
Association of Serum Levels of Plasticizers Compounds, Phthalates and Bisphenols, in Patients and Survivors of Breast Cancer: A Real Connection?

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients/Study Population
2.2. Collection of Breast Cancer Samples
Sample Treatment
2.3. Data Analysis
2.3.1. Reagents and Chemicals
2.3.2. GC-MS Conditions
2.3.3. Statistical Analysis
3. Results
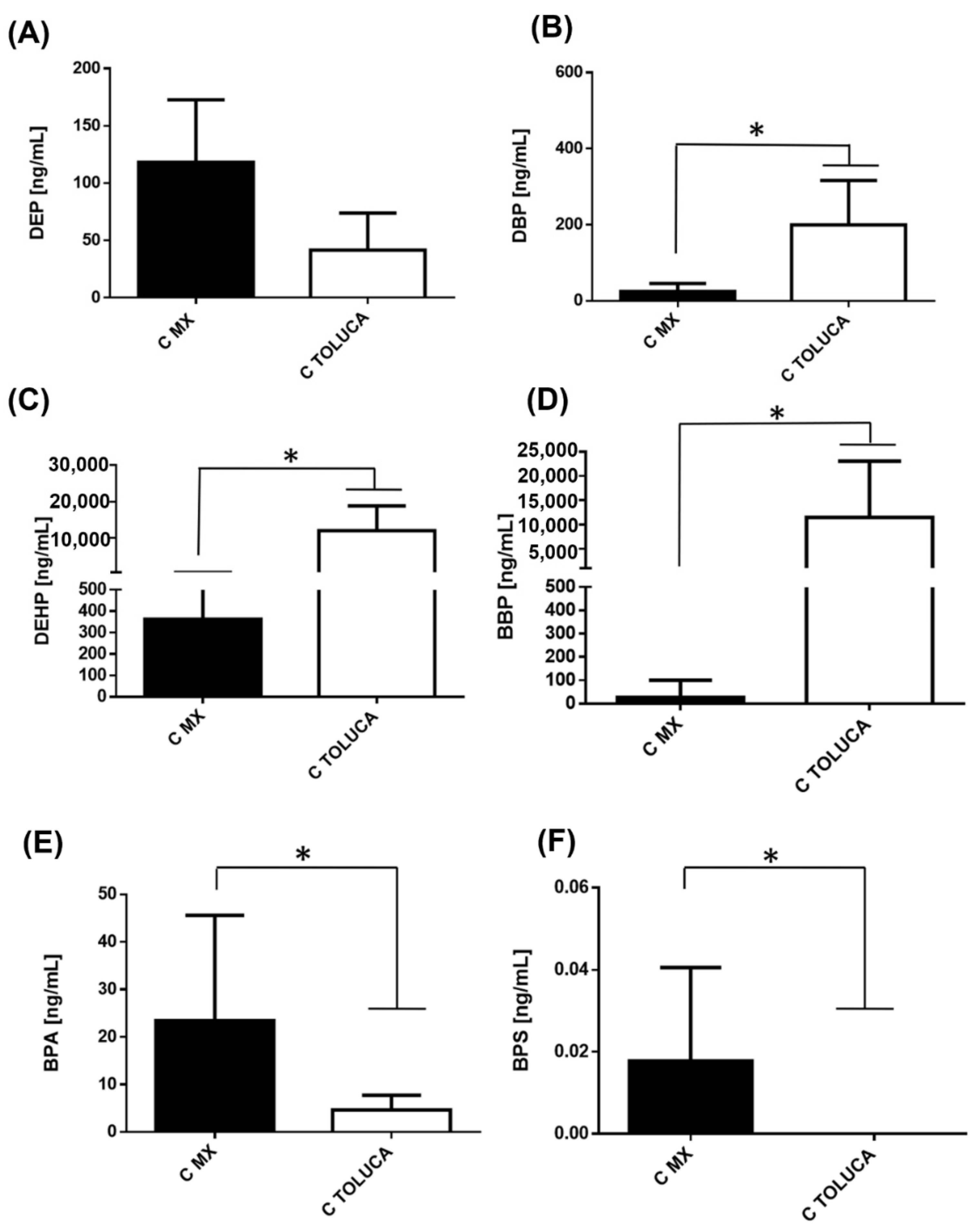
3.1. Comparison of Serum Levels of Phthalates and Bisphenols in Healthy Women between Mexico and Toluca City
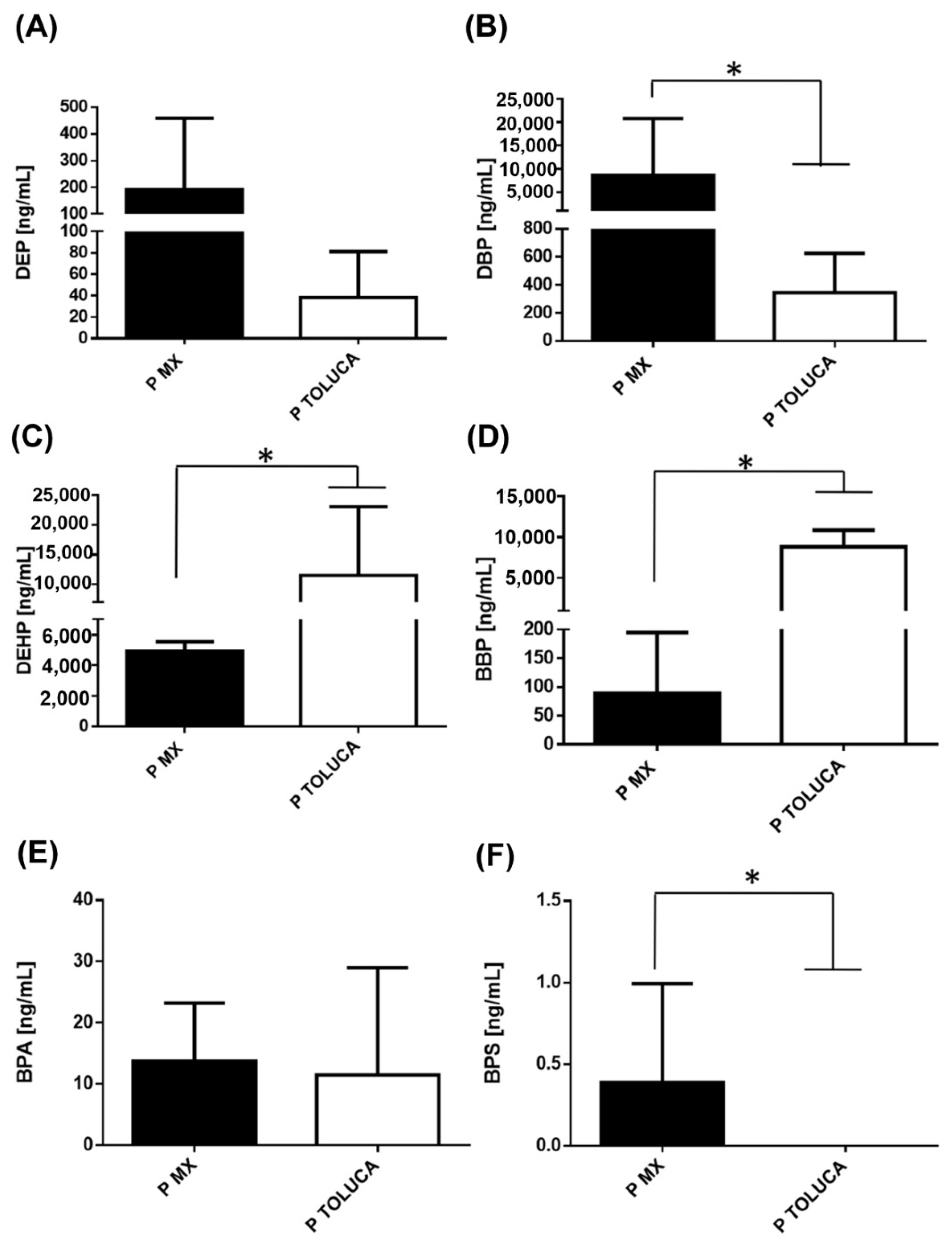
3.2. Comparison of Serum Levels of Phthalates and Bisphenols in Patients with BC between Mexico and Toluca City
3.3. Comparison of Serum Levels of Phthalates and Bisphenols in Patients with BC Classified by Clinical Stage between Mexico and Toluca City
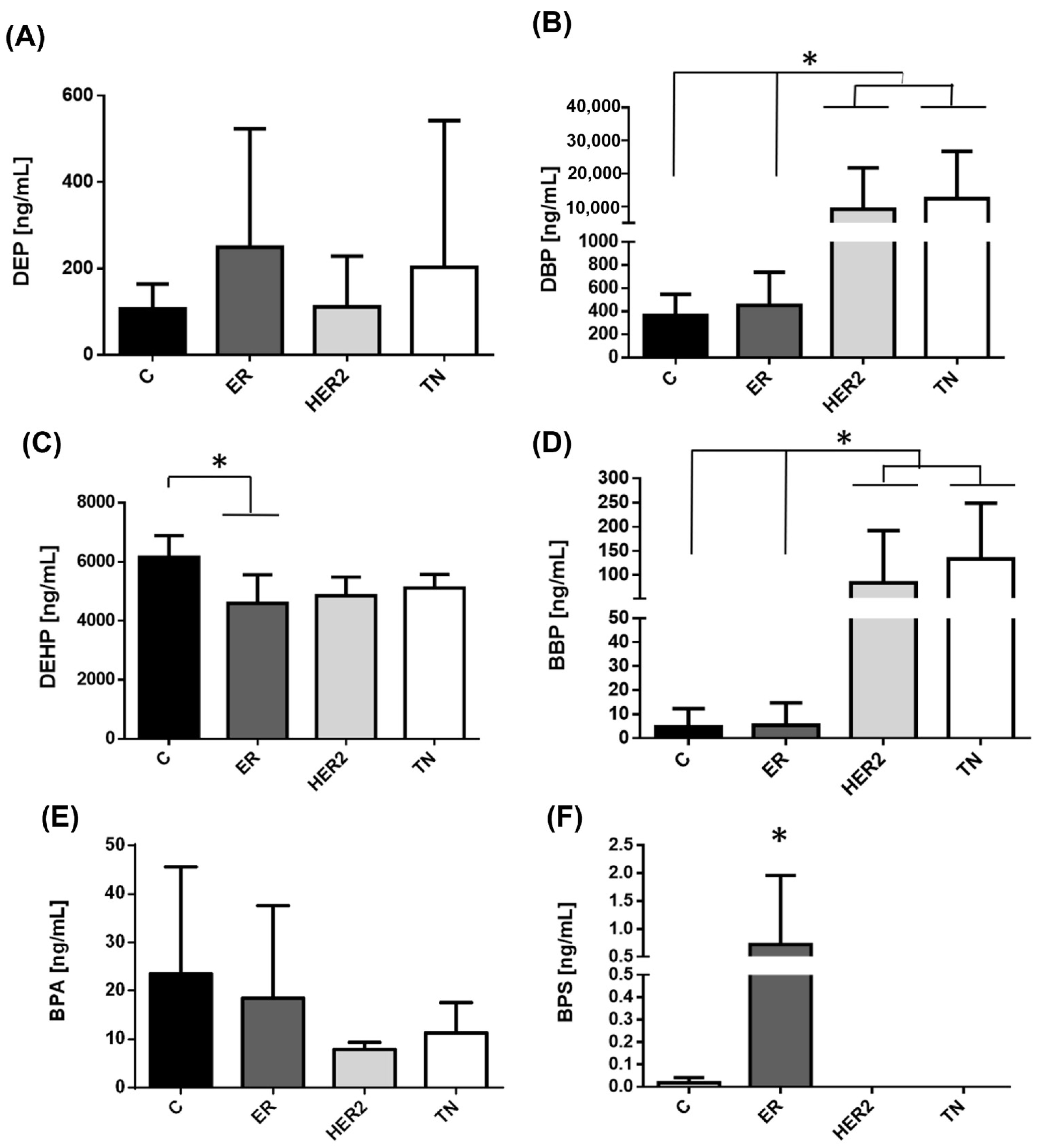
3.4. Comparison of Serum Levels of Phthalates and Bisphenols in Patients with BC by Molecular Type
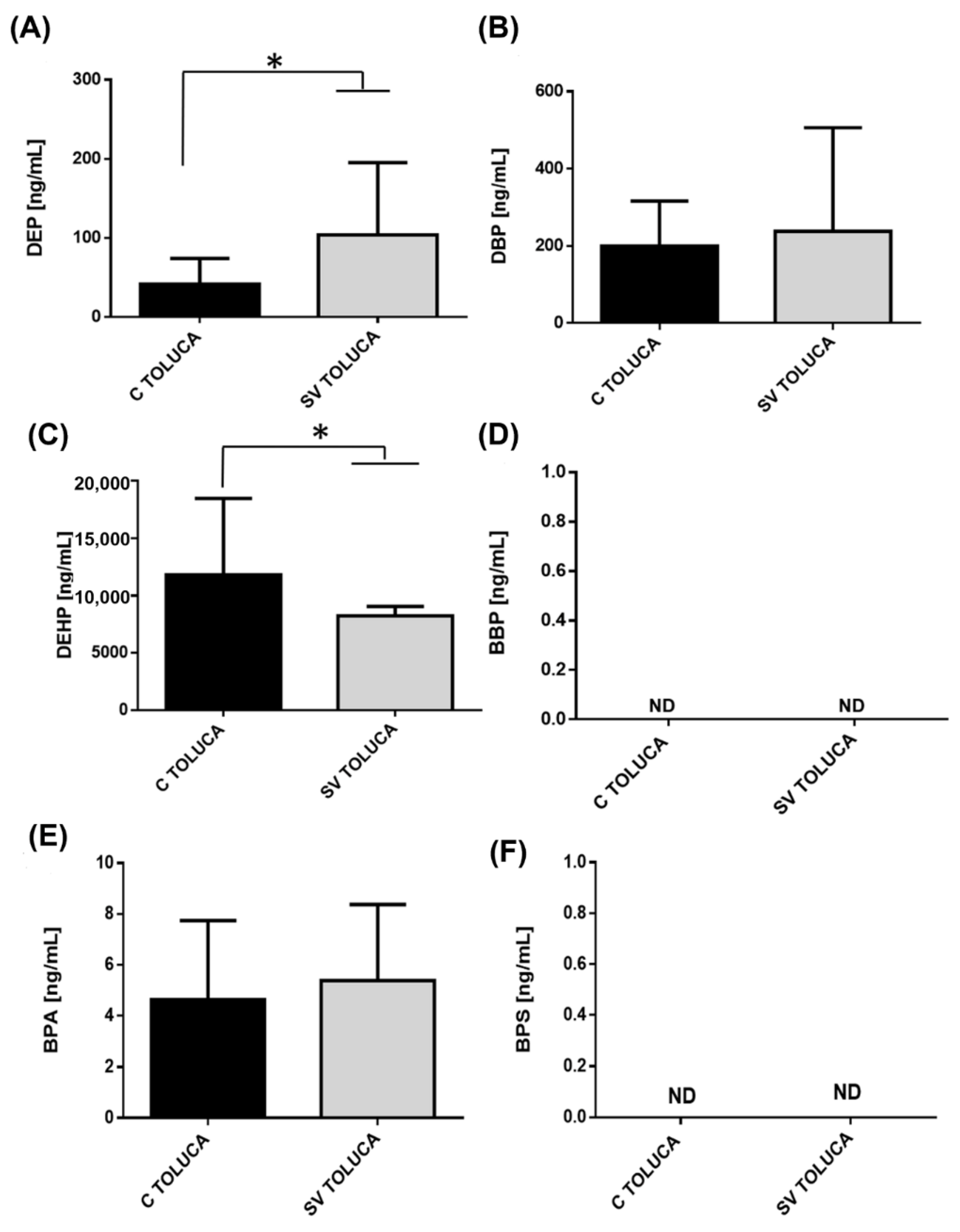
3.5. Comparison of Serum Levels of Phthalates and Bisphenols in BC Survivors, Women after 5 Years Free of Recurrence, in Toluca City
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Perou, C.M.; Sorlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Ding, N.-H.; Liu, C.-F.; Hu, C.; Yuan, J.-Q.; Liao, W.-H.; Xiao, Z. Prognostic Factors for Luminal B-like Breast Cancer. Curr. Med. Sci. 2019, 39, 396–402. [Google Scholar] [CrossRef]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer 2019, 11, 151–164. [Google Scholar] [CrossRef] [Green Version]
- Segovia-Mendoza, M.; Nava-Castro, K.E.; Palacios-Arreola, M.I.; Garay-Canales, C.; Morales-Montor, J. How microplastic components influence the immune system and impact on children health: Focus on cancer. Birth Defects Res. 2020, 112, 1341–1361. [Google Scholar] [CrossRef]
- Geens, T.; Goeyens, L.; Covaci, A. Are potential sources for human exposure to bisphenol-A overlooked? Int. J. Hyg. Environ. Health 2011, 214, 339–347. [Google Scholar] [CrossRef]
- Koniecki, D.; Wang, R.; Moody, R.P.; Zhu, J. Phthalates in cosmetic and personal care products: Concentrations and possible dermal exposure. Environ. Res. 2011, 111, 329–336. [Google Scholar] [CrossRef]
