
Italian Validation of the 12-Item Version of the Burnout Assessment Tool (BAT-12)

 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Burnout
2.2.2. Job Demands
2.2.3. Job Resources
2.2.4. Personal Resources
2.2.5. Positive Job Attitudes
2.3. Strategy of Analysis
2.3.1. Confirmatory Factor Analysis
- A single-factor model, in which all 12 items measuring the four hypothesized core symptoms (i.e., exhaustion, mental distance, emotional impairment, and cognitive impairment) are loaded on a general burnout factor. The test of such a parsimonious model excludes the influences of method bias on observed item covariances [57].
- A four-correlated factors model, in which the items loaded on the hypothesized four latent dimensions (i.e., core symptoms) and all of their correlations are freely estimated. This model was tested and compared against the second-order model to assess whether the latter can accurately model the relationships among first-order factors.
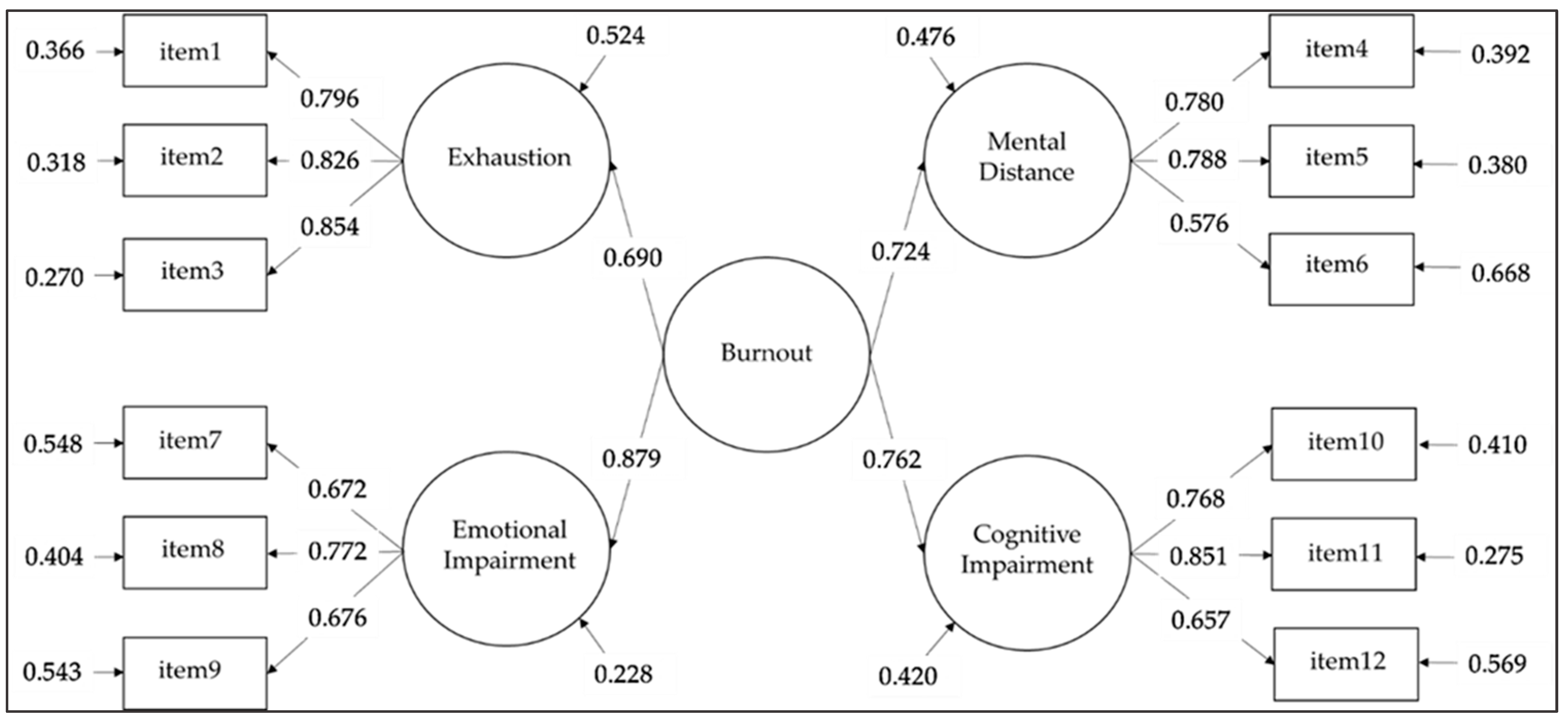
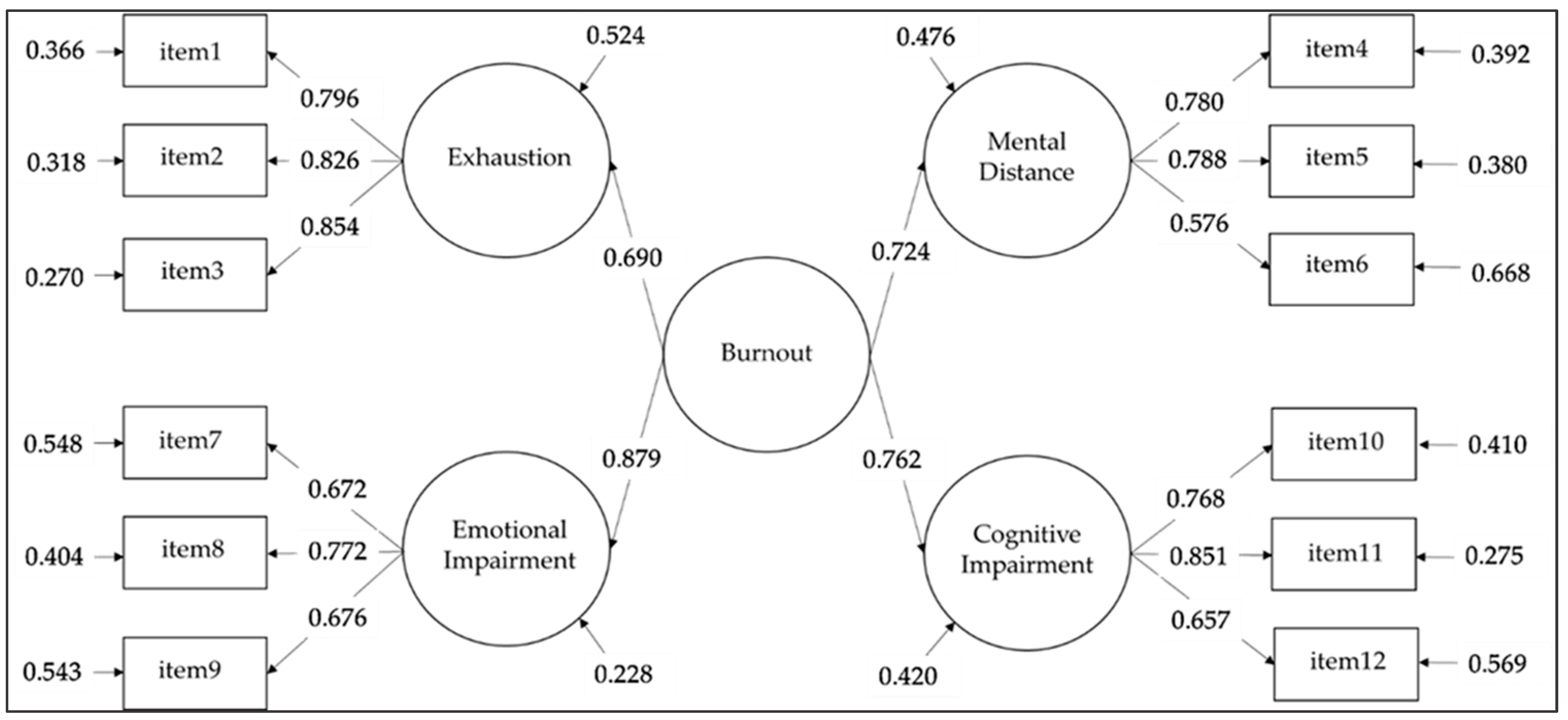
- A second-order model, in which the four core symptoms are loaded on a higher-order burnout factor that explains the covariations between the first-order factors.
- A bi-factor model, in which the items are loaded both onto a general burnout factor and onto the four orthogonal hypothesized core symptoms. This model was tested to exclude whether the correlations among first-order factors are attenuated by differences in how each factor is measured (e.g., content similarities).
