
The Apapacho Violence Prevention Parenting Program: Conceptual Foundations and Pathways to Scale

 , ,
, ,
Abstract
:1. Introduction
1.1. The Colombian Context
1.2. Violence Prevention Parenting Programs
1.3. Core Components and the Development of Complex Interventions
1.4. The Present Study
2. Materials and Methods
3. Results
3.1. Core Components of Evidence-Based Parenting Programs
Main Takeaway
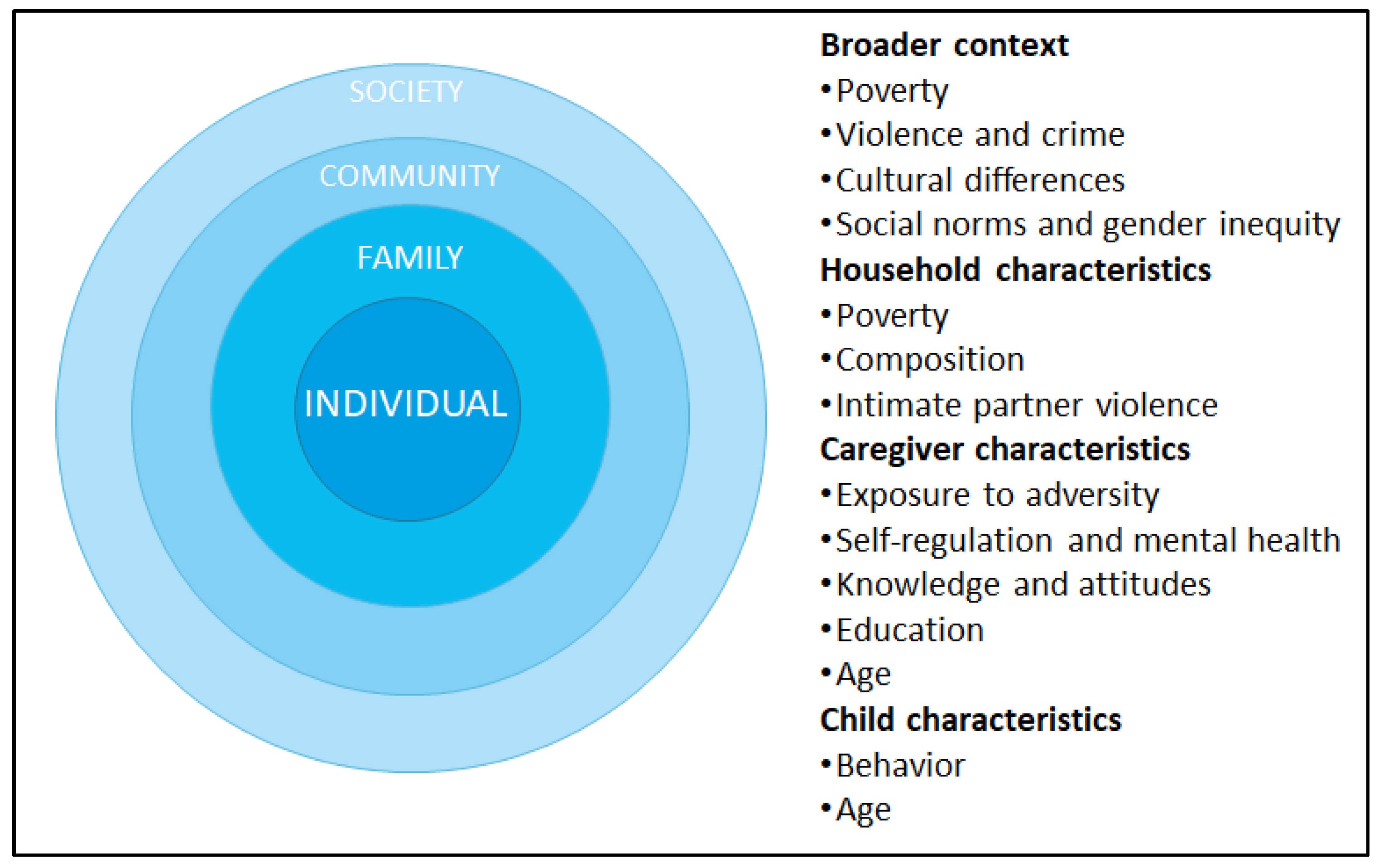
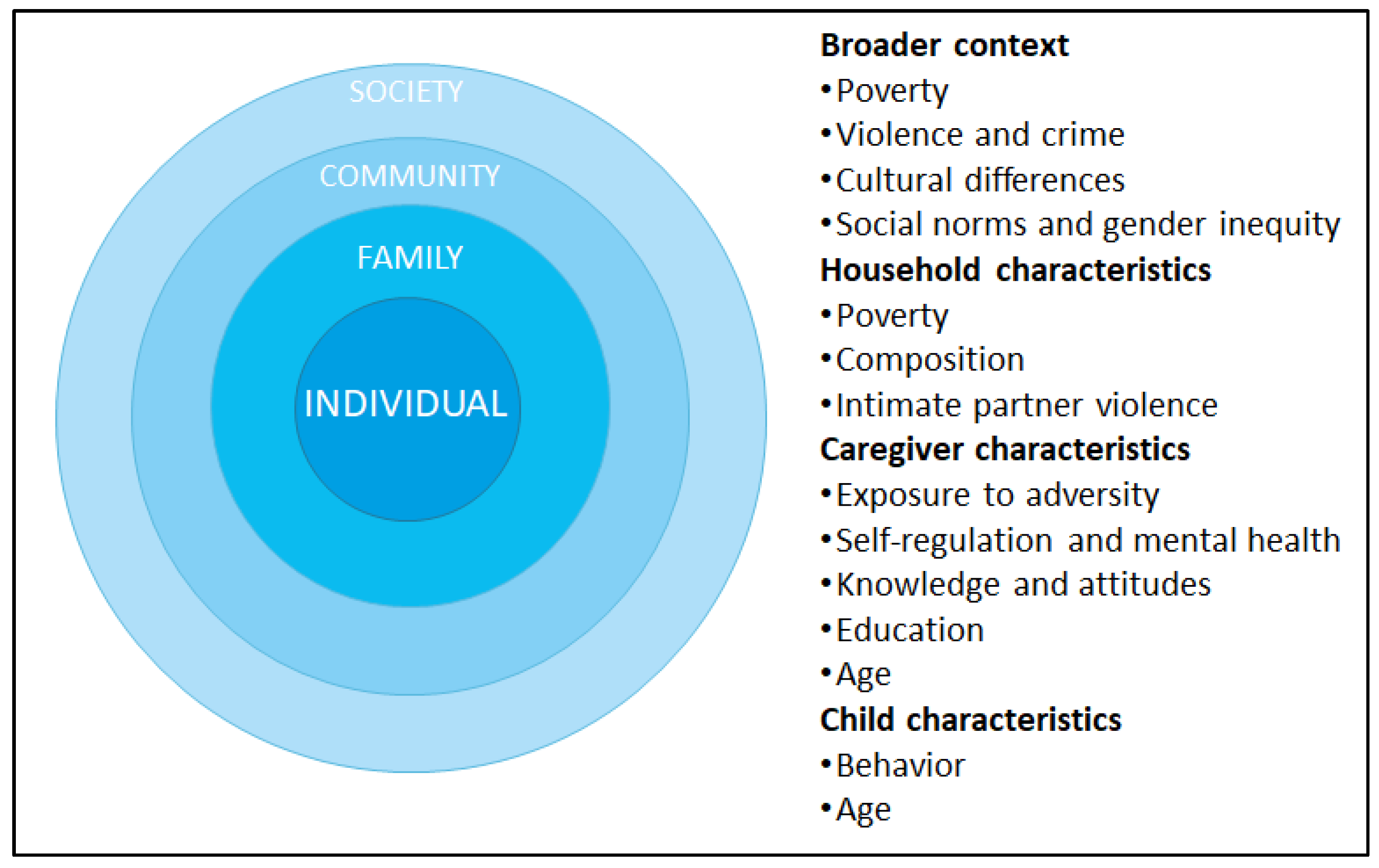
3.2. Drivers of VAC in Colombia
Main Takeaway
3.3. Pathways to Scale: Current Services and Infrastructure in Colombia
3.3.1. Services for Young Children
3.3.2. Other Services for Families and Communities
3.3.3. Main Takeaway
3.4. Putting It All Together: Conceptual Basis and Objectives of the Apapacho Violence Prevention Parenting Program
3.4.1. Ecological Perspective
3.4.2. Developmental Perspective
3.4.3. A Neuroscience-Informed Perspective on Adult and Child Core Capabilities
3.4.4. Objectives of the Apapacho Violence Prevention Parenting Program
- Prevent violence against children younger than five by parents/caregivers;
- Promote caregivers’ core capabilities for parenting (including knowledge, sense of competence, positive attitudes, adequate expectations, executive functions, and self-regulation) and daily positive-parenting practices (including play, other forms of stimulation, and developmentally appropriate discipline);
