
Socioeconomic Status and Distance to Reference Centers for Complex Cancer Diseases: A Source of Health Inequalities? A Population Cohort Study Based on Catalonia (Spain)

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Healthcare Setting
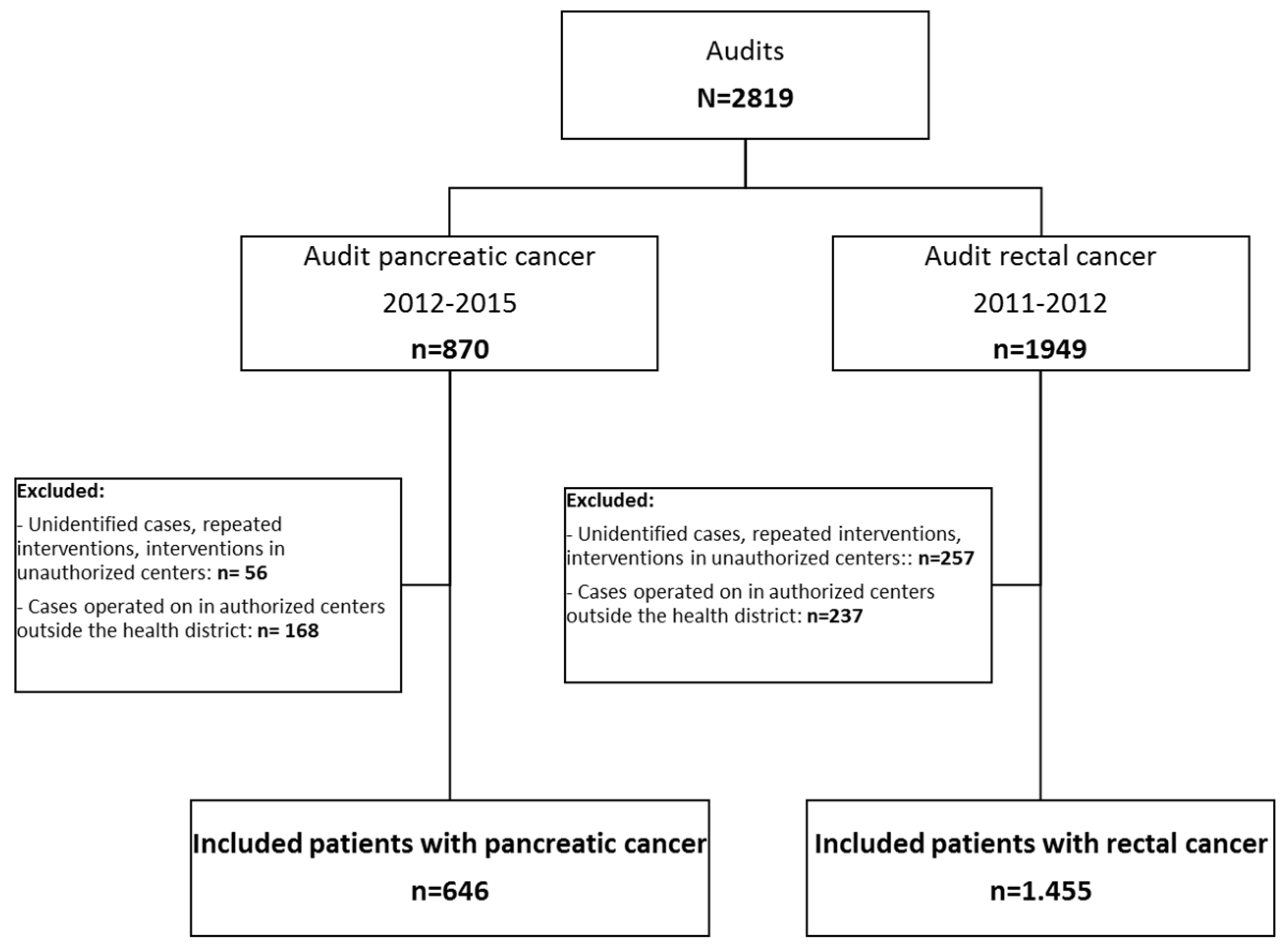
2.2. Study Design
2.3. Population
2.4. Variables
- Absence of emergency admission;
- Length of hospital stay not exceeding the 75th percentile;
- No reintervention within 90 days of the first surgical treatment;
- Lack of postsurgical complication within 30 days of the first surgical treatment;
- Radical resection (pancreas: R0; rectum: total mesorectal excision).
