
Effects of Acute Aquatic High-Intensity Intermittent Exercise on Blood Pressure and Arterial Stiffness in Postmenopausal Women with Different ACE Genotypes


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
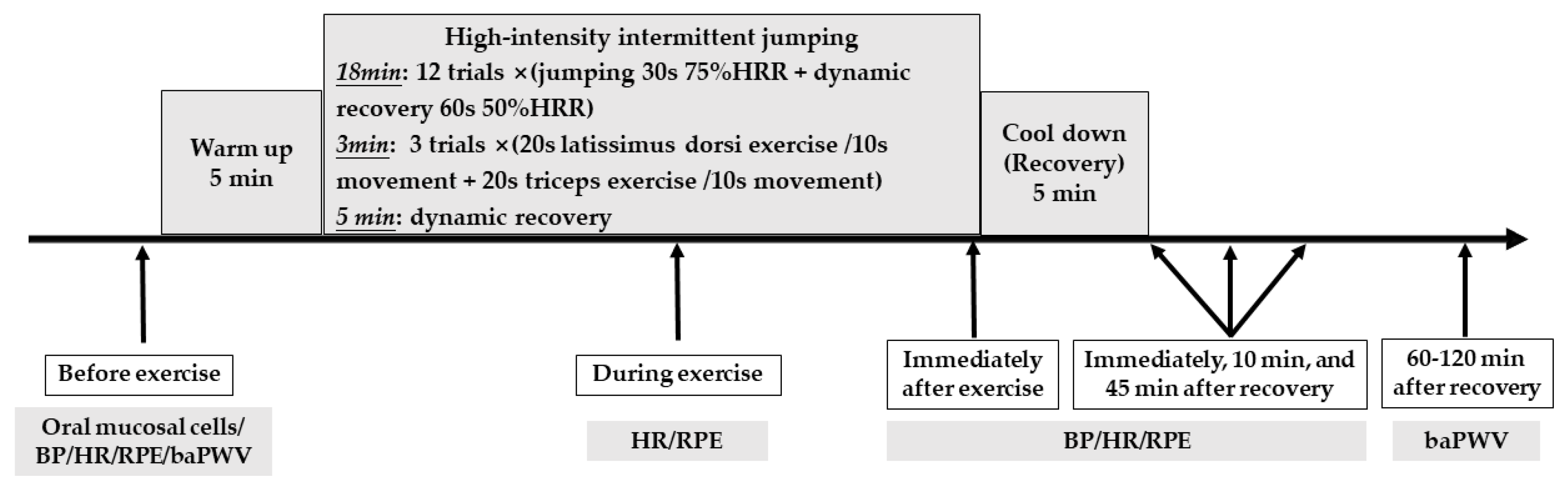
2.2. Study Procedures
2.3. Exercise Intervention
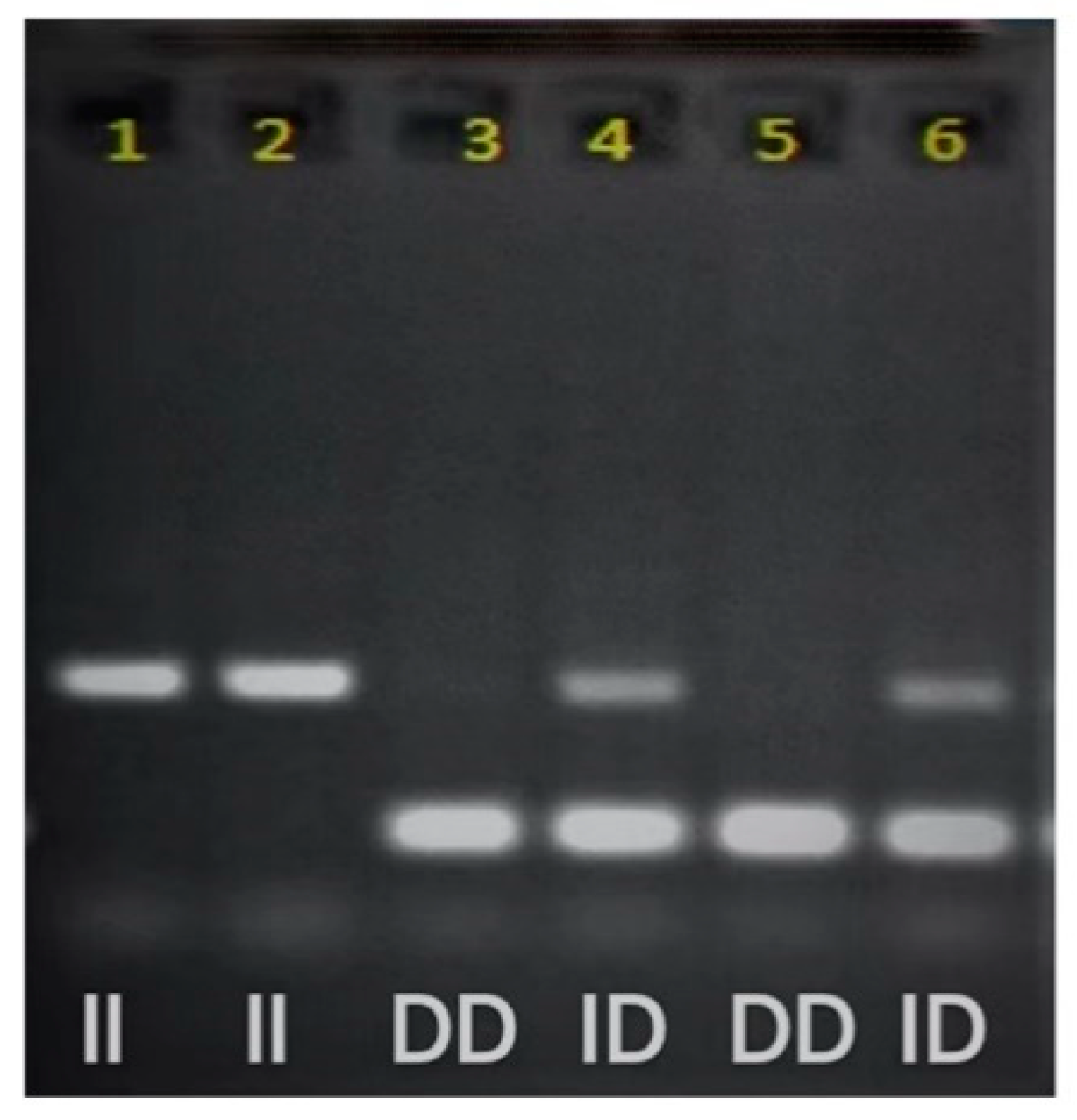
2.4. ACE Genotyping
2.5. Measures
2.5.1. Body Composition
2.5.2. Heart Rate
2.5.3. Blood Pressure
2.5.4. Brachial-Ankle Pulse Wave Velocity
2.6. Statistical Analysis
3. Results
3.1. Comparison of the Characteristics and Exercise Intensity for Different Genotypes
3.2. Comparison of BP for Different Genotypes during HIIJ Trial
3.3. Comparison of baPWV for Different Genotypes before and after Exercise and the Change of baPWV after the Exercise
4. Discussion
4.1. Comparison of Post-Exercise BP Response in Postmenopausal Women with Different Genotypes
4.2. Comparison of Post-Exercise baPWV in Postmenopausal Women with Different Genotypes
4.3. Comparison of Post-Exercise HR in Postmenopausal Women with Different Genotypes
4.4. Limitations
4.5. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [PubMed]
- Wang, D.; Zhou, Y.; Guo, Y.; Wang, C.; Wang, A.; Jin, Z.; Gao, X.; Wu, S.; Zhao, X.; Jonas, J.B. Arterial pre-hypertension and hypertension in intracranial versus extracranial cerebrovascular stenosis. Eur. J. Neurol. 2015, 22, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Bismar, H.; Diel, I.; Ziegler, R.; Pfeilschifter, J. Increased cytokine secretion by human bone marrow cells after menopause or discontinuation of estrogen replacement. J. Clin. Endocrinol. Metab. 1995, 80, 3351–3355. [Google Scholar]
- Carpenter, J.; Gass, M.L.S.; Maki, P.M.; Newton, K.M.; Pinkerton, J.V.; Taylor, M.; Utian, W.H.; Schnatz, P.F.; Kaunitz, A.M.; Shapiro, M. Nonhormonal management of menopause-associated vasomotor symptoms: 2015 Position Statement of The North American Menopause Society. Menopause 2015, 22, 1155–1174. [Google Scholar]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef]
- Heckman, G.A.; McKelvie, R.S. Cardiovascular Aging and exercise in healthy older adults. Clin. J. Sport Med. 2008, 18, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Mattace-Raso, F.U.; van der Cammen, T.J.; Hofman, A.; van Popele, N.M.; Bos, M.L.; Schalekamp, M.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.; Breteler, M.M. Arterial stiffness and risk of coronary heart disease and stroke: The Rotterdam study. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Safar, M.E.; London, G.M.; Plante, G.E. Arterial stiffness and kidney function. Hypertension 2004, 43, 163–168. [Google Scholar] [CrossRef]
- Ohkuma, T.; Ninomiya, T.; Tomiyama, H.; Kario, K.; Hoshide, S.; Kita, Y.; Inoguchi, T.; Maeda, Y.; Kohara, K.; Tabara, Y. Brachial-ankle pulse wave velocity and the risk prediction of cardiovascular disease: An individual participant data meta-analysis. Hypertension 2017, 69, 1045–1052. [Google Scholar] [CrossRef]
- Halliwill, J.R. Mechanisms and clinical implications of post-exercise hypotension in humans. Exerc. Sport Sci. Rev. 2001, 29, 65–70. [Google Scholar]