- Promote young children’s executive function and self-regulation skills to support their overall development.
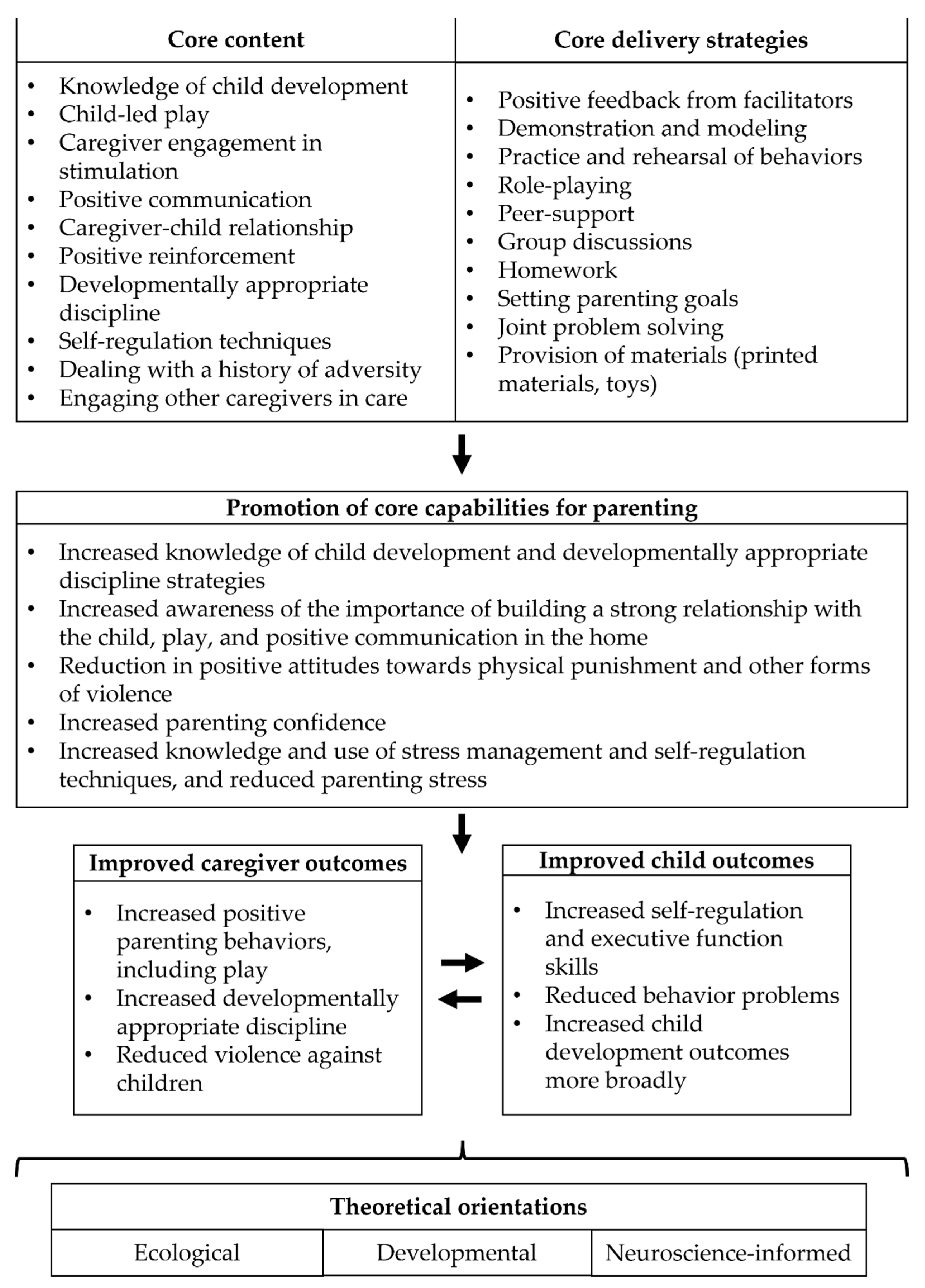
3.4.5. Initial Components of the Theory of Change
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Norman, R.E.; Byambaa, M.; De, R.; Butchart, A.; Scott, J.; Vos, T. The Long-Term Health Consequences of Child Physical Abuse, Emotional Abuse, and Neglect: A Systematic Review and Meta-Analysis. PLoS Med. 2012, 9, e1001349. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.A.; Weissman, D.; Bitrán, D. Childhood Adversity and Neural Development: A Systematic Review. Annu. Rev. Dev. Psychol. 2019, 1, 277–312. [Google Scholar] [CrossRef] [Green Version]
- Afifi, T.O.; Ford, D.; Gershoff, E.T.; Merrick, M.; Grogan-Kaylor, A.; Ports, K.A.; MacMillan, H.L.; Holden, G.W.; Taylor, C.A.; Lee, S.J.; et al. Spanking and adult mental health impairment: The case for the designation of spanking as an adverse childhood experience. Child Abus. Negl. 2017, 71, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.A., III; Gabard-Durnam, L.J. Early Adversity and Critical Periods: Neurodevelopmental Consequences of Violating the Expectable Environment. Trends Neurosci. 2020, 43, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Hillis, S.; Mercy, J.; Amobi, A.; Kress, H. Global Prevalence of Past-year Violence against Children: A Systematic Review and Minimum Estimates. Pediatrics 2016, 137, e20154079. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. A Familiar Face: Violence in the Lives of Children and Adolescents; UNICEF: New York, NY, USA, 2017. [Google Scholar]
