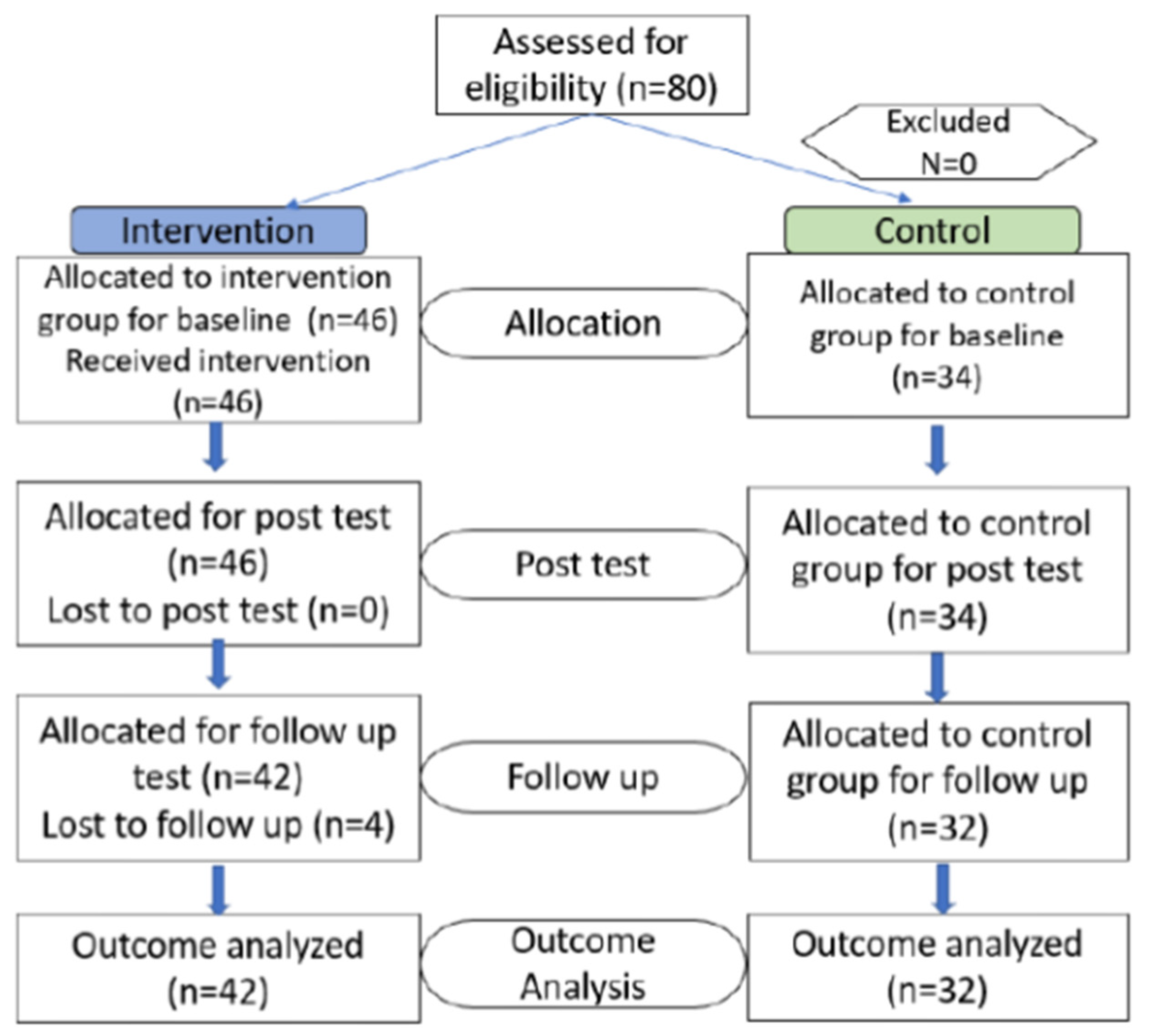
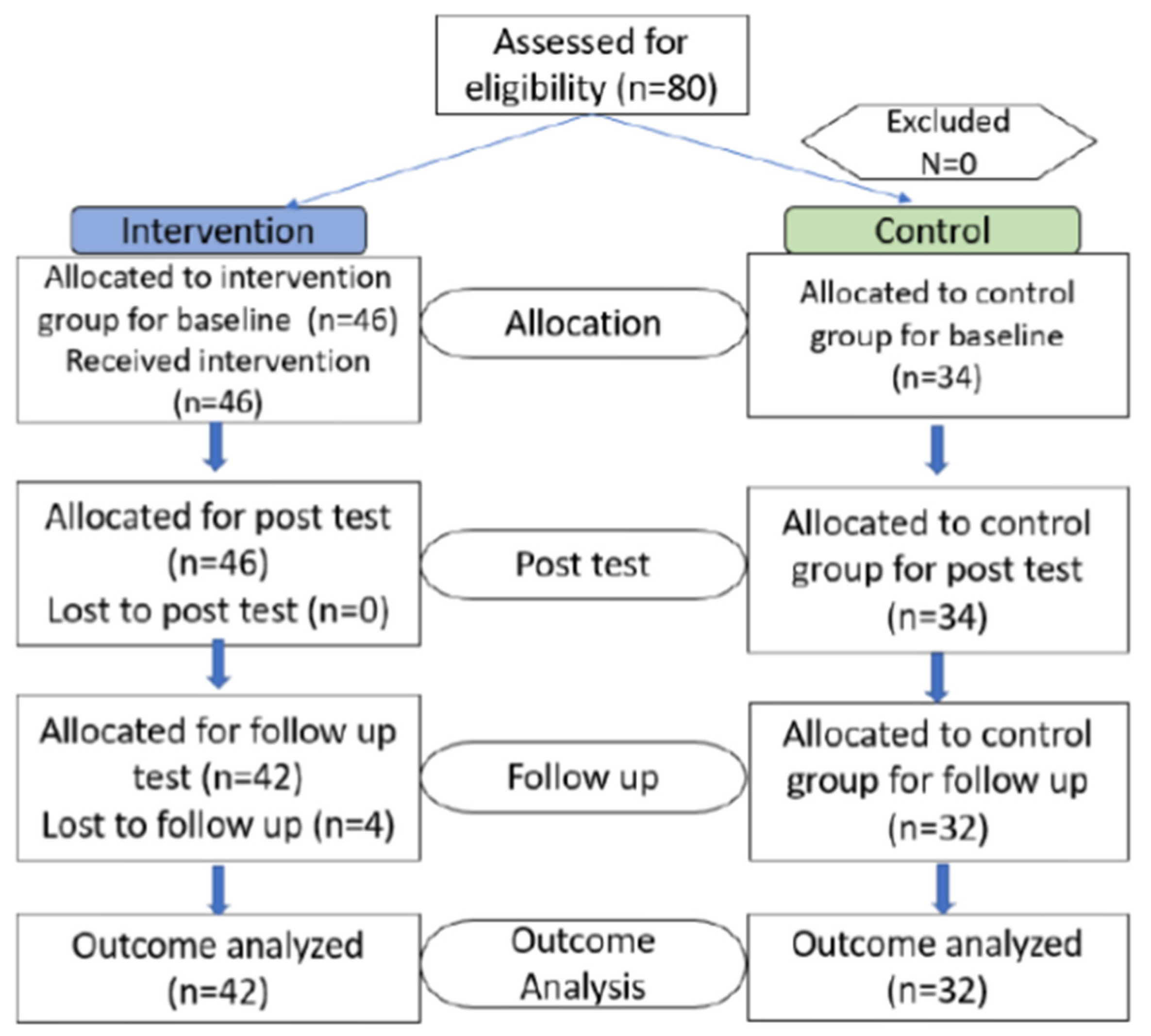
This is a quasi-experimental study, which consists of a cross-sectional study on all eligible institutionalised adolescents divided into intervention and control groups, measuring various parameters of their psychological wellbeing pre-intervention; implementation of the SSL programme for the intervention group; post-intervention survey to evaluate immediate changes in observed outcomes; and follow-up assessment after two months for the measurement of sustained immediate effects.