2.3.2. Analysis of Covariance
2.3.3. Internal Consistency
2.3.4. Convergent and Discriminant Validity
3. Results
3.1. Confirmatory Factor Analysis
3.2. Measurement Invariance
3.3. Mean Differences
3.4. Reliability and Correlations with Other Dimensions
4. Discussion
4.1. Limitations and Suggestions for Future Research
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Items | Factor Loadings | ||||||
|---|---|---|---|---|---|---|---|
| M | SD | rtot | Exhaustion | Mental Distance | Emotional Impairment | Cognitive Impairment | |
| Al lavoro mi sento mentalmente esausto/a. | 2.63 | 0.953 | 0.724 | 0.796 | |||
| Dopo una giornata di lavoro, per me è difficile recuperare le energie. | 2.56 | 0.992 | 0.751 | 0.826 | |||
| Al lavoro mi sento fisicamente esausto/a | 2.30 | 0.960 | 0.757 | 0.854 | |||
| Ho difficoltà a provare un qualche entusiasmo per il mio lavoro | 2.03 | 0.973 | 0.611 | 0.780 | |||
| Provo una forte avversione per il mio lavoro | 1.52 | 0.776 | 0.621 | 0.788 | |||
| Sono scettico/a rispetto al significato che il mio lavoro ha per gli altri | 2.12 | 1.071 | 0.484 | 0.576 | |||
| Al lavoro mi sento incapace di controllare le mie emozioni. | 1.71 | 0.763 | 0.564 | 0.672 | |||
| * Al lavoro mi capita di arrabbiarmi o sentirmi triste senza sapere perché. | 1.62 | 0.792 | 0.595 | 0.772 | |||
| Al lavoro mi capita di avere delle reazioni esagerate senza volerlo. | 1.48 | 0.650 | 0.579 | 0.676 | |||
| Al lavoro faccio fatica a mantenere l’attenzione. | 1.71 | 0.727 | 0.642 | 0.768 | |||
| * Quando lavoro ho difficoltà a pensare con lucidità. | 1.48 | 0.606 | 0.715 | 0.851 | |||
| Al lavoro faccio degli errori perché penso ad altro. | 1.56 | 0.605 | 0.575 | 0.657 | |||
| Cronbach’s α | 0.866 | 0.735 | 0.748 | 0.794 | |||
References
- Dyer, O. Physician burnout costs US $4.6bn a year, study finds. BMJ 2019, 365, l2361. [Google Scholar] [CrossRef] [PubMed]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef] [PubMed]
- WHO. Burn-Out an “Occupational Phenomenon”: International Classification of Diseases. 2019. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 14 May 2022).
- Maslach, C. Burned-Out. Hum. Behav. 1976, 5, 16–22. [Google Scholar]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Occup. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Lastovkova, A.; Carder, M.; Rasmussen, H.M.; Sjobergg, L.; de Groene, G.J.; Sauni, R.; Vevoda, J.; Vevodova, S.; Lasfargues, G.; Svartegren, M.; et al. Burnout Syndrome as an Occupational Disease in the European Union: An Exploratory Study. Ind. Health 2018, 56, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Salanova, M.; Llorens, S.; Garcia-Renedo, M.; Burriel, R.; Bresó, E.; Schaufeli, W.B. Toward a four-dimensional model of burnout: A multigroup factor-analytic study including depersonalization and cynicism. Educ. Psychol. Meas. 2005, 65, 901–991. [Google Scholar] [CrossRef]
- Borgogni, L.; Consiglio, C.; Alessandri, G.; Schaufeli, W.B. “Do not throw the baby out with the bath water!” interpersonal strain at work and burnout. Eur. J. Work Organ. Psychol. 2012, 21, 875–898. [Google Scholar] [CrossRef] [Green Version]
- De Beer, L.T.; Bianchi, R. Confirmatory factor analysis of the Maslach Burnout Inventory: A Bayesian structural equation modeling approach. Eur. J. Psychol. Assess. 2019, 35, 217–224. [Google Scholar] [CrossRef]
- Galanakis, M.; Moraitou, M.; Garivaldis, F.J.; Stalikas, A. Factorial structure and psychometric properties of the Maslach Burnout Inventory (MBI) in Greek midwives. Eur. J. Psychol. 2009, 5, 52–70. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P.; Jackson, S.E. Maslach Burnout Inventory Manual, 4th ed.; Mind Garden, Inc.: Palo Alto, CA, USA, 2017. [Google Scholar]
- Schaufeli, W.B.; De Witte, H.; Desart, S. De Burnout Assessment Tool (BAT): Een nieuw instrument voor het meten van burn-out. Tijdschr. Klin. Psychol. 2020, 50, 267–283. [Google Scholar]
- Schaufeli, W.B.; De Witte, H.; Desart, S. Handleiding Burnout Assessment Tool (BAT). KU Leuven België Intern. Rapp. 2019. Available online: https://burnoutassessmenttool.be/project_eng/#handleidingenvragenlijst (accessed on 15 February 2022).
