
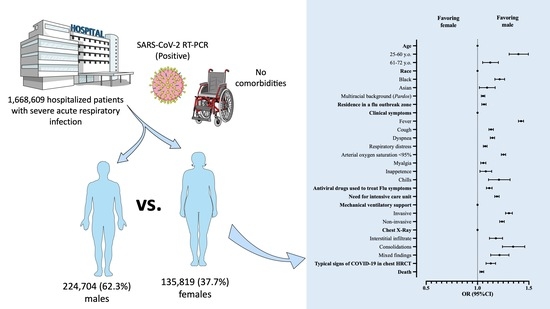
Characterization of Clinical Features of Hospitalized Patients Due to the SARS-CoV-2 Infection in the Absence of Comorbidities Regarding the Sex: An Epidemiological Study of the First Year of the Pandemic in Brazil


Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. General Aspects
4.2. Epidemiology
4.3. Genetic Aspects
4.4. Immune Aspects
4.5. Hormonal Aspects
4.6. Social and Environmental Factors
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of Sex and Gender on COVID-19 Outcomes in Europe. Biol. Sex. Differ. 2020, 11, 29. [Google Scholar] [CrossRef]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A Systematic Review and Meta-Analysis of Clinical Characteristics, Risk Factors, and Outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Viveiros, A.; Rasmuson, J.; Vu, J.; Mulvagh, S.L.; Yip, C.Y.Y.; Norris, C.M.; Oudit, G.Y. Sex Differences in COVID-19: Candidate Pathways, Genetics of ACE2, and Sex Hormones. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H296–H304. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex Differences in Immune Responses That Underlie COVID-19 Disease Outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef]
- Rettew, J.A.; Huet-Hudson, Y.M.; Marriott, I. Testosterone Reduces Macrophage Expression in the Mouse of Toll-like Receptor 4, a Trigger for Inflammation and Innate Immunity. Biol. Reprod. 2008, 78, 432–437. [Google Scholar] [CrossRef]
- Goren, A.; Vaño-Galván, S.; Wambier, C.G.; McCoy, J.; Gomez-Zubiaur, A.; Moreno-Arrones, O.M.; Shapiro, J.; Sinclair, R.D.; Gold, M.H.; Kovacevic, M.; et al. A Preliminary Observation: Male Pattern Hair Loss among Hospitalized COVID-19 Patients in Spain—A Potential Clue to the Role of Androgens in COVID-19 Severity. J. Cosmet. Dermatol. 2020, 19, 1545–1547. [Google Scholar] [CrossRef] [Green Version]
- de Jesus Soares, A.; Soares, C.F.; dos Santos Silva, F.C.; da Silva, A.F.; Estrela, F.M.; de Magalhães, J.R.; da Silva Oliveira, M.A.; Lima, A.M. Elementos da masculinidade que vulnerabilizam homens í morbimortalidade pela COVID-19: Revisão integrativa. Saúde Coletiva 2021, 11, 5926–5939. [Google Scholar] [CrossRef]
- Crimmins, E.M.; Shim, H.; Zhang, Y.S.; Kim, J.K. Differences between Men and Women in Mortality and the Health Dimensions of the Morbidity Process. Clin. Chem. 2019, 65, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Rogers, R.G.; Everett, B.G.; Onge, J.M.S.; Krueger, P.M. Social, Behavioral, and Biological Factors, and Sex Differences in Mortality. Demography 2010, 47, 555–578. [Google Scholar] [CrossRef]
- The Lancet. The Gendered Dimensions of COVID. Lancet 2020, 395, 1168. [Google Scholar] [CrossRef]
- Anderson, J.L.; Warren, C.A.; Perez, E.; Louis, R.I.; Phillips, S.; Wheeler, J.; Cole, M.; Misra, R. Gender and Ethnic Differences in Hand Hygiene Practices among College Students. Am. J. Infect. Control. 2008, 36, 361–368. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male Sex Identified by Global COVID-19 Meta-Analysis as a Risk Factor for Death and ITU Admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Haitao, T.; Vermunt, J.V.; Abeykoon, J.; Ghamrawi, R.; Gunaratne, M.; Jayachandran, M.; Narang, K.; Parashuram, S.; Suvakov, S.; Garovic, V.D. COVID-19 and Sex Differences: Mechanisms and Biomarkers. Mayo. Clin. Proc. 2020, 95, 2189–2203. [Google Scholar] [CrossRef]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Narang, K.; Enninga, E.A.L.; Gunaratne, M.D.S.K.; Ibirogba, E.R.; Trad, A.T.A.; Elrefaei, A.; Theiler, R.N.; Ruano, R.; Szymanski, L.M.; Chakraborty, R.; et al. SARS-CoV-2 Infection and COVID-19 During Pregnancy: A Multidisciplinary Review. Mayo. Clin. Proc. 2020, 95, 1750–1765. [Google Scholar] [CrossRef]
- Sawyer, C.C. Child Mortality Estimation: Estimating Sex Differences in Childhood Mortality since the 1970s. PLoS Med. 2012, 9, e1001287. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- Schröder, J.; Kahlke, V.; Staubach, K.H.; Zabel, P.; Stüber, F. Gender Differences in Human Sepsis. Arch. Surg. 1998, 133, 1200–1205. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.L.; Flanagan, K.L. Sex Differences in Immune Responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Jansen, A.; Chiew, M.; Konings, F.; Lee, C.-K.; Ailan, L. Sex Matters—A Preliminary Analysis of Middle East Respiratory Syndrome in the Republic of Korea. Western Pac. Surveill. Response J. 2015, 6, 68–71. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.H.; Tandi, T.E.; Choi, J.W.; Moon, J.M.; Kim, M.S. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Outbreak in South Korea, 2015: Epidemiology, Characteristics and Public Health Implications. J. Hosp. Infect. 2017, 95, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Noorwali, A.A.; Turkistani, A.M.; Asiri, S.I.; Trabulsi, F.A.; Alwafi, O.M.; Alzahrani, S.H.; Rashid, M.M.; Hegazy, S.A.; Alzaydi, M.D.; Bawakid, K.O. Descriptive Epidemiology and Characteristics of Confirmed Cases of Middle East Respiratory Syndrome Coronavirus Infection in the Makkah Region of Saudi Arabia, March to June. Ann. Saudi. Med. 2015, 35, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Abdelrahman, Z.; Li, M.; Wang, X. Comparative Review of SARS-CoV-2, SARS-CoV, MERS-CoV, and Influenza A Respiratory Viruses. Front. Immunol. 2020, 11, 552909. [Google Scholar] [CrossRef]
- Klein, S.L.; Hodgson, A.; Robinson, D.P. Mechanisms of Sex Disparities in Influenza Pathogenesis. J. Leukoc. Biol. 2012, 92, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, C.; Ferreira, P.M.; Masuda, E.T.; Lucas, P.C.d.C.; Palasio, R.G.S.; Nielsen, L.; Monteiro, P.d.C.M.; Trevisan, C.M.; Yu, A.L.F.; Carvalhanas, T.R.M.P. COVID-19 in the state of São Paulo: The evolution of a pandemic. Rev. Bras. Epidemiol. 2021, 24, e210040. [Google Scholar] [CrossRef]
- Johnson, H.D.; Sholcosky, D.; Gabello, K.; Ragni, R.; Ogonosky, N. Sex Differences in Public Restroom Handwashing Behavior Associated with Visual Behavior Prompts. Percept. Mot. Skills. 2003, 97, 805–810. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender Differences in the Utilization of Health Care Services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar]
- Pivonello, R.; Auriemma, R.S.; Pivonello, C.; Isidori, A.M.; Corona, G.; Colao, A.; Millar, R.P. Sex Disparities in COVID-19 Severity and Outcome: Are Men Weaker or Women Stronger? Neuroendocrinology 2021, 111, 1066–1085. [Google Scholar] [CrossRef]
- Vahidy, F.S.; Pan, A.P.; Ahnstedt, H.; Munshi, Y.; Choi, H.A.; Tiruneh, Y.; Nasir, K.; Kash, B.A.; Andrieni, J.D.; McCullough, L.D. Sex Differences in Susceptibility, Severity, and Outcomes of Coronavirus Disease 2019: Cross-Sectional Analysis from a Diverse US Metropolitan Area. PLoS ONE 2021, 16, e0245556. [Google Scholar] [CrossRef]
- de Souza, W.M.; Buss, L.F.; Candido, D.d.S.; Carrera, J.-P.; Li, S.; Zarebski, A.E.; Pereira, R.H.M.; Prete, C.A.; de Souza-Santos, A.A.; Parag, K.V.; et al. Epidemiological and Clinical Characteristics of the COVID-19 Epidemic in Brazil. Nat. Hum. Behav. 2020, 4, 856–865. [Google Scholar] [CrossRef]
- Zeiser, F.A.; Donida, B.; da Costa, C.A.; Ramos, G.d.O.; Scherer, J.N.; Barcellos, N.T.; Alegretti, A.P.; Ikeda, M.L.R.; Müller, A.P.W.C.; Bohn, H.C.; et al. First and Second COVID-19 Waves in Brazil: A Cross-Sectional Study of Patients’ Characteristics Related to Hospitalization and in-Hospital Mortality. Lancet Reg. Health 2022, 6, 100107. [Google Scholar] [CrossRef]
- He, W.; Liu, X.; Hu, B.; Li, D.; Chen, L.; Li, Y.; Zhu, K.; Tu, Y.; Xiong, S.; Wang, G.; et al. Gender and Ethnic Disparities of Acute Kidney Injury in COVID-19 Infected Patients: A Literature Review. Front. Cell. Infect. Microbiol. 2022, 11, 1402. [Google Scholar] [CrossRef]
- Arslani, K.; Eken, C.; Tschudin-Sutter, S.; Gebhard, C.E.; Zellweger, N.; Bassetti, S.; Bingisser, R.; Lampart, M.; Osswald, S.; Kuster, G.M.; et al. Sex Disparities in Patients with Suspected COVID-19 Presenting at an Emergency Department in Switzerland. Swiss Med. Wkl. 2022, 152, w30167. [Google Scholar] [CrossRef]
- Hamza, A.; Shah, N.N.; Azad, A.M.; Ghanshyam, O.S.; Khan, Z. Impact of Age, Gender and Comorbidities Affecting the Severity of COVID-19 Infection in Kashmir. J. Family Med. Prim. Care 2022, 11, 1519–1524. [Google Scholar] [CrossRef]
- Roso-Llorach, A.; Serra-Picamal, X.; Cos, F.X.; Pallejà-Millán, M.; Mateu, L.; Rosell, A.; Almirante, B.; Ferrer, J.; Gasa, M.; Gudiol, C.; et al. Evolving Mortality and Clinical Outcomes of Hospitalized Subjects during Successive COVID-19 Waves in Catalonia, Spain. Glob. Epidemiol. 2022, 4, 100071. [Google Scholar] [CrossRef]
- Al-Numair, N.S.; Alyounes, B.; Al-Saud, H.; Halwani, R.; Al-Muhsen, S. Clinical Characteristics, Risk Factors, and Rate of Severity of a Nationwide COVID-19 Saudi Cohort. Saudi J. Biol. Sci. 2022, 29, 103315. [Google Scholar] [CrossRef]
- The Sex, Gender and COVID-19 Project|Global Health 50/50. Available online: https://globalhealth5050.org/the-sex-gender-and-covid-19-project/ (accessed on 1 June 2022).