- MacDonald, J.R. Potential Causes, Mechanisms, and implications of post exercise hypotension. J. Hum. Hypertens. 2002, 16, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Roh, S.Y.; Yoon, S. An 8-week aquatic exercise program is effective at improving gait stability of the elderly. J. Phys. Ther. Sci. 2013, 25, 1467–1470. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cole, A.J.; Eagleston, R.E.; Moschetti, M.; Sinnett, E. Spine pain: Aquatic rehabilitation strategies. J. Back Musculoskelet Rehabil. 1994, 4, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.; Hillman, M.; Bulstrode, S. Loading of the lower limb when walking partially immersed: Implications for clinical practice. Physiotherapy 1992, 78, 164–166. [Google Scholar] [CrossRef]
- Forwood, M.R.; Larsen, J.A. Exercise recommendations for osteoporosis. A Position Statement of the Australian and New Zealand Bone and Mineral Society. Aust. Fam. Physician 2000, 29, 761–764. [Google Scholar]
- Cunha, R.M.; Costa, A.M.; Silva, C.N.F.; Póvoa, T.I.R.; Pescatello, L.S.; Lehnen, A.M. Postexercise hypotension after aquatic exercise in older women with hypertension: A randomized crossover clinical trial. Am. J. Hypertens. 2018, 31, 247–252. [Google Scholar] [CrossRef]
- Lai, B.; Jeng, B.; Vrongistinos, K.; Jung, T. Post-exercise hypotensive responses following an acute bout of aquatic and overground treadmill walking in people post-stroke: A pilot study. Top. Stroke Rehabil. 2015, 22, 231–238. [Google Scholar] [CrossRef]
- Rodriguez, D.; Prestes, J.; Rica, R.; Serra, A.J.; Bocalini, D.; Pontes Junior, F.L.; Silva, V. Hypotensive response after water-walking and land-walking exercise sessions in healthy trained and untrained women. Int. J. Gen. Med. 2011, 4, 549–554. [Google Scholar]
- Fagard, R.H.; Cornelissen, V.A. Effect of exercise on blood pressure control in hypertensive patients. Eur. J. Cardiol. Prev. Rehabil. 2007, 14, 12–17. [Google Scholar] [CrossRef]
- Kenney, M.J.; Seals, D.R. Postexercise hypotension. key features, mechanisms, and clinical significance. Hypertension 1993, 22, 653–664. [Google Scholar] [CrossRef]
- Whelton, S.P.; Chin, A.; Xin, X.; He, J. Effect of aerobic exercise on blood pressure: A meta-analysis of randomized, controlled trials. Ann. Intern. Med. 2002, 136, 493. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, B.E.; Tsongalis, G.J.; Guidry, M.A.; LaBelle, L.A.; Poulin, M.; Taylor, A.L.; Maresh, C.M.; Devaney, J.; Thompson, P.D.; Pescatello, L.S. RAAS polymorphisms alter the acute blood pressure response to aerobic exercise among men with hypertension. Eur. J. Appl. Physiol. 2006, 97, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.; An, P.; Gagnon, J.; Leon, A.S.; Skinner, J.S.; Wilmore, J.H.; Bouchard, C.; Rao, D.C. Heritability of HR and BP response to exercise training in the HERITAGE Family Study. Med. Sci. Sports. Exerc. 2002, 34, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Castellon, R.; Hamdi, H.K. Demystifying the ace polymorphism: From genetics to biology. Curr. Pharm. Des. 2007, 13, 1191–1198. [Google Scholar] [CrossRef]