- De Beer, L.T.; Schaufeli, W.B.; DeWitte, H.; Hakanen, J.J.; Shimazu, A.; Glaser, J.; Seubert, C.; Bosak, J.; Sinval, J.; Rudnev, M. Measurement invariance of the Burnout Assessment Tool (BAT) across seven cross-national representative samples. Int. J. Environ. Res. Public Health 2020, 17, 5604. [Google Scholar] [CrossRef] [PubMed]
- Cho, S. Validation of the Korean version of the Burnout Assessment Tool (K-BAT): A preliminary study. Korean J. Ind. Organ. Psychol. 2020, 33, 461–499. (In Korean) [Google Scholar] [CrossRef]
- Sakakibara, K.; Shimazu, A.; Toyama, H.; Schaufeli, W.B. Validation of the Japanese Version of the Burnout Assessment Tool (BAT-J). Front. Psychol. 2020, 11, 1819. [Google Scholar] [CrossRef] [PubMed]
- Sinval, J.; Vazquez, A.C.; Hutz, S.; Schaufeli, W.B.; Silva, S. Burnout Assessment Tool (BAT): Validity evidence for Brazil and Portugal. Int. J. Environ. Res. Public Health 2022, 19, 1344. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.; Mazzetti, G.; Schaufeli, W.B. Psychometric properties of the Italian version of the burnout assessment tool (BAT). Int. J. Environ. Res. Public Health 2021, 18, 9469. [Google Scholar] [CrossRef] [PubMed]
- Eisele, G.; Vachon, H.; Lafit, G.; Kuppens, P.; Houben, M.; Myin-Germeys, I.; Viechtbauer, W. The effects of sampling frequency and questionnaire length on perceived burden, compliance, and careless responding in experience sampling data in a student population. Assessment 2020, 29, 136–151. [Google Scholar] [CrossRef]
- Vinueza-Solórzano, A.M.; Portalanza-Chavarría, C.A.; de Freitas, C.P.; Schaufeli, W.B.; De Witte, H.; Hutz, C.S.; Souza Vazquez, A.C. The Ecuadorian version of the Burnout Assessment Tool (BAT): Adaptation and Validation. Int. J. Environ. Res. Public Health 2021, 18, 7121. [Google Scholar] [CrossRef]
- Oprea, B.; Iliescu, D.; De Witte, H. Romanian short version of the Burnout Assessment Tool: Psychometric properties. Eval. Health Prof. 2021, 44, 406–415. [Google Scholar] [CrossRef]
- Hadžibajramović, E.; Schaufeli, W.B.; De Witte, H. Shortening of the Burnout Assessment Tool (BAT)—From 23 to 12 items using content and Rasch analysis. BMC Public Health 2022, 22, 560. [Google Scholar] [CrossRef]
- Kan, F.P.; Raoofi, S.; Rafiei, S.; Khani, S.; Hosseinifard, H.; Tajik, F.; Raoofi, N.; Ahmadi, S.; Ghashghaee, A. A systematic review of the prevalence of anxiety among the general population during the COVID-19 pandemic. J. Affect. Disord. 2021, 293, 391–398. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, D.; Fontanesi, L.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. Parenting-related exhaustion during the Italian COVID-19 lockdown. J. Pediatr. Psychol. 2020, 45, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Schokkenbroek, J.M.; Hardyns, W.; Anrijs, S.; Ponnet, K. Partners in lockdown: Relationship stress in men and women during the COVID-19 pandemic. Couple Fam. Psychol. Res. Pract. 2021, 10, 149–157. [Google Scholar] [CrossRef]
- Chen, H.; Eyoun, K. Do mindfulness and perceived organizational support work? Fear of COVID-19 on restaurant frontline employees’ job insecurity and emotional exhaustion. Int. J. Hosp. Manag. 2021, 94, 102850. [Google Scholar] [CrossRef]
- Aguiar-Quintana, T.; Nguyen, T.H.H.; Araujo-Cabrera, Y.; Sanabria-Díaz, J.M. Do job insecurity, anxiety and depression caused by the COVID-19 pandemic influence hotel employees’ self-rated task performance? The moderating role of employee resilience. Int. J. Hosp. Manag. 2021, 94, 102868. [Google Scholar] [CrossRef] [PubMed]
- Ozamiz-Etxebarria, N.; Idoiaga Mondragon, N.; Bueno-Notivol, J.; Pérez-Moreno, M.; Santabárbara, J. Prevalence of anxiety, depression, and stress among teachers during the CoViD-19 pandemic: A rapid systematic review with meta-analysis. Brain Sci. 2021, 11, 1172. [Google Scholar] [CrossRef] [PubMed]