2.2. Study Population
The study population included female participants residing in correctional institutions located in Peninsular Malaysia. All participants were female as the welfare institutions within the sampling pool comprised of only female correctional institutions. This limited sampling pool was due to the implementation of Movement Control Order because of the COVID-19 crisis, in which many detention centres restricted the implementation of programmes by external agencies due to health and safety concerns.
2.3. Inclusion and Exclusion Criteria
Detained female participants who were aged 12–22 years old and were able to read and understand either English or Malay were included in the study. Female participants who were quarantined for disciplinary problems or health reasons or have cognitive abnormalities were excluded from the study.
2.4. Sample Size
The sample size included in the study was calculated based on a previous study by Amiri, Heshmati, and Shad 2010 that investigated depression, anxiety and stress parameters among orphanage residents [
15,
16]. After calculation, the maximum number selected as the final sample size was
n = 128 for both intervention and control groups.
2.5. Intervention Programme
Participants in the intervention group were arranged to participate in the SSL programme, whereas the control group would be excluded from the programme. The programme was implemented once a week over a period of two months. It was conducted by an experienced researcher, who had undergone intensive training by the author of the SSL programme, Professor Cecelia Essau, through a Training the Trainer (ToT) course organised in 2019 in Malaysia. The researcher was also appointed as a facilitator by the Malaysian Ministry of Youth and Sports to aid in the nationwide implementation of the SSL programme in secondary schools in 2019. The programme consisted of eight sessions, involving different activities as stated in
Table 1.
Prior to the SSL programme, participants were subjected to a pre-test in the form of a questionnaire available in both English and Malay where the participants could choose from. Upon completing the SSL session, participants were requested to complete another survey to evaluate the immediate and follow-up effects of the intervention. Participants in the control group were also requested to complete the same pre-test, post immediate and follow-up test in the form of a questionnaire to assess the outcome parameters.
2.6. Data Collection and Analysis
The study extended over a period of five months from October 2020 to February 2021. The study was conducted in three randomly selected correctional institutions located in Selangor, Malacca and Terengganu, Malaysia. Participants in the intervention and control groups were from two geographically distinct institutions, with the intervention group from correctional institutions in Selangor and Malacca, while the control group was from a correctional institution in Terengganu. This was to prevent knowledge transfer and contamination of intervention between the two groups. Socio-demographic information of the participants was obtained and tabulated according to the participation forms submitted by the participants.
The effectiveness of the SSL programme was assessed based on the outcome parameters, including mental health status (depression, anxiety, stress and mental wellbeing), resilience, perceived social support, self-esteem and coping skills, which were evaluated according to the different scales featured in the questionnaire. Two scales were used to measure mental health status among the participants, namely the Depression, Anxiety and Stress Scale-21 (DASS-21) and the Warwick-Edinburgh Mental Wellbeing (WEMWBS) (mental wellbeing). In brief, DASS-21 comprises three subscales with 7 items that measure each of the depression, anxiety, and stress outcome with a 4-point Likert scale, ranging from 0 (never) to 3 (mostly) based on what they had experienced over the past week. DASS-21 has a reported reliability scores of 0.95, 0.85 and 0.87, respectively, for Depression, Anxiety and Stress domains.
Additionally, measurement of mental health status was also achieved with the WEMWBS, a validated scale consisting of 14 items in the form of a 5-point Likert scale, ranging from 1 (none of the time) to 5 (all the time), covering both hedonic and eudaimonic aspects of mental health, including positive affect (feelings of optimism, cheerfulness, relaxation), satisfying interpersonal relationships and positive functioning (energy, clear thinking, self-acceptance, personal development, competence and autonomy). It displayed a high reliability with Cronbach alpha of 0.90.