- Joe, W.; Kumar, A.; Rajpal, S.; Mishra, U.S.; Subramanian, S.V. Equal Risk, Unequal Burden? Gender Differentials in COVID-19 Mortality in India. J. Glob. Health Sci. 2020, 2, e17. [Google Scholar] [CrossRef]
- Dehingia, N.; Raj, A. Sex Differences in COVID-19 Case Fatality: Do We Know Enough? Lancet Glob. Health 2021, 9, e14–e15. [Google Scholar] [CrossRef]
- Danielsen, A.C.; Lee, K.M.; Boulicault, M.; Rushovich, T.; Gompers, A.; Tarrant, A.; Reiches, M.; Shattuck-Heidorn, H.; Miratrix, L.W.; Richardson, S.S. Sex Disparities in COVID-19 Outcomes in the United States: Quantifying and Contextualizing Variation. Soc. Sci. Med. 2022, 294, 114716. [Google Scholar] [CrossRef] [PubMed]
- Islam, N.; Shkolnikov, V.M.; Acosta, R.J.; Klimkin, I.; Kawachi, I.; Irizarry, R.A.; Alicandro, G.; Khunti, K.; Yates, T.; Jdanov, D.A.; et al. Excess Deaths Associated with Covid-19 Pandemic in 2020: Age and Sex Disaggregated Time Series Analysis in 29 High Income Countries. BMJ 2021, 373, n1137. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study. Lancet 2018, 392, 1789–1858. [CrossRef] [Green Version]
- Gompers, A.; Bruch, J.D.; Richardson, S.S. Are COVID-19 Case Fatality Rates a Reliable Measure of Sex Disparities? Womens Health Issues 2022, 32, 87–89. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, Z.; Wang, Y.; Zhou, Y.; Ma, Y.; Zuo, W. Single-Cell RNA Expression Profiling of ACE2, the Receptor of SARS-CoV-2. Am. J. Respir. Crit. Care. Med. 2020, 202, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Habas, K.; Nganwuchu, C.; Shahzad, F.; Gopalan, R.; Haque, M.; Rahman, S.; Majumder, A.A.; Nasim, T. Resolution of Coronavirus Disease 2019 (COVID-19). Expert Rev. Anti. Infect. Ther. 2020, 18, 1201–1211. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.P.; Pritam, M.; Pandey, B.; Yadav, T.P. Microstructure, Pathophysiology, and Potential Therapeutics of COVID-19: A Comprehensive Review. J. Med. Virol. 2021, 93, 275–299. [Google Scholar] [CrossRef]
- Mousavizadeh, L.; Ghasemi, S. Genotype and Phenotype of COVID-19: Their Roles in Pathogenesis. J. Microbiol. Immunol. Infect. 2021, 54, 159–163. [Google Scholar] [CrossRef]
- Mohamed, M.S.; Moulin, T.C.; Schiöth, H.B. Sex Differences in COVID-19: The Role of Androgens in Disease Severity and Progression. Endocrine 2021, 71, 3–8. [Google Scholar] [CrossRef]
- Penna, C.; Mercurio, V.; Tocchetti, C.G.; Pagliaro, P. Sex-Related Differences in COVID-19 Lethality. Br. J. Pharmacol. 2020, 177, 4375–4385. [Google Scholar] [CrossRef]
- Chlamydas, S.; Papavassiliou, A.G.; Piperi, C. Epigenetic Mechanisms Regulating COVID-19 Infection. Epigenetics 2021, 16, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Tukiainen, T.; Villani, A.-C.; Yen, A.; Rivas, M.A.; Marshall, J.L.; Satija, R.; Aguirre, M.; Gauthier, L.; Fleharty, M.; Kirby, A.; et al. Landscape of X Chromosome Inactivation across Human Tissues. Nature 2017, 550, 244–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, R.A.S.; Oudit, G.Y.; Verano-Braga, T.; Canta, G.; Steckelings, U.M.; Bader, M. The Renin-Angiotensin System: Going beyond the Classical Paradigms. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H958–H970. [Google Scholar] [CrossRef]
- Emadi-Baygi, M.; Ehsanifard, M.; Afrashtehpour, N.; Norouzi, M.; Joz-Abbasalian, Z. Corona Virus Disease 2019 (COVID-19) as a System-Level Infectious Disease with Distinct Sex Disparities. Front Immunol. 2021, 12, 778913. [Google Scholar] [CrossRef] [PubMed]
- Bakhshandeh, B.; Sorboni, S.G.; Javanmard, A.-R.; Mottaghi, S.S.; Mehrabi, M.-R.; Sorouri, F.; Abbasi, A.; Jahanafrooz, Z. Variants in ACE2; Potential Influences on Virus Infection and COVID-19 Severity. Infect. Genet. Evol. 2021, 90, 104773. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Faidah, H.; Al-Maiahy, T.J.; Cruz-Martins, N.; Batiha, G.E.-S. The Looming Effects of Estrogen in Covid-19: A Rocky Rollout. Front. Nutr. 2021, 8, 649128. [Google Scholar] [CrossRef]