- Woods, D.R.; Humphries, S.E.; Montgomery, H.E. The ACE I/D polymorphism and human physical performance. Trends Endocrinol. Metab. 2000, 11, 416–420. [Google Scholar] [CrossRef]
- Cambien, F.; Poirier, O.; Lecerf, L.; Evans, A.; Cambou, J.-P.; Arveiler, D.; Luc, G.; Bard, J.-M.; Bara, L.; Ricard, S. Deletion polymorphism in the gene for angiotensin-converting enzyme is a potent risk factor for myocardial infarction. Nature 1992, 359, 641–644. [Google Scholar] [CrossRef]
- Danser, A.H.J.; Schalekamp, M.A.D.H.; Bax, W.A.; van den Brink, A.M.; Saxena, P.R.; Riegger, G.A.J.; Schunkert, H. Angiotensin-converting enzyme in the human heart: Effect of the deletion/insertion polymorphism. Circulation 1995, 92, 1387–1388. [Google Scholar] [CrossRef]
- Chen, S.P.; Hao, Q.K.; Yang, M.; Yue, J.R.; Cao, L.; Liu, G.J.; Zou, C.; Ding, X.; Pu, H.S.; Dong, B.R. Association between Angiotensin-converting enzyme insertion/deletion polymorphisms and frailty among Chinese older people. J. Am. Med. Dir. Assoc. 2015, 16, 438.e1–438.e6. [Google Scholar] [CrossRef]
- Chiu, L.L.; Chen, T.W.; Hsieh, S.S.; Hsieh, L.L. ACE I/D, ACTN3 R577X, PPARD T294C and PPARGC1A Gly482Ser polymorphisms and physical fitness in Taiwanese late adolescent girls. J. Physiol. Sci. 2012, 62, 115–121. [Google Scholar] [CrossRef]
- Woo, J.; Tang, N.L.; Leung, J.; Kwok, T. The Alu polymorphism of angiotensin I converting enzyme (ACE) and atherosclerosis, incident chronic diseases and mortality in an elderly Chinese population. J. Nutr. Health Aging 2012, 16, 262–268. [Google Scholar] [CrossRef]
- Harrap, S.B.; Tzourio, C.; Cambien, F.; Chapman, N.; Colman, S.; Leguennec, S.; MacMahon, S.; Neal, B.; Ohkubo, T.; Woodward, M.; et al. The ACE gene I/D polymorphism is not associated with the blood pressure and cardiovascular benefits of ACE inhibition. Hypertension 2003, 42, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Chuang, L.M.; Chiu, K.C.; Chiang, F.T.; Lee, K.C.; Wu, H.P.; Lin, B.J.; Tai, T.Y. Insertion/deletion polymorphism of the angiotensin I-converting enzyme gene in patients with hypertension, non-insulin-dependent diabetes mellitus, and coronary heart disease in Taiwan. Metabolism 1997, 46, 1211–1214. [Google Scholar] [CrossRef]
- Rigat, B.; Hubert, C.; Alhenc-Gelas, F.; Cambien, F.; Corvol, P.; Soubrier, F. An insertion/deletion polymorphism in the angiotensin i-converting enzyme gene accounting for half the variance of serum enzyme levels. J. Clin. Investig. 1990, 86, 1343–1346. [Google Scholar] [CrossRef] [PubMed]
- Goessler, K.F.; Cornelissen, V.A.; de Oliveira, E.M.; de F Mota, G.; Polito, M.D. ACE Polymorphisms and the acute response of blood pressure to a walk in medicated hypertensive patients. J. Renin-Angiotensin-Aldosterone Syst. 2015, 16, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Henskens, L.H.; Spiering, W.; Stoffers, H.E.; Soomers, F.L.; Vlietinck, R.F.; de Leeuw, P.W.; Kroon, A.A. Effects of ACE I/D and AT1R-A1166C polymorphisms on blood pressure in a healthy normotensive primary care population: First results of the hippocates study. J. Hypertens. 2003, 21, 81–86. [Google Scholar] [CrossRef][Green Version]