2.5. Statistical Analyses
3. Results
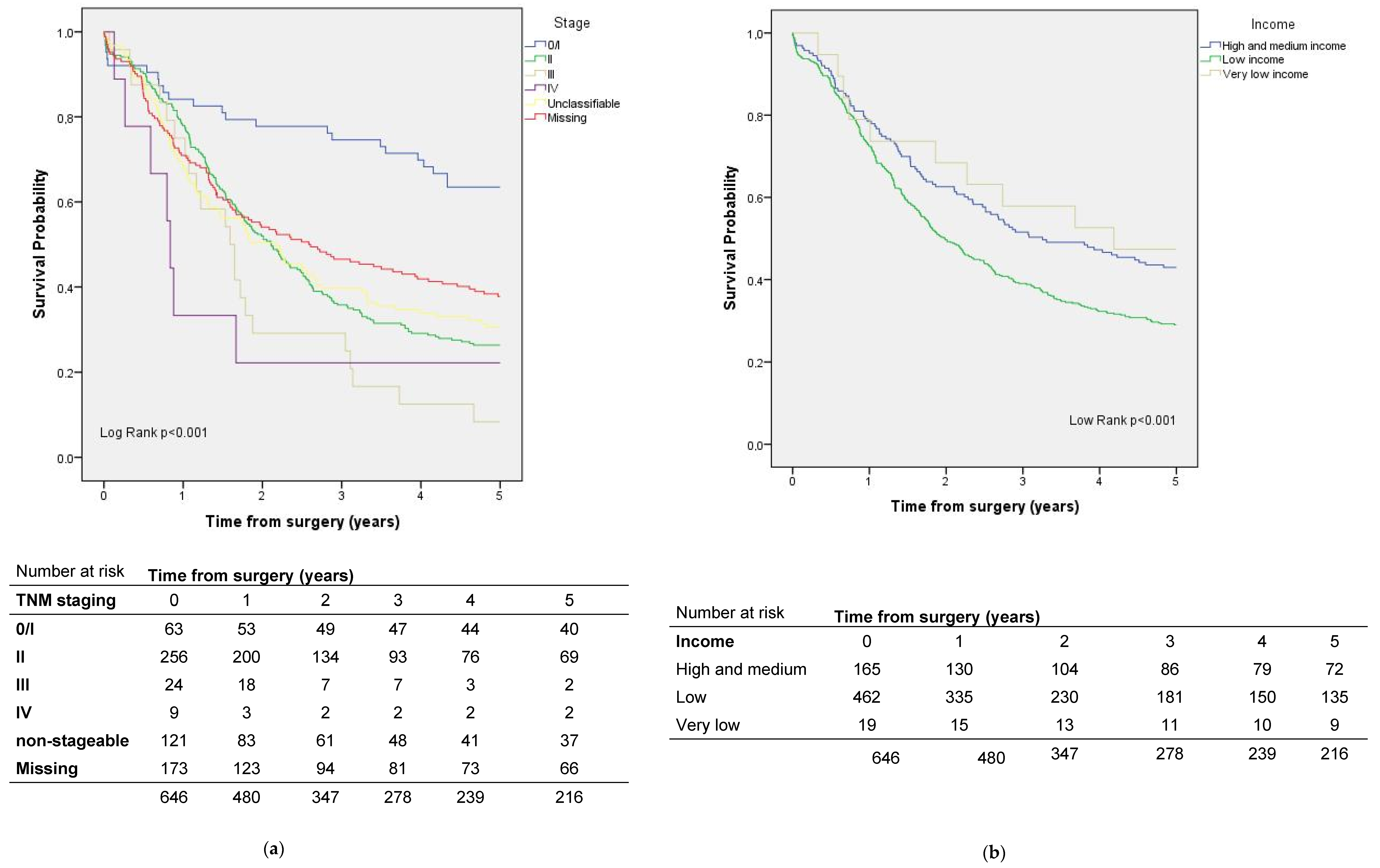
3.1. Factors Influencing Survival in Patients with Pancreatic Cancer
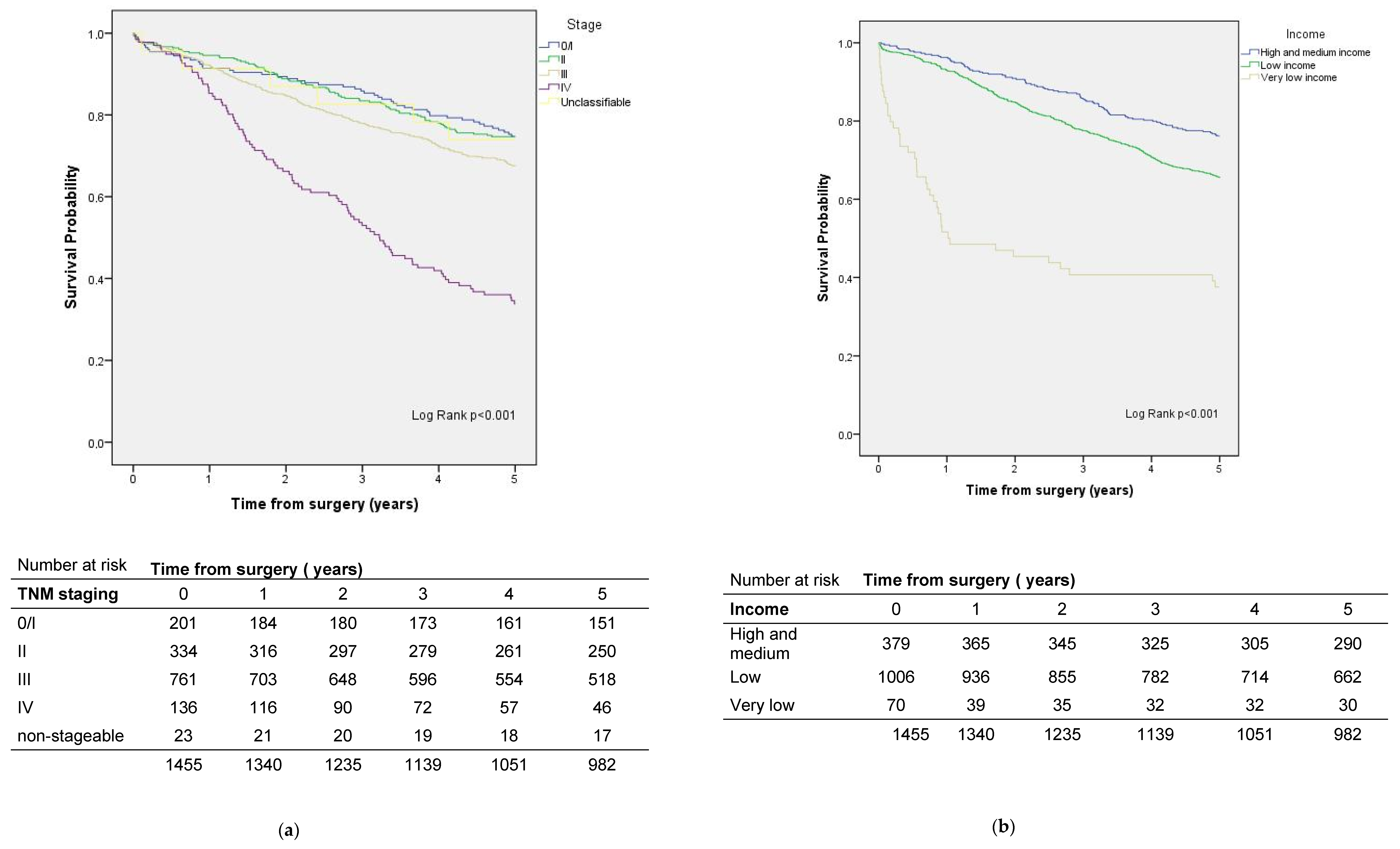
3.2. Factors That Influence Survival in Patients with Rectal Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Institute of Medicine (U.S.); Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Stitzenberg, K.B.; Sigurdson, E.R.; Egleston, B.L.; Starkey, R.B.; Meropol, N.J. Centralization of cancer surgery: Implications for patient access to optimal care. J. Clin. Oncol. 2009, 27, 4671–4678. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Pickle, L.W.; Stinchcomb, D.; Feuer, E.J. Detection of spatial clusters: Application to cancer survival as a continuous outcome. Epidemiology 2007, 18, 73–87. [Google Scholar] [CrossRef]
- Meilleur, A.; Subramanian, S.V.; Plascak, J.J.; Fisher, J.L.; Paskett, E.D.; Lamont, E.B. Rural residence and cancer outcomes in the United States: Issues and challenges. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1657–1667. [Google Scholar] [CrossRef] [Green Version]
- Coll-Ortega, C.; Prades, J.; Manchon-Walsh, P.; Borras, J.M. Centralisation of surgery for complex cancer diseases: A scoping review of the evidence base on pancreatic cancer. J. Cancer Policy 2022, 32, 100334. [Google Scholar] [CrossRef]