- Kumar, N.; Sharan, S.; Srivastava, S.; Roy, P. Assessment of estrogenic potential of diethyl phthalate in female reproductive system involving both genomic and non-genomic actions. Reprod. Toxicol. 2014, 49, 12–26. [Google Scholar] [CrossRef]
- Moral, R.; Santucci-Pereira, J.; Wang, R.; Russo, I.H.; Lamartiniere, C.A.; Russo, J. In utero exposure to butyl benzyl phthalate induces modifications in the morphology and the gene expression profile of the mammary gland: An experimental study in rats. Environ. Health A Glob. Access Sci. Source 2011, 10, 5. [Google Scholar] [CrossRef] [Green Version]
- Moral, R.; Wang, R.; Russo, I.H.; Lamartiniere, C.A.; Pereira, J.; Russo, J. Effect of prenatal exposure to the endocrine disruptor bisphenol A on mammary gland morphology and gene expression signature. J. Endocrinol. 2008, 196, 101–112. [Google Scholar] [CrossRef]
- Hsieh, T.H.; Tsai, C.F.; Hsu, C.Y.; Kuo, P.L.; Lee, J.N.; Chai, C.Y.; Wang, S.C.; Tsai, E.M. Phthalates induce proliferation and invasiveness of estrogen receptor-negative breast cancer through the AhR/HDAC6/c-Myc signaling pathway. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2012, 26, 778–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crobeddu, B.; Ferraris, E.; Kolasa, E.; Plante, I. Di(2-ethylhexyl) phthalate (DEHP) increases proliferation of epithelial breast cancer cells through progesterone receptor dysregulation. Environ. Res. 2019, 173, 165–173. [Google Scholar] [CrossRef]
- Chen, F.P.; Chien, M.H. Lower concentrations of phthalates induce proliferation in human breast cancer cells. Climacteric J. Int. Menopause Soc. 2014, 17, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Segovia-Mendoza, M.; Gómez de León, C.T.; Garcia-Becerra, R.; Ambrosio, J.; Nava-Castro, K.E.; Morales-Montor, J. The chemical environmental pollutants BPA and BPS induce alterations of the proteomic profile of different phenotypes of human breast cancer cells: A proposed interactome. Environ. Res. 2020, 191, 109960. [Google Scholar] [CrossRef]
