
Relationship between Anemia and Falls among Postmenopausal Women in Korea


Abstract
:1. Introduction
2. Materials and Methods
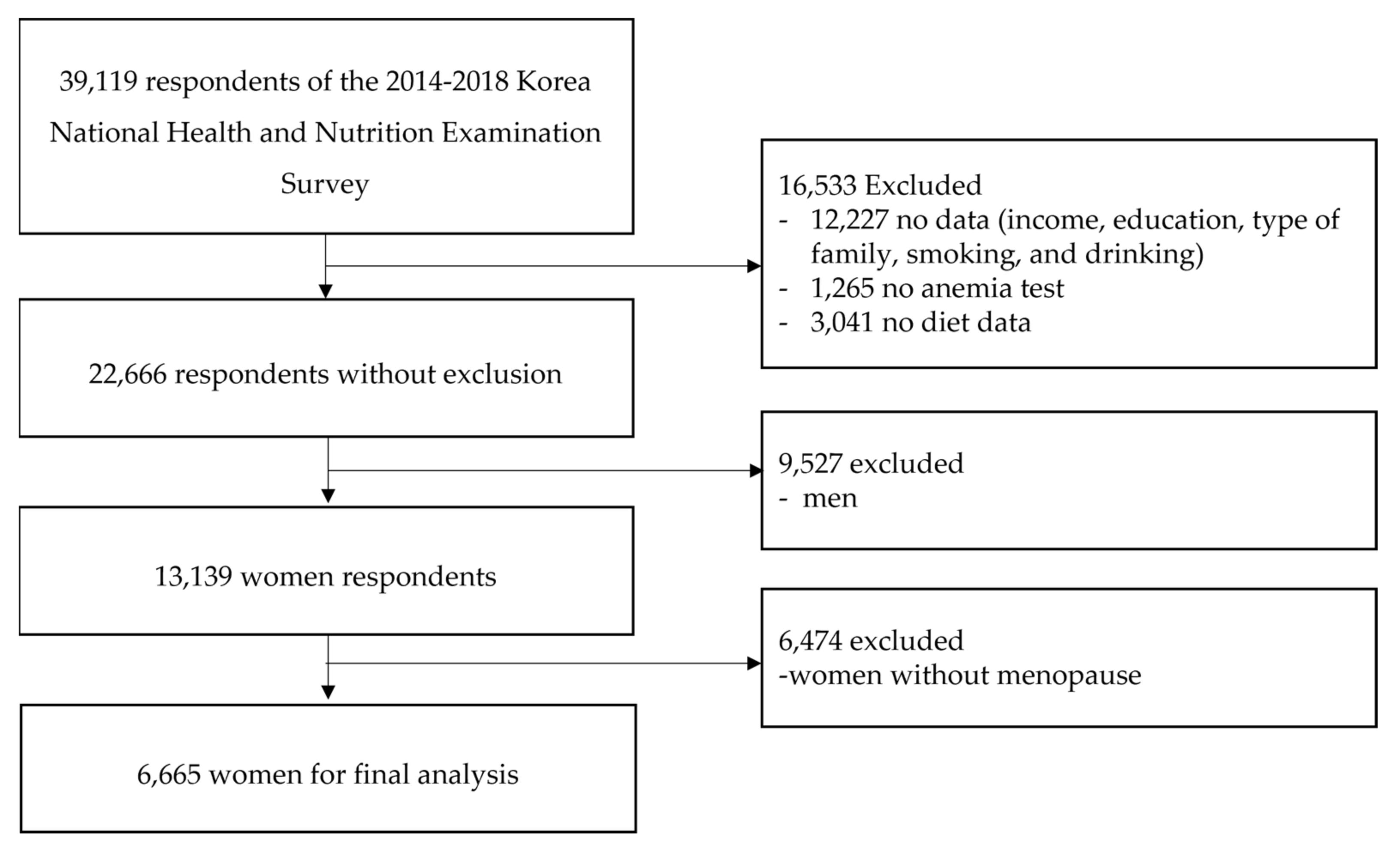
2.1. Data and Study Population
2.2. Measurement
2.2.1. Fall
2.2.2. Anemia
2.2.3. Nutrient Intake
2.2.4. Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Worldwide Prevalence of Anaemia 1993–2005: WHO Global Database on Anaemia; de Benoist, B., McLean, E., Egli, I., Cogswell, M., Eds.; World Health Organization: Geneva, Switzerland, 2008. Available online: https://apps.who.int/iris/handle/10665/43894 (accessed on 4 May 2022).