- Vonlanthen, R.; Lodge, P.; Barkun, J.S.; Farges, O.; Rogiers, X.; Soreide, K.; Kehlet, H.; Reynolds, J.V.; Käser, S.A.; Naredi, P.; et al. Toward a Consensus on Centralization in Surgery. Ann. Surg. 2018, 268, 712–724. [Google Scholar] [CrossRef] [Green Version]
- Bendzsak, A.M.; Baxter, N.N.; Darling, G.E.; Austin, P.C. Urbach DR Regionalization and outcomes of lung cancer surgery in Ontario, Canada. J. Clin. Oncol. 2017, 35, 2772–2780. [Google Scholar] [CrossRef] [Green Version]
- Timmermans, M.; Schuurman, M.S.; Ho, V.K.Y.; Massuger, L.F.; Nijman, H.W.; van Gorp, T.; Sonke, G.S.; Kruitwagen, R.F.P.M.; van der Aa, M.A. Centralization of ovarian cancer in the Netherlands: Hospital of diagnosis no longer determines patients’ probability of undergoing surgery. Gynecol Oncol. 2018, 148, 56–61. [Google Scholar] [CrossRef]
- Prades, J.; Arnold, D.; Brunner, T.; Cardone, A.; Carrato, A.; Coll-Ortega, C.; de Luze, S.; Garel, P.; Goossens, M.E.; Grilli, R.; et al. Bratislava Statement: Consensus recommendations for improving pancreatic cancer care. ESMO Open. 2020, 5, e001051. [Google Scholar] [CrossRef]
- Andritsch, E.; Beishon, M.; Bielack, S.; Bonvalot, S.; Casali, P.G.; Crul, M.; Delgado-Bolton, R.; Donati, D.M.; Douis, H.; Haas, R.; et al. ECCO Essential Requirements for Quality Cancer Care: Soft Tissue Sarcoma in Adults and Bone Sarcoma. A critical review. Crit. Rev. Oncol. Hematol. 2017, 110, 94–105. [Google Scholar] [CrossRef]
- Biganzoli, L.; Cardoso, F.; Beishon, M.; Cameron, D.; Cataliotti, L.; Coles, C.E.; Bolton, R.C.D.; Trill, M.D.; Erdem, S.; Fjell, M.; et al. The requirements of a specialist breast centre. Breast 2020, 51, 65–84. [Google Scholar] [CrossRef]
