
Risk Factors for Lung Cancer in the Province of Lecce: Results from the PROTOS Case–Control Study in Salento (Southern Italy)

 ,
,  ,
,  ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Recruitment
2.2. Questionnaire
2.3. Exposure Assessment
2.3.1. Exposure to Tobacco Smoking
2.3.2. Exposure Assessment to Industrial Plants and Occupational Factors
2.3.3. Exploratory Analysis to Assess Radon Exposure
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. Descriptive and Multiple Regression Analyses
3.2. Sensitivity Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrales, L.; Rosell, R.; Cardona, A.F.; Martín, C.; Zatarain-Barrón, Z.L.; Arrieta, O. Lung Cancer in Never Smokers: The Role of Different Risk Factors Other than Tobacco Smoking. Crit. Rev. Oncol. Hematol. 2020, 148, 102895. [Google Scholar] [CrossRef] [PubMed]
- Trama, A.; Boffi, R.; Contiero, P.; Buzzoni, C.; Pacifici, R.; Mangone, L. AIRTUM Working Group Trends in Lung Cancer and Smoking Behavior in Italy: An Alarm Bell for Women. Tumori J. 2017, 103, 543–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lortet-Tieulent, J.; Soerjomataram, I.; Ferlay, J.; Rutherford, M.; Weiderpass, E.; Bray, F. International Trends in Lung Cancer Incidence by Histological Subtype: Adenocarcinoma Stabilizing in Men but Still Increasing in Women. Lung Cancer 2014, 84, 13–22. [Google Scholar] [CrossRef]
- Jemal, A.; Miller, K.D.; Ma, J.; Siegel, R.L.; Fedewa, S.A.; Islami, F.; Devesa, S.S.; Thun, M.J. Higher Lung Cancer Incidence in Young Women Than Young Men in the United States. N. Engl. J. Med. 2018, 378, 1999–2009. [Google Scholar] [CrossRef]
- Fidler-Benaoudia, M.M.; Torre, L.A.; Bray, F.; Ferlay, J.; Jemal, A. Lung Cancer Incidence in Young Women vs. Young Men: A Systematic Analysis in 40 Countries. Int. J. Cancer 2020, 147, 811–819. [Google Scholar] [CrossRef]
- Dubin, S.; Griffin, D. Lung Cancer in Non-Smokers. Mo. Med. 2020, 117, 375–379. [Google Scholar]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [Green Version]
- Akhtar, N.; Bansal, J.G. Risk Factors of Lung Cancer in Nonsmoker. Curr. Probl. Cancer 2017, 41, 328–339. [Google Scholar] [CrossRef]
- Coté, M.L.; Liu, M.; Bonassi, S.; Neri, M.; Schwartz, A.G.; Christiani, D.C.; Spitz, M.R.; Muscat, J.E.; Rennert, G.; Aben, K.K.; et al. Increased Risk of Lung Cancer in Individuals with a Family History of the Disease: A Pooled Analysis from the International Lung Cancer Consortium. Eur. J. Cancer Clin. Oncol. 2012, 48, 1957–1968. [Google Scholar] [CrossRef] [PubMed]
- Yue, S.; Wang, Y.; Wang, J.; Chen, J. Relationships between Lung Cancer Incidences and Air Pollutants. Technol. Health Care 2017, 25, 411–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. 9 Out of 10 People Worldwide Breathe Polluted Air, but More Countries are Taking Action; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Liu, X.; Mubarik, S.; Wang, F.; Yu, Y.; Wang, Y.; Shi, F.; Wen, H.; Yu, C. Lung Cancer Death Attributable to Long-Term Ambient Particulate Matter (PM2.5) Exposure in East Asian Countries During 1990–2019. Front. Med. 2021, 8, 742076. [Google Scholar] [CrossRef] [PubMed]
- Collarile, P.; Bidoli, E.; Barbone, F.; Zanier, L.; Del Zotto, S.; Fuser, S.; Stel, F.; Panato, C.; Gallai, I.; Serraino, D. Residence in Proximity of a Coal-Oil-Fired Thermal Power Plant and Risk of Lung and Bladder Cancer in North-Eastern Italy. A Population-Based Study: 1995–2009. Int. J. Env. Res. Public Health 2017, 14, 860. [Google Scholar] [CrossRef] [Green Version]
- Ielpo, P.; Mangia, C.; Marra, G.P.; Comite, V.; Rizza, U.; Uricchio, V.F.; Fermo, P. Outdoor Spatial Distribution and Indoor Levels of NO2 and SO2 in a High Environmental Risk Site of the South Italy. Sci. Total Environ. 2019, 648, 787–797. [Google Scholar] [CrossRef]
- Shankar, A.; Dubey, A.; Saini, D.; Singh, M.; Prasad, C.P.; Roy, S.; Bharati, S.J.; Rinki, M.; Singh, N.; Seth, T.; et al. Environmental and Occupational Determinants of Lung Cancer. Transl. Lung Cancer Res. 2019, 8, S31–S49. [Google Scholar] [CrossRef]
- de Groot, P.; Munden, R.F. Lung Cancer Epidemiology, Risk Factors, and Prevention. Radiol. Clin. North Am. 2012, 50, 863–876. [Google Scholar] [CrossRef]
- Klebe, S.; Leigh, J.; Henderson, D.W.; Nurminen, M. Asbestos, Smoking and Lung Cancer: An Update. Int. J. Environ. Res. Public Health 2019, 17, 258. [Google Scholar] [CrossRef] [Green Version]
- IARC. Alcohol Consumption and Ethyl Carbamate; WHO Press: Geneva, Switzerland, 2010; Volume 96, ISBN 978-92-832-1296-6. [Google Scholar]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol Consumption and Site-Specific Cancer Risk: A Comprehensive Dose-Response Meta-Analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef]
- Troche, J.R.; Mayne, S.T.; Freedman, N.D.; Shebl, F.M.; Abnet, C.C. The Association between Alcohol Consumption and Lung Carcinoma by Histological Subtype. Am. J. Epidemiol. 2016, 183, 110–121. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.S.; Wong, M.Y.; Vogtmann, E.; Tang, R.Q.; Xie, L.; Yang, Y.S.; Wu, Q.J.; Zhang, W.; Xiang, Y.B. Meat Consumption and Risk of Lung Cancer: Evidence from Observational Studies. Ann. Oncol. 2012, 23, 3163–3170. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Kubo, J.; Luo, J.; Desai, M.; Hedlin, H.; Henderson, M.; Chlebowski, R.; Tindle, H.; Chen, C.; Gomez, S.; et al. Active and Passive Smoking in Relation to Lung Cancer Incidence in the Women’s Health Initiative Observational Study Prospective Cohort. Ann. Oncol. 2015, 26, 221–230. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C. Epidemiologia e prevenzione del cancro (I). Med. Syst. 1991, 57, 1–75. [Google Scholar]
- OER Puglia (O.E.R.P.). Tavole Della Mortalità in Puglia, Anni 2001–2011; O.E.R.P.: Toronto, ON, Canada, 2013. [Google Scholar]
- Vigotti, M.A.; Montinari, M.R.; Gianicolo, E.A.L. Mortality Trend in Apulia Provinces, Italy, 1949–2008. In Proceedings of the Environment and Health Bridging South North, East and West, Basel, Switzerland, 19 August 2013; p. 749. [Google Scholar]
- RTP. Rapporto Tumori 2015; RTP: Tak, Thailand, 2015. [Google Scholar]
- OER Puglia. Sistema di Sorveglianza PASSI-Rapporto Regione Puglia 2008 e Primo Semestre 2009; OER Puglia: Toronto, ON, Canada, 2011. [Google Scholar]
- Minelli, G.; Melcarne, A.; Fazzo, L.; Quarta, F.; Golizia, M.; De Maria, V.; Rashid, I.; Comba, P.; Conti, S. Il tumore polmonare nella Provincia di Lecce: Analisi di Cluster di incidenza e mortalità. In Proceedings of the “XVIII Convegno Annuale AIRTUM 2014”, Taranto, Italy, 9–11 April 2014; Available online: https://www.scribd.com/document/217461724/XVIII-Convegno-annuale-AIRTUM-Taranto-9-11-aprile-2014-Atti-Definitivo-Web (accessed on 21 June 2022).