- Chueh, H.W.; Jung, H.L.; Shim, Y.J.; Choi, H.S.; Han, J.Y. High anemia prevalence in Korean older adults, an advent healthcare problem: 2007–2016 KNHANES. BMC Geriatr. 2020, 20, 509. Available online: https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-020-01918-9 (accessed on 1 June 2022). [CrossRef] [PubMed]
- Guralnik, J.M.; Eisenstaedt, R.S.; Ferrucci, L.; Klein, H.G.; Woodman, R.C. Prevalence of anemia in persons 65 years and older in the United States: Evidence for a high rate of unexplained anemia. Blood 2004, 104, 2263–2268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tettamanti, M.; Lucca, U.; Gandini, F.; Recchia, A.; Mosconi, P.; Apolone, G.; Nobili, A.; Tallone, M.V.; DeToma, P.; Giacomin, A.; et al. Prevalence, incidence and types of mild anemia in the elderly: The “Health and Anemia” population-based study. Haematologica 2010, 95, 1849–1856. Available online: https://haematologica.org/article/view/5780 (accessed on 1 June 2022). [CrossRef] [PubMed] [Green Version]
- Penninx, B.W.J.H.; Pluijm, S.M.F.; Lips, P.; Woodman, R.; Miedema, K.; Guralnik, J.M.; Deeg, D.J.H. Late-Life Anemia Is Associated with Increased Risk of Recurrent Falls. J. Am. Geriatr. Soc. 2005, 53, 2106–2111. [Google Scholar] [CrossRef] [Green Version]
- Elsevier Health Sciences. Inadequate Diet Can Lead to Anemia in Postmenopausal Women—ScienceDaily; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011; Available online: https://www.sciencedaily.com/releases/2011/03/110325024934.htm (accessed on 1 June 2022).
- Duman, T.T.; Aktas, G.; Atak, B.M.; Kocak, M.Z.; Kurtkulagi, O.; Bilgin, S. General characteristics of anemia in postmenopausal women and elderly men. Aging Male 2019, 23, 780–784. Available online: https://www.tandfonline.com/doi/abs/10.1080/13685538.2019.1595571 (accessed on 1 June 2022). [CrossRef]
- Fishman, S.M.; Christian, P.; West, K.P. The role of vitamins in the prevention and control of anaemia. Public Health Nutr. 2000, 3, 125–150. [Google Scholar] [CrossRef] [Green Version]
- Goetz, L.G.; Valeggia, C. The ecology of anemia: Anemia prevalence and correlated factors in adult indigenous women in Argentina. Am. J. Hum. Biol. 2017, 29, e22947. [Google Scholar] [CrossRef]
- Thomson, C.A.; Stanaway, J.D.; Neuhouser, M.L.; Snetselaar, L.G.; Stefanick, M.L.; Arendell, L.; Chen, Z. Nutrient Intake and Anemia Risk in the Women’s Health Initiative Observational Study. J. Am. Diet. Assoc. 2011, 111, 532–541. [Google Scholar] [CrossRef] [Green Version]
- Minkin, M.J. Menopause: Hormones, Lifestyle, and Optimizing Aging. Obstet. Gynecol. Clin. N. Am. 2019, 46, 501–514. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Greendale, G.; Crawford, S.L.; Avis, N.E.; Brooks, M.M.; Thurston, R.C.; Waetjen, L.E.; Matthews, K. The menopause transition and women’s health at midlife: A progress report from the Study of Women’s Health across the Nation (SWAN). Menopause 2019, 26, 1213–1227. [Google Scholar] [CrossRef]
- Tussing-Humphreys, L.; Braunschweig, C. Anemia in postmenopausal women: Dietary inadequacy or nondietary factors? J. Am. Diet Assoc. 2011, 111, 528–531. [Google Scholar] [CrossRef]
- Tsujioka, T.; Tohyama, K. Prevalence of anemia in Japan. Nihon Rinsho 2008, 66, 429–432. [Google Scholar]