- Dejardin, O.; Jones, A.; Rachet, B.; Morris, E.; Bouvier, V.; Jooste, V.; Coombes, E.; Forman, D.; Bouvier, A.; Launoy, G. The influence of geographical access to health care and material deprivation on colorectal cancer survival: Evidence from France and England. Health Place 2014, 30, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Crawford, S.M.; Sauerzapf, V.; Haynes, R.; Zhao, H.; Forman, D.; Jones, A.P. Social and geographical factors affecting access to treatment of lung cancer. Br. J. Cancer 2009, 101, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Baade, P.D.; Dasgupta, P.; Aitken, J.F.; Turrell, G. Distance to the closest radiotherapy facility and survival after a diagnosis of rectal cancer in Queensland. Med. J. Aust. 2011, 195, 350–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prades, J.; Manchon-Walsh, P.; Solà, J.; Espinàs, J.A.; Guarga, A.; Borras, J.M. Improving clinical outcomes through centralization of rectal cancer surgery and clinical audit: A mixed-methods assessment. Eur. J. Public Health 2016, 26, 538–542. [Google Scholar] [CrossRef] [Green Version]
- Highly-Specialised Cancer Care Reorganisation Act, Catalan Health Service § 01/2019. 2019. Available online: https://scientiasalut.gencat.cat/bitstream/handle/11351/1323.3/catsalut_instruccio_01_2019.pdf?sequence=8&isAllowed=y (accessed on 15 January 2022).