- O’Donnell, C.J.; Lindpaintner, K.; Larson, M.G.; Rao, V.S.; Ordovas, J.M.; Schaefer, E.J.; Myers, R.H.; Levy, D. Evidence for association and genetic linkage of the angiotensin-converting enzyme locus with hypertension and blood pressure in men but not women in the Framingham heart study. Circulation 1998, 97, 1766–1772. [Google Scholar] [CrossRef]
- Freire, I.V.; Machado, M.; Ribeiro, Í.J.; Hackney, A.C.; Barbosa, A.A.; Pereira, R. The D allele of angiotensin-converting enzyme gene is associated with greater hemodynamic response to resistance exercises. J. Renin-Angiotensin-Aldosterone Syst. 2015, 16, 1251–1259. [Google Scholar] [CrossRef]
- Santana, H.A.; Moreira, S.R.; Neto, W.B.; Silva, C.B.; Sales, M.M.; Oliveira, V.N.; Asano, R.Y.; Espíndola, F.S.; Nóbrega, O.T.; Campbell, C.S. The higher exercise intensity and the presence of allele i of ace gene elicit a higher post-exercise blood pressure reduction and nitric oxide release in elderly women: An experimental study. BMC Cardiovasc. Disord. 2011, 11, 71. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Jae, S.Y.; Echols, G.H.; Lepine, N.R.; Fernhall, B. Arterial stiffness and wave reflection following exercise in resistance-trained men. Med. Sci. Sports Exerc. 2007, 39, 842–848. [Google Scholar] [CrossRef]
- Müller, J.; Wilms, M.; Oberhoffer, R. Acute effects of submaximal endurance training on arterial stiffness in healthy middle- and long-distance runners. Am. J. Hypertens. 2015, 17, 371–374. [Google Scholar] [CrossRef]
- Perissiou, M.; Bailey, T.G.; Windsor, M.; Greaves, K.; Nam, M.C.Y.; Russell, F.D.; O’Donnell, J.; Magee, R.; Jha, P.; Schulze, K.; et al. Aortic and systemic arterial stiffness responses to acute exercise in patients with small abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, J.; Swaminathan, N.; Pereira, N.M.; Henderson, K.; Brodie, D.A. Acute changes in arterial stiffness following exercise in people with metabolic syndrome. Diabetes Metab. Syndr. 2017, 11, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, K.; Collier, S.; Kelly, E.; Jae, S.; Fernhall, B. Arterial stiffness and baroreflex sensitivity following bouts of aerobic and resistance exercise. Int. J. Sports Med. 2007, 28, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Perissiou, M.; Bailey, T.G.; Windsor, M.; Nam, M.C.Y.; Greaves, K.; Leicht, A.S.; Golledge, J.; Askew, C.D. Effects of exercise intensity and cardiorespiratory fitness on the acute response of arterial stiffness to exercise in older adults. Eur. J. Appl. Physiol. 2018, 118, 1673–1688. [Google Scholar] [CrossRef]
- Sosner, P.; Gayda, M.; Dupuy, O.; Garzon, M.; Lemasson, C.; Gremeaux, V.; Lalongé, J.; Gonzales, M.; Hayami, D.; Juneau, M.; et al. Ambulatory blood pressure reduction following high-intensity interval exercise performed in water or dryland condition. J. Am. Soc. Hypertens. 2016, 10, 420–428. [Google Scholar] [CrossRef]