- UN World Health Organization. INSPIRE: Seven Strategies for Ending Violence Against Children; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Cuartas, J.; McCoy, D.C.; Rey-Guerra, C.; Britto, P.R.; Beatriz, E.; Salhi, C. Early childhood exposure to non-violent discipline and physical and psychological aggression in low- and middle-income countries: National, regional, and global prevalence estimates. Child Abus. Negl. 2019, 92, 93–105. [Google Scholar] [CrossRef] [PubMed]
- McCoy, D.C.; Seiden, J.; Cuartas, J.; Pisani, L.; Waldman, M. Estimates of a multidimensional index of nurturing care in the next 1000 days of life for children in low-income and middle-income countries: A modelling study. Lancet Child Adolesc. Health 2022, 6, 324–334. [Google Scholar] [CrossRef]
- Bourgault, S.; Peterman, A.; O’Donnell, M. Violence against Women and Children during COVID-19—One Year on and 100 Papers in: A Fourth Research Round Up. 2021. Available online: https://www.cgdev.org/publication/violence-against-women-and-children-during-covid-19-one-year-and-100-papers-fourth (accessed on 13 March 2022).
- Save the Children. Stolen Childhoods, End of Childhood Report 2017. 2017. Available online: https://resourcecentre.savethechildren.net/document/stolen-childhoods-end-childhood-report-2017/ (accessed on 18 March 2022).