- Urbanos-Garrido, R. La desigualdad en el acceso a las prestaciones sanitarias. Propuestas para lograr la equidad [Inequality in access to health care services. Policy recommendations aimed at achieving equity]. Gac. Sanit. 2016, 30 (Suppl. 1), 25–30. [Google Scholar] [CrossRef] [Green Version]
- Woods, L.M.; Rachet, B.; Coleman, M.P. Origins of socio-economic inequalities in cancer survival: A review. Ann Oncol. 2006, 17, 5–19. [Google Scholar] [CrossRef]
- Manchon-Walsh, P.; Espinàs, J.A.; Prades, J.; Aliste, L.; Pozuelo, A.; Benaque Guarga, A.; Borras, J.M. Evaluation of the Concentration Process of Highly Specialized Digestive Oncological Surgery in Catalonia; Catalan Agency for Health Information, Assessment and Quality (CAHIAQ): Barcelona, Spain, 2016. [Google Scholar]
- Manchon-Walsh, P.; Espinàs, J.A.; Prades, J.; Torrents, A.; Aliste, L.; Pozuelo, A.; Casanovas-Guitart, C.; Guarga, A.; Borras, J.M. Evaluation of the Concentration Process of Highly Specialized Digestive Oncological Surgery in Catalonia. Update 2014–2015; Catalan Agency for Health Information, Assessment and Quality (CAHIAQ): Barcelona, Spain, 2018. [Google Scholar]
- Kalff, M.C.; Vesseur, I.; Eshuis, W.J.; Heineman, D.J.; Daams, F.; van der Peet, D.L.; van Berge Henegouwen, M.I.; Gisbertz, S.S. The Association of Textbook Outcome and Long-Term Survival After Esophagectomy for Esophageal Cancer. Ann. Thorac. Surg. 2020, 112, 1134–1141. [Google Scholar] [CrossRef]
- Yang, C.C.; Tian, Y.F.; Liu, W.S.; Chou, C.L.; Cheng, L.C.; Chu, S.S.; Lee, C.C. The association between the composite quality measure “textbook outcome” and long term survival in operated colon cancer. Medicine 2020, 99, e22447. [Google Scholar] [CrossRef]
- Bilal, U.; Cainzos-Achirica, M.; Cleries, M.; Santaeugènia, S.; Corbella, X.; Comin-Colet, J.; Vela, E. Socioeconomic status, life expectancy and mortality in a universal healthcare setting: An individual-level analysis of >6 million Catalan residents. Prev. Med. 2019, 123, 91–94. [Google Scholar] [CrossRef]
- Fonseca, B.D.P.; Albuquerque, P.C.; Saldanha, R.D.F.; Zicker, F. Geographic accessibility to cancer treatment in Brazil: A network analysis. Lancet Reg. Heal. Am. 2022, 7, 100153. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Siewers, A.E.; Marth, N.J.; Goodman, D.C. Regionalization of high-risk surgery and implications for patient travel times. JAMA 2003, 290, 2703–2708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speicher, P.J.; Englum, B.; Ganapathi, A.; Wang, X.; Hartwig, M.G.; D’Amico, T.A.; Berry, M.F. Traveling to a High-volume Center is Associated With Improved Survival for Patients With Esophageal Cancer. Ann Surg. 2017, 265, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Baastrup, R.; Sørensen, M.; Hansen, J.; Hansen, R.D.; Würtzen, H.; Winther, J.F. Social inequality and incidence of and survival from cancers of the oesophagus, stomach and pancreas in a population-based study in Denmark, 1994–2003. Eur. J. Cancer 2008, 44, 1962–1977. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S. Social determinants of colorectal cancer risk, stage, and survival: A systematic review. Int. J. Color. Dis. 2020, 35, 985–995. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Europe’s Beating Cancer Plan. Communication from the Commission to the European Parliament and the Council. COM(2021)44. Available online: https://ec.europa.eu/health/system/files/2022-02/eu_cancer-plan_en_0.pdf (accessed on 12 February 2021).