- Fiocchetti, M.; Bastari, G.; Cipolletti, M.; Leone, S.; Acconcia, F.; Marino, M. The Peculiar Estrogenicity of Diethyl Phthalate: Modulation of Estrogen Receptor α Activities in the Proliferation of Breast Cancer Cells. Toxics 2021, 9, 237. [Google Scholar] [CrossRef]
- Acconcia, F.; Pallottini, V.; Marino, M. Molecular Mechanisms of Action of BPA. Dose-Response A Publ. Int. Hormesis Soc. 2015, 13, 1559325815610582. [Google Scholar] [CrossRef] [Green Version]
- Sangeetha, S.; Vimalkumar, K.; Loganathan, B. Environmental Contamination and Human Exposure to Select Endocrine-Disrupting Chemicals: A Review. Sustain. Chem. 2021, 2, 20. [Google Scholar] [CrossRef]
- Makarova, K.; Siudem, P.; Zawada, K.; Kurkowiak, J. Screening of Toxic Effects of Bisphenol A and Products of Its Degradation: Zebrafish (Danio rerio) Embryo Test and Molecular Docking. Zebrafish 2016, 13, 466–474. [Google Scholar] [CrossRef]
- Poerschmann, J.; Trommler, U.; Górecki, T. Aromatic intermediate formation during oxidative degradation of Bisphenol A by homogeneous sub-stoichiometric Fenton reaction. Chemosphere 2010, 79, 975–986. [Google Scholar] [CrossRef]
- Lopez-Carrillo, L.; Hernandez-Ramirez, R.U.; Calafat, A.M.; Torres-Sanchez, L.; Galvan-Portillo, M.; Needham, L.L.; Ruiz-Ramos, R.; Cebrian, M.E. Exposure to phthalates and breast cancer risk in northern Mexico. Environ. Health Perspect. 2010, 118, 539–544. [Google Scholar] [CrossRef]
- Ahern, T.P.; Broe, A.; Lash, T.L.; Cronin-Fenton, D.P.; Ulrichsen, S.P.; Christiansen, P.M.; Cole, B.F.; Tamimi, R.M.; Sorensen, H.T.; Damkier, P. Phthalate Exposure and Breast Cancer Incidence: A Danish Nationwide Cohort Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 1800–1809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeves, K.W.; Diaz Santana, M.; Manson, J.E.; Hankinson, S.E.; Zoeller, R.T.; Bigelow, C.; Sturgeon, S.R.; Spiegelman, D.; Tinker, L.; Luo, J.; et al. Urinary Phthalate Biomarker Concentrations and Postmenopausal Breast Cancer Risk. J. Natl. Cancer Inst. 2019, 111, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.K.; Koller, K.R.; Kieszak, S.M.; Sjodin, A.; Calafat, A.M.; Sacco, F.D.; Varner, D.W.; Lanier, A.P.; Rubin, C.H. Case-control study of breast cancer and exposure to synthetic environmental chemicals among Alaska Native women. Int. J. Circumpolar Health 2014, 73, 25760. [Google Scholar] [CrossRef] [Green Version]