- Couarraze, S.; Delamarre, L.; Marhar, F.; Quach, B.; Jiao, J.; Avilés Dorlhiac, R.; Saadaoui, F.; Lui, A.S.; Dubis, B.; Antunes, S.; et al. The major worldwide stress of healthcare professionals during the first wave of the COVID-19 pandemic–the international COVISTRESS survey. PLoS ONE 2021, 16, e0257840. [Google Scholar] [CrossRef]
- Fernandez, R.; Sikhosana, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzeh, I.; Alanzeh, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open 2021, 11, e054528. [Google Scholar] [CrossRef]
- Jalili, M.; Niroomand, M.; Hadavand, F.; Zeinali, K.; Fotouhi, A. Burnout among healthcare professionals during COVID-19 pandemic: A cross-sectional study. Int. Arch. Occup. Environ. Health 2021, 94, 1345–1352. [Google Scholar] [CrossRef]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M.; et al. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PLoS ONE 2020, 15, 9. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Job demands-resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Taris, T.W. Models in work and health research: The JDC (S), ERI and JD-R frameworks. In Research Handbook on Work and Well-being; Edward Elgar Publishing: Northampton, MA, USA, 2017. [Google Scholar]
- Schaufeli, W.B.; Bakker, A.B. Job demands, job resources, and their relationship with burnout and engagement: A multi-sample study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef] [Green Version]
- Solinger, O.N.; Van Olffen, W.; Roe, R.A. Beyond the three-component model of organizational commitment. J. Appl. Psychol. 2008, 93, 70–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lofquist, L.H.; Dawis, R.V. Essentials of Person-Environment-Correspondence Counseling; University of Minnesota Press: Minneapolis, MN, USA, 1991. [Google Scholar]
- Bakker, A.B.; Van Veldhoven, M.; Xanthopoulou, D. Beyond the demand-control model: Thriving on high job demands and resources. J. Pers. Psychol. 2010, 9, 3–16. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout Assessment Tool (BAT)—Development, Validity, and Reliability. Int. J. Environ. Res. Public Health 2020, 17, 9495. [Google Scholar] [CrossRef]
- Bowling, N.A.; Khazon, S.; Alarcon, G.M.; Blackmore, C.E.; Bragg, C.B.; Hoepf, M.R.; Barelka, A.; Kennedy, K.; Wang, Q.; Li, H. Building better measures of role ambiguity and role conflict: The validation of new role stressor scales. Work Stress 2017, 31, 1–23. [Google Scholar] [CrossRef]
- Leiter, M.; Maslach, C. Six areas of worklife: A model of the organizational context on burnout. J. Health Hum. Resour. Manag. 1999, 21, 472–489. [Google Scholar]
- Consiglio, C.; Borgogni, L.; Alessandri, G.; Schaufeli, W.B. Does self-efficacy matter for burnout and sickness absenteeism? the mediating role of demands and resources at the individual and team levels. Work Stress 2013, 27, 22–42. [Google Scholar] [CrossRef] [Green Version]
- Morgeson, F.P.; Humphrey, S.E. The Work Design Questionnaire (WDQ): Developing and validating a comprehensive measure for assessing job design and the nature of work. J. Appl. Psychol. 2006, 91, 1321–1339. [Google Scholar] [CrossRef] [Green Version]
- Rondinone, B.M.; Persechino, B.; Castaldi, T.; Valenti, A.; Ferrante, P.; Ronchetti, M.; Iavicoli, S. Work-related stress risk assessment in Italy: The validation study of health safety and executive indicator tool. G. Ital. Med. Lav. Ergon. 2012, 34, 392–399. [Google Scholar]
- Luthans, F.; Youssef, C.M.; Avolio, B.J. Psychological Capital; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Alessandri, G.; Borgogni, L.; Consiglio, C.; Mitidieri, G. Psychometric Properties of the Italian Version of the Psychological Capital Questionnaire. Int. J. Select. Assess. 2015, 23, 149–159. [Google Scholar] [CrossRef]
