
Unmet Healthcare Needs Predict Depression Symptoms among Older Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Study Design
2.2. Variables
2.2.1. Current Mental Health Outcomes
2.2.2. Unmet Healthcare Needs
2.2.3. Other Predictive Variables
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis
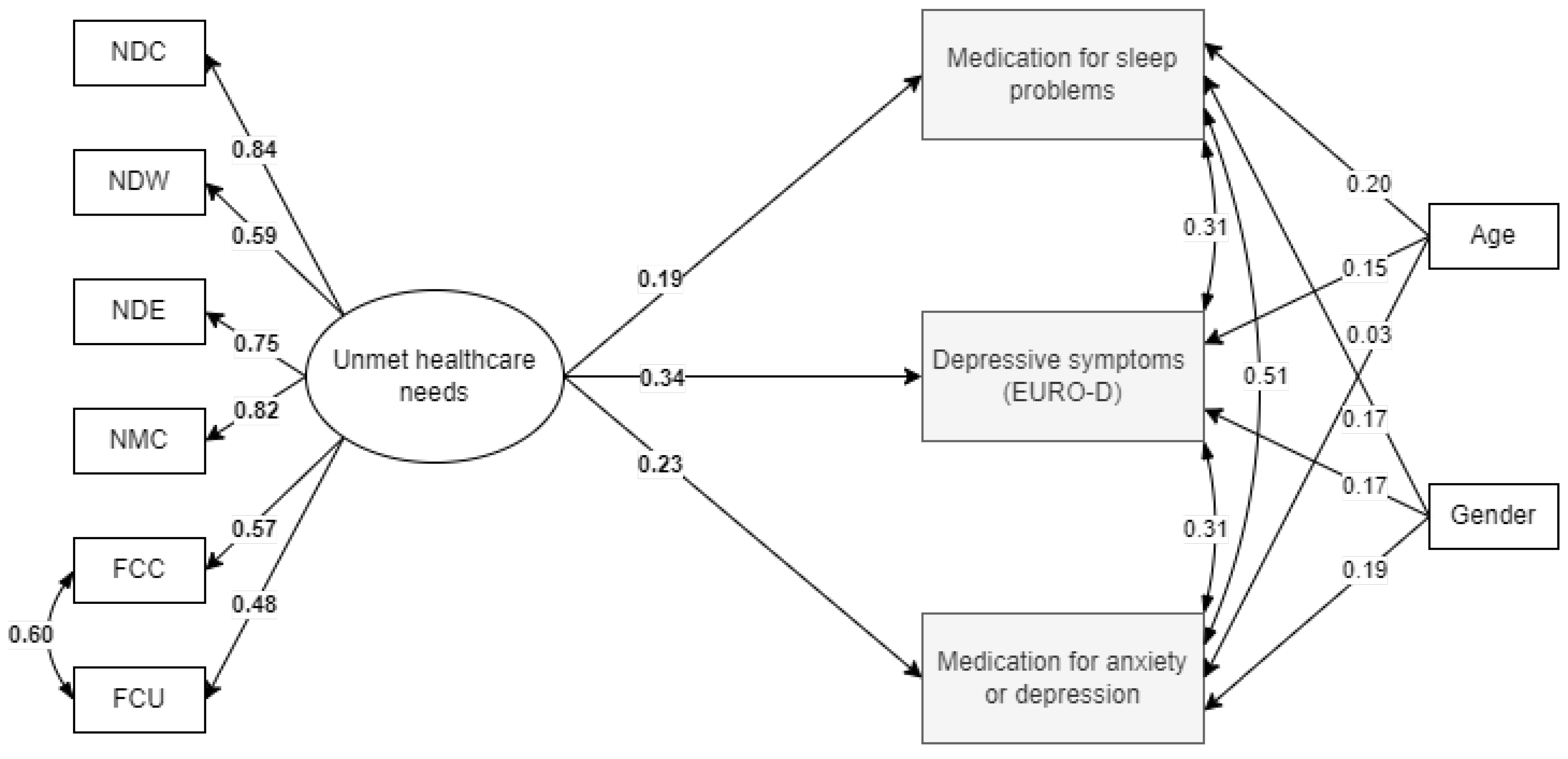
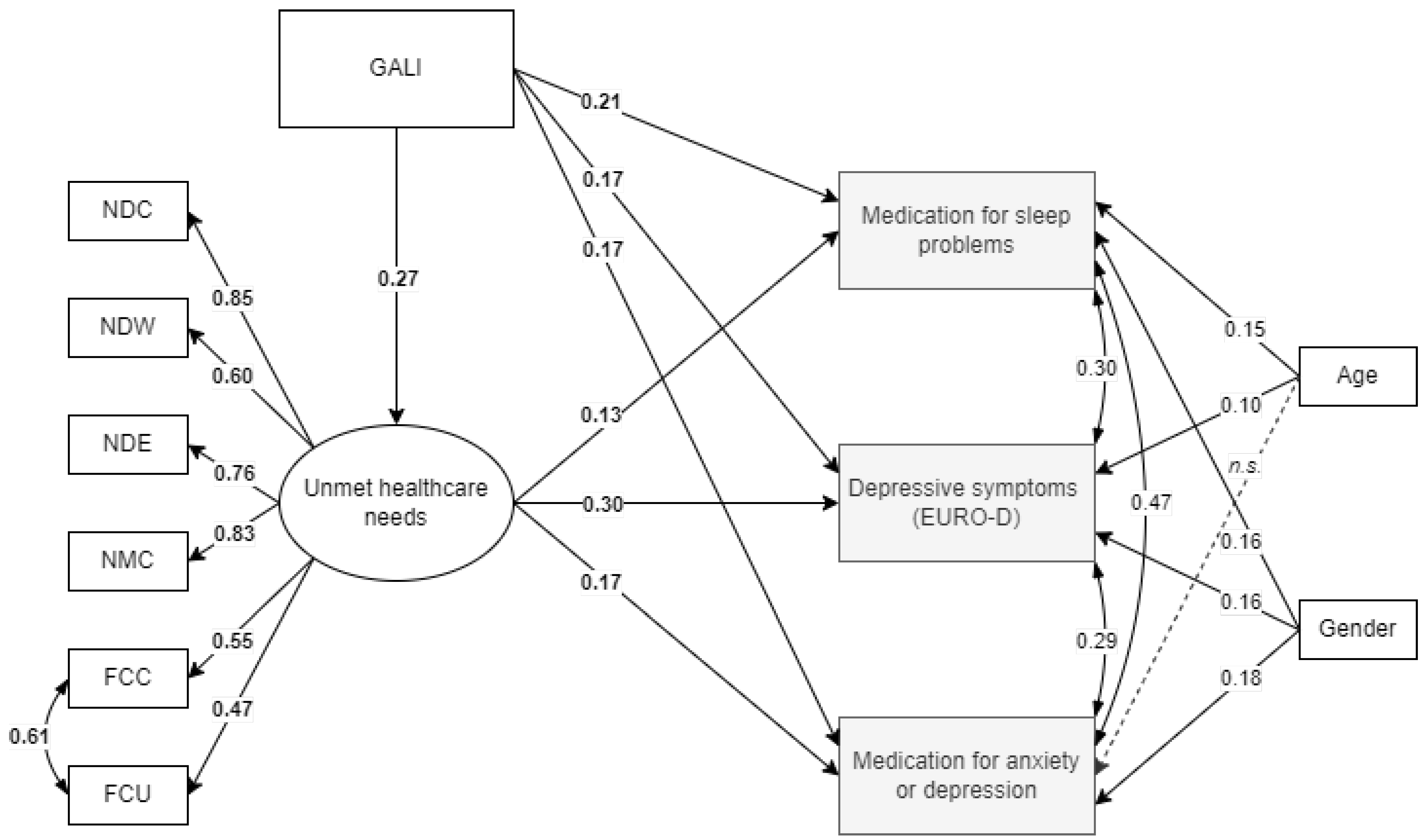
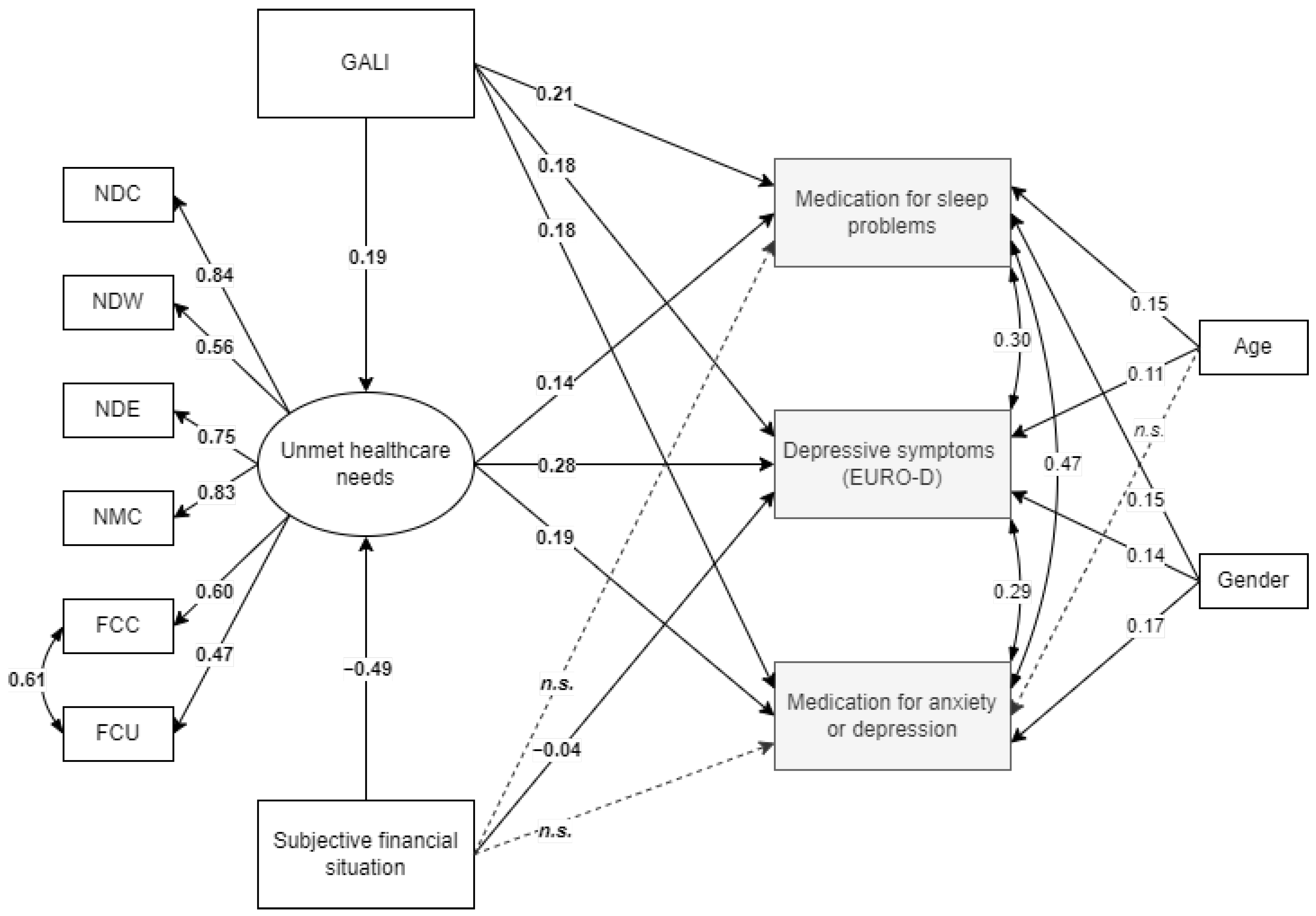
3.2. Path Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Volkert, J.; Schulz, H.; Härter, M.; Wlodarczyk, O.; Andreas, S. The Prevalence of Mental Disorders in Older People in Western Countries—A Meta-Analysis. Ageing Res. Rev. 2013, 12, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Abdoli, N.; Salari, N.; Darvishi, N.; Jafarpour, S.; Solaymani, M.; Mohammadi, M.; Shohaimi, S. The Global Prevalence of Major Depressive Disorder (MDD) among the Elderly: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2022, 132, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Zhao, X.; Wu, M.; Li, Z.; Luo, L.; Yang, C.; Yang, F. Prevalence of Depression in Older Adults: A Systematic Review and Meta-Analysis. Psychiatry Res. 2022, 311, 114511. [Google Scholar] [CrossRef]
