
Attachment-Based Compassion Therapy for Reducing Anxiety and Depression in Fibromyalgia


Abstract
:
1. Introduction
2. Materials and Methods
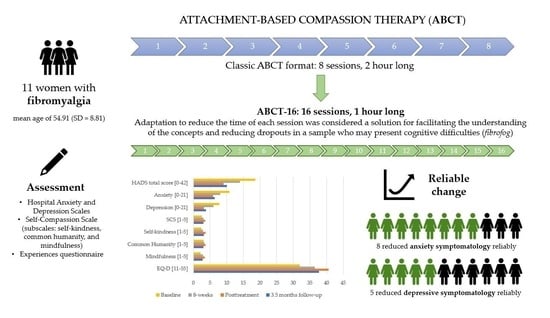
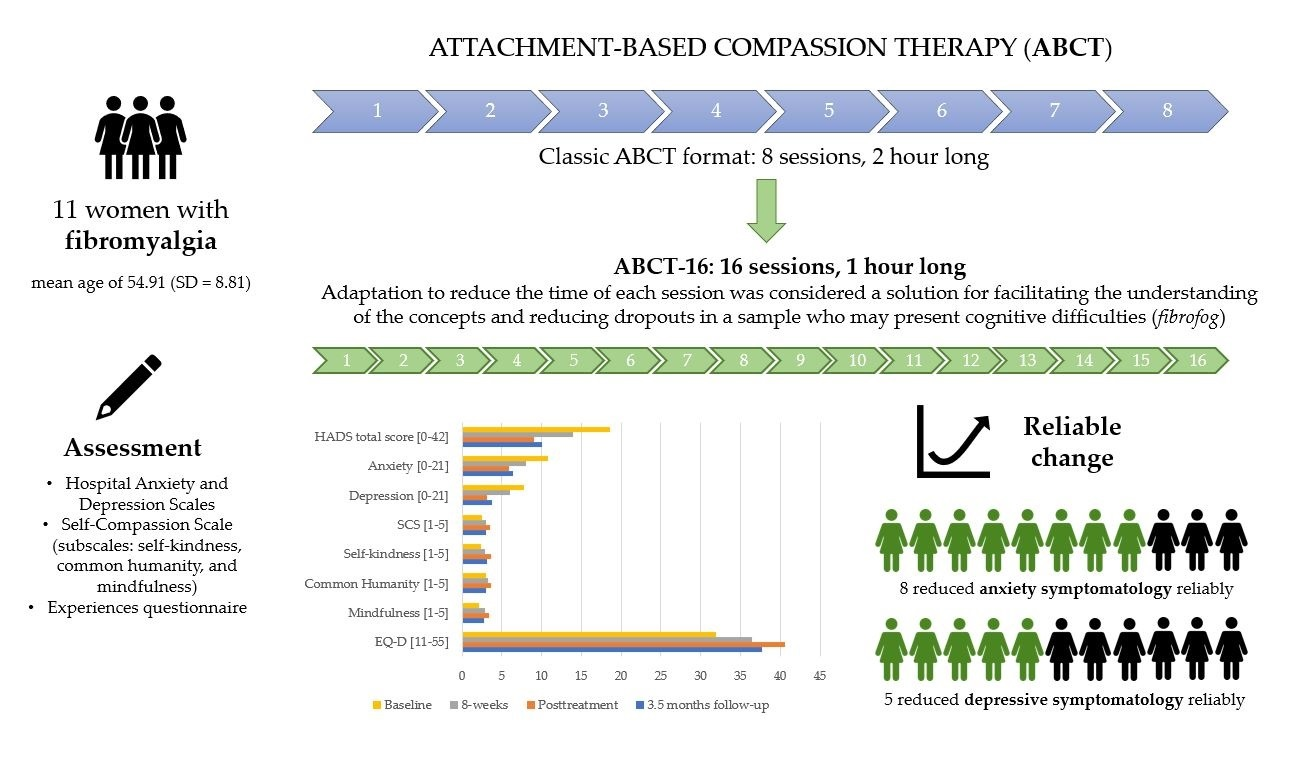
2.1. Participants
2.2. Intervention
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Adherence to the ABCT Program
3.2. Efficacy of ABCT on Anxiety and Depression
3.3. Efficacy of ABCT on Self-Compassion and Decentering
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bertolucci, P.H.F.; Oliveira, F.F. Cognitive Impairment in Fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 344. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef]
- Wolfe, F.; Brähler, E.; Hinz, A.; Häuser, W. Fibromyalgia prevalence, somatic symptom reporting, and the dimensionality of polysymptomatic distress: Results from a survey of the general population. Arthritis Care Res. 2013, 65, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.A.; Perrot, S.; Häuser, W. Comorbid fibromyalgia: A qualitative review of prevalence and importance. Eur. J. Pain 2018, 22, 1565–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glombiewski, J.A.; Sawyer, A.T.; Gutermann, J.; Koenig, K.; Rief, W.; Hofmann, S.G. Psychological treatments for fibromyalgia: A meta-analysis. Pain 2010, 151, 280–295. [Google Scholar] [CrossRef]
- Feldman, C.; Kuyken, W. Compassion in the landscape of suffering. Contemp. Buddhism 2011, 12, 143–155. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Soler, J.; Franquesa, A.; Feliu-Soler, A.; Cebolla, A.; García-Campayo, J.; Tejedor, R.; Demarzo, M.; Baños, R.; Pascual, J.C.; Portella, M.J. Assessing Decentering: Validation, Psychometric Properties, and Clinical Usefulness of the Experiences Questionnaire in a Spanish Sample. Behav. Ther. 2014, 45, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Kirby, J.N.; Tellegen, C.L.; Steindl, S.R. A Meta-Analysis of Compassion-Based Interventions: Current State of Knowledge and Future Directions. Behav. Ther. 2017, 48, 778–792. [Google Scholar] [CrossRef] [Green Version]
- García-Campayo, J.; Demarzo, M. Mindfulness y compasión: Una perspectiva iberoamericana. Mindfulness Compassion 2016, 1, 1. [Google Scholar] [CrossRef]
- Navarro-Gil, M.; Lopez-del-Hoyo, Y.; Modrego-Alarcón, M.; Montero-Marin, J.; Van Gordon, W.; Shonin, E.; Garcia-Campayo, J. Effects of Attachment-Based Compassion Therapy (ABCT) on Self-compassion and Attachment Style in Healthy People. Mindfulness 2020, 11, 51–62. [Google Scholar] [CrossRef]