- Cuartas, J. Physical punishment against the early childhood in Colombia: National and regional prevalence, sociodemographic gaps, and ten-year trends. Child. Youth Serv. Rev. 2018, 93, 428–440. [Google Scholar] [CrossRef]
- Cuartas, J.; Grogan-Kaylor, A.; Ma, J.; Castillo, B. Civil conflict, domestic violence, and poverty as predictors of corporal punishment in Colombia. Child Abus. Negl. 2019, 90, 108–119. [Google Scholar] [CrossRef]
- Gobierno de Colombia. Estrategia Nacional Pedagógica y de Prevención del Castigo Físico, Tratos Crueles, Humillantes o Degradantes Contra Niños, Niñas y Adolescentes; Gobierno de Colombia: Bogotá, Colombia, 2021. [Google Scholar]
- Skar, A.S.; Sherr, L.; Macedo, A.; Tetzchner, S.V.; Fostervold, K.I. Evaluation of Parenting Interventions to Prevent Violence Against Children in Colombia: A Randomized Controlled Trial. J. Interpers. Violenc 2021, 36, Np1098–Np1126. [Google Scholar] [CrossRef]
- Scott, S.; Gardner, F. Parenting programs. In Rutter’s Child and Adolescent Psychiatry; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 483–495. [Google Scholar]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Ip, P.; Fernald, L.C.H.; et al. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef] [Green Version]
- Jeong, J.; Franchett, E.E.; Ramos de Oliveira, C.V.; Rehmani, K.; Yousafzai, A.K. Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Med. 2021, 18, e1003602. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.P.; Chang, S.M.; Smith, J.A.; Baker-Henningham, H. The Reach up Early Childhood Parenting Program: Origins, Content, and Implementation. Zero Three 2018, 38, 37–43. [Google Scholar]
- Chen, M.; Chan, K.L. Effects of Parenting Programs on Child Maltreatment Prevention: A Meta-Analysis. Trauma Violence Abus. 2015, 17, 88–104. [Google Scholar] [CrossRef]
- McCoy, A.; Melendez-Torres, G.J.; Gardner, F. Parenting interventions to prevent violence against children in low- and middle-income countries in East and Southeast Asia: A systematic review and multi-level meta-analysis. Child Abus. Negl. 2020, 103, 104444. [Google Scholar] [CrossRef]
- Coore Desai, C.; Reece, J.-A.; Shakespeare-Pellington, S. The prevention of violence in childhood through parenting programmes: A global review. Psychol. Health Med. 2017, 22, 166–186. [Google Scholar] [CrossRef] [Green Version]
- Francis, T.; Baker-Henningham, H. The Irie Homes Toolbox: A cluster randomized controlled trial of an early childhood parenting program to prevent violence against children in Jamaica. Child. Youth Serv. Rev. 2021, 126, 106060. [Google Scholar] [CrossRef]
- McCoy, A.; Lachman, J.M.; Ward, C.L.; Tapanya, S.; Poomchaichote, T.; Kelly, J.; Mukaka, M.; Cheah, P.Y.; Gardner, F. Feasibility pilot of an adapted parenting program embedded within the Thai public health system. BMC Public Health 2021, 21, 1009. [Google Scholar] [CrossRef]
- Ward, C.L.; Wessels, I.M.; Lachman, J.M.; Hutchings, J.; Cluver, L.D.; Kassanjee, R.; Nhapi, R.; Little, F.; Gardner, F. Parenting for Lifelong Health for Young Children: A randomized controlled trial of a parenting program in South Africa to prevent harsh parenting and child conduct problems. J. Child Psychol. Psychiatry 2020, 61, 503–512. [Google Scholar] [CrossRef]
- Altafim, E.R.P.; Linhares, M.B.M. Preventive intervention for strengthening effective parenting practices: A randomized controlled trial. J. Appl. Dev. Psychol. 2019, 62, 160–172. [Google Scholar] [CrossRef]
- Baker-Henningham, H.; Walker, S.; Powell, C.; Gardner, J.M. A pilot study of the Incredible Years Teacher Training programme and a curriculum unit on social and emotional skills in community pre-schools in Jamaica. Child Care Health Dev. 2009, 35, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Mejia, A.; Calam, R.; Sanders, M.R. A Pilot Randomized Controlled Trial of a Brief Parenting Intervention in Low-Resource Settings in Panama. Prev. Sci. 2015, 16, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Sumargi, A.; Sofronoff, K.; Morawska, A. A Randomized-Controlled Trial of the Triple P-Positive Parenting Program Seminar Series with Indonesian Parents. Child Psychiatry Hum. Dev. 2015, 46, 749–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, F. Parenting interventions: How well do they transport from one country to another? J. Am. Acad. Child Adolesc. Psychiatry 2017, 55, 610–670. [Google Scholar]
- Leijten, P.; Melendez-Torres, G.J.; Knerr, W.; Gardner, F. Transported Versus Homegrown Parenting Interventions for Reducing Disruptive Child Behavior: A Multilevel Meta-Regression Study. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 610–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundell, K.; Beelmann, A.; Hasson, H.; von Thiele Schwarz, U. Novel Programs, International Adoptions, or Contextual Adaptations? Meta-Analytical Results from German and Swedish Intervention Research. J. Clin. Child Adolesc. Psychol. 2016, 45, 784–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morelli, G.; Bard, K.; Chaudhary, N.; Gottlieb, A.; Keller, H.; Murray, M.; Quinn, N.; Rosabal-Coto, M.; Scheidecker, G.; Takada, A.; et al. Bringing the Real World Into Developmental Science: A Commentary on Weber, Fernald, and Diop (2017). Child Dev. 2018, 89, e594–e603. [Google Scholar] [CrossRef] [Green Version]
- Morelli, G.; Quinn, N.; Chaudhary, N.; Vicedo, M.; Rosabal-Coto, M.; Keller, H.; Murray, M.; Gottlieb, A.; Scheidecker, G.; Takada, A. Ethical Challenges of Parenting Interventions in Low- to Middle-Income Countries. J. Cross-Cult. Psychol. 2017, 49, 5–24. [Google Scholar] [CrossRef]
- Embry, D.; Biglan, A. Evidence-based Kernels: Fundamental Units of Behavioral Influence. Clin. Child Fam. Psychol. Rev. 2008, 11, 75–113. [Google Scholar] [CrossRef] [Green Version]
- Blase, K.; Fixsen, D. Core Intervention Components: Identifying and Operationalizing What Makes Programs Work; U.S. Department of Health and Human Services: Washington, DC, USA, 2013.