- Brenes, G.A. Depression, and QOL in Primary Care Patients. Prim Care Companion J. Clin. Psychiatry 2007, 9, 437. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Milaneschi, Y.; Lamers, F.; Vogelzangs, N. Understanding the Somatic Consequences of Depression: Biological Mechanisms and the Role of Depression Symptom Profile. BMC Med. 2013, 11, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Chen, Y.; Ma, L. Depression and Cardiovascular Disease in Elderly: Current Understanding. J. Clin. Neurosci. 2018, 47, 1–5. [Google Scholar] [CrossRef]
- Kim, H.-K.; Seo, J.-H.; Kim, H.-K.; Seo, J.-H. Effects of Health Status, Depression, Gerotranscendence, Self-Efficacy, and Social Support on Healthy Aging in the Older Adults with Chronic Diseases. Int. J. Environ. Res. Public Health 2022, 19, 7930. [Google Scholar] [CrossRef]
- Vink, D.; Aartsen, M.J.; Schoevers, R.A. Risk Factors for Anxiety and Depression in the Elderly: A Review. J. Affect. Disord. 2008, 106, 29–44. [Google Scholar] [CrossRef]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.T.; et al. Relationship between Depression and Frailty in Older Adults: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Laird, K.T.; Krause, B.; Funes, C.; Lavretsky, H. Psychobiological Factors of Resilience and Depression in Late Life. Transl. Psychiatry 2019, 9, 1–18. [Google Scholar] [CrossRef]