Furthermore, several personal factors were measured using a Resilience Scale (resilience), Multidimensional Scale of Perceived Social Support (MSPSS) (perceived social support), Rosenberg Scale of Self-Esteem (RSES) (self-esteem) and Brief-COPE (coping skills). In particular, the Resilience Scale is made up of 25 items which can be rated on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree) on statements about resilience. It has been shown to have high validity and reliability in diverse settings with alpha coefficient measurements of an internal consistency reliability of between 0.87 and 0.95.
The MSPSS, on the other hand, comprises a total of 12 questions with 4 questions exploring each of the different sources of social support, namely family, friends and a significant other. Each item in MSPSS is measured with 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). It has displayed good internal consistency with Cronbach alpha value of 0.89.
For self-esteem measurement, RSES is a ten-item Likert scale with items answered on a four-point scale, from strongly agree to strongly disagree. With a Cronbach alpha value of 0.8, it uses a scale of 0–40 where a score less than 15 may indicate a problematic low self- esteem. Finally, Brief-COPE is an abbreviated version of the COPE (Coping Orientation to Problems Experienced) Inventory, a self-administered questionnaire developed to assess a broad range of coping responses. The instrument consists of 28 items that measure 14 factors of 2 items each, which correspond to a Likert scale ranging from 0 = I have not been doing this at all to 3 = I have been doing this a lot. This study used a translated and validated Malay version of the Brief COPE with a total Cronbach alpha value of 0.83.
Data obtained from the pre- and post-intervention and a 2 month follow-up assessment were analysed using the Statistical Package for Social Science (SPSS) desktop version 22.0 software (SPSS Inc., Chicago, IL, USA), focusing on intention to treat (ITT) calculations to evaluate the effectiveness of the SSL programme. The pre-post effect sizes were also calculated and compared. Pearson correlation analysis was used in inferential statistics to determine the contribution of each factor (socio-demographic and personal factors) and in predicting mental health status. Statistical difference was considered significant if the p-value was less than 0.05. Meanwhile, the mean difference of outcome parameters (depression, anxiety, stress, mental wellbeing, resilience, perceived social support, self-esteem and coping skills) between the intervention and control group for the three intervention phases (pre, post and 2 month follow-up) was assessed using a Bonferroni test. Assumptions including normality, homogeneity of variance and co-variance were verified before running the test. The effect size was also measured using partial eta squared, whereby 0.01 was considered small effect size, 0.06 was considered moderate effect size while 0.14 was considered large effect size.
2.7. Ethical Considerations
Ethics approval was obtained from the University of Malaya Research Ethics Committee (UMREC) with a reference number of TNC2/UMREC–817 prior to the commencement of the study. Written consent was obtained from all participants. For participants aged 18 and below, an additional informed consent was obtained from their respective legal guardians. The study was conducted in full compliance with the laws and regulations of the Malaysia Data Protection Act 1998. All information pertaining to participants’ mental wellbeing were kept confidential. Disclosure of any personal issues was dealt with confidentiality.
4. Discussion
The current study evaluates the effectiveness of the SSL programme in improving the mental wellbeing of institutionalised adolescents in terms of mental health status (depression, anxiety and stress) and personal protective skills (resilience, perceived social support and self-esteem). Considering the risk of knowledge transfer and contamination, the study population for this study was derived from different institutions for each of the experimental groups. However, homogeneity of the baseline characteristics among the participants could not be established when there were significant differences on the results of the socio-demographic profile of the participants in terms of age, number of siblings, child order number in family, number of family members in one household, parents’ marital status and incarceration duration found.
In terms of outcome measure parameters, the variation observed with the socio-demographic characteristics were not apparent with participants’ mental health status of interest (depression, anxiety and stress, resilience, perceived social support and self-esteem). Nevertheless, study results before the intervention showed that over 70% of them experienced some forms of mental health issues of varying degrees of seriousness (
Table 3). This finding corresponds with a previous systematic review encompassing 47 studies from 19 countries involving 28,033 male and 4754 female adolescents from juvenile correctional institutions. The research reported about 76.5% of female adolescents suffered from mental disorders, such as major depression and attention-deficit/hyperactivity disorder (ADHD) [
1].