- Merida-Ortega, A.; Hernandez-Alcaraz, C.; Hernandez-Ramirez, R.U.; Garcia-Martinez, A.; Trejo-Valdivia, B.; Salinas-Rodriguez, A.; Svensson, K.; Cebrian, M.E.; Franco-Marina, F.; Lopez-Carrillo, L. Phthalate exposure, flavonoid consumption and breast cancer risk among Mexican women. Environ. Int. 2016, 96, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.; Deoraj, A.; Felty, Q.; Roy, D. Environmental estrogen-like endocrine disrupting chemicals and breast cancer. Mol. Cell Endocrinol. 2017, 457, 89–102. [Google Scholar] [CrossRef]
- Fu, Z.; Zhao, F.; Chen, K.; Xu, J.; Li, P.; Xia, D.; Wu, Y. Association between urinary phthalate metabolites and risk of breast cancer and uterine leiomyoma. Reprod. Toxicol. 2017, 74, 134–142. [Google Scholar] [CrossRef]
- Trabert, B.; Falk, R.T.; Figueroa, J.D.; Graubard, B.I.; Garcia-Closas, M.; Lissowska, J.; Peplonska, B.; Fox, S.D.; Brinton, L.A. Urinary bisphenol A-glucuronide and postmenopausal breast cancer in Poland. Cancer Causes Control. 2014, 25, 1587–1593. [Google Scholar] [CrossRef] [Green Version]
- Parada, H., Jr.; Gammon, M.D.; Ettore, H.L.; Chen, J.; Calafat, A.M.; Neugut, A.I.; Santella, R.M.; Wolff, M.S.; Teitelbaum, S.L. Urinary concentrations of environmental phenols and their associations with breast cancer incidence and mortality following breast cancer. Environ. Int. 2019, 130, 104890. [Google Scholar] [CrossRef]
- Yang, M.; Kim, S.Y.; Chang, S.S.; Lee, I.S.; Kawamoto, T. Urinary concentrations of bisphenol A in relation to biomarkers of sensitivity and effect and endocrine-related health effects. Environ. Mol. Mutagenesis 2006, 47, 571–578. [Google Scholar] [CrossRef]
- Volkel, W.; Colnot, T.; Csanady, G.A.; Filser, J.G.; Dekant, W. Metabolism and kinetics of bisphenol a in humans at low doses following oral administration. Chem. Res. Toxicol. 2002, 15, 1281–1287. [Google Scholar] [CrossRef]