- Kuo, P.-H.; Tsuang, B.-J.; Chen, C.-J.; Hu, S.-W.; Chiang, C.-J.; Tsai, J.-L.; Tang, M.-L.; Chen, G.-J.; Ku, K.-C. Risk Assessment of Mortality for All-Cause, Ischemic Heart Disease, Cardiopulmonary Disease, and Lung Cancer Due to the Operation of the World’s Largest Coal-Fired Power Plant. Atmos. Environ. 2014, 96, 117–124. [Google Scholar] [CrossRef]
- Hime, N.J.; Marks, G.B.; Cowie, C.T. A Comparison of the Health Effects of Ambient Particulate Matter Air Pollution from Five Emission Sources. Int. J. Environ. Res. Public Health 2018, 15, 1206. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-K.; Lin, R.-T.; Chen, P.-C.; Wang, P.; De Marcellis-Warin, N.; Zigler, C.; Christiani, D.C. A Global Perspective on Sulfur Oxide Controls in Coal-Fired Power Plants and Cardiovascular Disease. Sci. Rep. 2018, 8, 2611. [Google Scholar] [CrossRef] [Green Version]
- Hua, H.; Jiang, S.; Sheng, H.; Zhang, Y.; Liu, X.; Zhang, L.; Yuan, Z.; Chen, T. A High Spatial-Temporal Resolution Emission Inventory of Multi-Type Air Pollutants for Wuxi City. J. Clean. Prod. 2019, 229, 278–288. [Google Scholar] [CrossRef]
- ARPAS. Analisi Ambientale Del Comparto Produttivo Cementifici; ARPAS: Washington, DC, USA, 2004. [Google Scholar]
- Mangia, C.; Schipa, I.; Tanzarella, A.; Cervino, M.; Rizza, U. Simulazioni Modellistiche Meteo-Diffusive in Provincia di Lecce; Consiglio Nazionale Delle Ricerche: Roma, Italy, 2016.
- Pielke, R.; Cotton, W.; Walko, R.; Tremback, C.; Lyons, W.; Grasso, L.; Nicholls, M.; Moran, M.; Wesley, D.; Lee, T.; et al. A Comprehensive Meteorological Modeling System–RAMS. Meteorol. Atmos. Phys. 1992, 49, 69–91. [Google Scholar] [CrossRef]
- Scire, J.S.; Strimaitis, D.G.; Yamartino, R.J. A User’s Guide for the CALPUFF Dispersion Model (Version 5); Earth Tech, Inc.: Land O Lakes, FL, USA, 2000. [Google Scholar]
- Bauleo, L.; Ancona, C.; Morabito, A.; Nocioni, A.; Giua, R.; Spagnolo, G.; Epifani, S.; Spagnolo, S.; Intini, F.; Pastore, T.; et al. Studio di Coorte Sugli Effetti Delle Esposizioni Ambientali Sulla Mortalità e Morbosità Della Popolazione Residente a Brindisi e Nei Comuni Limitrofi; ASL Taranto: Taranto, Italy, 2017. [Google Scholar]
- Tinarelli, G.; Anfossi, D.; Trini Castelli, S.; Bider, M.; Ferrero, E. A New High Performance Version of the Lagrangian Particle Dispersion Model Spray, Some Case Studies. In Air Pollution Modeling and Its Application XIII; Gryning, S.-E., Batchvarova, E., Eds.; Springer: Boston, MA, USA, 2000; pp. 499–507. ISBN 978-1-4615-4153-0. [Google Scholar]
- Giua, R.; Morabito, A.; Tanzarella, A.; Spagnolo, S.; Pastore, T.; Bevere, M.; Valentini, E.; La Ghezza, V.; De Gennaro, G.; Brusasca, G.; et al. Application of a Lagrangian Particle Model to the Source Apportionment for Primary Macropollutants in Taranto Area (South Italy). Int. J. Environ. Poll. 2014, 55, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Biggeri, A.; Catelan, D.; Barbone, F. Reporting Uncertainty. Epidemiol. Prev. 2010, 34, 91–95. [Google Scholar] [PubMed]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Full Article: Moving to a World Beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Bagordo, F.; Migoni, D.; Grassi, T.; Serio, F.; Idolo, A.; Guido, M.; Zaccarelli, N.; Fanizzi, F.P.; De Donno, A. Using the DPSIR Framework to Identify Factors Influencing the Quality of Groundwater in Grecìa Salentina (Puglia, Italy). Rend. Fis. Acc. Lincei 2016, 27, 113–125. [Google Scholar] [CrossRef]
- Idolo, A.; Grassi, T.; Bagordo, F.; Panico, A.; De Giorgi, M.; Serio, F.; Guido, M.; Piscitelli, P.; De Filippis, G.; Raho, A.; et al. Micronuclei in Exfoliated Buccal Cells of Children Living in a Cluster Area of Salento (Southern Italy) with a High Incidence of Lung Cancer: The IMP. AIR Study. Int. J. Environ. Res. Public Health 2018, 15, 1659. [Google Scholar] [CrossRef] [Green Version]