In addition, a total of 57.5% reported low scores in resilience before the intervention, while in contrast, a total of 66.3% of participants reported high scores in perceived social support prior to the intervention programme (
Table 3). According to a study, it was found that female adolescents who were institutionalised due to delinquent behaviour developed pseudo-family relationships among themselves, where they often shared their feelings and belongings, thus forging a sense of camaraderie. Additionally, perceived social support in a closed community would need a collective behavioural change among a sizeable group of participants in order to generate an organic sustained perceived peer support. This would take practice and time before such genuine feelings of peer support were formed and felt [
17]. This would explain how and where participants in this study received social support in the institution setting. However, there is no significant difference between two institutions in terms of mental health status. Besides, significant difference among social support between the two groups may be meaningless as the mean social support demonstrated by all the participants were considered in the range of high perceived social support.
Furthermore, the heterogeneity of the baseline characteristics of the participants motivates the correlation analysis between the socio-demographic characteristics and the outcome measured at baseline. The results showed that age was negatively correlated with depression (
Table 4), which indicated that younger adolescents were more likely to experience depression compared to older adolescents. This finding contradicts a previous study, which reported that the estimated prevalence of depression among adolescents significantly increased with age, from 4% at age 13 to 19% at age 16 [
18]. However, the targeted subjects of the study were adolescents who were not institutionalised. This current study, on the other hand, targeted institutionalised adolescents. Thus, the difference in findings may be due to the difference in circumstances of targeted subjects.
Next, the number of family members in one household was found to be correlated with depression, anxiety, perceived social support and self-esteem. Increasing number of residents in one household was found to have significantly increased the level of depression and anxiety as well as lowering the self-esteem of the participants. Although the study has not shown the association of the number of family members with depression, anxiety and self-esteem, family discord was identified to be one of the contributing factors for the occurrence of depression and anxiety among adolescents [
19]. So, it is possible that increasing number of family members may invoke unpleasant competition among the children for the parents’ approval. In addition, larger families may have a difficulty with supporting their children due to limited resources, which then may lower the self-esteem and cause depression and anxiety in the children [
20]. Nonetheless, its positive correlation with perceived social support is reasonable and desirable as this will be helpful for the participants to cope with their circumstances in confinement.
As for personal protective factors, low perceived social support and self-esteem were significantly correlated with depression, anxiety and stress. This finding corresponds with a previous study, which reported low self-esteem to be ranked as a modestly specific and highly feasible risk factor, while lack of social support was ranked as a modestly feasible risk factor for mental health issues in adolescents, such as depression, anxiety and stress [
21]. Although the socio-demographic factors, such as age and number of family members, are difficult to manipulate, it is possible to improve the mental wellbeing of institutionalised adolescents by improving personal factors, such as perceived social support and self-esteem. This is possible through the intervention of the SSL programme.
Due to the heterogeneity of the participants, it is important to consider the confounding factors that may affect the analysis of the results. Significant improvement was observed for anxiety levels among the participants after the SSL intervention (
Table 5). Similar findings are also noted in a study conducted among the Spanish youth who were at risk of developing anxiety disorders. The study reported a significant drop in symptoms of generalised anxiety and social phobia among the youth after the SSL intervention [
12].
Next, stress emerged as another outcome that is positively impacted by SSL intervention among all three types of mental health status (
Table 5). Apart from the acute characteristic of stress, another possible reason could be that the participants had understood and practiced the stress-relieving techniques that were taught during the sessions in SSL programme. Besides, they had even adopted a positive outlook towards their circumstances, which is the intended purpose of the SSL intervention.
Meanwhile, the level of depression showed some positive changes as compared with anxiety and stress, albeit insignificant when interaction of both time and intervention were considered (
Table 5). This is probably due to the nature of depression, which requires more in-depth and targeted intervention, or even a combination of psychotherapy and pharmacotherapy [
22]. Nonetheless, this finding contradicts with those of another study, which showed significant improvement in the symptoms of depression among children and adolescents aged 9–14 from the SSL intervention group [
23].