- Yokota, H.; Iwano, H.; Endo, M.; Kobayashi, T.; Inoue, H.; Ikushiro, S.; Yuasa, A. Glucuronidation of the environmental oestrogen bisphenol A by an isoform of UDP-glucuronosyltransferase, UGT2B1, in the rat liver. Biochem. J. 1999, 340 Pt 2, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.J.; Reidy, J.A.; Herbert, A.R.; Preau, J.L., Jr.; Needham, L.L.; Calafat, A.M. Detection of phthalate metabolites in human amniotic fluid. Bull. Environ. Contam. Toxicol. 2004, 72, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Haggerty, D.K.; Rappolee, D.A.; Ruden, D.M. Phthalate Exposure and Long-Term Epigenomic Consequences: A Review. Front. Genet. 2020, 11, 405. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, H.; Kannan, K. A Review of Biomonitoring of Phthalate Exposures. Toxics 2019, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, A.; Roy, D. In vitro conversion of environmental estrogenic chemical bisphenol A to DNA binding metabolite(s). Biochem. Biophys. Res. Commun. 1995, 210, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Street, C.M.; Zhu, Z.; Finel, M.; Court, M.H. Bisphenol-A glucuronidation in human liver and breast: Identification of UDP-glucuronosyltransferases (UGTs) and influence of genetic polymorphisms. Xenobiotica Fate Foreign Compd. Biol. Syst. 2017, 47, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Corrales, J.; Kristofco, L.A.; Steele, W.B.; Yates, B.S.; Breed, C.S.; Williams, E.S.; Brooks, B.W. Global Assessment of Bisphenol A in the Environment: Review and Analysis of Its Occurrence and Bioaccumulation. Dose-Response A Publ. Int. Hormesis Soc. 2015, 13, 1559325815598308. [Google Scholar] [CrossRef] [Green Version]
- Genuis, S.J.; Beesoon, S.; Birkholz, D.; Lobo, R.A. Human Excretion of Bisphenol A: Blood, Urine, and Sweat (BUS) Study. J. Environ. Public Health 2012, 2012, 185731. [Google Scholar] [CrossRef] [Green Version]
- Main, K.M.; Mortensen, G.K.; Kaleva, M.M.; Boisen, K.A.; Damgaard, I.N.; Chellakooty, M.; Schmidt, I.M.; Suomi, A.M.; Virtanen, H.E.; Petersen, D.V.; et al. Human breast milk contamination with phthalates and alterations of endogenous reproductive hormones in infants three months of age. Environ. Health Perspect. 2006, 114, 270–276. [Google Scholar] [CrossRef]