- Lachman, J.M.; Sherr, L.T.; Cluver, L.; Ward, C.L.; Hutchings, J.; Gardner, F. Integrating Evidence and Context to Develop a Parenting Program for Low-Income Families in South Africa. J. Child Fam. Stud. 2016, 25, 2337–2352. [Google Scholar] [CrossRef]
- Francis, T.; Baker-Henningham, H. Design and Implementation of the Irie Homes Toolbox: A Violence Prevention, Early Childhood, Parenting Program. Front. Public Health 2020, 8, 582961. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for Implementation Research: Conceptual Distinctions, Measurement Challenges, and Research Agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [Green Version]
- Movsisyan, A.; Arnold, L.; Evans, R.; Hallingberg, B.; Moore, G.; O’Cathain, A.; Pfadenhauer, L.M.; Segrott, J.; Rehfuess, E. Adapting evidence-informed complex population health interventions for new contexts: A systematic review of guidance. Implement. Sci. 2019, 14, 105. [Google Scholar] [CrossRef] [Green Version]
- Dawson-Squibb, J.-J.; Davids, E.L.; Chase, R.; Puffer, E.; Rasmussen, J.D.M.; Franz, L.; de Vries, P.J. Bringing Parent–Child Interaction Therapy to South Africa: Barriers and Facilitators and Overall Feasibility—First Steps to Implementation. Int. J. Environ. Res. Public Health 2022, 19, 4450. [Google Scholar] [CrossRef] [PubMed]
- van der Put, C.E.; Assink, M.; Gubbels, J.; Boekhout van Solinge, N.F. Identifying Effective Components of Child Maltreatment Interventions: A Meta-analysis. Clinical Child and Family Psychology Review 2018, 21, 171–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melendez-Torres, G.J.; Leijten, P.; Gardner, F. What are the Optimal Combinations of Parenting Intervention Components to Reduce Physical Child Abuse Recurrence? Reanalysis of a Systematic Review using Qualitative Comparative Analysis. Child Abus. Rev. 2019, 28, 181–197. [Google Scholar] [CrossRef]
- Temcheff, C.E.; Letarte, M.-J.; Boutin, S.; Marcil, K. Common components of evidence-based parenting programs for preventing maltreatment of school-age children. Child Abus. Negl. 2018, 80, 226–237. [Google Scholar] [CrossRef]
- Wyatt Kaminski, J.; Valle, L.A.; Filene, J.H.; Boyle, C.L. A Meta-analytic Review of Components Associated with Parent Training Program Effectiveness. J. Abnorm. Child Psychol. 2008, 36, 567–589. [Google Scholar] [CrossRef]
- Garland, A.F.; Hawley, K.M.; Brookman-Frazee, L.; Hurlburt, M.S. Identifying Common Elements of Evidence-Based Psychosocial Treatments for Children’s Disruptive Behavior Problems. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 505–514. [Google Scholar] [CrossRef]
- Leijten, P.; Gardner, F.; Melendez-Torres, G.J.; van Aar, J.; Hutchings, J.; Schulz, S.; Knerr, W.; Overbeek, G. Meta-Analyses: Key Parenting Program Components for Disruptive Child Behavior. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 180–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betancourt, T.S.; Jensen, S.K.G.; Barnhart, D.A.; Brennan, R.T.; Murray, S.M.; Yousafzai, A.K.; Farrar, J.; Godfroid, K.; Bazubagira, S.M.; Rawlings, L.B.; et al. Promoting parent-child relationships and preventing violence via home-visiting: A pre-post cluster randomised trial among Rwandan families linked to social protection programmes. BMC Public Health 2020, 20, 621. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.K.; Placencio-Castro, M.; Murray, S.M.; Brennan, R.T.; Goshev, S.; Farrar, J.; Yousafzai, A.; Rawlings, L.B.; Wilson, B.; Habyarimana, E.; et al. Effect of a home-visiting parenting program to promote early childhood development and prevent violence: A cluster-randomized trial in Rwanda. BMJ Glob. Health 2021, 6, e003508. [Google Scholar] [CrossRef] [PubMed]
- Dybdahl, R. Children and Mothers in War: An Outcome Study of a Psychosocial Intervention Program. Child Dev. 2001, 72, 1214–1230. [Google Scholar] [CrossRef]
- Lachman, J.M.; Cluver, L.; Ward, C.L.; Hutchings, J.; Mlotshwa, S.; Wessels, I.; Gardner, F. Randomized controlled trial of a parenting program to reduce the risk of child maltreatment in South Africa. Child Abus. Negl. 2017, 72, 338–351. [Google Scholar] [CrossRef] [Green Version]
- Lachman, J.M.; Alampay, L.P.; Jocson, R.M.; Alinea, C.; Madrid, B.; Ward, C.; Hutchings, J.; Mamauag, B.L.; Garilao, M.A.V.F.V.; Gardner, F. Effectiveness of a parenting programme to reduce violence in a cash transfer system in the Philippines: RCT with follow-up. Lancet Reg. Health–West. Pac. 2021, 17, 100279. [Google Scholar] [CrossRef]
- Oveisi, S.; Ardabili, H.E.; Dadds, M.R.; Majdzadeh, R.; Mohammadkhani, P.; Rad, J.A.; Shahrivar, Z. Primary prevention of parent-child conflict and abuse in Iranian mothers: A randomized-controlled trial. Child Abus. Negl. 2010, 34, 206–213. [Google Scholar] [CrossRef]
- Puffer, E.S.; Green, E.P.; Chase, R.M.; Sim, A.L.; Zayzay, J.; Friis, E.; Garcia-Rolland, E.; Boone, L. Parents make the difference: A randomized-controlled trial of a parenting intervention in Liberia. Glob. Ment. Health 2015, 2, e15. [Google Scholar] [CrossRef] [Green Version]