- Viana, A.A.; Fernandes, B.; Alvarez, C.; Guimarães, G.V.; Ciolac, E.G. Prescribing high-intensity interval exercise by RPE in individuals with type 2 diabetes: Metabolic and hemodynamic responses. Appl. Physiol. Nutr. Metab. 2019, 44, 348–356. [Google Scholar] [CrossRef]
- Chewning, J.M.; Krist, P.S.; de Figueiredo, P.A.P. Monitoring your aquatic heart rate: Increasing accuracy with the kruel aquatic adaptation. Aquatic Exercise Association Research Council Project. 2011. Available online: https://aeawave.org/Articles-More/Research (accessed on 20 February 2022).
- Rigat, B.; Hubert, C.; Corvol, P.; Soubrier, R. PCR detection of the insertion/deletion polymorphism of the human angiotensin converting enzyme gene (DCP1) (Dipeptidyl Carboxypeptidase 1). Nucleic Acids Res. 1992, 20, 1433. [Google Scholar] [CrossRef]
- Williams, B.; Baschiera, F.; Lacy, P.S.; Botha, J.; Prescott, M.F.; Brunel, P. Blood pressure and plasma renin activity responses to different strategies to inhibit the renin-angiotensin-aldosterone system during exercise. J. Renin-Angiotensin-Aldosterone Syst. 2013, 14, 56–66. [Google Scholar] [CrossRef]
- Fornage, M.; Amos, C.I.; Kardia, S.; Sing, C.F.; Turner, S.T.; Boerwinkle, E. Variation in the region of the angiotensin-converting enzyme gene influences interindividual differences in blood pressure levels in young white males. Circulation 1998, 97, 1773–1779. [Google Scholar] [CrossRef][Green Version]
- Lind, L. Endothelium-dependent vasodilation in hypertension: A review. Blood Press. 2000, 9, 4–15. [Google Scholar] [CrossRef]
- Tanriverdi, H.; Evrengul, H.; Tanriverdi, S.; Turgut, S.; Akdag, B.; Kaftan, H.A.; Semiz, E. Improved endothelium dependent vasodilation in endurance athletes and its relation with ACE I/D polymorphism. Circ. J. 2005, 69, 1105–1110. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Asahina, M.; Asahina, M.K.; Yamanaka, Y.; Mitsui, K.; Kitahara, A.; Murata, A. Cardiovascular response during aquatic exercise in patients with osteoarthritis. Am. J. Phys. Med. Rehabil. 2010, 89, 731–735. [Google Scholar] [CrossRef]
- Friedl, W.; Krempler, F.; Sandhofer, F.; Paulweber, B. Insertion/Deletion Polymorphism in the angiotensin-converting-enzyme gene and blood pressure during ergometry in normal males. Clin. Genet. 2008, 50, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, C.G., Jr.; Gomides, R.S.; Queiroz, A.C.C.; Pinto, L.G.; da Lobo, F.S.; Tinucci, T.; Mion, D., Jr.; de Forjaz, C.L.M. Acute and chronic effects of aerobic and resistance exercise on ambulatory blood pressure. Clinics 2010, 65, 317–325. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Franklin, B.A.; Fagard, R.; Farquhar, W.B.; Kelley, G.A.; Ray, C.A. Exercise and hypertension. Med. Sci. Sports Exerc. 2004, 36, 533–553. [Google Scholar] [CrossRef] [PubMed]
- Dengel, D. Role of angiotensin converting enzyme genotype in sodium sensitivity in older hypertensives. Am. J. Hypertens. 2001, 14, 1178–1184. [Google Scholar] [CrossRef][Green Version]