- Borgogni, L.; Dello Russo, S.; Petitta, L.; Vecchione, M. Predicting job satisfaction and job performance in a privatized organization. Int. Public Manag. J. 2010, 13, 275–296. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Balducci, C.; Fraccaroli, F.; Schaufeli, W.B. Psychometric Properties of the Italian Version of the Utrecht Work Engagement Scale (UWES-9). Eur. J. Psychol. Assess. 2010, 26, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Allen, N.J.; Meyer, J.P. The measurement and antecedents of affective, continuance, and normative commitment. J. Occup. Psychol. 1990, 63, 1–18. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthen & Muthen: Los Angeles, CA, USA, 2017. [Google Scholar]
- Satorra, A.; Bentler, P.M. Scaling corrections for chi-square statistics in covariance structure analysis. In Proceedings of the Business and Economics Sections; American Statistical Association: Boston, MA, USA, 1988; pp. 308–313. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Credé, M.; Harms, P.D. 25 years of higher-order confirmatory factor analysis in the organizational sciences: A critical review and development of reporting recommendations. J. Organ. Behav. 2015, 36, 845–872. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y. Common method biases in behavioural research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with Mplus: Basic Concepts, Applications, and Programming, 1st ed.; Routledge: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Chen, F.F.; Karen, H.S.; Stephen, G.W. Teacher’s corner: Testing measurement invariance of second-order factor models. Struct. Equ. Modeling 2005, 12, 471–492. [Google Scholar] [CrossRef]
- Putnick, D.L.; Bornstein, M.H. Measurement invariance conventions and reporting: The state of the art and future directions for psychological research. Dev. Rev. 2016, 41, 71–90. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.S.; Stein, J.A.; Bentler, P.M. Structural equation analyses of clinical subpopulation differences and comparative treatment outcomes: Characterizing the daily lives of drug addicts. J. Consult. Clin. Psychol. 1994, 62, 488–499. [Google Scholar] [CrossRef] [PubMed]
- Purvanova, R.K.; Muros, J.P. Gender differences in burnout: A meta-analysis. J. Vocat. Behav. 2010, 77, 168–185. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Anderson, R.E.; Babin, B.J.; Black, W.C. Multivariate Data Analysis: A Global Perspective; Pearson Education: Upper Saddle River, NJ, USA, 2010; p. 7. [Google Scholar]
- Mäkikangas, A.; Feldt, T.; Kinnunen, U.; Tolvanen, A. Do low burnout and high work engagement always go hand in hand? Investigation of the energy and identification dimensions in longitudinal data. Anxiety Stress Coping 2012, 25, 93–116. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Deligkaris, P.; Panagopoulou, E.; Montgomery, A.J.; Masoura, E. Job burnout and cognitive functioning: A systematic review. Work Stress 2014, 28, 107–123. [Google Scholar] [CrossRef]
- Kahill, S. Symptoms of professional burnout: A review of the empirical evidence. Can. Psychol. 1988, 29, 284–297. [Google Scholar] [CrossRef]
- Sharma, M.K.; Anand, N.; Singh, P.; Vishwakarma, A.; Mondal, I.; Thakur, P.C.; Kohli, T. Researcher burnout: An overlooked aspect in mental health research in times of COVID-19. Asian J. Psychiatry 2020, 54, 102367. [Google Scholar] [CrossRef]
- Sokal, L.; Trudel, L.E.; Babb, J. Canadian teachers’ attitudes toward change, efficacy, and burnout during the COVID-19 pandemic. Int. J. Educ. Res. Open 2020, 1, 100016. [Google Scholar] [CrossRef]