- Domènech-Abella, J.; Mundó, J.; Leonardi, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Ayuso-Mateos, J.L.; Haro, J.M. The Association between Socioeconomic Status and Depression among Older Adults in Finland, Poland and Spain: A Comparative Cross-Sectional Study of Distinct Measures and Pathways. J. Affect. Disord. 2018, 241, 311–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houtjes, W.; Van Meijel, B.; Deeg, D.J.H.; Beekman, A.T.F. Major Depressive Disorder in Late Life: A Multifocus Perspective on Care Needs. Aging Ment. Health 2010, 14, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Dautzenberg, G.; Lans, L.; Meesters, P.D.; Kupka, R.; Beekman, A.; Stek, M.L.; Dols, A. The Care Needs of Older Patients with Bipolar Disorder. Aging Ment. Health 2016, 20, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.; Liegert, P.; Dorow, M.; König, H.H.; Riedel-Heller, S.G. Unmet Health Care Needs in Old Age and Their Association with Depression—Results of a Population-Representative Survey. J. Affect. Disord. 2019, 245, 998–1006. [Google Scholar] [CrossRef]
- Choi, N.G.; McDougall, G. Unmet Needs and Depressive Symptoms Among Low-Income Older Adults. J. Gerontol. Soc. Work. 2009, 52, 567–583. [Google Scholar] [CrossRef]
- Ju, Y.J.; Kim, T.H.; Han, K.T.; Lee, H.J.; Kim, W.; Lee, S.A.; Park, E.C. Association between Unmet Healthcare Needs and Health-Related Quality of Life: A Longitudinal Study. Eur. J. Public Health 2017, 27, 631–637. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Lee, J.; Moon, Y.; Kim, K.J.; Lee, K.; Choi, J.; Han, S.H. Unmet Healthcare Needs of Elderly People in Korea. BMC Geriatr. 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.A.; Safian, N.; Ahmad, S.; Nurumal, S.R.; Mohammad, Z.; Mansor, J.; Ibadullah, W.A.H.W.; Shobugawa, Y.; Rosenberg, M. Unmet Healthcare Needs Among Elderly Malaysians. J. Multidiscip. Healthc. 2021, 14, 2931. [Google Scholar] [CrossRef]
- Gao, Q.; Prina, M.; Wu, Y.T.; Mayston, R. Unmet Healthcare Needs among Middle-Aged and Older Adults in China. Age Ageing 2022, 51, afab235. [Google Scholar] [CrossRef]
- OECD. Unmet Needs for Health Care: Comparing Approaches and Results from International Surveys; OECD: Paris, France, 2022.