- Rincón, P.; Cova, F.; Saldivia, S.; Bustos, C.; Grandón, P.; Inostroza, C.; Streiner, D.; Bühring, V.; King, M. Effectiveness of a Positive Parental Practices Training Program for Chilean Preschoolers’ Families: A Randomized Controlled Trial. Front. Psychol. 2018, 9, 1751. [Google Scholar] [CrossRef] [Green Version]
- Santini, P.M.; Williams, L.C.A. A randomized controlled trial of an intervention program to Brazilian mothers who use corporal punishment. Child Abus. Negl. 2017, 71, 80–91. [Google Scholar] [CrossRef]
- Araujo, M.C.; Dormal, M.; Grantham-McGregor, S.; Lazarte, F.; Rubio-Codina, M.; Schady, N. Home visiting at scale and child development. J. Public Econ. Plus 2021, 2, 100003. [Google Scholar] [CrossRef]
- Cerna-Turoff, I.; Fang, Z.; Meierkord, A.; Wu, Z.; Yanguela, J.; Bangirana, C.A.; Meinck, F. Factors Associated with Violence Against Children in Low- and Middle-Income Countries: A Systematic Review and Meta-Regression of Nationally Representative Data. Trauma Violence Abus. 2021, 22, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Fry, D.; Padilla, K.; Germanio, A.; Lu, M.; Ivatury, S.; Vindrola, S. Violence against Children in Latin America and the Caribbean 2015–2021: A Systematic Review; UNICEF: New York, NY, USA, 2021. [Google Scholar]
- Ward, K.P.; Grogan-Kaylor, A.; Pace, G.T.; Cuartas, J.; Lee, S.J. A Multilevel Ecological Analysis of the Predictors of Spanking across 65 Countries. BMJ Open 2021, 11, e046075. [Google Scholar] [CrossRef] [PubMed]
- Lansford, J.E.; Godwin, J.; Uribe Tirado, L.M.; Zelli, A.; Al-Hassan, S.M.; Bacchini, D.; Bombi, A.S.; Bornstein, M.H.; Chang, L.; Deater-Deckard, K.; et al. Individual, family, and culture level contributions to child physical abuse and neglect: A longitudinal study in nine countries. Dev. Psychopathol. 2015, 27, 1417–1428. [Google Scholar] [CrossRef] [Green Version]
- Cuartas, J. Neighborhood crime undermines parenting: Violence in the vicinity of households as a predictor of aggressive discipline. Child Abus. Negl. 2018, 76, 388–399. [Google Scholar] [CrossRef] [Green Version]
- Cicchetti, D.; Toth, S.L.; Maughan, A. An ecological–transactional model of child maltreatment. In Handbook of Developmental Psychopathology, 2nd ed.; Kluwer Academic Publishers: Dordrecht, The Netherlands, 2000; pp. 689–722. [Google Scholar]
- Bronfenbrenner, U.; Morris, P. The Bioecological Model of Human Development. In Handbook of Child Psychology; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Instituto Colombiano de Bienestar Familiar (ICBF). Manual Operativo: Modalidad Institucional Para la Atención a la Primera Infancia; Instituto Colombiano de Bienestar Familiar (ICBF): Bogotá, Colombia, 2022. [Google Scholar]
- Bernal, R.; Ramírez, S.M. Improving the quality of early childhood care at scale: The effects of “From Zero to Forever”. World Dev. 2019, 118, 91–105. [Google Scholar] [CrossRef]
- Maldonado-Carreño, C.; Yoshikawa, H.; Escallón, E.; Ponguta, L.A.; Nieto, A.M.; Kagan, S.L.; Rey-Guerra, C.; Cristancho, J.C.; Mateus, A.; Caro, L.A.; et al. Measuring the quality of early childhood education: Associations with children’s development from a national study with the IMCEIC tool in Colombia. Child Dev. 2022, 93, 254–268. [Google Scholar] [CrossRef]
- Instituto Colombiano de Bienestar Familiar (ICBF). Manual Operativo: Modalidad Familiar Para la Atención a la Primera Infancia; Instituto Colombiano de Bienestar Familiar (ICBF): Bogotá, Colombia, 2022. [Google Scholar]
- Attanasio, O.; Baker-Henningham, H.; Bernal, R.; Meghir, C.; Pineda, D.; Rubio-Codina, M. Early Stimulation and Nutrition: The Impacts of a Scalable Intervention. J. Eur. Econ. Assoc. 2022, jvac005. [Google Scholar] [CrossRef]
- Instituto Colombiano de Bienestar Familiar (ICBF). Manual Operativo: Modalidad Comunitaria Para la Atención a la Primera Infancia; Instituto Colombiano de Bienestar Familiar (ICBF): Bogotá, Colombia, 2022. [Google Scholar]
- Bernal, R.; Fernández, C. Subsidized childcare and child development in Colombia: Effects of Hogares Comunitarios de Bienestar as a function of timing and length of exposure. Soc. Sci. Med. 2013, 97, 241–249. [Google Scholar] [CrossRef]
- Motta, A.; Yoshikawa, H. Progress toward Sustainable Development Goal 4 in a Culturally Diverse World: The Experience of Modalidad Propia in Colombia. In Developmental Science and Sustainable Development Goals for Children and Youth; Verma, S., Petersen, A.C., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 59–75. [Google Scholar]
- Instituto Colombiano de Bienestar Familiar (ICBF). Manual Operativo: Modalidad Propia e Intercultural Para la Atención a La Primera Infancia; Instituto Colombiano de Bienestar Familiar (ICBF): Bogotá, Colombia, 2022. [Google Scholar]
- Instituto Colombiano de Bienestar Familiar (ICBF). Manual Operativo: Mi Familia; Instituto Colombiano de Bienestar Familiar (ICBF): Bogotá, Colombia, 2022. [Google Scholar]
- Berens, A.E.; Nelson, C.A. Neurobiology of fetal and infant development: Implications for infant mental health. In Handbook of Infant Mental Health; Zeanah, C.H., Ed.; Guilford Press: New York, NY, USA, 2019. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1986; p. xiii + x617. [Google Scholar]