- Cooper, J.W.; Burfield, A.H. Medication interventions for fall prevention in the older adult. J. Am. Pharm. Assoc. 2009, 49, e70–e84. [Google Scholar] [CrossRef]
- Sekaran, N.K.; Choi, H.; Hayward, R.A.; Langa, K.M. Fall Associated Difficulty with Activities of Daily Living (ADL) in Functionally Independent Older Adults Aged 65 to 69 in the United States: A Cohort Study. J. Am. Geriatr. Soc. 2013, 61, 96–100. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3807864/ (accessed on 1 June 2022). [CrossRef] [Green Version]
- Pin, S.; Spini, D. Impact of falling on social participation and social support trajectories in a middle-aged and elderly European sample. SSM-Popul. Health 2016, 2, 382–389. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5757958/ (accessed on 1 June 2022). [CrossRef] [Green Version]
- Kim, K.J.; Heo, M. The Relationship between Falling and Quality of Life for The Elderly over 65: Using Korean community health survey. J. Korean Soc. Integr. Med. 2021, 9, 175–183. [Google Scholar] [CrossRef]
- Lee, Y.G.; Kim, S.C.; Chang, M.; Nam, E.; Kim, S.G.; Cho, S.I.; Ryu, D.H.; Kam, S.; Choi, B.Y.; Kim, M.J.; et al. Complications and Socioeconomic Costs Associated With Falls in the Elderly Population. Ann. Rehabil. Med. 2018, 42, 120–129. [Google Scholar] [CrossRef] [Green Version]
- Noh, J.-W.; Kim, K.-B.; Lee, J.H.; Lee, B.-H.; Kwon, Y.D.; Lee, S.H. The elderly and falls: Factors associated with quality of life A cross-sectional study using large-scale national data in Korea. Arch. Gerontol. Geriatr. 2017, 73, 279–283. [Google Scholar] [CrossRef]
- Kim, T.; Choi, S.D.; Xiong, S. Epidemiology of fall and its socioeconomic risk factors in community-dwelling Korean elderly. PLoS ONE 2020, 15, e0234787. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0234787 (accessed on 1 June 2022). [CrossRef]
- Lin, C.-H.; Liao, K.-C.; Pu, S.-J.; Chen, Y.-C.; Liu, M.-S. Associated Factors for Falls among the Community-Dwelling Older People Assessed by Annual Geriatric Health Examinations. PLoS ONE 2011, 6, e18976. [Google Scholar] [CrossRef]
- Lee, Y.-Y.; Chen, C.-L.; Lee, I.-C.; Lee, I.-C.; Chen, N.-C. History of Falls, Dementia, Lower Education Levels, Mobility Limitations, and Aging Are Risk Factors for Falls among the Community-Dwelling Elderly: A Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 9356. [Google Scholar] [CrossRef]
- Kim, M.; Chang, M.; Nam, E.; Kim, S.G.; Cho, S.-I.; Ryu, D.H.; Kam, S.; Choi, B.Y.; Kim, M.J. Fall characteristics among elderly populations in urban and rural areas in Korea. Medicine 2020, 99, e23106. [Google Scholar] [CrossRef]
- Tang, S.; Liu, M.; Yang, T.; Ye, C.; Gong, Y.; Yao, L.; Xu, Y.; Bai, Y. Association between falls in elderly and the number of chronic diseases and health-related behaviors based on CHARLS 2018: Health status as a mediating variable. BMC Geriatr. 2022, 22, 374. [Google Scholar] [CrossRef]
- Ogliari, G.; Ryg, J.; Andersen-Ranberg, K.; Scheel-Hincke, L.L.; Masud, T. Association between body mass index and falls in community-dwelling men and women: A prospective, multinational study in the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. Geriatr. Med. 2021, 12, 837–849. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. National Health and Nutrition Survey Raw Data Usage Guidelines 8th 1st and 2nd Years (2019–2020); Korea Disease Control and Prevention Agency: Osong, Korea, 2022.