- Parry, M.G.; Sujenthiran, A.; Cowling, T.E.; Nossiter, J.; Cathcart, P.; Clarke, N.W.; Payne, H.; Aggarwal, A.; van der Meulen, J. Impact of cancer service centralisation on the radical treatment of men with high-risk and locally advanced prostate cancer: A national cross-sectional analysis in England. Int. J. Cancer 2019, 145, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Versteeg, S.E.; Ho, V.K.Y.; Siesling, S.; Varkevisser, M. Centralisation of cancer surgery and the impact on patients’ travel burden. Int. J. Cancer 2018, 145, 40–48. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pancreatic Cancer (N = 646) | Rectal Cancer (N = 1455) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Sex | ||||
| Male | 379 | 58.7 | 947 | 65.1 |
| Female | 267 | 41.3 | 508 | 34.9 |
| Age | ||||
| Median (IQR) | 69.0 (14.0) | 69.6 (16.9) | ||
| <60 years | 141 | 21.8 | 311 | 21.4 |
| 60–69 years | 206 | 31.9 | 423 | 29.1 |
| 70–79 years | 227 | 35.1 | 459 | 31.5 |
| ≥80 years | 72 | 11.1 | 262 | 18.0 |
| Physical status score | ||||
| ASA I | 17 | 2.6 | 89 | 6.1 |
| ASA II | 168 | 26.0 | 738 | 50.7 |
| ASA III | 162 | 25.1 | 486 | 33.4 |
| ASA IV | 13 | 2.0 | 49 | 3.4 |
| Missing | 286 | 44.3 | 93 | 6.4 |
| TNM staging | ||||
| 0/I | 63 | 9.8 | 201 | 13.8 |
| II | 256 | 39.6 | 334 | 23.0 |
| III | 24 | 3.7 | 761 | 52.3 |
| IV | 9 | 1.4 | 136 | 9.3 |
| Non-stageable | 121 | 18.7 | 23 | 1.6 |
| Missing | 173 | 26.8 | 0 | 0.0 |
| Income | ||||
| High–medium | 165 | 25.5 | 379 | 26.0 |
| Low | 462 | 71.5 | 1006 | 69.1 |
| Very low | 19 | 2.9 | 70 | 4.8 |
| Distance from patient residence to reference center (km) | ||||
| Median (IQR) Range | 7.00 (32.83) 0.53–246.07 | 4.37 (8.89) 0.18–134.86 | ||
| 0–10 km | 380 | 58.8 | 1040 | 71.5 |
| >10 km to < 90th% * | 202 | 31.3 | 273 | 18.8 |
| ≥90th% * | 64 | 9.9 | 142 | 9.8 |
| District hospital | ||||
| Non-reference center | 273 | 42.3 | 183 | 12.6 |
| Reference center | 373 | 57.7 | 1272 | 87.4 |
| Pancreatic Cancer (N = 646) Rectal Cancer (N = 1455) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–10 km | >10 km to <90th% | ≥90th% | 0–10 km | >10 km to <90th% | ≥90th% | ||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| Age | <60 years | 84 | 22.1 | 42 | 20.8 | 15 | 23.4 | 208 | 20.0 | 70 | 25.6 | 33 | 23.2 |
| 60–69 years | 113 | 29.7 | 70 | 34.7 | 23 | 35.9 | 300 | 28.8 | 84 | 30.8 | 39 | 27.5 | |
| 70–79 years | 134 | 35.3 | 74 | 36.6 | 19 | 29.7 | 333 | 32.0 | 76 | 27.8 | 50 | 35.2 | |
| ≥80 years | 49 | 12.9 | 16 | 7.9 | 7 | 10.9 | 199 | 19.1 | 43 | 15.8 | 20 | 14.1 | |
| p-value | 0.52 | 0.21 | |||||||||||
| Physical status score | ASA I | 9 | 2.4 | 5 | 2.5 | 3 | 4.7 | 62 | 6.0 | 19 | 7.0 | 8 | 5.6 |
| ASA II | 105 | 27.6 | 45 | 22.3 | 18 | 28.1 | 540 | 51.9 | 131 | 48.0 | 67 | 47.2 | |
| ASA III | 86 | 22.6 | 64 | 31.7 | 12 | 18.8 | 346 | 33.3 | 88 | 32.2 | 52 | 36.6 | |
| ASA IV | 9 | 2.4 | 3 | 1.5 | 1 | 1.6 | 38 | 3.7 | 5 | 1.8 | 6 | 4.2 | |
| ASA V | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Missing | 171 | 45.0 | 85 | 42.1 | 30 | 46.9 | 54 | 5.2 | 30 | 11.0 | 9 | 6.3 | |
| p-value | 0.33 | 0.044 * | |||||||||||
| Tumor stage | 0/I | 46 | 12.1 | 12 | 5.9 | 5 | 7.8 | 151 | 14.5 | 30 | 11.0 | 20 | 14.1 |
| II | 142 | 37.4 | 87 | 43.1 | 27 | 42.2 | 244 | 23.5 | 62 | 22.7 | 28 | 19.7 | |