- Black, M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Solis, S.L.; Liu, C.W.; Popp, J.M. Learning to Cope through Play: Playful Learning as an Approach to Support Children’s Coping during Times of Heightened Stress and Adversity. 2020. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiYjJj8m_P4AhW9sVYBHfiwBM8QFnoECAwQAQ&url=https%3A%2F%2Fcms.learningthroughplay.com%2Fmedia%2Fjqifsynb%2Flearning-to-cope-through-play.pdf&usg=AOvVaw1GBErNvN5Uhggn6BdDWPCF (accessed on 20 April 2022).
- Zosh, J.M.; Hopkins, E.J.; Liu, H.J.; Neale, D.; Hirsh-Pasek, K.; Solis, S.L.; Whitebread, D. Learning Through Play: A Review of the Evidence; LEGO Fonden: Billund, Denmark, 2017. [Google Scholar]
- UNICEF. Designing Parenting Programmes for Violence Prevention: A Guidance Note; UNICEF: New York, NY, USA, 2020. [Google Scholar]
- Cuartas, J.; Rey-Guerra, C. Guidance for Families to Prevent Violence in Early Childhood in the Time of COVID-19: Toolkit; UNICEF: New York, NY, USA, 2020. [Google Scholar]
- UNICEF. Care for Child Development; UNICEF: New York, NY, USA, 2012. [Google Scholar]
- Johnson, M.H.; De Haan, M. Developmental Cognitive Neuroscience: An Introduction, 4th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2015. [Google Scholar]
- Durrant, J. Positive Discipline in Everyday Parenting, 4th ed.; Save the Children Sweden. 2016. Available online: https://resourcecentre.savethechildren.net/document/positive-discipline-everyday-parenting-pdep-fourth-edition/ (accessed on 12 February 2022).
- Magnuson, K.A.; Schindler, H.S. Supporting Children’s Early Development by Building Caregivers’ Capacities and Skills: A Theoretical Approach Informed by New Neuroscience Research. J. Fam. Theory Rev. 2019, 11, 59–78. [Google Scholar] [CrossRef] [Green Version]
- Center on the Developing Child at Harvard University. Building Core Capabilities for Life: The Science Behind the Skills Adults Need to Succeed in Parenting and in the Workplace; Center on the Developing Child at Harvard University: Cambridge, MA, USA, 2016. [Google Scholar]
- Liew, J. Effortful Control, Executive Functions, and Education: Bringing Self-Regulatory and Social-Emotional Competencies to the Table. Child Dev. Perspect. 2012, 6, 105–111. [Google Scholar] [CrossRef]
- Bornstein, M.H. Children’s Parents. In Handbook of Child Psychology and Developmental Science; Lerner, R.M., Bornstein, M.H., Leventhal, T., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2015; Volume 4, pp. 55–132. [Google Scholar]
- Center on the Developing Child at Harvard University. Enhancing and Practicing Executive Function Skills with Children from Infancy to Adolescence; Center on the Developing Child at Harvard University: Cambridge, MA, USA, 2014. [Google Scholar]
- National Scientific Council on the Developing Child. Supportive Relationships and Active Skill-Building Strengthen the Foundations of Resilience; Working Paper 13; National Scientific Council on the Developing Child: Cambridge, MA, USA, 2015. [Google Scholar]
- Cicchetti, D. Annual Research Review: Resilient functioning in maltreated children–past, present, and future perspectives. J. Child Psychol. Psychiatry 2013, 54, 402–422. [Google Scholar] [CrossRef]
- Gershoff, E.T.; Lee, S.J.; Durrant, J. Promising intervention strategies to reduce parents’ use of physical punishment. Child Abus. Negl. 2017, 71, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Holland, G.W.O.; Holden, G.W. Changing orientations to corporal punishment: A randomized, control trial of the efficacy of a motivational approach to psycho-education. Psychol. Violence 2016, 6, 233–242. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Outcome | Definition | Expected Outputs of Using Evidence-Based Core Components as Starting Point |
|---|---|---|
| Acceptability | Extent to which the intervention or program is agreeable or satisfactory to key implementation stakeholders | The development of the intervention is more flexible and can respond to local needs, preferences, and culture, ensuring acceptability |
| Adoption | Initial intention, decision, or action to implement the intervention or program | The interventions can be developed with active participation of key stakeholders to ensure future adoption |
| Appropriateness | Refers to the fit, relevance, or compatibility of the intervention or program for a specific setting, culture, social service or infrastructure, implementation stakeholder, user, and for addressing the unmet need or problem | Core components can be adapted through qualitative and quantitative research and rapid-learning cycles to the specific setting, culture, and social infrastructure, maximizing its appropriateness |
| Feasibility | Extent to which the intervention or program can be successfully employed or implemented by the implementation stakeholders within a particular social infrastructure | Combining core components with an in-depth knowledge of the local institutional infrastructure allows adapting these components to fit existing services, social infrastructure, and implementation capacity, increasing its feasibility |