- Lindström, C.; Rosvall, M.; Lindström, M. Unmet Health-Care Needs and Mortality: A Prospective Cohort Study from Southern Sweden. Scand. J. Public Health 2020, 48, 267–274. [Google Scholar] [CrossRef]
- Ko, H. Unmet Healthcare Needs and Health Status: Panel Evidence from Korea. Health Policy 2016, 120, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.R.; Dias, C.C.; Fernandes, L. Needs in Nursing Homes and Their Relation with Cognitive and Functional Decline, Behavioral and Psychological Symptoms. Front. Aging Neurosci. 2016, 8, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alltag, S.; Stein, J.; Pabst, A.; Weyerer, S.; Werle, J.; Maier, W.; Miebach, L.; Scherer, M.; Stark, A.; Wiese, B.; et al. Unmet Needs in the Depressed Primary Care Elderly and Their Relation to Severity of Depression: Results from the AgeMooDe Study. Aging Ment. Health 2017, 22, 1032–1039. [Google Scholar] [CrossRef]
- Clignet, F.; Houtjes, W.; van Straten, A.; Cuijpers, P.; van Meijel, B. Unmet Care Needs, Care Provision and Patient Satisfaction in Patients with a Late Life Depression: A Cross-Sectional Study. Aging Ment. Health 2018, 23, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Altamura, A.C.; Dell’Osso, B.; Vismara, S.; Mundo, E. May Duration of Untreated Illness Influence the Long-Term Course of Major Depressive Disorder? Eur. Psychiatry 2008, 23, 92–96. [Google Scholar] [CrossRef]
- Ghio, L.; Gotelli, S.; Cervetti, A.; Respino, M.; Natta, W.; Marcenaro, M.; Serafini, G.; Vaggi, M.; Amore, M.; Belvederi Murri, M. Duration of Untreated Depression Influences Clinical Outcomes and Disability. J. Affect. Disord. 2015, 175, 224–228. [Google Scholar] [CrossRef]
- Bukh, J.D.; Bock, C.; Vinberg, M.; Kessing, L.V. The Effect of Prolonged Duration of Untreated Depression on Antidepressant Treatment Outcome. J. Affect. Disord. 2013, 145, 42–48. [Google Scholar] [CrossRef]
- Hu, B.; Wang, J. Unmet Long-Term Care Needs and Depression: The Double Disadvantage of Community-Dwelling Older People in Rural China. Health Soc. Care Community 2019, 27, 126–138. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 7, Release version: 8.0.0.; SHARE-ERIC: Munich, Germany, 2022. [Google Scholar] [CrossRef]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8, Release version: 8.0.0.; SHARE-ERIC: Munich, Germany, 2022. [Google Scholar] [CrossRef]
- SHARE Wave 7 Methodology: Panel Innovations and Life Histories; Bergmann, M.; Scherpenzeel, A.; Börsch-Supan, A. (Eds.) MEA, Max Planck Institute for Social Law and Social Policy: Munich, Germany, 2019. [Google Scholar]
- SHARE Wave 8 Methodology: Collecting Cross-National Survey Data in Times of COVID-19; Bergmann, M.; Börsch-Supan, A. (Eds.) MEA, Max Planck Institute for Social Law and Social Policy: Munich, Germany, 2021. [Google Scholar]
- Prince, M.J.; Reischies, F.; Beekman, A.T.F.; Fuhrer, R.; Jonker, C.; Kivela, S.L.; Lawlor, B.A.; Lobo, A.; Magnusson, H.; Fichter, M.; et al. Development of the EURO–D Scale—A European Union Initiative to Compare Symptoms of Depression in 14 European Centres. Br. J. Psychiatry 1999, 174, 330–338. [Google Scholar] [CrossRef]
- Maskileyson, D.; Seddig, D.; Davidov, E. The EURO-D Measure of Depressive Symptoms in the Aging Population: Comparability Across European Countries and Israel. Front. Polit. Sci. 2021, 3, 90. [Google Scholar] [CrossRef]
- Fang, H.; Tu, S.; Sheng, J.; Shao, A. Depression in Sleep Disturbance: A Review on a Bidirectional Relationship, Mechanisms and Treatment. J. Cell. Mol. Med. 2019, 23, 2324–2332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ancoli-Israel, S. Sleep and Its Disorders in Aging Populations. Sleep Med. 2009, 10, S7–S11. [Google Scholar] [CrossRef]