- Go, Y.J.; Lee, D.C.; Lee, H.J. Association between handgrip strength asymmetry and falls in elderly Koreans: A nationwide population-based cross-sectional study. Arch. Gerontol. Geriatr. 2021, 96, 104470. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data Resource Profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Oh, K.; Kim, Y.; Kweon, S.; Kim, S.; Yun, S.; Park, S.; Lee, Y.-K.; Kim, Y.-T.; Park, O.; Jeong, E.K. Korea National Health and Nutrition Examination Survey, 20th anniversary: Accomplishments and future directions. Epidemiol. Health 2021, 43, e2021025. [Google Scholar] [CrossRef]
- Yun, S.H.; Shim, J.-S.; Kweon, S.; Oh, K. Development of a Food Frequency Questionnaire for the Korea National Health and Nutrition Examination Survey: Data from the Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Korean J. Nutr. 2013, 46, 186–196. [Google Scholar] [CrossRef] [Green Version]
- The Korean Nutrition Society. 2020 Dietary Reference Intakes for Koreans: Energy and Macronutrients; The Korean Nutrition Society: Sejong, Korea, 2020. Available online: http://www.mohw.go.kr/react/jb/sjb030301vw.jsp?PAR_MENU_ID=03&MENU_ID=032901&CONT_SEQ=362385 (accessed on 6 June 2022).
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Duh, M.S.; Mody, S.H.; Lefebvre, P.; Woodman, R.C.; Buteau, S.; Piech, C.T. Anaemia and the Risk of Injurious Falls in a Community-Dwelling Elderly Population. Drugs Aging 2008, 25, 325–334. [Google Scholar] [CrossRef]
- Dharmarajan, T.; Avula, S.; Norkus, E.P. Anemia Increases Risk for Falls in Hospitalized Older Adults: An Evaluation of Falls in 362 Hospitalized, Ambulatory, Long-Term Care, and Community Patients. J. Am. Med Dir. Assoc. 2007, 8 (Suppl. 2), e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Hopstock, L.A.; Utne, E.B.; Horsch, A.; Skjelbakken, T. The association between anemia and falls in community-living women and men aged 65 years and older from the fifth Tromsø Study 2001–2002: A replication study. BMC Geriatr. 2017, 17, 292. [Google Scholar] [CrossRef] [PubMed]
- Sanford, A.M.; Morley, J.E. Editorial: Anemia of Old Age. J. Nutr. Health Aging 2019, 23, 602–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variables | Category | Total | Fall Experience | Anemia | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Unweighted n (Total) | Unweighted n (Weighted %) | Rao-Scott χ2 (df) | p | Phi (φ)/ Cramer’s V | Unweighted n (Weighted %) | Rao-Scott χ2 (df) | p | Phi (φ)/ Cramer’s V | ||
| Age (year) (64.14 ± 9.07) * | >64 | 3573 | 120 (3.4) | 6.25 | 0.100 | 194 (5.6) | 161.42 | <0.001 | 0.270 | |