- Panico, A.; Grassi, T.; Bagordo, F.; Idolo, A.; Serio, F.; Tumolo, M.R.; De Giorgi, M.; Guido, M.; Tutino, M.; De Donno, A. Micronucleus Frequency in Exfoliated Buccal Cells of Children Living in an Industrialized Area of Apulia (Italy). Int. J. Environ. Res. Public Health 2020, 17, 1208. [Google Scholar] [CrossRef] [Green Version]
- Bagordo, F.; Panico, A.; Zizza, A.; Serio, F.; Idolo, A.; Tumolo, M.R.; Guido, M.; Gambino, I.; Grassi, T. Buccal Micronucleus Cytome Assay in Children Living in an Area with Low Anthropogenic Pressure: The EFFE. BI.P. Study. Mutat. Res. Genet. Toxicol. Environ. Mutagenesis 2022, 873, 503424. [Google Scholar] [CrossRef]
- Korte, J.E.; Brennan, P.; Henley, S.J.; Boffetta, P. Dose-Specific Meta-Analysis and Sensitivity Analysis of the Relation between Alcohol Consumption and Lung Cancer Risk. Am. J. Epidemiol. 2002, 155, 496–506. [Google Scholar] [CrossRef] [Green Version]
- Ubago-Guisado, E.; Rodríguez-Barranco, M.; Ching-López, A.; Petrova, D.; Molina-Montes, E.; Amiano, P.; Barricarte-Gurrea, A.; Chirlaque, M.-D.; Agudo, A.; Sánchez, M.-J. Evidence Update on the Relationship between Diet and the Most Common Cancers from the European Prospective Investigation into Cancer and Nutrition (EPIC) Study: A Systematic Review. Nutrients 2021, 13, 3582. [Google Scholar] [CrossRef]
- Cai, H.; Sobue, T.; Kitamura, T.; Ishihara, J.; Sawada, N.; Iwasaki, M.; Shimazu, T.; Tsugane, S. Association between Meat and Saturated Fatty Acid Intake and Lung Cancer Risk: The Japan Public Health Center-Based Prospective Study. Int. J. Cancer 2020, 147, 3019–3028. [Google Scholar] [CrossRef]
- Barrera-Rodriguez, R.; Morales-Fuentes, J. Lung Cancer in Women. Lung Cancer 2012, 3, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Das, A.; Krishnamurthy, A.; Ramshankar, V.; Sagar, T.G.; Swaminathan, R. The Increasing Challenge of Never Smokers with Adenocarcinoma Lung: Need to Look beyond Tobacco Exposure. Indian J. Cancer. 2017, 54, 172–177. [Google Scholar] [CrossRef]
- Zakkouri, F.A.; Saloua, O.; Halima, A.; Rachid, R.; Hind, M.; Hassan, E. Smoking, Passive Smoking and Lung Cancer Cell Types among Women in Morocco: Analysis of Epidemiological Profiling of 101 Cases|BMC Research Notes|Full Text. BMC Res. Notes 2015, 8, 530. [Google Scholar] [CrossRef] [Green Version]
- Kanwal, M.; Ding, X.-J.; Cao, Y. Familial Risk for Lung Cancer. Oncol. Lett. 2017, 13, 535–542. [Google Scholar] [CrossRef] [Green Version]
- Lissowska, J.; Foretova, L.; Dąbek, J.; Zaridze, D.; Szeszenia-Dabrowska, N.; Rudnai, P.; Fabianova, E.; Cassidy, A.; Mates, D.; Bencko, V.; et al. Family History and Lung Cancer Risk: International Multicentre Case–Control Study in Eastern and Central Europe and Meta-Analyses. Cancer Causes Control 2010, 21, 1091–1104. [Google Scholar] [CrossRef]
- Olsson, A.C.; Vermeulen, R.; Schüz, J.; Kromhout, H.; Pesch, B.; Peters, S.; Behrens, T.; Portengen, L.; Mirabelli, D.; Gustavsson, P.; et al. Exposure-Response Analyses of Asbestos and Lung Cancer Subtypes in a Pooled Analysis of Case-Control Studies. Epidemiology 2017, 28, 288–299. [Google Scholar] [CrossRef] [Green Version]
- Scungio, M.; Buonanno, G.; Stabile, L.; Ficco, G. Lung Cancer Risk Assessment at Receptor Site of a Waste-to-Energy Plant. Waste Manag. 2016, 56, 207–215. [Google Scholar] [CrossRef]
- IARC. Outdoor Air Pollution; IARC: Lyon, France, 2016; Volume 109, ISBN 978-92-832-0147-2. [Google Scholar]
- IARC. Outdoor Air Pollution a Leading Environmental Cause of Cancer Deaths; IARC: Lyon, France, 2013. [Google Scholar]
- Loomis, D.; Grosse, Y.; Lauby-Secretan, B.; Ghissassi, F.E.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. The Carcinogenicity of Outdoor Air Pollution. Lancet Oncol. 2013, 14, 1262–1263. [Google Scholar] [CrossRef]
- Coleman, N.C.; Burnett, R.T.; Higbee, J.D.; Lefler, J.S.; Merrill, R.M.; Ezzati, M.; Marshall, J.D.; Kim, S.-Y.; Bechle, M.; Robinson, A.L.; et al. Cancer Mortality Risk, Fine Particulate Air Pollution, and Smoking in a Large, Representative Cohort of US Adults. Cancer Causes Control 2020, 31, 767–776. [Google Scholar] [CrossRef]