- Raudenská, J.; Steinerová, V.; Javůrková, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef]
- Meyer, B.; Zill, A.; Dilba, D.; Gerlach, R.; Schumann, S. Employee psychological well-being during the COVID-19 pandemic in Germany: A longitudinal study of demands, resources, and exhaustion. Int. J. Psychol. 2021, 56, 532–550. [Google Scholar] [CrossRef]
| Total Sample (n = 2277) | |
|---|---|
| Gender | |
| Female | 57.4% |
| Male | 42.6% |
| Age | |
| Up to 30 years old | 13.9% |
| From 31 to 50 years old | 59.0% |
| More than 50 years old | 27.1% |
| Work sector | |
| Health, social services, law enforcement | 26.4% |
| Business services | 7.7% |
| Industry | 5.1% |
| Public Administration | 41.5% |
| Educational sector | 14.4% |
| Wholesale or retail trade, repairs | 0.6% |
| Construction | 0.4% |
| Tourism, hospitality, catering | 0.6% |
| Other | 3.2% |
| Education level | |
| Middle School | 6.0% |
| High School | 27.0% |
| University degree | 50.3% |
| Post-graduate degree | 16.7% |
| Work contract | |
| Open-ended contract | 74.6% |
| Fixed-term contract | 15.7% |
| Other | 9.7% |
| Working hours by contract | |
| Full time | 55.7% |
| Part-time | 44.3% |
| Job tenure | |
| Up to 10 years | 58.1% |
| From 11 to 20 years | 25.4% |
| More than 20 years | 16.5% |
| Time of administration | |
| Pre-COVID-19 pandemic | 57.5% |
| During COVID-19 pandemic | 42.5% |
| Model Fit | |||||||
|---|---|---|---|---|---|---|---|
| Model (M) | χ2 | df | Scaling Correction Factor | RMSEA (90% CI) | CFI | TLI | SRMR |
| M1: Single-factor model | 2586.476 ** | 54 | 1.2813 | 0.144 (0.139–0.148) | 0.705 | 0.640 | 0.086 |
| M2: Four-correlated factors model | 195.829 ** | 48 | 1.2342 | 0.037 (0.031–0.042) | 0.983 | 0.976 | 0.027 |
| M3: Second-order model | 218.042 ** | 50 | 1.2399 | 0.038 (0.033–0.044) | 0.980 | 0.974 | 0.031 |
| M4: Bi-factor model | 163.79 ** | 42 | 1.2244 | 0.036 (0.030–0.042) | 0.986 | 0.978 | 0.025 |
| Model difference | |||||||
| Model comparison | ΔSB χ2 | Δdf | ΔCFI | ΔTLI | ΔRMSEA | ΔSRMR | |
| M2-M1 | 1852.94 ** | 6 | 0.278 | 0.336 | −0.107 | −0.059 | |
| M3-M2 | 20.81 ** | 2 | −0.003 | −0.002 | 0.001 | 0.004 | |
| M4-M3 | 52.83 ** | 8 | 0.006 | 0.004 | −0.002 | −0.006 | |
| M4-M2 | 31.58 ** | 6 | 0.003 | 0.002 | −0.001 | −0.002 | |
| Model Fit | |||||||
|---|---|---|---|---|---|---|---|
| Model (M) | χ2 | df | Scaling Correction Factor | RMSEA (90% CI) | CFI | TLI | SRMR |
| Baseline Pre-COVID-19 | 157.068 ** | 50 | 1.2986 | 0.040 (0.033–0.047) | 0.978 | 0.970 | 0.033 |
| Baseline During COVID-19 | 121.031 ** | 50 | 1.1681 | 0.039 (0.030–0.048) | 0.981 | 0.975 | 0.036 |
| M1: Configural invariance | 279.923 ** | 100 | 1.2304 | 0.040 (0.034–0.045) | 0.979 | 0.972 | 0.035 |
| M2: Metric invariance (first-order factor loadings invariant) | 310.635 ** | 108 | 1.2164 | 0.041 (0.035–0.046) | 0.976 | 0.971 | 0.040 |
| M3: Metric invariance (first- and second-order factor loadings invariant) | 317.436 ** | 111 | 1.2123 | 0.040 (0.035–0.047) | 0.976 | 0.971 | 0.043 |
| M4: Scalar invariance (intercepts of measured variables invariant) | 348.827 ** | 119 | 1.1990 | 0.041 (0.036–0.046) | 0.974 | 0.971 | 0.043 |
| M5: Scalar invariance (intercepts of measured variables and first-order factors invariant) | 411.177 ** | 122 | 1.1950 | 0.046 (0.041–0.050) | 0.966 | 0.964 | 0.051 |
| M6: Strict invariance (residual variances of measured variables) | 466.668 ** | 134 | 1.2297 | 0.047 (0.042–0.051) | 0.961 | 0.962 | 0.061 |
| M7: Strict invariance (residual variances of measured variables and first-order factors) | 491.095 ** | 138 | 1.2327 | 0.047 (0.043–0.052) | 0.959 | 0.961 | 0.071 |
| Model difference | |||||||
| Model comparison | ΔSB χ2 | Δdf | ΔCFI | ΔTLI | ΔRMSEA | ΔSRMR | |
| M2-M1 | 32.11 ** | 8 | −0.003 | −0.001 | 0.001 | 0.005 | |