- Mjaess, G.; Karam, A.; Aoun, F.; Albisinni, S.; Roumeguère, T. COVID-19 and the Male Susceptibility: The Role of ACE2, TMPRSS2 and the Androgen Receptor. Prog. Urol. 2020, 30, 484–487. [Google Scholar] [CrossRef]
- Li, Y.; Jerkic, M.; Slutsky, A.S.; Zhang, H. Molecular Mechanisms of Sex Bias Differences in COVID-19 Mortality. Crit. Care 2020, 24, 405. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A Crucial Role of Angiotensin Converting Enzyme 2 (ACE2) in SARS Coronavirus-Induced Lung Injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef]
- Lan, J.; Ge, J.; Yu, J.; Shan, S.; Zhou, H.; Fan, S.; Zhang, Q.; Shi, X.; Wang, Q.; Zhang, L.; et al. Structure of the SARS-CoV-2 Spike Receptor-Binding Domain Bound to the ACE2 Receptor. Nature 2020, 581, 215–220. [Google Scholar] [CrossRef] [Green Version]
- McCoy, J.; Wambier, C.G.; Herrera, S.; Vaño-Galván, S.; Gioia, F.; Comeche, B.; Ron, R.; Serrano-Villar, S.; Iwasiow, R.M.; Tayeb, M.A.; et al. Androgen Receptor Genetic Variant Predicts COVID-19 Disease Severity: A Prospective Longitudinal Study of Hospitalized COVID-19 Male Patients. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e15–e17. [Google Scholar] [CrossRef] [PubMed]
- Totura, A.L.; Baric, R.S. SARS Coronavirus Pathogenesis: Host Innate Immune Responses and Viral Antagonism of Interferon. Curr. Opin. Virol. 2012, 2, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Sa Ribero, M.; Jouvenet, N.; Dreux, M.; Nisole, S. Interplay between SARS-CoV-2 and the Type I Interferon Response. PLoS Pathog. 2020, 16, e1008737. [Google Scholar] [CrossRef] [PubMed]
- Steen, E.H.; Wang, X.; Balaji, S.; Butte, M.J.; Bollyky, P.L.; Keswani, S.G. The Role of the Anti-Inflammatory Cytokine Interleukin-10 in Tissue Fibrosis. Adv. Wound. Care. 2020, 9, 184–198. [Google Scholar] [CrossRef] [Green Version]
- Scully, E.P.; Schumock, G.; Fu, M.; Massaccesi, G.; Muschelli, J.; Betz, J.; Klein, E.Y.; West, N.E.; Robinson, M.; Garibaldi, B.T.; et al. Sex and Gender Differences in Testing, Hospital Admission, Clinical Presentation, and Drivers of Severe Outcomes From COVID-19. Open Forum Infect. Dis. 2021, 8, ofab448. [Google Scholar] [CrossRef]
- Qi, S.; Ngwa, C.; Morales Scheihing, D.A.; Al Mamun, A.; Ahnstedt, H.W.; Finger, C.E.; Colpo, G.D.; Sharmeen, R.; Kim, Y.; Choi, H.A.; et al. Sex Differences in the Immune Response to Acute COVID-19 Respiratory Tract Infection. Biol. Sex Differ. 2021, 12, 66. [Google Scholar] [CrossRef]
- CDC. COVID-19 Vaccine Breakthrough Case Investigations Team COVID-19 Vaccine Breakthrough Infections Reported to CDC-United States, 1 January–30 April. MMWR Morb. Mortal. Wkly Rep. 2021, 70, 792–793. [Google Scholar] [CrossRef]
- Demonbreun, A.R.; Sancilio, A.; Velez, M.E.; Ryan, D.T.; Pesce, L.; Saber, R.; Vaught, L.A.; Reiser, N.L.; Hsieh, R.R.; D’Aquila, R.T.; et al. COVID-19 MRNA Vaccination Generates Greater Immunoglobulin G Levels in Women Compared to Men. J. Infect. Dis. 2021, 224, 793–797. [Google Scholar] [CrossRef]
- Jacobsen, H.; Klein, S.L. Sex Differences in Immunity to Viral Infections. Front. Immunol. 2021, 12, 720952. [Google Scholar] [CrossRef]
- AbdulHussain, G.; Azizieh, F.; Makhseed, M.; Raghupathy, R. Effects of Progesterone, Dydrogesterone and Estrogen on the Production of Th1/Th2/Th17 Cytokines by Lymphocytes from Women with Recurrent Spontaneous Miscarriage. J. Reprod. Immunol. 2020, 140, 103132. [Google Scholar] [CrossRef]