- Hvidtfeldt, U.A.; Severi, G.; Andersen, Z.J.; Atkinson, R.; Bauwelinck, M.; Bellander, T.; Boutron-Ruault, M.-C.; Brandt, J.; Brunekreef, B.; Cesaroni, G.; et al. Long-Term Low-Level Ambient Air Pollution Exposure and Risk of Lung Cancer-A Pooled Analysis of 7 European Cohorts. Environ. Int. 2021, 146, 106249. [Google Scholar] [CrossRef]
- Cohen, S.S.; Sadoff, M.M.; Jiang, X.; Fryzek, J.P.; Garabrant, D.H. A Review and Meta-Analysis of Cancer Risks in Relation to Portland Cement Exposure. Occup. Environ. Med. 2014, 71, 796–802. [Google Scholar] [CrossRef]
- Marcon, A.; Pesce, G.; Girardi, P.; Marchetti, P.; Blengio, G.; de Zolt Sappadina, S.; Falcone, S.; Frapporti, G.; Predicatori, F.; de Marco, R. Association between PM10 Concentrations and School Absences in Proximity of a Cement Plant in Northern Italy. Int. J. Hyg. Environ. Health 2014, 217, 386–391. [Google Scholar] [CrossRef]
- Fell, A.K.M.; Nordby, K.C. Association between Exposure in the Cement Production Industry and Non-Malignant Respiratory Effects: A Systematic Review. BMJ Open 2017, 7, e012381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffetti, E.; Treccani, M.; Donato, F. Cement Plant Emissions and Health Effects in the General Population: A Systematic Review. Chemosphere 2019, 218, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Spyratos, D.; Zarogoulidis, P.; Porpodis, K.; Tsakiridis, K.; Machairiotis, N.; Katsikogiannis, N.; Kougioumtzi, I.; Dryllis, G.; Kallianos, A.; Rapti, A.; et al. Occupational Exposure and Lung Cancer. J. Thorac. Dis. 2013, 5, S440–S445. [Google Scholar] [CrossRef] [PubMed]
- Christiani, D.C. Occupational Exposures and Lung Cancer. Am. J. Respir. Crit. Care Med. 2020, 202, 317–319. [Google Scholar] [CrossRef]
- Jones, R.R.; Barone-Adesi, F.; Koutros, S.; Lerro, C.C.; Blair, A.; Lubin, J.; Heltshe, S.L.; Hoppin, J.A.; Alavanja, M.C.R.; Beane Freeman, L.E. Incidence of Solid Tumors Among Pesticide Applicators Exposed to the Organophosphate Insecticide Diazinon in the Agricultural Health Study: An Updated Analysis. Occup. Environ. Med. 2015, 72, 496–503. [Google Scholar] [CrossRef]
- Silver, S.R.; Bertke, S.J.; Hines, C.J.; Alavanja, M.C.R.; Hoppin, J.A.; Lubin, J.H.; Rusiecki, J.A.; Sandler, D.P.; Beane Freeman, L.E. Cancer Incidence and Metolachlor Use in the Agricultural Health Study: An Update. Int. J. Cancer 2015, 137, 2630–2643. [Google Scholar] [CrossRef] [Green Version]
- Bonner, M.R.; Freeman, L.E.B.; Hoppin, J.A.; Koutros, S.; Sandler, D.P.; Lynch, C.F.; Hines, C.J.; Thomas, K.; Blair, A.; Alavanja, M.C.R. Occupational Exposure to Pesticides and the Incidence of Lung Cancer in the Agricultural Health Study. Environ. Health Perspect. 2017, 125, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Ferri, G.M.; Intranuovo, G.; Cavone, D.; Corrado, V.; Birtolo, F.; Tricase, P.; Fuso, R.; Vilardi, V.; Sumerano, M.; L’abbate, N.; et al. Estimates of the Lung Cancer Cases Attributable to Radon in Municipalities of Two Apulia Provinces (Italy) and Assessment of Main Exposure Determinants. Int. J. Environ. Res. Public Health 2018, 15, 1294. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables Selected for Each Section | Description | Type |
|---|---|---|
| 1—PERSONAL INFORMATION | ||
| Age | Age at the interview | Continuous |
| Schooling | 4 categories | Ordinal |
| Elementary school or no degree | ||
| Middle school license | ||
| Higher middle school license | ||
| Graduation | ||
| Marital status | 2 categories | Dichotomous |
| Married/Cohabiting | ||
| Single, separated, divorced, widower | ||
| Body size | Self-declaration of body size (4 categories) | Ordinal |
| Underweight | ||
| Normal weight | ||
| Overweight | ||
| Obesity | ||
| 2—BEHAVIOURS AND LIFESTYLES | ||
| Physical activity | Self-declaration of the type of physical activity that may be practiced (3 categories) | Nominal |
| Active (hard work + other physical activity) | ||