| III | 16 | 4.2 | 8 | 4.0 | 0 | 0.0 | 538 | 51.7 | 147 | 53.8 | 76 | 53.5 | |
| IV | 7 | 1.8 | 1 | 0.5 | 1 | 1.6 | 87 | 8.4 | 31 | 11.4 | 18 | 12.7 | |
| Non-stageable | 69 | 18.2 | 41 | 20.3 | 11 | 17.2 | 20 | 1.9 | 3 | 1.1 | 0 | 0.0 | |
| Missing | 100 | 26.3 | 53 | 26.2 | 20 | 31.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| p-value | 0.29 | 0.24 | |||||||||||
| Income | High-medium | 108 | 28.4 | 41 | 20.3 | 16 | 25.0 | 291 | 28.0 | 63 | 23.1 | 25 | 17.6 |
| Low | 258 | 67.9 | 158 | 78.2 | 46 | 71.9 | 697 | 67.0 | 199 | 72.9 | 110 | 77.5 | |
| Very low | 14 | 3.7 | 3 | 1.5 | 2 | 3.1 | 52 | 5.0 | 11 | 4.0 | 7 | 4.9 | |
| p-value | 0.11 | 0.052 | |||||||||||
| Total | 380 | 100.0 | 202 | 100.0 | 64 | 100.0 | 1040 | 100.0 | 273 | 100.0 | 142 | 100.0 | |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | n | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Sex | |||||||
| Male | 379 | 1 | 1 | ||||
| Female | 267 | 0.97 | 0.80, 1.77 | 0.79 | 0.87 | 0.71, 1.06 | 0.71 |
| Age | |||||||
| <60 years | 141 | 1 | <0.001 | 1 | 0.008 | ||
| 60–69 years | 206 | 1.52 | 1.15, 2.02 | 0.004 | 1.37 | 1.02, 1.84 | 0.034 |
| 70–79 years | 227 | 1.75 | 1.33, 2.31 | <0.001 | 1.53 | 1.15, 2.05 | 0.004 |
| ≥80 years | 72 | 2.02 | 1.42, 2.86 | <0.001 | 1.82 | 1.25, 2.65 | 0.002 |
| Physical status score | |||||||
| ASA I | 17 | 1 | 0.014 | 1 | 0.067 | ||
| ASA II | 168 | 2.18 | 0.96, 4.97 | 0.064 | 1.75 | 0.76, 4.04 | 0.19 |
| ASA III | 162 | 2.97 | 1.31, 6.76 | 0.009 | 2.02 | 0.87, 4.70 | 0.10 |
| ASA IV | 13 | 3.21 | 1.17, 8.85 | 0.024 | 2.31 | 0.82, 6.48 | 0.11 |
| Missing | 286 | 2.85 | 1.26, 6.42 | 0.012 | 2.93 | 1.20, 7.19 | 0.019 |
| TNM staging | |||||||
| 0/I | 63 | 1 | <0.001 | 1 | <0.001 | ||
| II | 256 | 2.78 | 1.80, 4.30 | <0.001 | 2.84 | 1.82, 4.42 | <0.001 |
| III | 24 | 4.22 | 2.35, 7.59 | <0.001 | 3.37 | 1.86, 6.12 | <0.001 |
| IV | 9 | 4.59 | 1.97, 10.71 | <0.001 | 4.52 | 1.80, 11.33 | 0.001 |
| Non-stageable | 121 | 2.68 | 1.69, 4.25 | <0.001 | 1.70 | 0.96, 3.03 | 0.070 |
| Missing | 173 | 2.24 | 1.43, 3.51 | <0.001 | 1.60 | 0.94, 2.72 | 0.083 |
| Textbook outcome | |||||||
| Yes | 284 | 1 | 1 | ||||
| No | 362 | 1.48 | 1.22, 1.79 | <0.001 | 1.344 | 1.10, 1.64 | 0.004 |
| Distance from patient home to reference center | |||||||
| 0–10 km | 380 | 1 | 0.90 | 1 | 0.92 | ||
| 11 km to <90th% | 202 | 1.04 | 0.84, 1.28 | 0.74 | 1.05 | 0.80, 1.39 | 0.71 |
| ≥90th% | 64 | 0.96 | 0.70, 1.33 | 0.81 | 1.08 | 0.72, 1.61 | 0.73 |
| Income | |||||||
| High–medium | 165 | 1 | 0.003 | 1 | 0.003 | ||
| Low | 462 | 1.45 | 1.15, 1.82 | 0.002 | 1.47 | 1.15, 1.87 | 0.002 |
| Very low | 19 | 0.87 | 0.45, 1.67 | 0.678 | 0.84 | 0.43, 1.63 | 0.60 |
| District center | |||||||
| Non-reference center | 273 | 1 | 1 | ||||
| Reference center | 373 | 1.03 | 0.85, 1.25 | 0.75 | 1.14 | 0.86, 1.50 | 0.362 |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | n | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Sex | |||||||
| Male | 947 | 1 | 1 | ||||
| Female | 508 | 0.96 | 0.79, 1.16 | 0.64 | 0.95 | 0.78, 1.15 | 0.59 |
| Age | |||||||
| <60 years | 311 | 1 | <0.001 | 1 | <0.001 | ||
| 60–69 years | 423 | 1.07 | 0.78, 1.45 | 0.69 | 1.17 | 0.86, 1.61 | 0.32 |
| 70–79 years | 459 | 1.79 | 1.35, 2.37 | <0.001 | 1.85 | 1.38, 2.49 | <0.001 |
| ≥80 years | 262 | 2.87 | 2.15, 3.84 | <0.001 | 3.33 | 2.43, 4.57 | <0.001 |