- Aksoyalp, Z.Ş.; Nemutlu-Samur, D. Sex-Related Susceptibility in Coronavirus Disease 2019 (COVID-19): Proposed Mechanisms. Eur. J. Pharmacol. 2021, 912, 174548. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Agrawal, P.; Gautam, A.; Pursnani, N.; Agarwal, M.; Agarwal, A.; Parihar, A.; Pandey, A. COVID-19 Outcomes in Postmenopausal and Perimenopausal Females: Is Estrogen Hormone Attributing to Gender Differences? J. Midlife Health 2020, 11, 250–256. [Google Scholar] [CrossRef]
- Dhindsa, S.; Zhang, N.; McPhaul, M.J.; Wu, Z.; Ghoshal, A.K.; Erlich, E.C.; Mani, K.; Randolph, G.J.; Edwards, J.R.; Mudd, P.A.; et al. Association of Circulating Sex Hormones With Inflammation and Disease Severity in Patients With COVID. JAMA Netw. Open 2021, 4, e2111398. [Google Scholar] [CrossRef] [PubMed]
- Rastrelli, G.; Di Stasi, V.; Inglese, F.; Beccaria, M.; Garuti, M.; Di Costanzo, D.; Spreafico, F.; Greco, G.F.; Cervi, G.; Pecoriello, A.; et al. Low Testosterone Levels Predict Clinical Adverse Outcomes in SARS-CoV-2 Pneumonia Patients. Andrology 2021, 9, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Lima, D.L.F.; Dias, A.A.; Rabelo, R.S.; da Cruz, I.D.; Costa, S.C.; Nigri, F.M.N.; Neri, J.R. COVID-19 no estado do Ceará, Brasil: Comportamentos e crenças na chegada da pandemia. Ciênc. Saúde Coletiva 2020, 25, 1575–1586. [Google Scholar] [CrossRef] [PubMed]
- Clements, J.M. Knowledge and Behaviors toward COVID-19 Among US Residents During the Early Days of the Pandemic: Cross-Sectional Online Questionnaire. JMIR Public Health Surveill. 2020, 6, e19161. [Google Scholar] [CrossRef]
- Wolf, M.S.; Serper, M.; Opsasnick, L.; O’Conor, R.M.; Curtis, L.; Benavente, J.Y.; Wismer, G.; Batio, S.; Eifler, M.; Zheng, P.; et al. Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the U.S. Outbreak: A Cross-Sectional Survey. Ann. Intern. Med. 2020, 173, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Galasso, V.; Pons, V.; Profeta, P.; Becher, M.; Brouard, S.; Foucault, M. Gender Differences in COVID-19 Attitudes and Behavior: Panel Evidence from Eight Countries. Proc. Natl. Acad. Sci. USA 2020, 117, 27285–27291. [Google Scholar] [CrossRef]
- Pflugeisen, B.M.; Mou, J. Gender Discrepancies in SARS-CoV-2 Pandemic Related Beliefs, Attitudes, and Practices. Front. Public Health 2021, 9, 711460. [Google Scholar] [CrossRef]
- Tejpal, A.; Gianos, E.; Cerise, J.; Hirsch, J.S.; Rosen, S.; Kohn, N.; Lesser, M.; Weinberg, C.; Majure, D.; Satapathy, S.K.; et al. Sex-Based Differences in COVID-19 Outcomes. J. Womens Health 2021, 30, 492–501. [Google Scholar] [CrossRef]
- Azevedo, R.B.; Botelho, B.G.; Hollanda, J.V.G.D.; Ferreira, L.V.L.; Junqueira de Andrade, L.Z.; Oei, S.S.M.L.; Mello, T.d.S.; Muxfeldt, E.S. Covid-19 and the Cardiovascular System: A Comprehensive Review. J. Hum. Hypertens 2021, 35, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Schlichthorst, M.; Sanci, L.A.; Pirkis, J.; Spittal, M.J.; Hocking, J.S. Why Do Men Go to the Doctor? Socio-Demographic and Lifestyle Factors Associated with Healthcare Utilisation among a Cohort of Australian Men. BMC Public Health 2016, 16, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, C.A.; Pope, C.R. Gender, Psychosocial Factors and the Use of Medical Services: A Longitudinal Analysis. Soc. Sci. Med. 1999, 48, 1363–1372. [Google Scholar] [CrossRef]
- Banks, I.; Baker, P. Men and Primary Care: Improving Access and Outcomes. Trends Urol. Men’s Health 2013, 4, 39–41. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
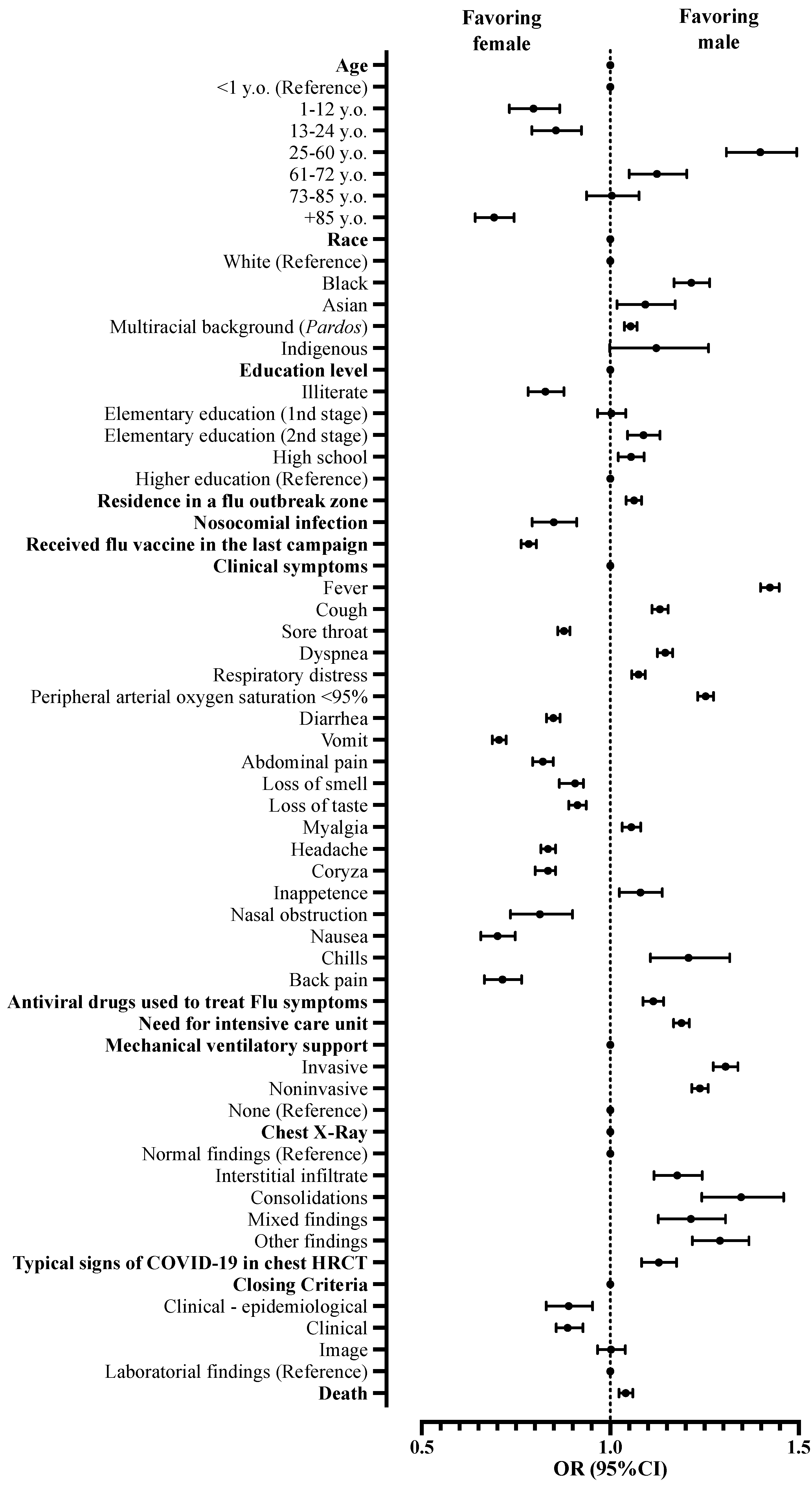
| Patients’ Features | Data | Male | Female | Total | p | OR | 95%CI |
|---|---|---|---|---|---|---|---|
| Age | <1 year old | 2126 (1.0%) | 1499 (1.2%) | 3625 (1.1%) | - | 1 | Reference |
| 1–12 years old | 2990 (1.4%) | 2648 (2.1%) | 5638 (1.7%) | <0.001 | 0.796 | 0.732–0.866 | |
| 13–24 years old | 5358 (2.5%) | 4416 (3.6%) | 9774 (2.9%) | <0.001 | 0.856 | 0.792–0.924 | |