| Hard work without other physical activity | ||
| Sedentary work and no physical activity | ||
| Excessive alcohol consumption | Self-declaration of consumption of more than 2 glasses of alcohol per day | Dichotomous |
| Yes | ||
| No | ||
| Excessive meat consumption (>2 times in a week) | Self-declaration of consumption of more than 2 times in a week | Dichotomous |
| Yes | Yes | |
| No | No | |
| Smoking habits | Self-declaration of smoking habits in 3 categories | Nominal |
| Smoker | Smoker | |
| Former smoker | Former smoker | |
| No smoker | Non-smoker | |
| ANPYC Average Number of Packages Year of Cigarette | self-declaration of number of cigarettes smoked per day ANPYC = (average number of cigarette per day × years of active smoking)/20 | Continuous |
| Exposure to second hand smoke | Self-declaration of exposure to second-hand smoke | Dichotomous |
| Yes | Yes | |
| No | No | |
| 3—PERSONAL AND FAMILY CLINICAL HISTORY | ||
| Positive family history for cancer | at least one family member including mother/father, brother/sister, grandfather/grandmother | Dichotomous |
| Yes | ||
| No | ||
| 4—EXPOSURE TO SOURCES OF AIR POLLUTION | ||
| Frequent use of the wood-fired fireplace? | Self-declaration refers to the house in which the subject lived for at least 10 continuous years before 2006 | Dichotomous |
| Yes | ||
| No | ||
| Presence of asbestos artefacts nearby? | Self-declaration refers to the house in which the subjects lived for at least 10 continuous years before 2006. Artefacts such as asbestos roofing, asbestos water tanks, asbestos flues, and in general buildings containing asbestos | Dichotomous |
| Yes | ||
| No | ||
| In the vicinity of the residence, presence of | Self-declaration refers to the house in which the subjects lived for at least 10 continuous years before 2006. | |
| Intense traffic | Dichotomous | |
| Chemical/petrochemical plant | Dichotomous | |
| Thermoelectric power plant | Dichotomous | |
| Port | Dichotomous | |
| Industrial Area | Dichotomous | |
| Activities with potential presence of asbestos | As a shipyard, sheds covered with asbestos, railway rolling stock production/repair plants | Dichotomous |
| Quarrying or mining | Dichotomous | |
| Incinerator | Dichotomous | |
| Landfill | Dichotomous | |
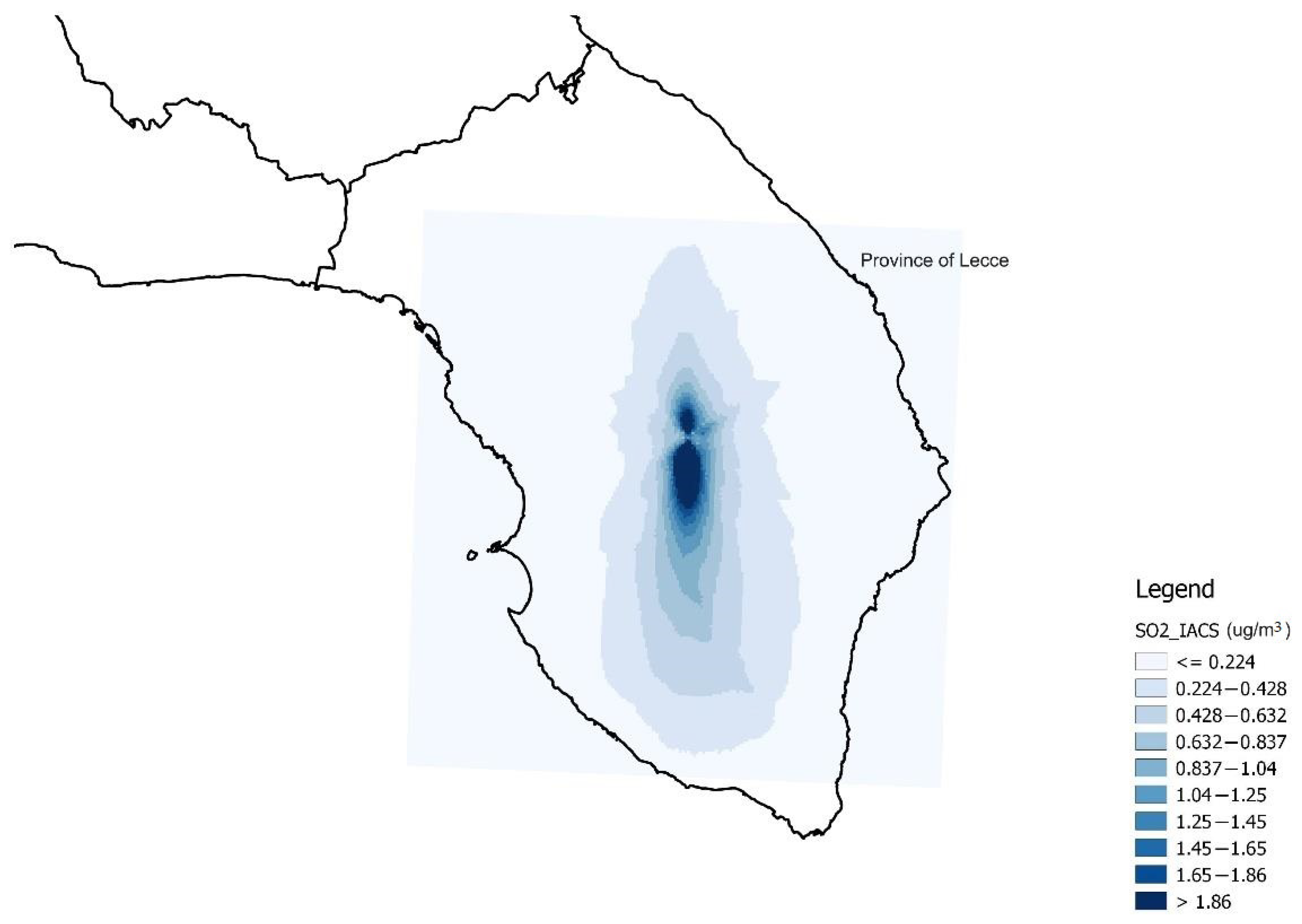
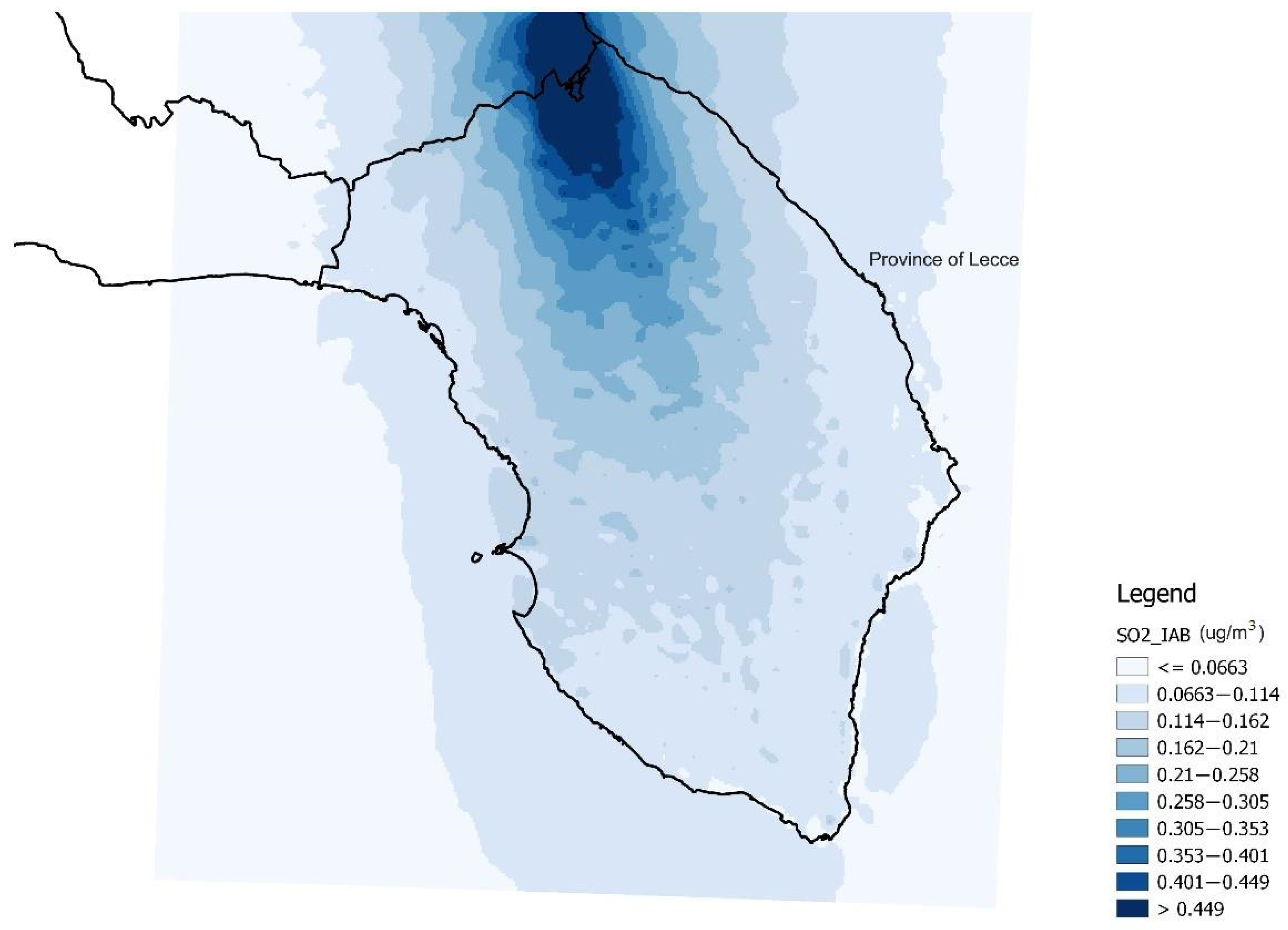
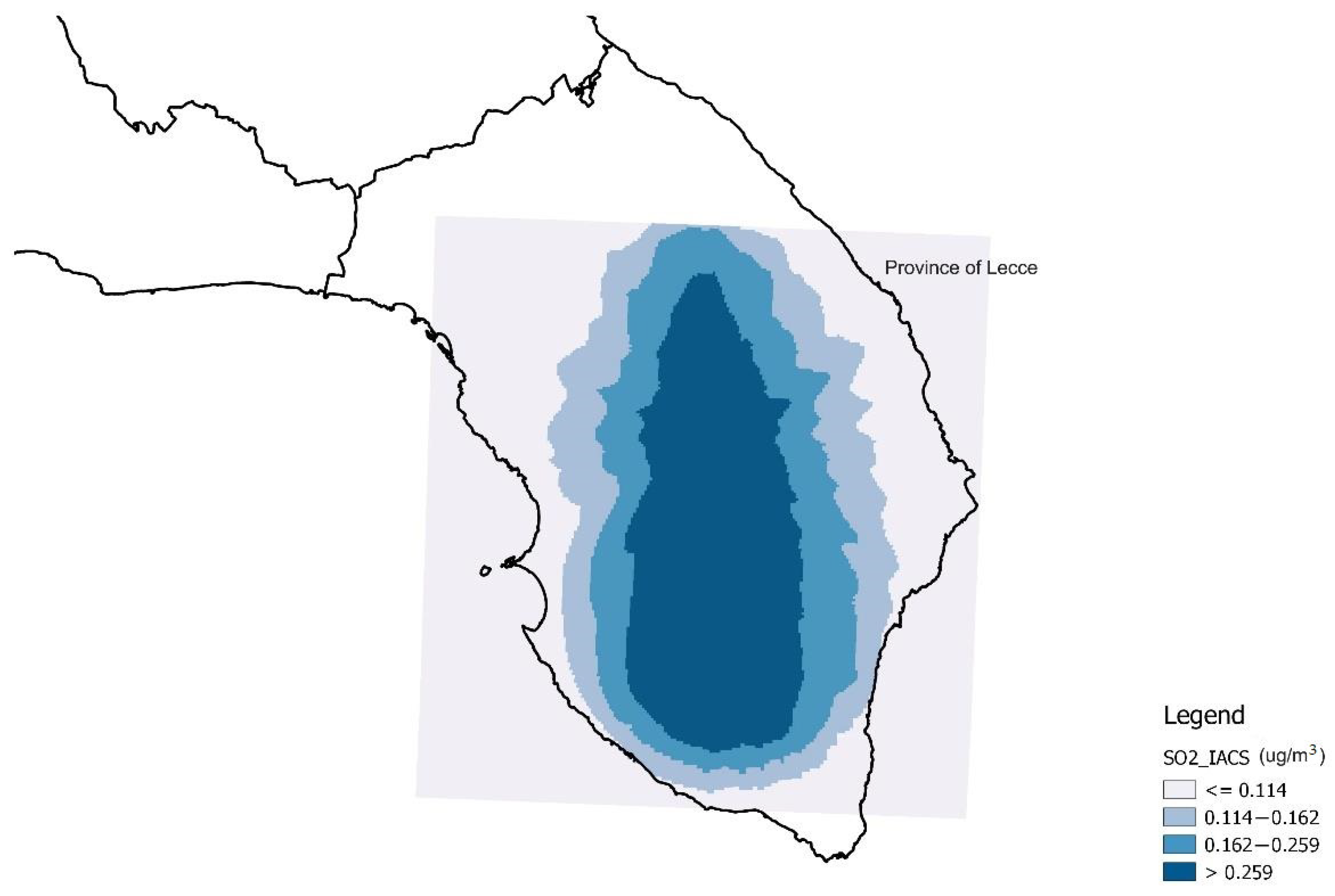
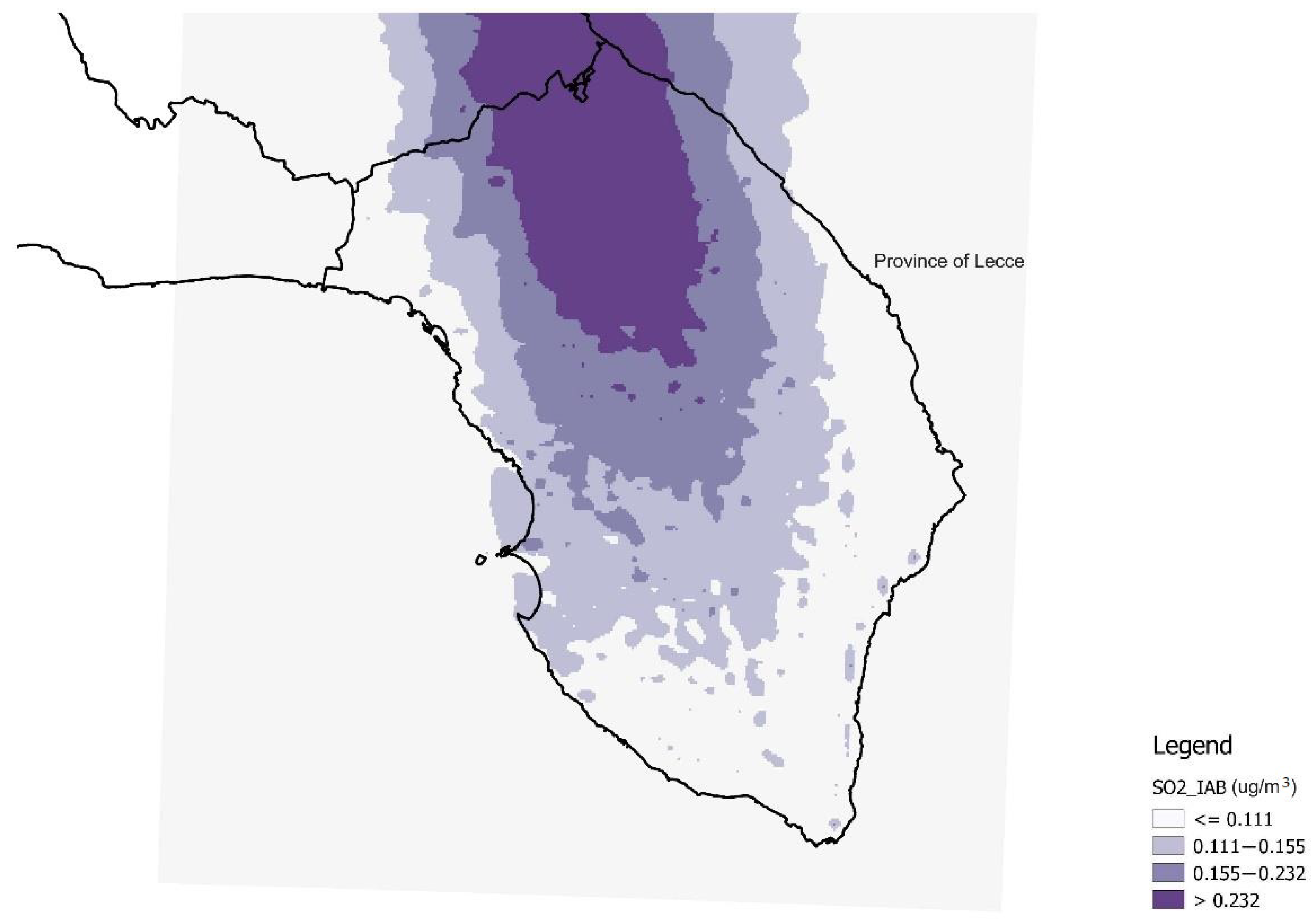
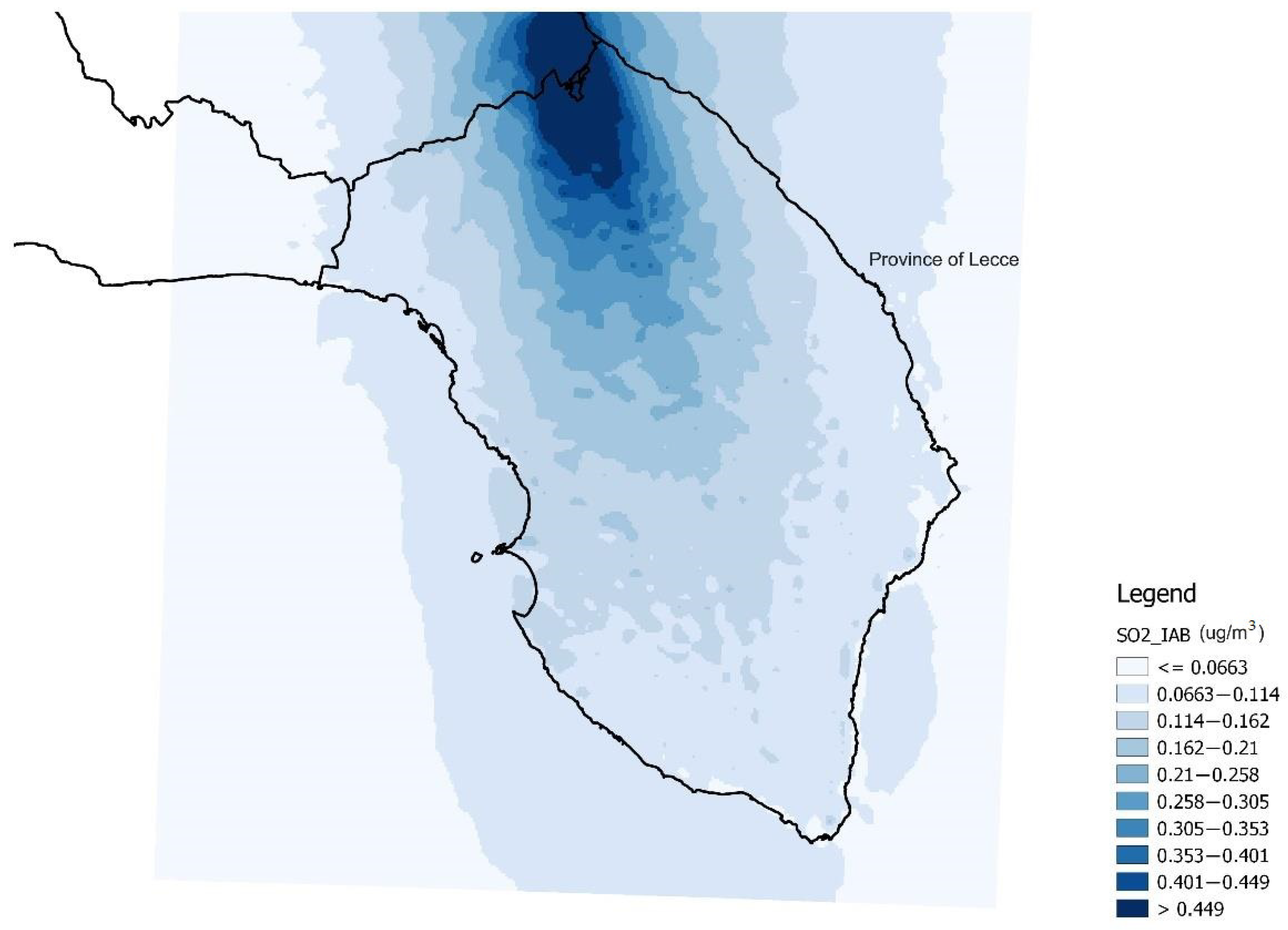
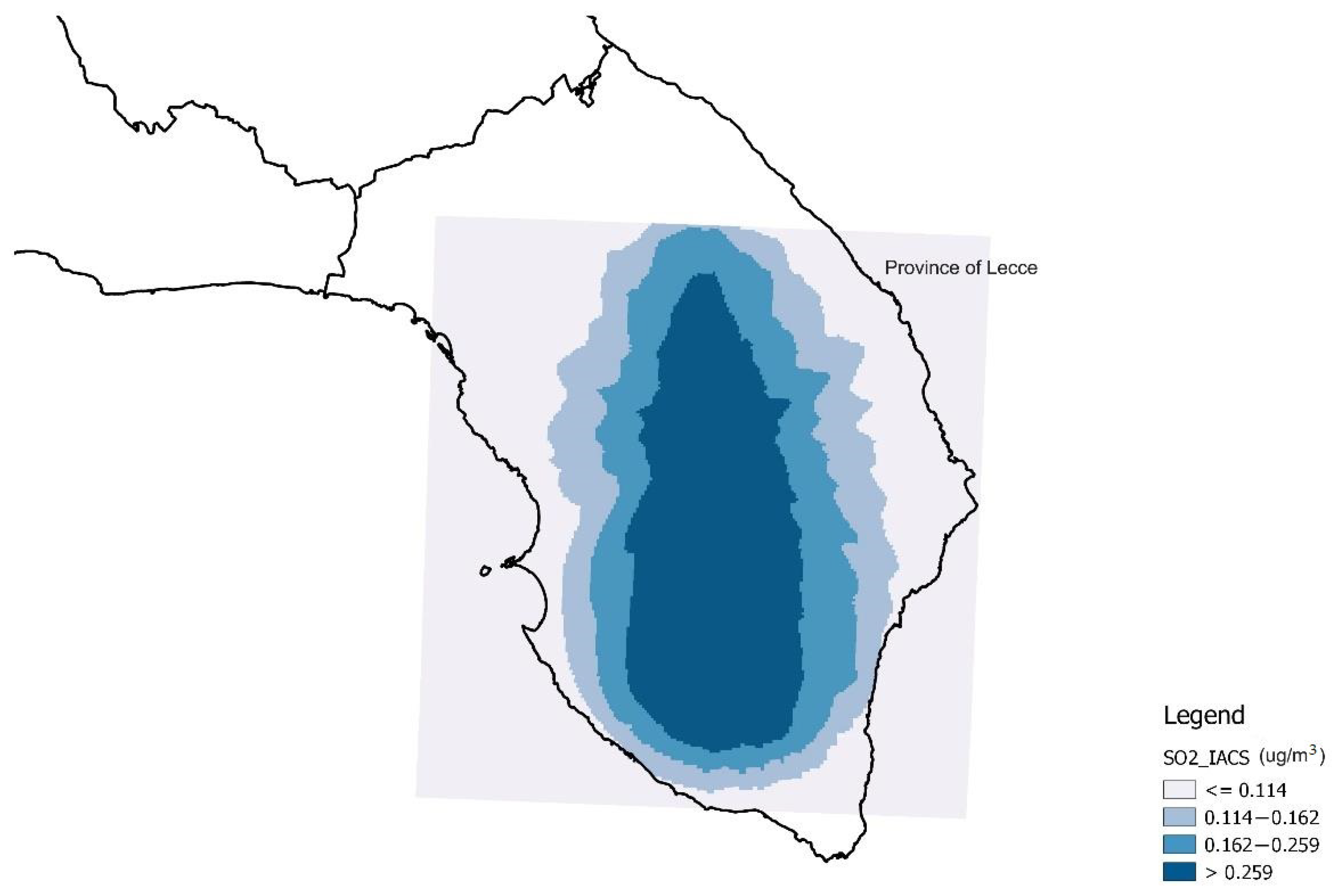
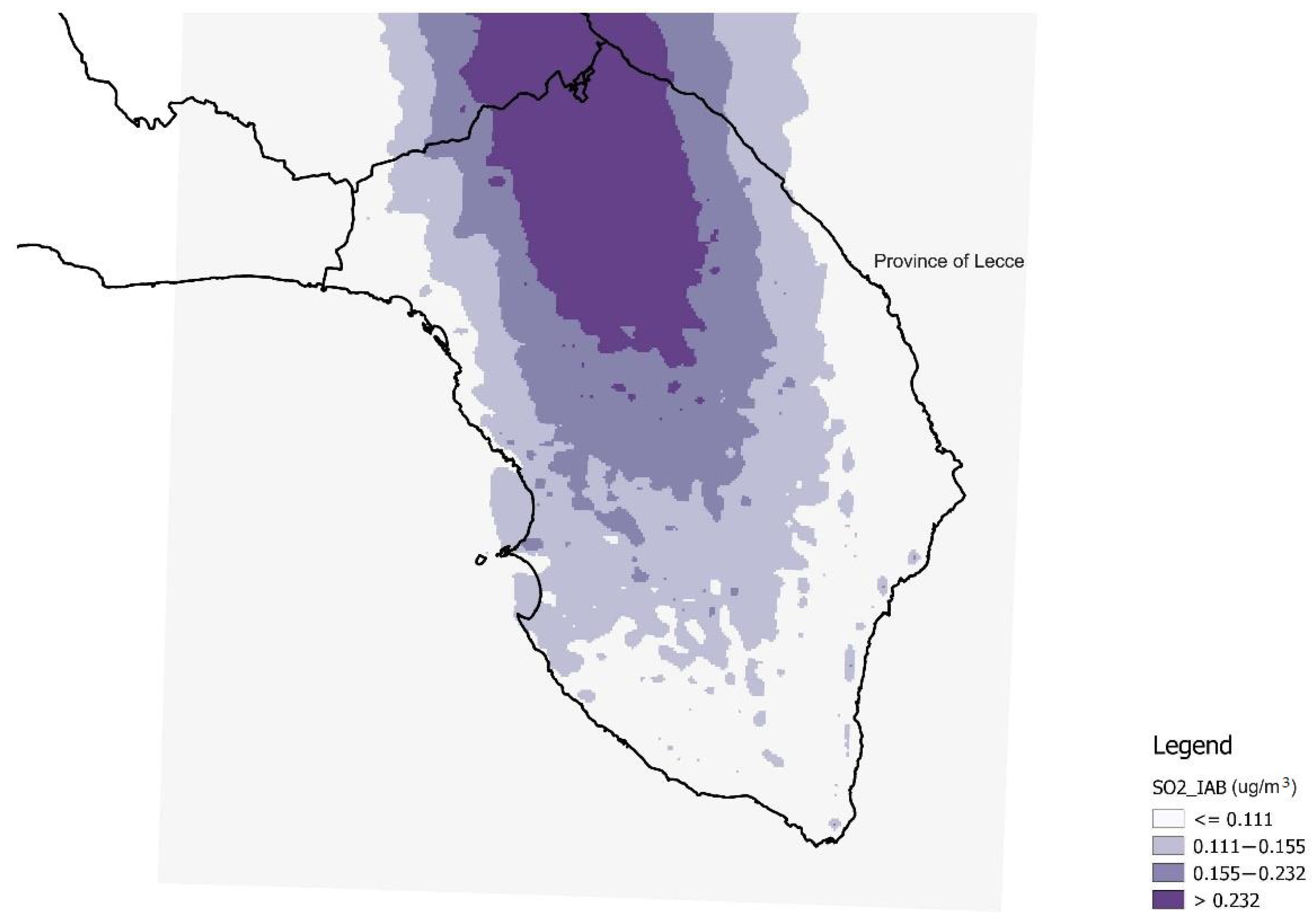
| SO2 exposure from industrial plants | Data from dispersion models of SO2 | |
| expSO2_IACS | Individual exposure to the Industrial Area of Central Salento (IACS), defined on the basis of the SO2 distribution produced by IACS (emission data from 1990; meteorological data from 2005) | Continuous |
| expSO2_IAB | Individual exposure to the Industrial Area of Brindisi (IAB), defined on the basis of the SO2 distribution produced by the IAB (emission data from 1993; meteorological data from 2005) | Continuous |
| 6—WORK AND PROFESSIONAL HISTORY | ||
| Occupational exposure to hazardous substances | Hazardous substances such as solvents, paints, abrasives, silica, cement, asbestos, fibrous material, physical agents/radiation and chemical substances in potentially critical production sectors (chemistry, construction, wood and similar, metallurgy, mining, agriculture) defined according to the National Institute for Occupational Accident Insurance code. | Dichotomous |
| Yes | ||
| No | ||
| Prevalent activity (≥10 years, accrued by 2007) in potentially critical sector | Prevalent activity declared in the questionnaire (carried out for at least 10 years from 2007) in potentially critical sectors (chemistry, construction, wood and similar, metallurgy, mining, agriculture) defined according to the National Institute for Occupational Accident Insurance code | Dichotomous |