- Kaufmann, H.; Norcliffe-Kaufmann, L.; Palma, J.-A. Baroreflex dysfunction. N. Engl. J. Med. 2020, 382, 163–178. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Kips, J.G.; Jacobs, D.R.; Brumback, L.; Duprez, D.A.; Kronmal, R.; Bluemke, D.A.; Townsend, R.R.; Vermeersch, S.; Segers, P. Arterial wave reflections and incident cardiovascular events and heart failure. J. Am. Coll. Cardiol. 2012, 60, 2170–2177. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial stiffness and cardiovascular events: The Framingham heart study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.M.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Yamato, Y.; Hasegawa, N.; Sato, K.; Hamaoka, T.; Ogoh, S.; Iemitsu, M. Acute effect of static stretching exercise on arterial stiffness in healthy young adults. Am. J. Phys. Med. Rehabil. 2016, 95, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Brandes, R.; Fleming, I.; Busse, R. Endothelial aging. Cardiovasc. Res. 2005, 66, 286–294. [Google Scholar] [CrossRef]
- Versari, D.; Daghini, E.; Virdis, A.; Ghiadoni, L.; Taddei, S. The ageing endothelium, cardiovascular risk and disease in man: Ageing and endothelium. Exp. Physiol. 2009, 94, 317–321. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Hashimoto, J. Mechanical factors in arterial aging. J. Am. Coll. Cardiol. 2007, 50, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Aquatic Exercise Association. Standards and Guidelines for Aquatic Fitness Programming; Aquatic Exercise Association: Nokomis, FL, USA, 2008. [Google Scholar]
- Darby, L.A.; Yaekle, B.C. Physiological responses during two types of exercise performed on land and in the water. J. Sports Med. Phys. Fitness 2000, 40, 303–311. [Google Scholar]
- Barbosa, T.M.; Garrido, M.F.; Bragada, J. Physiological adaptations to head-out aquatic exercises with different levels of body immersion. J. Strength Cond. Res. 2007, 21, 1255–1259. [Google Scholar]
- Epstein, M. Renal effects of head-out water immersion in humans: A 15-year update. Physiol. Rev. 1992, 72, 563–621. [Google Scholar] [CrossRef]
- Pendergast, D.R.; Lundgren, C.E.G. The underwater environment: Cardiopulmonary, thermal, and energetic demands. J. Appl. Physiol. 2009, 106, 276–283. [Google Scholar] [CrossRef]
- Al Haddad, H.; Laursen, P.B.; Chollet, D.; Lemaitre, F.; Ahmaidi, S.; Buchheit, M. Effect of cold or thermoneutral water immersion on post-exercise heart rate recovery and heart rate variability indices. Auton. Neurosci. 2010, 156, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Peiffer, J.J.; Abbiss, C.R.; Laursen, P.B. Effect of cold water immersion on postexercise parasympathetic reactivation. Am. J. Phys. Med. Rehabil. 2009, 296, H421–H427. [Google Scholar] [CrossRef] [PubMed]
- Colado, J.C.; Triplett, N.T.; Tella, V.; Saucedo, P.; Abellán, J. Effects of aquatic resistance training on health and fitness in postmenopausal women. Eur. J. Appl. Physiol. 2009, 106, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Ha, G.C.; Yoon, J.R.; Yoo, C.G.; Kang, S.J.; Ko, K.J. Effects of 12-week aquatic exercise on cardiorespiratory fitness, knee isokinetic function, and Western Ontario and McMaster University osteoarthritis index in patients with knee osteoarthritis women. J. Exerc. Rehabil. 2018, 14, 870–876. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ASCM’s Resource Manual for Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Dolbow, D.R.; Farley, R.S.; Kim, J.K.; Caputo, J.L. Oxygen consumption, heart rate, rating of perceived exertion, and systolic blood pressure with water treadmill walking. J. Aging Phys. Act. 2009, 16, 14–23. [Google Scholar] [CrossRef][Green Version]