| 25–60 years old | 135,046 (63.4%) | 68,098 (55.2%) | 203,144 (60.4%) | <0.001 | 1.398 | 1.308–1.495 | |
| 61–72 years old | 37,983 (17.8%) | 23,820 (19.3%) | 61,803 (18.4%) | <0.001 | 1.124 | 1.050–1.203 | |
| 73–85 years old | 23,289 (10.9%) | 16,350 (13.3%) | 39,639 (11.8%) | 0.917 | 1.004 | 0.937–1.076 | |
| +85 years old | 6359 (3.0%) | 6481 (5.3%) | 12,840 (3.8%) | <0.001 | 0.692 | 0.642–0.0745 | |
| Race | White | 78,237 (47.2%) | 48,634 (48.8%) | 126,871 (47.8%) | - | 1 | Reference |
| Black | 8118 (4.9%) | 4153 (4.2%) | 12,271 (4.6%) | <0.001 | 1.215 | 1.169–1.264 | |
| Asian | 2204 (1.3%) | 1254 (1.3%) | 3458 (1.3%) | 0.014 | 1.093 | 1.018–1.172 | |
| Pardos | 76,424 (46.1%) | 45,081 (45.3%) | 121,505 (45.8%) | <0.001 | 1.054 | 1.037–1.071 | |
| Indigenous | 794 (0.5%) | 440 (0.4%) | 1234 (0.5%) | 0.058 | 1.122 | 0.999–1.261 | |
| Schooling | Illiterate | 3437 (4.5%) | 2601 (5.6%) | 6038 (4.9%) | <0.001 | 0.828 | 0.782–0.877 |
| Elementary school (1st stage) | 14,820 (19.6%) | 9256 (19.8%) | 24,076 (19.7%) | 0.861 | 1.003 | 0.967–1.041 | |
| Elementary school (2nd stage) | 12,525 (16.5%) | 7214 (15.4%) | 19,739 (16.1%) | <0.001 | 1.088 | 1.046–1.132 | |
| High school | 28,139 (37.1%) | 16,718 (35.8%) | 44,857 (36.6%) | 0.001 | 1.055 | 1.021–1.090 | |
| Higher education | 14,432 (19.0%) | 9045 (19.3%) | 23,477 (19.2%) | - | 1 | Reference | |
| Not applicable | 2420 (3.2%) | 1916 (4.1%) | 4336 (3.5%) | - | - | - | |
| Place of residence | Urban | 174,266 (94.6%) | 102,249 (94.8%) | 276,515 (94.7%) | 1 | Reference | |
| Rural | 9249 (5.0%) | 5323 (4.9%) | 14,572 (5.0%) | 0.275 | 1.019 | 0.985–1.055 | |
| Peri-urban | 620 (0.3%) | 340 (0.3%) | 960 (0.3%) | 0.319 | 1.070 | 0.937–1.222 | |
| Residing in an Influenza syndrome outbreak area | Yes | 40,896 (31.2%) | 23,296 (30.0%) | 64,192 (30.8%) | <0.001 | 1.063 | 1.042–1.083 |
| No | 89,993 (68.8%) | 54,469 (70.0%) | 144,462 (69.2%) | 1 | Reference | ||
| Presence of nosocomial infection | Yes | 1994 (1.4%) | 1381 (1.7%) | 3375 (1.5%) | <0.001 | 0.850 | 0.793–0.911 |
| No | 139,316 (98.6%) | 82,026 (98.3%) | 221,342 (98.5%) | 1 | Reference | ||
| Flu vaccination in the last campaign | Yes | 18,422 (21.5%) | 13,571 (25.9%) | 31,993 (23.1%) | <0.001 | 0.784 | 0.764–0.804 |
| No | 67,346 (78.5%) | 38,869 (74.1%) | 106,215 (76,9%) | - | 1 | Reference |
| Clinical Signs | Data | Male | Female | Total | p | OR | 95%CI |
|---|---|---|---|---|---|---|---|
| Fever | Yes | 138,913 (76.7%) | 71,334 (69.8%) | 210,247 (74.2%) | <0.001 | 1.424 | 1.399–1.448 |
| No | 42,228 (23.3%) | 30,873 (30.2%) | 73,101 (25.8%) | 1 | Reference | ||
| Cough | Yes | 150,059 (81.7%) | 84,429 (79.8%) | 234,488 (81.0%) | <0.001 | 1.132 | 1.111–1.154 |
| No | 33,571 (18.3%) | 21,381 (20.2%) | 54,952 (19.0%) | 1 | Reference | ||
| Sore throat | Yes | 44,737 (30.2%) | 28,751 (33.0%) | 73,488 (31.2%) | <0.001 | 0.877 | 0.861–0.893 |
| No | 103,629 (69.8%) | 58,381 (67.0%) | 162,010 (68.8%) | 1 | Reference | ||
| Dyspnea | Yes | 140,964 (77.9%) | 78,403 (75.5%) | 219,367 (77.0%) | <0.001 | 1.146 | 1.125–1.166 |
| No | 39,972 (22.1%) | 25,467 (24.5%) | 65,439 (23.0%) | 1 | Reference | ||
| Respiratory distress | Yes | 114,711 (68.5%) | 64,836 (66.9%) | 179,547 (67.9%) | <0.001 | 1.075 | 1.057–1.093 |
| No | 52,782 (31.5%) | 32,057 (33.1%) | 84,839 (32.1%) | 1 | Reference | ||
| Peripheral arterial oxygen saturation < 95% | Yes | 114,264 (67.8%) | 60,320 (62.7%) | 174,584 (65.9%) | <0.001 | 1.253 | 1.232–1.274 |
| No | 54,310 (32.2%) | 35,917 (37.3%) | 90,227 (34.1%) | 1 | Reference | ||
| Diarrhea | Yes | 27,272 (19.1%) | 18,246 (21.7%) | 45,518 (20.1%) | <0.001 | 0.849 | 0.831–0.867 |
| No | 115,633 (80.9%) | 65,648 (78.3%) | 181,281 (79.9%) | 1 | Reference | ||