| Fidelity | Degree to which the intervention or program is implemented as planned in the original protocol or design | Core components can be adapted to meet the local implementation capacity (e.g., characteristics of potential facilitators), making it more likely that the intervention can be implemented with fidelity |
| Integration | Degree to which the intervention or program integrates within an existing social service or infrastructure | Core components underlying the intervention can be adapted to fit existing social services and infrastructure, increasing the integration of the intervention |
| Sustainability | Extent to which an intervention or program can be maintained or institutionalized within an existing social service or infrastructure | As the intervention is designed specifically for the context, using existing services and existing staff, it is more likely to be sustainable at scale |
| Program | Evaluation Country | Format | Selected Key Content | Selected Key Delivery Strategies |
|---|---|---|---|---|
| ACT Raising Safe Kids | Brazil [26] | An initial meeting and eight 2-h group sessions, once a week for eight weeks | Knowledge and attitudes
|
|
| Cuna Más | Peru [58] | Weekly 1-h home visits | Family relationships
|
|
| Día a Día | Chile [56] | Six 2-h weekly sessions in preschool education centers | Play and other stimulation
|
|
| Adaptation of the International Child Development Programme | Bosnia [51] Colombia [15] | Group meetings, but different number of sessions in different countries | Knowledge and attitudes
|
|
| Irie Homes Toolbox | Jamaica [23] | Group meetings, 90-min sessions, once per week for eight weeks | Knowledge and attitudes
|
|
| Parenting for Lifelong Health | Philippines [53] South Africa [25,52] Thailand [24] | Group meetings, 2–3 h sessions, once per week for 12 weeks | Knowledge and attitudes
|
|
| Parents Make the Difference | Liberia [55] | Group-based sessions and one home visit, 2-h each for 10 weeks | Knowledge and attitudes
|
|
| Triple P | Indonesia [29] Panama [28] | Three 90-min seminars, once per week | Emotional self-regulation
|
|
| Projeto Parceria | Brazil [57] | 16 weekly sessions, 50–60 min each | Knowledge and attitudes
|
|
| SOS! Help for Parents | Iran [54] | Two 2-h sessions, one per week | Knowledge and attitudes
|
|
| Sugira Muryango | Rwanda [49,50] | 12 home visits, 90-min each | Knowledge and attitudes
|
|
| Modality (Children and Pregnant Women in 2022) | Approach | Target Population | Examples of Services |
|---|---|---|---|
| Institutional (461,525) | Center-based | Targets children between ages 2 to 5 years |
|
| Family (661,100) | Home-based | Children younger than six years, prioritizing children younger than five, who do not have access to other modalities of early care and education, with a focus on rural areas |
|
| Community (473,599) | Community-based | Children between ages 18 months and 5 years from urban and rural areas |
|
| Ethnic and Intercultural (95,306) | Multiple approaches | Children younger than five years from ethnic and rural communities |
|
| Some Needs and Risk Factors Related to VAC | Potential Content of Parenting Programs to Prevent VAC | ||
|---|---|---|---|
| Children | Caregivers | ||
| Childbirth |
|
|
|
| Infancy (<12 months) |
|
|
|
| Toddlerhood (12–36 months) |
|
|
|
| Early childhood (3–6 years) |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuartas, J.; Baker-Henningham, H.; Cepeda, A.; Rey-Guerra, C.; Instituto Colombiano de Bienestar Familiar (ICBF) Early Childhood Team. The Apapacho Violence Prevention Parenting Program: Conceptual Foundations and Pathways to Scale. Int. J. Environ. Res. Public Health 2022, 19, 8582. https://doi.org/10.3390/ijerph19148582
Cuartas J, Baker-Henningham H, Cepeda A, Rey-Guerra C, Instituto Colombiano de Bienestar Familiar (ICBF) Early Childhood Team. The Apapacho Violence Prevention Parenting Program: Conceptual Foundations and Pathways to Scale. International Journal of Environmental Research and Public Health. 2022; 19(14):8582. https://doi.org/10.3390/ijerph19148582
Chicago/Turabian StyleCuartas, Jorge, Helen Baker-Henningham, Andrés Cepeda, Catalina Rey-Guerra, and Instituto Colombiano de Bienestar Familiar (ICBF) Early Childhood Team. 2022. "The Apapacho Violence Prevention Parenting Program: Conceptual Foundations and Pathways to Scale" International Journal of Environmental Research and Public Health 19, no. 14: 8582. https://doi.org/10.3390/ijerph19148582
APA StyleCuartas, J., Baker-Henningham, H., Cepeda, A., Rey-Guerra, C., & Instituto Colombiano de Bienestar Familiar (ICBF) Early Childhood Team. (2022). The Apapacho Violence Prevention Parenting Program: Conceptual Foundations and Pathways to Scale. International Journal of Environmental Research and Public Health, 19(14), 8582. https://doi.org/10.3390/ijerph19148582