| Yes | ||
| No | ||
| Prevalent activity (≥10 years, accrued by 2007) in the agricultural sector using plant protection products with no personal protection equipment | Prevalent activity declared in the questionnaire (carried out for at least 10 years from 2007) in the agricultural sector using plant protection products with no personal protection equipment | Dichotomous |
| Yes | ||
| No | ||
| SO2 (µg/m3) | n | Mean | SD | p25 | p50 | p75 | p90 | min | max |
|---|---|---|---|---|---|---|---|---|---|
| expSO2_IACS | 1703 | 0.276 | 0.528 | 0.114 | 0.162 | 0.259 | 0.467 | 0.020 | 5.378 |
| expSO2_IAB | 1703 | 0.183 | 0.093 | 0.111 | 0.155 | 0.232 | 0.316 | 0.042 | 0.551 |
| Men (n = 1404) | Women (n = 364) | |||||
|---|---|---|---|---|---|---|
| Variables | Cases [n (%)] | Controls [n (%)] | p-Value | Cases [n (%)] | Controls [n (%)] | p-Value |
| Classifications of pulmonary neoplasms | ||||||
| Adenocarcinoma | 119 (33.90) | <0.001 # | 57 (62.64) | <0.001 # | ||
| Squamous carcinoma | 99 (28.21) | 7 (7.69) | ||||
| Small cell carcinoma | 40 (11.40) | 6 (6.59) | ||||
| Less frequent neoplasms ç | 51 (14.53) | 13 (14.29) | ||||
| Other çç | 42 (11.97) | 8 (8.79) | ||||
| Age (mean ± Standard Deviation) | 351 | 1053 | 91 | 273 | ||
| 71.00 ± 8.90 | 70.40 ± 9.70 | 0.241 | 65.9 ± 11.70 | 65.9 ± 11.90 | 0.962 | |
| Schooling | 350 | 1040 | 90 | 269 | ||
| Elementary school or no degree | 186 (53.14) | 409 (39.33) | <0.001 | 43 (47.78) | 133 (49.44) | 0.032 |
| Middle school license | 91 (26.00) | 325 (31.25) | 13 (14.44) | 71 (26.39) | ||
| Higher middle school license | 56 (16.00) | 247 (23.75) | 23 (25.56) | 42 (15.61) | ||
| Graduation | 17 (4.86) | 59 (5.67) | 11 (12.22) | 23 (8.55) | ||
| Marital status | 349 | 1051 | 90 | 270 | ||
| Married/Cohabiting | 287 (82.23) | 921 (87.63) | 0.011 | 62 (68.89) | 187 (69.26) | 0.947 |
| Single, separated, divorced, widower | 62 (17.77) | 130 (12.37) | 28 (31.11) | 83 (30.74) | ||
| Physical activity | 351 | 1053 | 91 | 273 | ||
| Active (hard work + other physical activity) | 88 (25.07) | 350 (33.24) | <0.001 | 28 (30.77) | 66 (24.18) | 0.386 |
| Hard work without other physical activity | 169 (48.15) | 346 (32.86) | 23 (25.27) | 67 (24.54) | ||
| Sedentary work and no physical activity | 94 (26.78) | 357 (33.90) | 40 (43.96) | 140 (51.28) | ||
| Body size | 351 | 1051 | 91 | 273 | ||
| Underweight | 118 (33.62) | 306 (29.12) | 36 (39.56) | 95 (34.80) | ||
| Normal weight | 167 (47.58) | 555 (52.81) | 0.006 | 46 (50.55) | 136 (49.82) | 0.264 |
| Overweight | 53 (15.10) | 177 (16.84) | 9 (9.89) | 32 (11.72) | ||
| Obesity | 13 (3.70) | 13 (1.24) | <3 | 10 (3.66) | ||
| Excessive alcohol consumption (>2 glasses of alcohol per day) | 351 | 1044 | 91 | 273 | ||
| Yes | 142 (40.46) | 352 (33.72) | 0.022 | 11 (12.09) | 34 (12.45) | 0.927 |
| No | 209 (59.54) | 692 (66.28) | 80 (87.91) | 239 (87.55) | ||
| Excessive meat consumption (>2 times in a week) | 351 | 1053 | 91 | 273 | ||
| Yes | 279 (79.49) | 845 (80.25) | 0.758 | 72 (79.12) | 193 (70.70) | 0.118 |
| No | 72 (20.51) | 208 (19.75) | 19 (20.88) | 80 (29.30) | ||
| Smoking habits | 351 | 1053 | 91 | 273 | ||
| Smoker | 82 (23.36) | 207 (19.66) | <0.001 | 15 (16.48) | 37 (13.55) | <0.001 |
| Former smoker | 261 (74.36) | 522 (49.57) | 45 (49.45) | 48 (17.58) | ||
| No smoker | 8 (2.28) | 324 (30.77) | 31 (34.07) | 188 (68.86) | ||
| ANPYC $ (n) mean ± Standard Deviation (Packs/year) | 351 | 1053 | 91 | 273 | ||
| 62.7 ± 36.60 | 26.6 ± 30.40 | <0.001 | 22.7 ± 25.10 | 5.9 ± 13.70 | <0.001 | |
| Exposure to second hand smoke | 351 | 1053 | 91 | 273 | ||
| Yes | 125 (35.61) | 315 (29.91) | 0.046 | 65 (71.43) | 159 (58.24) | 0.025 |
| No | 226 (64.39) | 738 (70.09) | 26 (28.57) | 114 (41.76) | ||
| Positive family history for cancer § | 351 | 1053 | 91 | 273 | ||
| Yes | 168 (47.86) | 373 (35.42) | <0.001 | 47 (51.65) | 123 (45.05) | 0.275 |
| No | 183 (52.14) | 680 (64.58) | 44 (48.35) | 150 (54.95) | ||