| Vomit | Yes | 14,127 (10.1%) | 11,299 (13.8%) | 25,426 (11.5%) | <0.001 | 0.705 | 0.687–0.724 |
| No | 125,104 (89.9%) | 70,570 (86.2%) | 195,674 (88.5%) | 1 | Reference | ||
| Abdominal pain | Yes | 9191 (9.2%) | 6482 (11.0%) | 15,673 (9.9%) | <0.001 | 0.821 | 0.794–0.849 |
| No | 90,372 (90.8%) | 52,337 (89.0%) | 142,709 (90.1%) | 1 | Reference | ||
| Fatigue and asthenia | Yes | 42,918 (39.4%) | 25,490 (39.8%) | 68,408 (39.6%) | 0.105 | 0.983 | 0.964–1.003 |
| No | 65,932 (60.6%) | 38,517 (60.2%) | 104,449 (60.4%) | 1 | Reference | ||
| Loss of smell | Yes | 21,298 (20.4%) | 13,662 (22.1%) | 34,960 (21.1%) | <0.001 | 0.907 | 0.865–0.929 |
| No | 82,863 (79.6%) | 48,209 (77.9%) | 131,072 (78.9%) | 1 | Reference | ||
| Loss of taste | Yes | 19,893 (19.4%) | 12,686 (20.8%) | 32,579 (19.9%) | <0.001 | 0.913 | 0.890–0.936 |
| No | 82,757 (80.6%) | 48,166 (79.2%) | 130,923 (80.1%) | 1 | Reference | ||
| Myalgia | Yes | 23,447 (16.8%) | 13,137 (16.0%) | 36,584 (16.5%) | <0.001 | 1.056 | 1.032–1.081 |
| No | 116,532 (83.2%) | 68,963 (84.0%) | 185,495 (83.5%) | 1 | Reference | ||
| Headache | Yes | 21,762 (15.5%) | 14,829 (18.1%) | 36,591 (16.5%) | <0.001 | 0.835 | 0.816–0.855 |
| No | 118,217 (84.5%) | 67,271 (81.9%) | 185,488 (83.5%) | 1 | Reference | ||
| Coryza | Yes | 5820 (4.2%) | 4056 (4.9%) | 9876 (4.4%) | <0.001 | 0.835 | 0.801–0.870 |
| No | 134,159 (95.8%) | 78,044 (95.1%) | 212,203 (95.6%) | 1 | Reference | ||
| Inappetence | Yes | 4012 (2.9%) | 2184 (2.7%) | 6196 (2.8%) | 0.004 | 1.080 | 1.024–1.138 |
| No | 135,965 (97.1%) | 79,914 (97.3%) | 215,879 (97.2%) | 1 | Reference | ||
| Nasal obstruction | Yes | 897 (0.6%) | 646 (0.8%) | 1543 (0.7%) | <0.001 | 0.813 | 0.735–0.900 |
| No | 139,080 (99.4%) | 81,452 (99.2%) | 220,532 (99.3%) | 1 | Reference | ||
| Vertigo | Yes | 781 (0.6%) | 510 (0.6%) | 1291 (0.6%) | 0.058 | 0.897 | 0.802–1.003 |
| No | 139,196 (99.4%) | 81,588 (99.4%) | 220,784 (99.4%) | 1 | Reference | ||
| Prostration | Yes | 2469 (1.8%) | 1492 (1.8%) | 3961 (1.8%) | 0.358 | 0.970 | 0.909–1.035 |
| No | 137,508 (98.2%) | 80,606 (98.2%) | 218,114 (98.2%) | 1 | Reference | ||
| Nausea | Yes | 2073 (1.5%) | 1724 (2.1%) | 3797 (1.7%) | <0.001 | 0.701 | 0.657–0.748 |
| No | 137,904 (98.5%) | 80,374 (97.9%) | 218,278 (98.3%) | 1 | Reference | ||
| Malaise | Yes | 2081 (1.5%) | 1231 (1.5%) | 3312 (1.5%) | 0.811 | 0.991 | 0.923–1.064 |
| No | 137,896 (98.5%) | 80,867 (98.5%) | 218,763 (98.5%) | 1 | Reference | ||
| Chills | Yes | 1568 (1.1%) | 763 (0.9%) | 2331 (1.0%) | <0.001 | 1.208 | 1.107–1.317 |
| No | 138,409 (98.9%) | 81,335 (99.1%) | 219,744 (99.0%) | 1 | Reference | ||
| Chest pain | Yes | 4088 (2.9%) | 2429 (3.0%) | 6517 (2.9%) | 0.607 | 0.987 | 0.938–1.038 |
| No | 135,889 (97.1%) | 79,669 (97.0%) | 215,558 (97.1%) | 1 | Reference | ||
| Back pain | Yes | 1803 (1.3%) | 1474 (1.8%) | 3277 (1.5%) | <0.001 | 0.714 | 0.666–0.765 |
| No | 138,174 (98.7%) | 80,624 (98.2%) | 218,798 (98.5%) | 1 | Reference | ||
| Arthralgia | Yes | 778 (0.6%) | 405 (0.5%) | 1183 (0.5%) | 0.051 | 1.127 | 0.999–1.272 |
| No | 139,199 (99.4%) | 81,693 (99.5%) | 220,892 (99.5%) | 1 | Reference |
| Patients’ Features | Data | Male | Female | Total | p | OR | 95%CI |
|---|---|---|---|---|---|---|---|
| Antiviral drug to treat flu symptoms | Yes | 20,998 (14.7%) | 11,324 (13.4%) | 32,322 (14.2%) | <0.001 | 1.114 | 1.087–1.142 |
| No | 121,814 (85.3%) | 73,200 (86.6%) | 195,014 (85.8%) | - | 1 | Reference | |
| Intensive care unit | Yes | 50,398 (29.6%) | 25,067 (26.2%) | 75,465 (28.4%) | <0.001 | 1.189 | 1.168–1.210 |
| No | 119,679 (70.4%) | 70,779 (73.8%) | 190,458 (71.6%) | 1 | Reference | ||
| Use of ventilatory support | Invasive | 25,070 (14.9%) | 12,850 (13.3%) | 37,920 (14.3%) | <0.001 | 1.306 | 1.273–1.339 |