| Physical status score | |||||||
| ASA I | 89 | 1 | <0.001 | 1 | <0.001 | ||
| ASA II | 738 | 1.43 | 0.86, 2.38 | 0.17 | 1.15 | 0.68, 1.95 | 0.60 |
| ASA III | 486 | 2.74 | 1.65, 4.56 | <0.001 | 1.96 | 1.16, 3.34 | 0.013 |
| ASA IV | 49 | 5.28 | 2.90, 9.63 | <0.001 | 3.73 | 1.98, 7.01 | <0.001 |
| Missing | 93 | 3.15 | 1.78, 5.60 | <0.001 | 2.35 | 1.30, 4.26 | 0.005 |
| TNM staging | |||||||
| 0/I | 201 | 1 | <0.001 | 1 | <0.001 | ||
| II | 334 | 1.01 | 0.71, 1.43 | 0.97 | 1.04 | 0.73, 1.48 | 0.81 |
| III | 761 | 1.36 | 1.00, 1.85 | 0.047 | 1.72 | 1.26, 2.34 | 0.001 |
| IV | 136 | 3.61 | 2.55, 5.10 | <0.001 | 4.77 | 3.34, 6.81 | <0.001 |
| Non-stageable | 23 | 1.05 | 0.45, 2.45 | 0.91 | 0.85 | 0.36, 1.99 | 0.70 |
| Textbook outcome | |||||||
| Yes | 529 | 1 | 1 | ||||
| No | 926 | 1.58 | 1.30, 1.93 | <0.001 | 1.46 | 1.20, 1.79 | <0.001 |
| Distance from patient home to reference center | |||||||
| 0–10 km | 1040 | 1 | 0.70 | 1 | 0.044 | ||
| 11 km to <90th% | 273 | 1.09 | 0.87, 1.37 | 0.47 | 1.08 | 0.84, 1.38 | 0.55 |
| ≥90th% | 142 | 0.95 | 0.70, 1.30 | 0.75 | 0.67 | 0.46, 0.97 | 0.034 |
| Income | |||||||
| High–medium | 379 | 1 | <0.001 | 1 | <0.001 | ||
| Low | 1006 | 1.55 | 1.23, 1.96 | <0.001 | 1.28 | 1.00, 1.63 | 0.047 |
| Very low | 70 | 4.69 | 3.23, 6.81 | <0.001 | 5.24 | 3.58, 7.67 | <0.001 |
| District center | |||||||
| Non-reference center | 183 | 1 | 1 | ||||
| Reference center | 1272 | 0.78 | 0.61, 1.01 | 0.058 | 0.76 | 0.55, 1.04 | 0.081 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manchon-Walsh, P.; Aliste, L.; Borràs, J.M.; Coll-Ortega, C.; Casacuberta, J.; Casanovas-Guitart, C.; Clèries, M.; Cruz, S.; Guarga, À.; Mompart, A.; et al. Socioeconomic Status and Distance to Reference Centers for Complex Cancer Diseases: A Source of Health Inequalities? A Population Cohort Study Based on Catalonia (Spain). Int. J. Environ. Res. Public Health 2022, 19, 8814. https://doi.org/10.3390/ijerph19148814
Manchon-Walsh P, Aliste L, Borràs JM, Coll-Ortega C, Casacuberta J, Casanovas-Guitart C, Clèries M, Cruz S, Guarga À, Mompart A, et al. Socioeconomic Status and Distance to Reference Centers for Complex Cancer Diseases: A Source of Health Inequalities? A Population Cohort Study Based on Catalonia (Spain). International Journal of Environmental Research and Public Health. 2022; 19(14):8814. https://doi.org/10.3390/ijerph19148814
Chicago/Turabian StyleManchon-Walsh, Paula, Luisa Aliste, Josep M. Borràs, Cristina Coll-Ortega, Joan Casacuberta, Cristina Casanovas-Guitart, Montse Clèries, Sergi Cruz, Àlex Guarga, Anna Mompart, and et al. 2022. "Socioeconomic Status and Distance to Reference Centers for Complex Cancer Diseases: A Source of Health Inequalities? A Population Cohort Study Based on Catalonia (Spain)" International Journal of Environmental Research and Public Health 19, no. 14: 8814. https://doi.org/10.3390/ijerph19148814
APA StyleManchon-Walsh, P., Aliste, L., Borràs, J. M., Coll-Ortega, C., Casacuberta, J., Casanovas-Guitart, C., Clèries, M., Cruz, S., Guarga, À., Mompart, A., Planella, A., Pozuelo, A., Ticó, I., Vela, E., & Prades, J. (2022). Socioeconomic Status and Distance to Reference Centers for Complex Cancer Diseases: A Source of Health Inequalities? A Population Cohort Study Based on Catalonia (Spain). International Journal of Environmental Research and Public Health, 19(14), 8814. https://doi.org/10.3390/ijerph19148814