When considered collectively, the mental wellbeing of participants showed a significant improvement as their incarceration duration progressed (
Table 5). However, the effect of SSL on mental wellbeing could not be established when considering both time and intervention effect.
As mentioned earlier, perceived social support and self-esteem were correlated with mental health status of the participants (
Table 4). This means that the improvement in perceived social support and self-esteem will reduce depression, anxiety and stress of the participants, which in turn will improve their mental wellbeing. As shown in the study results, improvements observed in depression, anxiety, stress, perceived social support and self-esteem did lead to better mental wellbeing among participants in the intervention group (
Table 5). Since the majority of the participants were already institutionalised for more than six months before the commencement of the intervention, such drastic improvement of mental wellbeing (anxiety and stress) after the relatively short 2 month intervention was mainly attributed to the SSL programme.
On the other hand, the level of perceived social support recorded significant improvement in the SSL intervention group compared to the control group. However, this may be due to the differences observed in the perceived social support during pre-intervention phase instead of an effect produced by the SSL. When interaction between time and intervention was analysed, no significant difference could be established. Nevertheless, the level of the perceived social support in both groups are already considered high and might not be a clinically significant choice.
Similarly, significant improvement was observed in the self-esteem of the participants from intervention groups following enrolment in the SSL programme (
Table 5). This finding corresponds with a study conducted among school children, which showed significant improvement in self-esteem after the SSL intervention [
14]. However, this difference might be influenced by the different baseline characteristics of the participants from different institutions.
A similar improvement was also observed in coping skills among the participants after the SSL intervention (
Table 5). The result was again in-line with those reported in previous studies, which showed that the coping abilities of juveniles to deal with their behavioural issues were greatly improved in both short- and long-term ways following the SSL intervention [
11,
23]. Similarly, this difference might be influenced by the different baseline characteristics of the participants at pre-intervention as no significant improvement of coping skills was observed when investigating the effect of time.
Finally, the SSL intervention was found not to change the level of resilience in this study (
Table 6). According to
Table 7, there was no interaction between time intervention and age, number of siblings, number of family members, parents’ marital status, incarceration duration, social support and self-esteem in the level of anxiety. Similarly, there were also no interactions found between time intervention and age, number of siblings, number of family members, parents’ marital status, incarceration duration, social support and self-esteem in the level of stress.
Overall, the institutionalised adolescents enrolled in the SSL programme from the intervention group reported sustained positive mental wellbeing as compared to those from the control group who demonstrated a more stagnant and insignificant improvement in their mental wellbeing (
Table 5). This finding is consistent with a previous study conducted among school children. Similar findings, such as improvements in mood, self-esteem and a reduction in psychological discomfort, were observed among adolescents after the SSL intervention [
13]. This is because the programme was designed to build emotional resilience among youth, while at the same time increasing their ability to deal with stressful life events, especially drastic life changes [
24].
Besides, several previous studies also showed the effectiveness of the SSL programme in lowering the symptoms of depression and anxiety, while increasing the efficiency to manage short- and long-term behavioural issues among juveniles [
11,
14]. This is evident in the present study, in which there was a significant improvement in anxiety and stress (
Table 5). This indicates the effectiveness of the SSL programme, whereby the knowledge and skills transferred to the participants were well received, practiced and normalised in their daily life, which then resulted in behavioural changes.
One of the limitations is the study design. This quasi-experimental study design may increase the possibility of selection bias, which may then affect the study outcome. Therefore, instead of a quasi-experimental study design, a randomised controlled study design is recommended to eliminate possible selection bias through the randomisation of participants.
Another limitation is the small sampling parameter that includes only a specific group of participants, which is made up of only Malay female adolescents. This limitation prevents analysis based on gender and ethnicity. Thus, the results of this study does not represent a generalised picture on the mental wellbeing of adolescents in all detention centres in Malaysia. Hence, the sampling frame should be extended in future research to include both male and female participants from all major ethnicities for a better representation of adolescents’ mental wellbeing.





{kind=link}