- Yang, M.; Ryu, J.H.; Jeon, R.; Kang, D.; Yoo, K.Y. Effects of bisphenol A on breast cancer and its risk factors. Arch. Toxicol. 2009, 83, 281–285. [Google Scholar] [CrossRef]
- Stillwater, B.J.; Bull, A.C.; Romagnolo, D.F.; Neumayer, L.A.; Donovan, M.G.; Selmin, O.I. Bisphenols and Risk of Breast Cancer: A Narrative Review of the Impact of Diet and Bioactive Food Components. Front. Nutr. 2020, 7, 581388. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.; Rudnitskaya, A.; Blackburn, G.J.; Mohd Fauzi, N.; Pitt, A.R.; Spickett, C.M. A comparison of five lipid extraction solvent systems for lipidomic studies of human LDL. J. Lipid Res. 2013, 54, 1812–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisler, J.; Chaput, G.; Sussman, J.; Ozokwelu, E. Follow-up after treatment for breast cancer: Practical guide to survivorship care for family physicians. Can. Fam. Physician Med. De Fam. Can. 2016, 62, 805–811. [Google Scholar]
- Sun, Y.S.; Zhao, Z.; Yang, Z.N.; Xu, F.; Lu, H.J.; Zhu, Z.Y.; Shi, W.; Jiang, J.; Yao, P.P.; Zhu, H.P. Risk Factors and Preventions of Breast Cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giulivo, M.; Lopez de Alda, M.; Capri, E.; Barcelo, D. Human exposure to endocrine disrupting compounds: Their role in reproductive systems, metabolic syndrome and breast cancer. Rev. Environ. Res. 2016, 151, 251–264. [Google Scholar] [CrossRef]
- Chen, F.P.; Chien, M.H.; Chern, I.Y. Impact of low concentrations of phthalates on the effects of 17beta-estradiol in MCF-7 breast cancer cells. Taiwan J. Obstet. Gynecol. 2016, 55, 826–834. [Google Scholar] [CrossRef]
- Hsieh, T.H.; Tsai, C.F.; Hsu, C.Y.; Kuo, P.L.; Hsi, E.; Suen, J.L.; Hung, C.H.; Lee, J.N.; Chai, C.Y.; Wang, S.C.; et al. n-Butyl benzyl phthalate promotes breast cancer progression by inducing expression of lymphoid enhancer factor 1. PLoS ONE 2012, 7, e42750. [Google Scholar] [CrossRef]
- Wang, Y.C.; Tsai, C.F.; Chuang, H.L.; Chang, Y.C.; Chen, H.S.; Lee, J.N.; Tsai, E.M. Benzyl butyl phthalate promotes breast cancer stem cell expansion via SPHK1/S1P/S1PR3 signaling. Oncotarget 2016, 7, 29563–29576. [Google Scholar] [CrossRef]