| 65–69 | 1066 | 61 (5.2) | (3) | 92 (9.1) | (3) | |||||
| 70–74 | 890 | 42 (4.4) | 111 (12.6) | |||||||
| 75–79 | 1136 | 51 (4.0) | 199 (18.0) | |||||||
| Education | ≥College | 815 | 24 (3.0) | 1.38 | 0.501 | 47 (5.3) | 29.55 | <0.001 | 0.094 | |
| High school | 1591 | 59 (3.8) | 95 (6.5) | (2) | ||||||
| ≤Middle school | 4259 | 191 (4.0) | 454 (10.6) | |||||||
| Type of family | Living alone | 1271 | 75 (5.3) | 7.32 (1) | 0.007 | 0.033 | 151 (11.7) | 10.60 | 0.001 | 0.033 |
| Living with someone | 5394 | 199 (3.6) | 445 (8.2) | |||||||
| Residential area | Urban area | 5173 | 214 (3.8) | 0.02 | 0.900 | 442 (8.3) | 5.06 | 0.025 | 0.002 | |
| Rural area | 1492 | 60 (3.9) | 154 (10.8) | |||||||
| Economic activity | Inactive | 3768 | 178 (4.3) | 3.92 | 0.048 | 0.024 | 398 (10.3) | 17.41 | <0.001 | 0.024 |
| Active | 2897 | 96 (3.2) | (1) | 198 (6.9) | (1) | |||||
| Household income | High | 2862 | 98 (3.5) | 1.68 | 0.194 | 187 (6.5) | 33.65 | <0.001 | 0.016 | |
| Low | 3803 | 176 (4.2) | 409 (10.8) | (1) | ||||||
| High-risk drinking | No | 6510 | 267 (3.8) | 0 | 0.989 | 589 (8.9) | 3.65 | 0.056 | ||
| Yes | 155 | 7 (3.8) | 7 (4.1) | |||||||
| Present smoker | No | 6456 | 265 (3.8) | 0.39 | 0.530 | 581 (9.0) | 1.32 | 0.250 | ||
| Yes | 209 | 9 (4.8) | 15 (7.2) | |||||||
| Aerobic physical activity | No | 4179 | 177 (4.0) | 0.37 | 0.543 | 420 (9.9) | 10.89 | 0.001 | 0.007 | |
| Yes | 2486 | 97 (3.6) | 176 (7.0) | |||||||
| Having chronic disease | No | 1858 | 68 (3.4) | 1.44 | 0.231 | 89 (5.0) | 35.99 | <0.001 | 0.015 | |
| Yes | 4807 | 206 (4.1) | 507 (10.4) | (1) | ||||||
| BMI (kg/m2) (24.24 ± 3.31) * | <18.5 | 136 | 5 (2.6) | 4.43 | 0.109 | 13 (9.9) | 5.59 | 0.061 | ||
| 18.5–24.9 | 4068 | 157 (3.5) | 390 (9.4) | |||||||
| ≥25 | 2461 | 112 (4.5) | 193 (7.5) | |||||||
| Variables | Category | No Anemia | Anemia | Rao–Scott χ2 (df) | p | |
|---|---|---|---|---|---|---|
| Unweighted n (Weighted %) | Unweighted n (Weighted %) | Phi (φ) | ||||
| Energy | Meets EER standards | 2566 (92.5) | 214 (7.5) | 7.13 (1) | 0.008 | 0.033 |
| Below EER | 3503 (90.3) | 382 (9.7) | ||||
| Protein | Meets RNI standards | 2974 (92.8) | 230 (7.2) | 13.93 (1) | <0.001 | 0.046 |
| Below RNI | 3095 (89.7) | 366 (10.3) | ||||
| Iron | Meets RNI standards | 4699 (92.2) | 411 (7.8) | 17.34 (1) | <0.001 | 0.051 |
| Below RNI | 1370 (88.0) | 185 (12.0) | ||||
| Vitamin C | Meets RNI standards | 1940 (93.4) | 133 (6.6) | 12.17 (1) | 0.001 | 0.043 |
| Below RNI | 4129 (90.2) | 463 (9.8) |
| Energy and Nutrient Intake | No Anemia | Anemia | t | p | Cohen’s d |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| Energy (kcal/day) | 1598.16 ± 9.80 | 1518.54 ± 28.21 | 2.63 | 0.009 | 0.064 |