| Frequent use of the wood-fired fireplace? ° | 351 | 1053 | 91 | 273 | ||
| Si | 225 (64.10) | 726 (68.95) | 0.093 | 60 (65.93) | 183 (67.03) | 0.847 |
| No | 126 (35.90) | 327 (31.05) | 31 (34.07) | 90 (32.97) | ||
| Presence of asbestos artefacts nearby? °^ | 306 | 949 | 78 | 241 | ||
| Yes | 94 (30.72) | 213 (22.44) | 0.003 | 24 (30.77) | 60 (24.90) | 0.306 |
| No | 212 (69.28) | 736 (77.56) | 54 (69.23) | 181 (75.10) | ||
| In the vicinity of the residence, presence of ° | 351 | 1053 | 91 | 272 | ||
| Intense traffic | 53 (15.10) | 182 (17.28) | 0.591 | 13 (14.29) | 48 (17.65) | 0.495 |
| Chemical/petrochemical plant | 4 (1.14) | 4 (0.38) | 0.101 | <3 | <3 | nc |
| Thermoelectric power plant | <3 | 6 (0.57) | nc | <3 | <3 | nc |
| Port | 4 (1.14) | 7 (0.66) | 0.382 | <3 | <3 | nc |
| Industrial Area | 19 (5.41) | 67 (6.36) | 0.521 | 10 (10.99) | 28 (10.26) | 0.843 |
| Activities with potential presence of asbestos * | 22 (6.27) | 50 (4.75) | 0.264 | 10 (10.99) | 9 (3.30) | 0.004 |
| Quarrying or mining | 18 (5.13) | 34 (3.23) | 0.103 | 4 (4.40) | 3 (1.10) | 0.047 |
| Incinerator | 9 (2.56) | 5 (0.47) | 0.001 | <3 | <3 | nc |
| Landfill | 26 (7.41) | 45 (4.27) | 0.020 | 9 (9.89) | 14 (5.13) | 0.106 |
| SO2 exposure from industrial plants | ||||||
| expSO2_IACS ** (n) | 333 | 1021 | 86 | 263 | ||
| mean ± Standard Deviation (µg/m3) | 0.363 ± 0.739 | 0.253 ± 0.428 | <0.001 | 0.259 ± 0.389 | 0.259 ± 0.588 | 0.995 |
| expSO2_IAB *** (n) | 333 | 1021 | 86 | 263 | ||
| mean ± Standard Deviation (µg/m3) | 0.187 ± 0.097 | 0.184 ± 0.094 | 0.596 | 0.179 ± 0.092 | 0.177 ± 0.088 | 0.855 |
| Prevalent activity (≥10 years, accrued by 2007) in potentially critical sector @ | 351 | 1053 | 91 | 273 | ||
| Yes | 182 (51.85) | 485 (46.06) | 12 (13.19) | 70 (25.64) | ||
| No | 169 (48.15) | 568 (53.94) | 0.06 | 79 (86.81) | 23 (74.36) | 0.014 |
| Occupational exposure to hazardous substances **** | 351 | 1053 | 91 | 273 | ||
| Yes | 95 (27.07) | 301 (28.58) | 0.584 | <3 | 21 (7.69) | nc |
| No | 256 (72.93) | 752 (71.42) | 89 (97.80) | 252 (92.31) | ||
| Prevalent activity (≥10 years, accrued by 2007) in the agricultural sector using plant protection products with no personal protection equipment | 31 | 74 | <3 | <3 | ||
| Yes | 20 (64.52) | 26 (35.14) | 0.006 | <3 | <3 | nc |
| No | 11 (35.48) | 48 (64.86) | <3 | <3 | ||
| Variables | Variables Coding | aOR | p | 90%CI | aOR | p | 90%CI |
|---|---|---|---|---|---|---|---|
| Men | Women | ||||||
| Schooling | |||||||
| Reference class: elementary school or no degree | Middle school license | 0.59 | 0.021 | 0.40–0.86 | 0.52 | 0.209 | 0.22–1.22 |
| Higher middle school license | 0.47 | 0.005 | 0.31–0.73 | 2.08 | 0.140 | 0.92–4.72 | |
| Graduation | 0.77 | 0.540 | 0.39–1.54 | 1.12 | 0.878 | 0.34–3.67 | |
| Marital status | |||||||
| Reference class: Married or cohabiting | Single, separated, divorced, widower | 0.68 | 0.098 | 0.46–1.00 | 1.99 | 0.093 | 1.01–3.92 |
| Physical activity | |||||||
| Reference class: active (hard work + other physical activity) | Hard work without other physical activity | 1.88 | 0.005 | 1.31–2.72 | 0.77 | 0.607 | 0.33–1.78 |
| Sedentary work and no physical activity | 0.97 | 0.905 | 0.67–1.41 | 0.56 | 0.185 | 0.27–1.15 | |
| Body size | |||||||
| Reference class: normal weight | Under weight | 1.08 | 0.699 | 0.77–1.51 | 0.53 | 0.155 | 0.25–1.10 |
| Overweight | 0.72 | 0.192 | 0.48–1.09 | 0.97 | 0.965 | 0.36–2.67 | |
| Obesity | 2.49 | 0.105 | 0.98–6.28 | nc | |||
| Alcohol consumption | |||||||
| Excessive alcohol consumption (>2 glasses of alcohol per day) | 1.22 | 0.232 | 0.93–1.62 | 2.44 | 0.099 | 1.01–5.94 | |
| Red meat consumption | |||||||
| Excessive meat consumption (>2 times a week) | 0.81 | 0.318 | 0.56–1.15 | 1.29 | 0.530 | 0.66–2.55 | |
| Smoking habits | |||||||
| ANPYC $ | Unit increase of packets year of cigarettes | 1.03 | <0.001 | 1.03–1.04 | 1.06 | <0.001 | 1.04–1.08 |