| M3-M2 | 6.55 (n.s.) | 3 | 0.000 | 0.000 | −0.001 | 0.003 | |
| M4-M3 | 32.94 ** | 8 | −0.002 | 0.000 | 0.001 | 0.000 | |
| M5-M4 | 70.55 ** | 3 | −0.008 | −0.007 | 0.005 | 0.008 | |
| M6-M5 | 52.14 ** | 12 | −0.002 | −0.002 | 0.001 | 0.010 | |
| M7-M6 | 23.64 ** | 4 | −0.002 | −0.001 | 0.000 | 0.010 | |
| 95% Confidence Interval | ||||
|---|---|---|---|---|
| Time of Administration | BAT-12 Adjusted Mean | SE | Lower | Upper |
| 1. Pre-COVID-19 | 1.82 | 0.0149 | 1.80 | 1.85 |
| 2. During COVID-19 | 1.98 | 0.0176 | 1.95 | 2.02 |
| F | p | η2 | η2p | |
| Overall model | 38.9 | <0 .001 | ||
| Time of administration (1 = pre-COVID-19; 2 = during COVID-19) | 42.7 | <0 .001 | 0.018 | 0.019 |
| Occupational sector (1 = lower risk sector; 2 = higher risk sector) | 16.1 | < 0.001 | 0.007 | 0.007 |
| Gender (1 = men; 2 = women) | 65.3 | < 0.001 | 0.027 | 0.028 |
| Correlated Dimensions (And Related n of Respondents) | Mean | SD | α | BAT-12 | Exhaustion | Mental Distance | Emotional Impairment | Cognitive Impairment |
|---|---|---|---|---|---|---|---|---|
| Workload (n = 871) | 4.10 | 1.02 | 0.73 | 0.267 ** | 0.413 ** | 0.058 | 0.144 ** | 0.114 ** |
| Time Pressure (n = 500) | 3.82 | 1.20 | 0.78 | 0.188 ** | 0.268 ** | 0.119 ** | 0.099 * | 0.056 |
| Role Conflict (n = 386) | 2.52 | 0.89 | 0.73 | 0.500 ** | 0.430 ** | 0.401 ** | 0.345 ** | 0.362 ** |
| Job Autonomy (n = 871) | 5.11 | 1.13 | 0.86 | −0.284 ** | −0.120 ** | −0.336 ** | −0.170 ** | −0.181 ** |
| Coworkers’ Support (n = 485) | 3.68 | 0.86 | 0.85 | −0.163 ** | −0.115 * | −0.239 ** | −0.108 * | −0.075 |
| Optimism (n = 594) | 3.75 | 0.60 | 0.64 | −0.317 ** | −0.174 ** | −0.344 ** | −0.252 ** | −0.204 ** |
| Social Self-efficacy (n = 862) | 5.34 | 0.98 | 0.86 | −0.317 ** | −0.145 ** | −0.195 ** | −0.300 ** | −0.341 ** |
| Task Self-efficacy (n = 862) | 5.67 | 0.94 | 0.89 | −0.309 ** | −0.156 ** | −0.146 ** | −0.265 ** | −0.406 ** |
| Job Satisfaction (n = 871) | 5.10 | 1.24 | 0.83 | −0.477 ** | −0.199 ** | −0.665 ** | −0.239 ** | −0.200 ** |
| Affective Commitment (n = 871) | 5.51 | 1.10 | 0.78 | −0.346 ** | −0.073 * | −0.468 ** | −0.186 ** | −0.266 ** |
| Vigor a (n = 722) | 3.02 | 0.99 | 0.95 | −0.278 ** | −0.034 | −0.379 ** | −0.126 ** | −0.350 ** |
| Dedication a (n = 486) | 2.82 | 0.97 | 0.93 | −0.587 ** | −0.503 ** | −0.561 ** | −0.404 ** | −0.495 ** |
| Absorption a (n = 1038) | 3.46 | 1.04 | 0.90 | −0.298 ** | −0.097 ** | −0.401 ** | −0.183 ** | −0.327 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzetti, G.; Consiglio, C.; Santarpia, F.P.; Borgogni, L.; Guglielmi, D.; Schaufeli, W.B. Italian Validation of the 12-Item Version of the Burnout Assessment Tool (BAT-12). Int. J. Environ. Res. Public Health 2022, 19, 8562. https://doi.org/10.3390/ijerph19148562
Mazzetti G, Consiglio C, Santarpia FP, Borgogni L, Guglielmi D, Schaufeli WB. Italian Validation of the 12-Item Version of the Burnout Assessment Tool (BAT-12). International Journal of Environmental Research and Public Health. 2022; 19(14):8562. https://doi.org/10.3390/ijerph19148562
Chicago/Turabian StyleMazzetti, Greta, Chiara Consiglio, Ferdinando Paolo Santarpia, Laura Borgogni, Dina Guglielmi, and Wilmar B. Schaufeli. 2022. "Italian Validation of the 12-Item Version of the Burnout Assessment Tool (BAT-12)" International Journal of Environmental Research and Public Health 19, no. 14: 8562. https://doi.org/10.3390/ijerph19148562
APA StyleMazzetti, G., Consiglio, C., Santarpia, F. P., Borgogni, L., Guglielmi, D., & Schaufeli, W. B. (2022). Italian Validation of the 12-Item Version of the Burnout Assessment Tool (BAT-12). International Journal of Environmental Research and Public Health, 19(14), 8562. https://doi.org/10.3390/ijerph19148562