- Crowley, K. Sleep and Sleep Disorders in Older Adults. Neuropsychol. Rev. 2011, 21, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, S.M.; Nietert, P.J.; Jenkins, R.G.; Litvin, C.B. The Prevalence of Chronic Diseases and Multimorbidity in Primary Care Practice: A PPRNet Report. J. Am. Board Fam. Med. 2013, 26, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Makovski, T.T.; Le Coroller, G.; Putrik, P.; Choi, Y.H.; Zeegers, M.P.; Stranges, S.; Castell, M.R.; Huiart, L.; Van Den Akker, M. Role of Clinical, Functional and Social Factors in the Association between Multimorbidity and Quality of Life: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). PLoS ONE 2020, 15, e0240024. [Google Scholar] [CrossRef] [PubMed]
- Read, J.R.; Sharpe, L.; Modini, M.; Dear, B.F. Multimorbidity and Depression: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2017, 221, 36–46. [Google Scholar] [CrossRef]
- Robine, J.M.; Jagger, C.; Egidi, V.; Gispert, R.; Nusselder, W.; Perenboom, R.; Rasmussen, N.; Ritchie, K.; Van den Berg, J.; Van Oyen, H. Creating a Coherent Set of Indicators to Monitor Health across Europe: The Euro-REVES 2 Project. Eur. J. Public Health 2003, 13, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2015. [Google Scholar]
- Markland, D. The Golden Rule Is That There Are No Golden Rules: A Commentary on Paul Barrett’s Recommendations for Reporting Model Fit in Structural Equation Modelling. Pers. Individ. Differ. 2007, 42, 851–858. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Yu, C.-Y. Evaluating Cutoff Criteria of Model Fit Indices for Latent Variable Models with Binary and Continuous Outcomes; University of California: Los Angeles, CA, USA, 2002. [Google Scholar]
- Barua, A.; Ghosh, M.K.; Kar, N.; Basilio, M.A. Socio-Demographic Factors of Geriatric Depression. Indian J. Psychol. Med. 2010, 32, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Böhm, K.; Schmid, A.; Götze, R.; Landwehr, C.; Rothgang, H. Five Types of OECD Healthcare Systems: Empirical Results of a Deductive Classification. Health Policy 2013, 113, 258–269. [Google Scholar] [CrossRef]
- Blazer, D.G.; Sachs-Ericsson, N.; Hybels, C.F. Perception of Unmet Basic Needs as a Predictor of Depressive Symptoms Among Community-Dwelling Older Adults. J. Gerontol. Ser. A 2007, 62, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Harb, N.; Foster, J.M.; Dobler, C.C. Patient-Perceived Treatment Burden of Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 1641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demain, S.; Gonçalves, A.C.; Areia, C.; Oliveira, R.; Marcos, A.J.; Marques, A.; Parmar, R.; Hunt, K. Living With, Managing and Minimising Treatment Burden in Long Term Conditions: A Systematic Review of Qualitative Research. PLoS ONE 2015, 10, e0125457. [Google Scholar] [CrossRef]
- Han, K.M.; Han, C.; Shin, C.; Jee, H.J.; An, H.; Yoon, H.K.; Ko, Y.H.; Kim, S.H. Social Capital, Socioeconomic Status, and Depression in Community-Living Elderly. J. Psychiatr. Res. 2018, 98, 133–140. [Google Scholar] [CrossRef]
- Xue, Y.; Lu, J.; Zheng, X.; Zhang, J.; Lin, H.; Qin, Z.; Zhang, C. The Relationship between Socioeconomic Status and Depression among the Older Adults: The Mediating Role of Health Promoting Lifestyle. J. Affect. Disord. 2021, 285, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Lasserre, A.M.; Imtiaz, S.; Roerecke, M.; Heilig, M.; Probst, C.; Rehm, J. Socioeconomic Status, Alcohol Use Disorders, and Depression: A Population-Based Study. J. Affect. Disord. 2022, 301, 331–336. [Google Scholar] [CrossRef]