- Chien, K.Y.; Chen, W.C.; Kan, N.W.; Hsu, M.C.; Lee, S.L. Responses of blood pressure and lactate levels to various aquatic exercise movements in postmenopausal women. J. Sports Med. Phys. Fitness 2015, 55, 1423–1430. [Google Scholar]



{kind=link}
{kind=link}
| DD Genotype (n = 12) | II/ID Genotype (n = 61) | p | |
|---|---|---|---|
| Age | 62.3 ± 1.45 | 62.2 ± 0.79 | 0.957 |
| Weight (kg) | 58.5 ± 2.23 | 57.2 ± 0.88 | 0.557 |
| BMI (kg/m2) | 23.5 ± 0.56 | 23.2 ± 0.34 | 0.728 |
| Body fat (%) | 32.6 ± 1.44 | 31.9 ± 0.71 | 0.663 |
| Skeletal muscle mass (kg) | 21.7 ± 0.77 | 20.8 ±0.29 | 0.692 |
| Regular exercise percentage (%) | 91.7 | 90.7 | 0.872 |
| Proportion of people suffering from HTN (%) | 16.7 | 19.7 | 0.809 |
| Prevalence of circulatory system diseases (%) | 16.7 | 9.8 | 0.489 |
| Prevalence of bone and joints diseases (%) | 25.0 | 13.1 | 0.293 |
| Prevalence of endocrine diseases (%) | 8.3 | 19.7 | 0.348 |
| Prevalence of digestive system diseases (%) | 16.7 | 14.8 | 0.866 |
| Prevalence of ear and eye diseases (%) | 25.0 | 23.0 | 0.878 |
| Prevalence of respiratory system diseases (%) | 8.3 | 1.6 | 0.194 |
| Prevalence of cancer (%) | 8.3 | 3.3 | 0.420 |
| DD Genotype (n = 12) | II/ID Genotype (n = 61) | p | |
|---|---|---|---|
| HR_SRL (bpm) | 77.1 ± 1.84 | 73.9 ± 1.21 | 0.268 |
| HR_SRW–SRL (bpm) | −9.6 ± 1.20 | −7.1 ± 0.53 | 0.046 |
| HR of aquatic jumping (bpm) | 133.5 ± 1.69 | 134.8 ± 0.86 | 0.535 |
| Intensity of aquatic jumping (%HRR) | 75.2 ± 1.63 | 74.6 ± 0.64 | 0.732 |
| RPE of aquatic jumping | 4.1 ± 0.33 | 4.1 ± 0.14 | 0.915 |
| HR of muscle resistance exercises (bpm) | 134.3 ± 3.26 | 131.4 ± 1.66 | 0.481 |
| Intensity of muscle resistance exercises (%HRR) | 75.7 ± 4.12 | 70.9 ± 1.56 | 0.234 |
| RPE of muscle resistance | 4.4 ± 0.44 | 4.4 ± 0.18 | 0.967 |
| Number of jumps (times) | 421.8 ± 24.92 | 419.4 ± 6.97 | 0.899 |
| Number of muscle resistance exercises (times) | 157.5 ± 8.02 | 155.1 ± 2.29 | 0.712 |
| DD Genotype (n = 12) | II/ID Genotype (n = 61) | p | ||
|---|---|---|---|---|
| SBP (mmHg) | Before exercise | 114.3 ± 3.52 | 118.7 ± 1.56 | 0.262 |
| Immediately after exercise | 144.7 ± 4.55 | 138.7 ± 2.04 | 0.236 | |
| Immediately after recovery | 122.6 ± 3.88 | 121.2 ± 1.73 | 0.736 | |
| 10 min after recovery | 113.4 ± 3.82 | 112.3 ± 1.69 | 0.795 | |
| 45 min after recovery | 109.0 ± 3.36 | 102.5 ± 1.49 | 0.343 | |
| Immediately after exercise-before exercise | 30.8 ± 4.48 | 20.4 ± 2.00 | 0.038 | |
| 10 min after recovery-before exercise | −0.7 ± 3.28 | −6.4 ± 1.45 | 0.117 | |
| 45 min after recovery-before exercise | −5.1 ± 3.26 | −13.2 ± 1.44 | 0.026 | |
| DBP (mmHg) | Before exercise | 70.0 ± 2.30 | 70.0 ± 1.02 | 0.977 |
| Immediately after exercise | 67.4 ± 2.65 | 67.8 ± 1.18 | 0.901 | |