- Gilbert, P. The Compassionate Mind (Compassion Focused Therapy); Desclée de Brouwer: Bilbao, Spain, 2015. [Google Scholar]
- Amutio, A.; Franco, C.; Pérez-Fuentes, M.d.C.; Gázquez, J.J.; Mercader, I. Mindfulness training for reducing anger, anxiety, and depression in fibromyalgia patients. Front. Psychol. 2015, 5, 1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, S.; Grossman, P.; Schwarzer, B.; Jena, S.; Naumann, J.; Walach, H. Treating fibromyalgia with mindfulness-based stress reduction: Results from a 3-armed randomized controlled trial. Pain 2011, 152, 361–369. [Google Scholar] [CrossRef]
- Sephton, S.E.; Salmon, P.; Weissbecker, I.; Ulmer, C.; Floyd, A.; Hoover, K.; Studts, J.L. Mindfulness meditation alleviates depressive symptoms in women with fibromyalgia: Results of a randomized clinical trial. Arthritis Rheum. 2007, 57, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Montero-Marín, J.; Navarro-Gil, M.; Puebla-Guedea, M.; Luciano, J.V.; Van Gordon, W.; Shonin, E.; García-Campayo, J. Efficacy of “attachment-based compassion therapy” in the treatment of fibromyalgia: A randomized controlled trial. Front. Psychiatry 2018, 8, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feliu-Soler, A.; Pérez-Aranda, A.; Andrés-Rodríguez, L.; Butjosa, A.; Diaz, N.S.; Trujols, J.; Nuñez, C.; Stephan-Otto, C.; Rozadilla-Sacanell, A.; Serrano-Blanco, A.; et al. Digging into the construct of fibrofog: Psychometric properties of the Spanish version of the Multidimensional Inventory of Subjective Cognitive Impairment in patients with fibromyalgia. J. Appl. Biobehav. Res. 2018, 23, 12134. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bjellan, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Terol-Cantero, M.C.; Cabrera-Perona, V.; Martín-Aragón, M. Revisión de estudios de la Escala de Ansiedad y Depresión Hospitalaria (HAD) en muestras españolas. An. De Psicol. Ann. Psychol. 2015, 31, 494–503. [Google Scholar] [CrossRef] [Green Version]