- Zimmerman, F.J.; Katon, W. Socioeconomic Status, Depression Disparities, and Financial Strain: What Lies behind the Income-Depression Relationship? Health Econ. 2005, 14, 1197–1215. [Google Scholar] [CrossRef]
- Feral-Pierssens, A.L.; Claret, P.G.; Chouihed, T. Collateral Damage of the COVID-19 Outbreak: Expression of Concern. Eur. J. Emerg. Med. 2020, 233–234. [Google Scholar] [CrossRef]
- Smolić, Š.; Čipin, I.; Međimurec, P. Access to Healthcare for People Aged 50+ in Europe during the COVID-19 Outbreak. Eur. J. Ageing 2021, 1, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Eimontas, J.; Pakalniškienė, V.; Biliunaite, I.; Andersson, G. A Tailored Internet-Delivered Modular Intervention Based on Cognitive Behavioral Therapy for Depressed Older Adults: A Study Protocol for a Randomized Controlled Trial. Trials 2021, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | % (N) | Variable | % (N) |
|---|---|---|---|
| Didn’t see a doctor due to cost (lifetime) | 4.4 (1369) | House hold is able to make ends meet… | |
| Didn’t see a doctor due to long wait for appointment (lifetime) | 6.0 (1860) | … with great difficulty | 12.1 (3283) |
| Postponed dentist visit due to cost (lifetime) | 7.2 (2264) | … with some difficulty | 27.6 (7489) |
| Forgone taking medication due to cost (lifetime) | 2.7 (842) | … fairly easily | 29.5 (8003) |
| Forgone healthcare services due to cost (last 12 months) | 8.1 (3189) | … easily | 30.7 (8335) |
| Forgone healthcare services due to unavailability (last 12 months) | 6.5 (2572) | Reported limitations due to health problems (GALI) | 45.8 (18,066) |
| N | χ2 (df) | RMSEA [90% C.I.] | CFI | TLI | SRMR | |
|---|---|---|---|---|---|---|
| CFA (initial) | 44594 | 1747.914 *** (9) | 0.066 [0.063–0.068] | 0.906 | 0.843 | 0.113 |
| CFA (final) | 44594 | 72.800 *** (8) | 0.013 [0.011–0.016] | 0.996 | 0.993 | 0.022 |
| Model A | 44594 | 1152.452 *** (35) | 0.027 [0.025–0.028] | 0.965 | 0.946 | 0.049 |
| Model B (initial) | 39484 | 2850.845 *** (41) | 0.042 [0.040–0.043] | 0.908 | 0.858 | 0.073 |
| Model B (final) | 39484 | 1329.730 *** (40) | 0.029 [0.027–0.030] | 0.958 | 0.933 | 0.061 |
| Model C (initial) | 27110 | 5095.106 *** (46) | 0.064 [0.062–0.065] | 0.760 | 0.624 | 0.175 |
| Model C (final) | 27110 | 1040.496 *** (45) | 0.029 [0.027–0.030] | 0.953 | 0.924 | 0.057 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eimontas, J.; Gegieckaitė, G.; Zamalijeva, O.; Pakalniškienė, V. Unmet Healthcare Needs Predict Depression Symptoms among Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 8892. https://doi.org/10.3390/ijerph19158892
Eimontas J, Gegieckaitė G, Zamalijeva O, Pakalniškienė V. Unmet Healthcare Needs Predict Depression Symptoms among Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(15):8892. https://doi.org/10.3390/ijerph19158892
Chicago/Turabian StyleEimontas, Jonas, Goda Gegieckaitė, Olga Zamalijeva, and Vilmantė Pakalniškienė. 2022. "Unmet Healthcare Needs Predict Depression Symptoms among Older Adults" International Journal of Environmental Research and Public Health 19, no. 15: 8892. https://doi.org/10.3390/ijerph19158892
APA StyleEimontas, J., Gegieckaitė, G., Zamalijeva, O., & Pakalniškienė, V. (2022). Unmet Healthcare Needs Predict Depression Symptoms among Older Adults. International Journal of Environmental Research and Public Health, 19(15), 8892. https://doi.org/10.3390/ijerph19158892