- Caldwell, J.C. DEHP: Genotoxicity and potential carcinogenic mechanisms—A review. Mutat. Res. 2012, 751, 82–157. [Google Scholar] [CrossRef]
- Buteau-Lozano, H.; Velasco, G.; Cristofari, M.; Balaguer, P.; Perrot-Applanat, M. Xenoestrogens modulate vascular endothelial growth factor secretion in breast cancer cells through an estrogen receptor-dependent mechanism. J. Endocrinol. 2008, 196, 399–412. [Google Scholar] [CrossRef] [Green Version]
- Al-Badry, M.S.; Knowles, C.O. Phthalate-organophosphate interactions: Toxicity, penetration, and metabolism studies with house flies. Arch. Environ. Contam. Toxicol. 1980, 9, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Baralić, K.; Buha Djordjevic, A.; Živančević, K.; Antonijević, E.; Anđelković, M.; Javorac, D.; Ćurčić, M.; Bulat, Z.; Antonijević, B.; Đukić-Ćosić, D. Toxic Effects of the Mixture of Phthalates and Bisphenol A—Subacute Oral Toxicity Study in Wistar Rats. Int. J. Environ. Res. Public Health 2020, 17, 746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, D.K.; Agarwal, S.; Seth, P.K. Interaction of di-(2-ethylhexyl) phthalate with the pharmacological response and metabolic aspects of ethanol in mice. Biochem. Pharmacol. 1982, 31, 3419–3423. [Google Scholar] [CrossRef]
- Kim, J.Y.; Choi, H.G.; Lee, H.M.; Lee, G.A.; Hwang, K.A.; Choi, K.C. Effects of bisphenol compounds on the growth and epithelial mesenchymal transition of MCF-7 CV human breast cancer cells. J. Biomed. Res. 2017, 31, 358–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, E.; Shoemaker, R.; Larian, N.; Cassis, L. Adipose Tissue as a Site of Toxin Accumulation. Compr. Physiol. 2017, 7, 1085–1135. [Google Scholar] [CrossRef] [Green Version]
- Charisiadis, P.; Andrianou, X.D.; van der Meer, T.P.; den Dunnen, W.F.A.; Swaab, D.F.; Wolffenbuttel, B.H.R.; Makris, K.C.; van Vliet-Ostaptchouk, J.V. Possible Obesogenic Effects of Bisphenols Accumulation in the Human Brain. Sci. Rep. 2018, 8, 8186. [Google Scholar] [CrossRef] [Green Version]