- Luciano, J.V.; Barrada, J.R.; Aguado, J.; Osma, J.; García-Campayo, J. Bifactor analysis and construct validity of the HADS: A cross-sectional and longitudinal study in fibromyalgia patients. Psychol. Assess. 2014, 26, 395–406. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Campayo, J.; Navarro-Gil, M.; Andrés, E.; Montero-Marin, J.; López-Artal, L.; Demarzo, M.M.P. Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the Self-Compassion Scale (SCS). Health. Qual. Life Outcomes 2014, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fresco, D.M.; Moore, M.T.; Van Dulmen, M.H.M.; Segal, Z.V.; Ma, S.H.; Teasdale, J.D.; Mark, J.; Williams, G. Initial Psychometric Properties of the Experiences Questionnaire: Validation of a Self-Report Measure of Decentering. Behav. Ther. 2007, 38, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.S.; Truax, P. Clinical Significance: A Statistical Approach to Defining Meaningful Change in Psychotherapy Research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.R.; Henry, J.D.; Crombie, C.; Taylor, E.P. Normative data for the HADS from a large non-clinical sample. Br. J. Clin. Psychol. 2001, 40, 429–434. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Pérez-Aranda, A.; Feliu-Soler, A.; Montero-Marín, J.; García-Campayo, J.; Andrés-Rodríguez, L.; Borràs, X.; Rozadilla-Sacanell, A.; Peñarrubia-Maria, M.T.; Angarita-Osorio, N.; McCracken, L.M.; et al. A randomized controlled efficacy trial of mindfulness-based stress reduction compared with an active control group and usual care for fibromyalgia: The EUDAIMON study. Pain 2019, 160, 2508–2523. [Google Scholar] [CrossRef]
- Montero-Marin, J.; Van Gordon, W.; Shonin, E.; Navarro-Gil, M.; Gasión, V.; López-del-Hoyo, Y.; Luciano, J.V.; Garcia-Campayo, J. Attachment-Based Compassion Therapy for Ameliorating Fibromyalgia: Mediating Role of Mindfulness and Self-Compassion. Mindfulness 2020, 11, 816–828. [Google Scholar] [CrossRef]
- Elices, M.; Carmona, C.; Pascual, J.C.; Feliu-Soler, A.; Martin-Blanco, A.; Soler, J. Compassion and self-compassion: Construct and measurement. Mindfulness Compassion 2017, 2, 34–40. [Google Scholar] [CrossRef]
- McCracken, L.M.; Gutiérrez-Martínez, O.; Smyth, C. “Decentering” reflects psychological flexibility in people with chronic pain and correlates with their quality of functioning. Health Psychol. 2013, 32, 820–823. [Google Scholar] [CrossRef]

{kind=link}
| Baseline | Session 8 | Posttreatment | Follow-Up | |
|---|---|---|---|---|
| HADS total score HADS Anxiety HADS Depression | 18.55 (5.85) | 14.00 (4.81) | 9.09 (3.24) | 10.09 (3.78) |
| 10.82 (3.92) | 8.00 (2.58) | 5.91 (2.12) | 6.36 (1.69) | |
| 7.73 (2.65) | 6.00 (2.94) | 3.18 (1.78) | 3.73 (2.87) | |