| Protein (g/day) | 53.71 ± 0.42 | 51.12 ± 1.32 | 1.88 | 0.060 | 0.046 |
| Iron (g/day) | 13.54 ± 0.17 | 12.20 ± 0.33 | 3.63 | <0.001 | 0.089 |
| Vitamin C (mg/day) | 98.09 ± 2.38 | 81.42 ± 5.47 | 2.93 | 0.004 | 0.072 |
| Model | Reference Category | Category | OR (95% CI) | p |
|---|---|---|---|---|
| Unadjusted | Anemia (Ref: no) | Yes | 1.89 (1.27~2.81) | 0.002 |
| Age-adjusted | Age (Ref: under 64) | 65–69 | 1.52 (1.06~2.18) | 0.025 |
| 70–74 | 1.23 (0.79~1.90) | 0.356 | ||
| 75–79 | 1.07 (0.72~1.60) | 0.729 | ||
| Anemia (Ref: no anemia) | Anemia | 1.84 (1.23~2.77) | 0.003 | |
| Fully adjusted | Age (Ref: under 64) | 65–69 | 1.36 (0.91~2.02) | 0.131 |
| 70–74 | 1.02 (0.63~1.66) | 0.934 | ||
| 75–79 | 0.84 (0.52~1.37) | 0.494 | ||
| Education (Ref: ≤middle school) | ≥College | 0.90 (0.51~1.58) | 0.716 | |
| High school | 1.11 (0.74~1.67) | 0.614 | ||
| Type of family (Ref: living alone) | Living with someone | 0.69 (0.50~0.94) | 0.020 | |
| Residential area (Ref: urban area) | Rural area | 1.01 (0.71~1.44) | 0.938 | |
| Economic activity (Ref: inactive) | Active | 0.78 (0.56~1.08) | 0.134 | |
| Household income (Ref: high) | Low | 1.01 (0.71~1.44) | 0.954 | |
| High-risk drinking (Ref: no) | Yes | 0.98 (0.40~2.43) | 0.971 | |
| Present smoking (Ref: no) | Yes | 1.24 (0.53~2.92) | 0.615 | |
| Aerobic physical activity (Ref: no) | Yes | 0.96 (0.70~1.32) | 0.815 | |
| Having chronic disease (Ref: no) | Yes | 1.03 (0.70~1.52) | 0.880 | |
| BMI (Ref: 18.5–24.9) | <18.5 | 0.72 (0.28~1.83) | 0.483 | |
| ≥25 | 1.28 (0.95~1.73) | 0.109 | ||
| Anemia (Ref: no anemia) | Anemia | 1.88 (1.24~2.84) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kim, J. Relationship between Anemia and Falls among Postmenopausal Women in Korea. Int. J. Environ. Res. Public Health 2022, 19, 8242. https://doi.org/10.3390/ijerph19148242
Kim Y, Kim J. Relationship between Anemia and Falls among Postmenopausal Women in Korea. International Journal of Environmental Research and Public Health. 2022; 19(14):8242. https://doi.org/10.3390/ijerph19148242
Chicago/Turabian StyleKim, Yunmi, and Jiyun Kim. 2022. "Relationship between Anemia and Falls among Postmenopausal Women in Korea" International Journal of Environmental Research and Public Health 19, no. 14: 8242. https://doi.org/10.3390/ijerph19148242
APA StyleKim, Y., & Kim, J. (2022). Relationship between Anemia and Falls among Postmenopausal Women in Korea. International Journal of Environmental Research and Public Health, 19(14), 8242. https://doi.org/10.3390/ijerph19148242