| Noninvasive | 92,216 (54.9%) | 49,854 (51.6%) | 142,070 (53.7%) | <0.001 | 1.238 | 1.216–1.260 | |
| Not necessary | 50,571 (30.1%) | 33,843 (35.1%) | 84,414 (31.9%) | - | 1 | Reference | |
| Thorax X-ray result | Normal | 3800 (3.7%) | 2520 (4.2%) | 6320 (3.9%) | - | 1 | Reference |
| Interstitial infiltrate | 25,876 (25.1%) | 14,563 (24.3%) | 40,439 (24.8%) | <0.001 | 1.178 | 1.116–1.244 | |
| Consolidation | 2966 (2.9%) | 1460 (2.4%) | 4426 (2.7%) | <0.001 | 1.347 | 1.243–1.460 | |
| Mixed | 3798 (3.7%) | 2075 (3.5%) | 5873 (3.6%) | <0.001 | 1.214 | 1.128–1.306 | |
| Other | 14,127 (13.7%) | 7257 (12.1%) | 21,384 (13.1%) | <0.001 | 1.291 | 1.218–1.368 | |
| Not carried out | 52,384 (50.9%) | 32,168 (53.6%) | 84,552 (51.9%) | - | - | - | |
| Thorax HRCT | Typical COVID-19 | 58,965 (67.8%) | 31,262 (62.8%) | 90,227 (65.9%) | <0.001 | 1.129 | 1.083–1.176 |
| Undetermined COVID-19 | 2110 (2.4%) | 1344 (2.7%) | 3454 (2.5%) | - | 1 | Reference | |
| Atypical COVID-19 | 1100 (1.3%) | 682 (1.4%) | 1782 (1.3%) | - | 1 | Reference | |
| Negative for pneumonia | 231 (0.3%) | 238 (0.5%) | 469 (0.3%) | - | 1 | Reference | |
| Other | 3341 (3.8%) | 1801 (3.6%) | 5142 (3.8%) | - | 1 | Reference | |
| Not carried out | 21,286 (24.5%) | 14,458 (29.0%) | 35,744 (26.1%) | - | - | - | |
| Closing criterion | Laboratorial | 188,426 (92.6%) | 108,199 (92.2%) | 296,625 (92.4%) | - | 1 | Reference |
| Epidemiological clinical | 2088 (1.0%) | 1348 (1.1%) | 3436 (1.1%) | <0.001 | 0.890 | 0.830–0.953 | |
| Clinical | 4826 (2.4%) | 3126 (2.7%) | 7952 (2.5%) | <0.001 | 0.887 | 0.847–0.928 | |
| Image clinical | 8173 (4.0%) | 4683 (4.0%) | 12,856 (4.0%) | 0.915 | 1.002 | 0.966–1.040 | |
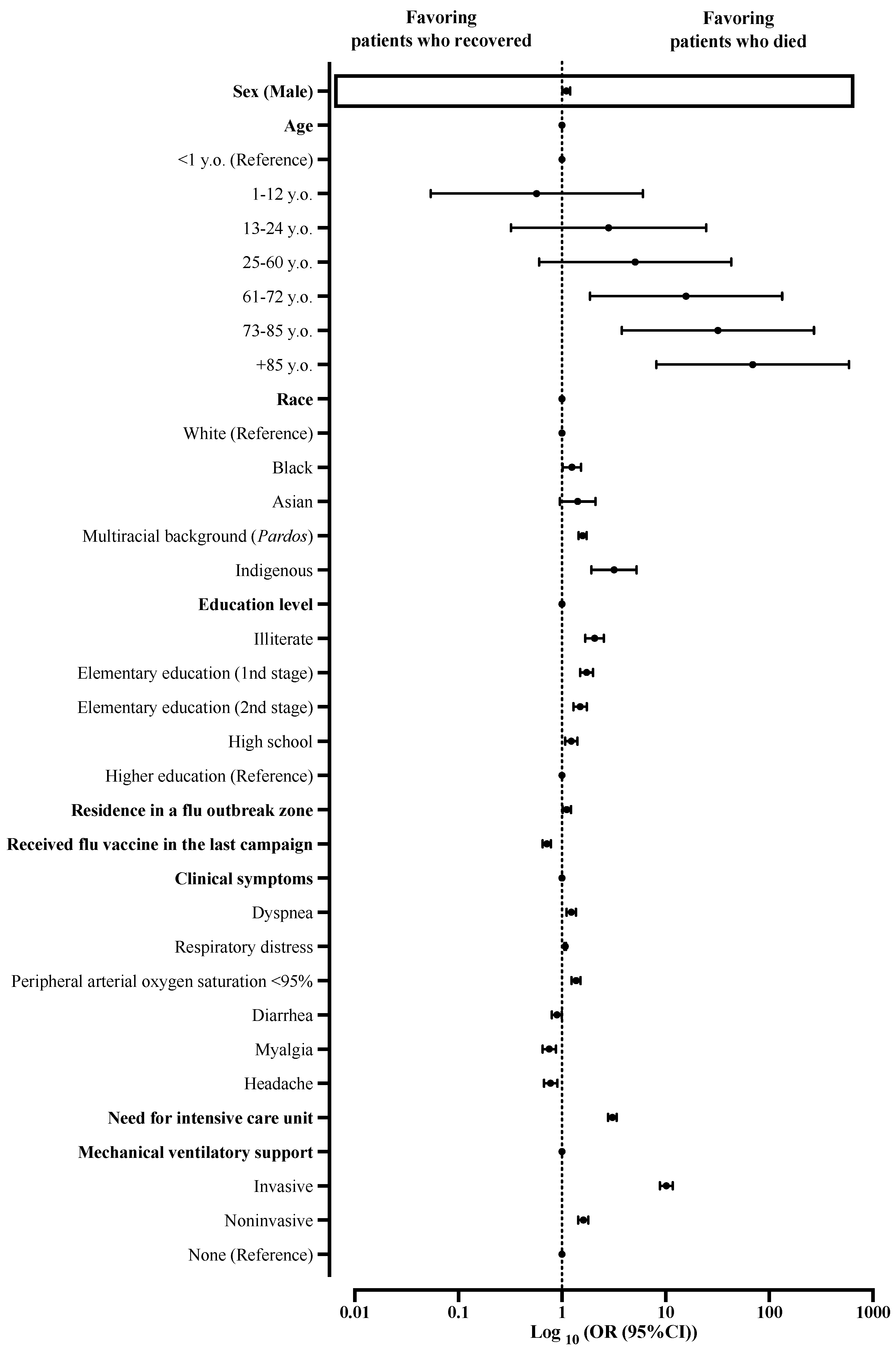
| Outcome | Cure | 130,340 (73.4%) | 76,470 (74.2%) | 206,810 (73.7%) | <0.001 | 1 | Reference |
| Death * | 47,158 (26.6%) | 26,565 (25.8%) | 73,723 (26.3%) | - | 1.041 | 1.023–1.060 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sansone, N.M.S.; Pereira, L.R.; Boschiero, M.N.; Valencise, F.E.; Fraga, A.M.A.; Marson, F.A.L. Characterization of Clinical Features of Hospitalized Patients Due to the SARS-CoV-2 Infection in the Absence of Comorbidities Regarding the Sex: An Epidemiological Study of the First Year of the Pandemic in Brazil. Int. J. Environ. Res. Public Health 2022, 19, 8895. https://doi.org/10.3390/ijerph19158895
Sansone NMS, Pereira LR, Boschiero MN, Valencise FE, Fraga AMA, Marson FAL. Characterization of Clinical Features of Hospitalized Patients Due to the SARS-CoV-2 Infection in the Absence of Comorbidities Regarding the Sex: An Epidemiological Study of the First Year of the Pandemic in Brazil. International Journal of Environmental Research and Public Health. 2022; 19(15):8895. https://doi.org/10.3390/ijerph19158895
Chicago/Turabian StyleSansone, Nathália Mariana Santos, Letícia Rogini Pereira, Matheus Negri Boschiero, Felipe Eduardo Valencise, Andréa Melo Alexandre Fraga, and Fernando Augusto Lima Marson. 2022. "Characterization of Clinical Features of Hospitalized Patients Due to the SARS-CoV-2 Infection in the Absence of Comorbidities Regarding the Sex: An Epidemiological Study of the First Year of the Pandemic in Brazil" International Journal of Environmental Research and Public Health 19, no. 15: 8895. https://doi.org/10.3390/ijerph19158895
APA StyleSansone, N. M. S., Pereira, L. R., Boschiero, M. N., Valencise, F. E., Fraga, A. M. A., & Marson, F. A. L. (2022). Characterization of Clinical Features of Hospitalized Patients Due to the SARS-CoV-2 Infection in the Absence of Comorbidities Regarding the Sex: An Epidemiological Study of the First Year of the Pandemic in Brazil. International Journal of Environmental Research and Public Health, 19(15), 8895. https://doi.org/10.3390/ijerph19158895