| Immediately after recovery | 66.6 ± 2.13 | 66.8 ± 0.95 | 0.914 | |
| 10 min after recovery | 71.1 ± 2.50 | 70.8 ± 1.11 | 0.897 | |
| 45 min after recovery | 68.3 ± 2.09 | 66.7 ± 0.93 | 0.501 | |
| Immediately after exercise-before exercise | −2.6 ± 2.22 | −2.5 ± 0.99 | 0.937 | |
| 10 min after recovery-before exercise | 1.1 ± 1.50 | 0.8± 0.66 | 0.864 | |
| 45 min after recovery-before exercise | −1.8 ± 1.84 | −3.2 ± 0.81 | 0.466 | |
| MAP (mmHg) | Before exercise | 84.5 ± 3.20 | 86.3 ± 1.40 | 0.591 |
| Immediately after exercise | 93.1 ± 2.68 | 91.2 ± 1.32 | 0.558 | |
| Immediately after recovery | 85.0 ± 2.72 | 85.0 ± 1.22 | 0.973 | |
| 10 min after recovery | 85.0 ± 2.27 | 84.7 ± 1.39 | 0.921 | |
| 45 min after recovery | 81.4 ± 2.77 | 79.7 ± 1.16 | 0.564 | |
| Immediately after exercise-before exercise | 8.6 ± 1.89 | 4.8 ± 1.27 | 0.203 | |
| 10 min after recovery-before exercise | 0.4 ± 1.87 | −1.6 ± 0.82 | 0.325 | |
| 45 min after recovery-before exercise | −3.2 ± 2.42 | −6.6 ± 0.95 | 0.161 |
| DD Genotype (n = 12) | II/ID Genotype (n = 61) | All Participants (n = 73) | ||
|---|---|---|---|---|
| baPWV (cm/s) | Before exercise_R | 1477.7 ± 63.77 | 1436.1 ± 28.22 | 1442.1 ± 30.34 |
| After exercise_R | 1533.3 ± 68.74 # | 1461.5 ± 30.42 * | 1472.0 ± 33.09 * | |
| Before exercise_L | 1482.0 ± 63.92 | 1438.6 ± 28.29 | 1444.8 ± 29.54 | |
| After exercise_L | 1553.0 ± 66.51 | 1459.7 ± 29.43 # | 1473.4 ± 32.36 * | |
| Change_R | 55.7 ± 28.20 | 25.4 ± 12.48 | - | |
| Change_L | 71.0 ± 28.24 | 21.1 ± 12.50 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, W.-S.; Yang, A.-L.; Chen, C.-N.; Kan, N.-W.; Kuo, J.T.-H.; Chen, L.-H.; Chien, K.-Y. Effects of Acute Aquatic High-Intensity Intermittent Exercise on Blood Pressure and Arterial Stiffness in Postmenopausal Women with Different ACE Genotypes. Int. J. Environ. Res. Public Health 2022, 19, 8985. https://doi.org/10.3390/ijerph19158985
Zhou W-S, Yang A-L, Chen C-N, Kan N-W, Kuo JT-H, Chen L-H, Chien K-Y. Effects of Acute Aquatic High-Intensity Intermittent Exercise on Blood Pressure and Arterial Stiffness in Postmenopausal Women with Different ACE Genotypes. International Journal of Environmental Research and Public Health. 2022; 19(15):8985. https://doi.org/10.3390/ijerph19158985
Chicago/Turabian StyleZhou, Wen-Sheng, Ai-Lun Yang, Chiao-Nan Chen, Nai-Wen Kan, Joanna Ting-Hui Kuo, Lee-Hwa Chen, and Kuei-Yu Chien. 2022. "Effects of Acute Aquatic High-Intensity Intermittent Exercise on Blood Pressure and Arterial Stiffness in Postmenopausal Women with Different ACE Genotypes" International Journal of Environmental Research and Public Health 19, no. 15: 8985. https://doi.org/10.3390/ijerph19158985
APA StyleZhou, W.-S., Yang, A.-L., Chen, C.-N., Kan, N.-W., Kuo, J. T.-H., Chen, L.-H., & Chien, K.-Y. (2022). Effects of Acute Aquatic High-Intensity Intermittent Exercise on Blood Pressure and Arterial Stiffness in Postmenopausal Women with Different ACE Genotypes. International Journal of Environmental Research and Public Health, 19(15), 8985. https://doi.org/10.3390/ijerph19158985