| SCS Self-kindness Common humanity Mindfulness | 2.47 (0.56) 2.34 (0.70) | 2.99 (0.43) 2.93 (0.66) | 3.50 (0.60) 3.57 (0.59) | 2.97 (0.57) 3.09 (0.66) |
| 2.95 (0.67) 2.11 (0.52) | 3.23 (0.49) 2.83 (0.53) | 3.57 (0.74) 3.36 (0.66) | 3.02 (0.85) 2.80 (0.47) | |
| EQ-D | 31.91 (5.54) | 36.50 (5.74) | 40.55 (3.24) | 37.73 (3.82) |
| From Baseline to Session 8 | From Baseline to Posttreatment | From Baseline to Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Z | p | r | Z | p | r | Z | p | r | |
| HADS total score | −2.43 | 0.015 | 0.73 | −2.94 | 0.003 | 0.89 | −2.81 | 0.005 | 0.85 |
| HADS Anxiety | −2.39 | 0.017 | 0.72 | −2.95 | 0.003 | 0.89 | −2.94 | 0.003 | 0.89 |
| HADS Depression | −2.40 | 0.016 | 0.72 | −2.94 | 0.003 | 0.89 | −2.85 | 0.004 | 0.86 |
| SCS total score | −1.84 | 0.066 | 0.55 | −2.50 | 0.012 | 0.75 | −1.78 | 0.075 | 0.54 |
| Self-kindness | −1.83 | 0.068 | 0.55 | −2.59 | 0.010 | 0.78 | −2.41 | 0.016 | 0.73 |
| Common humanity | −1.33 | 0.182 | 0.40 | −1.69 | 0.090 | 0.51 | −0.49 | 0.622 | 0.15 |
| Mindfulness | −2.40 | 0.017 | 0.72 | −2.71 | 0.007 | 0.82 | −2.32 | 0.021 | 0.70 |
| EQ-D | −2.30 | 0.022 | 0.69 | −2.67 | 0.008 | 0.80 | −2.49 | 0.013 | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, A.; Crespo, I.; Pérez-Aranda, A.; Beltrán-Ruiz, M.; Puebla-Guedea, M.; García-Campayo, J. Attachment-Based Compassion Therapy for Reducing Anxiety and Depression in Fibromyalgia. Int. J. Environ. Res. Public Health 2022, 19, 8152. https://doi.org/10.3390/ijerph19138152
Santos A, Crespo I, Pérez-Aranda A, Beltrán-Ruiz M, Puebla-Guedea M, García-Campayo J. Attachment-Based Compassion Therapy for Reducing Anxiety and Depression in Fibromyalgia. International Journal of Environmental Research and Public Health. 2022; 19(13):8152. https://doi.org/10.3390/ijerph19138152
Chicago/Turabian StyleSantos, Alicia, Iris Crespo, Adrián Pérez-Aranda, María Beltrán-Ruiz, Marta Puebla-Guedea, and Javier García-Campayo. 2022. "Attachment-Based Compassion Therapy for Reducing Anxiety and Depression in Fibromyalgia" International Journal of Environmental Research and Public Health 19, no. 13: 8152. https://doi.org/10.3390/ijerph19138152
APA StyleSantos, A., Crespo, I., Pérez-Aranda, A., Beltrán-Ruiz, M., Puebla-Guedea, M., & García-Campayo, J. (2022). Attachment-Based Compassion Therapy for Reducing Anxiety and Depression in Fibromyalgia. International Journal of Environmental Research and Public Health, 19(13), 8152. https://doi.org/10.3390/ijerph19138152