| Passive smoke | 1.04 | 0.820 | 0.77–1.41 | 1.75 | 0.148 | 0.93–3.30 | |
| Positive family history for cancer § | 1.28 | 0.149 | 0.97–1.69 | 1.81 | 0.094 | 1.01–3.24 | |
| Sources of atmospheric pollution inside or in the proximity of the residence * | |||||||
| Presence of wood-fired fireplace | 0.82 | 0.291 | 0.60–1.12 | 0.87 | 0.716 | 0.45–1.67 | |
| Asbestos artefacts ^ | 1.30 | 0.205 | 0.92–1.82 | 1.20 | 0.685 | 0.57–2.55 | |
| Intense traffic | 0.93 | 0.763 | 0.63–1.37 | 0.73 | 0.546 | 0.31–1.73 | |
| Chemical/petrochemical plant | 5.31 | 0.179 | 0.69–40.91 | nc | |||
| Activity with potential presence of asbestos # | 1.15 | 0.742 | 0.58–2.27 | 11.81 | 0.005 | 2.76–50.49 | |
| Quarrying or mining | 0.82 | 0.666 | 0.38–1.76 | 3.90 | 0.231 | 0.60–25.26 | |
| Incinerator | 9.83 | 0.007 | 2.45–39.44 | 1.57 | 0.765 | 0.13–19.04 | |
| Landfill | 1.42 | 0.348 | 0.77–2.63 | 0.70 | 0.599 | 0.23–2.15 | |
| SO2 exposure from industrial plants (values in µg/m3) | |||||||
| IACS ** | 2nd quartile (0.115–0.162) | 1.18 | 0.498 | 0.79–1.78 | 0.74 | 0.532 | 0.34–1.62 |
| Reference class: 1st quartile | 3rd quartile (0.162–0.259) | 1.08 | 0.760 | 0.71–1.64 | 1.30 | 0.582 | 0.60–2.82 |
| 4th quartile (>0.259) | 2.42 | 0.001 | 1.58–3.72 | 1.25 | 0.667 | 0.54–2.90 | |
| trend for increase of 1 µg/m3 | 1.21 | 0.162 | 0.97–1.51 | 0.91 | 0.734 | 0.58–1.43 | |
| IAB *** | 2nd quartile (0.115–0.115) | 0.57 | 0.031 | 0.37–0.88 | 0.63 | 0.397 | 0.25–1.55 |
| Reference class: 1st quartile | 3rd quartile (0.115–0.232) | 0.55 | 0.017 | 0.37–0.83 | 1.75 | 0.290 | 0.73–4.16 |
| 4th quartile (>0.232) | 1.49 | 0.110 | 0.99–2.26 | 0.62 | 0.348 | 0.27–1.42 | |
| trend for increase of 1 µg/m3 | 2.67 | 0.298 | 0.57–12.60 | 0.23 | 0.468 | 0.01–6.36 | |
| Occupational exposure | |||||||
| Prevalent activity (≥10 years, accrued by 2007) in potentially critical sector @ | 1.08 | 0.727 | 0.75–1.56 | 0.39 | 0.067 | 0.17–0.91 | |
| Occupational exposure to hazardous substances **** | 0.76 | 0.158 | 0.55–1.05 | 0.27 | 0.175 | 0.06–1.32 | |
| Prevalent activity (≥10 years, accrued by 2007) in the agricultural sector using plant protection products with no personal protection equipment. | 5.26 | 0.023 | 1.58–17.53 | nc | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minichilli, F.; Gorini, F.; De Filippis, G.; Bustaffa, E.; Raho, A.M.; Melcarne, A.; Quarta, F.; Maggiore, G.; Idolo, A.; Serio, F.; et al. Risk Factors for Lung Cancer in the Province of Lecce: Results from the PROTOS Case–Control Study in Salento (Southern Italy). Int. J. Environ. Res. Public Health 2022, 19, 8775. https://doi.org/10.3390/ijerph19148775
Minichilli F, Gorini F, De Filippis G, Bustaffa E, Raho AM, Melcarne A, Quarta F, Maggiore G, Idolo A, Serio F, et al. Risk Factors for Lung Cancer in the Province of Lecce: Results from the PROTOS Case–Control Study in Salento (Southern Italy). International Journal of Environmental Research and Public Health. 2022; 19(14):8775. https://doi.org/10.3390/ijerph19148775
Chicago/Turabian StyleMinichilli, Fabrizio, Francesca Gorini, Giovanni De Filippis, Elisa Bustaffa, Anna Maria Raho, Anna Melcarne, Fabrizio Quarta, Giuseppe Maggiore, Adele Idolo, Francesca Serio, and et al. 2022. "Risk Factors for Lung Cancer in the Province of Lecce: Results from the PROTOS Case–Control Study in Salento (Southern Italy)" International Journal of Environmental Research and Public Health 19, no. 14: 8775. https://doi.org/10.3390/ijerph19148775
APA StyleMinichilli, F., Gorini, F., De Filippis, G., Bustaffa, E., Raho, A. M., Melcarne, A., Quarta, F., Maggiore, G., Idolo, A., Serio, F., Grassi, T., Bagordo, F., Castorini, I. F., Imbriani, G., Bianchi, F., & Piscitelli, P., on behalf of RePOL Study Group. (2022). Risk Factors for Lung Cancer in the Province of Lecce: Results from the PROTOS Case–Control Study in Salento (Southern Italy). International Journal of Environmental Research and Public Health, 19(14), 8775. https://doi.org/10.3390/ijerph19148775