- Wolinsky, J.B.; Colson, Y.L.; Grinstaff, M.W. Local drug delivery strategies for cancer treatment: Gels, nanoparticles, polymeric films, rods, and wafers. J. Control. Release Off. J. Control. Release Soc. 2012, 159, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Day, C.M.; Hickey, S.M.; Song, Y.; Plush, S.E.; Garg, S. Novel Tamoxifen Nanoformulations for Improving Breast Cancer Treatment: Old Wine in New Bottles. Molecules 2020, 25, 1182. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.P.; Lee, Y.K.; Huang, S.Y.; Shi, P.C.; Hsu, P.C.; Chang, C.F. Phthalate exposure promotes chemotherapeutic drug resistance in colon cancer cells. Oncotarget 2018, 9, 13167–13180. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.L.; Hung, J.Y.; Tsai, E.M.; Wu, C.Y.; Ho, Y.W.; Jian, S.F.; Yen, M.C.; Chang, W.A.; Hou, M.F.; Kuo, P.L. Benzyl butyl phthalate increases the chemoresistance to doxorubicin/cyclophosphamide by increasing breast cancer-associated dendritic cell-derived CXCL1/GROalpha and S100A8/A9. Oncol. Rep. 2015, 34, 2889–2900. [Google Scholar] [CrossRef] [Green Version]
- Hafezi, S.A.; Abdel-Rahman, W.M. The Endocrine Disruptor Bisphenol A (BPA) Exerts a Wide Range of Effects in Carcinogenesis and Response to Therapy. Curr. Mol. Pharmacol. 2019, 12, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Luo, N.; Wu, X.; Xu, Z.; Wang, X.; Pan, X. The modulatory role of low concentrations of bisphenol A on tamoxifen-induced proliferation and apoptosis in breast cancer cells. Environ. Sci. Pollut. Res. Int. 2019, 26, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Margarita, I.P.-A.; Palacios-Arreola, M.I.; Morales-Montor, J.; Cazares-Martinez, C.J.; Gomez-Arroyo, S.; Nava-Castro, K.E. Environmental pollutants: An immunoendocrine perspective on phthalates. Front. Biosci. 2021, 26, 401–430. [Google Scholar] [CrossRef]
- Walker, C.L. Minireview: Epigenomic Plasticity and Vulnerability to EDC Exposures. Mol. Endocrinol. 2016, 30, 848–855. [Google Scholar] [CrossRef] [Green Version]
- Shirakawa, H.; Rochman, M.; Furusawa, T.; Kuehn, M.R.; Horigome, S.; Haketa, K.; Sugita, Y.; Inada, T.; Komai, M.; Bustin, M. The nucleosomal binding protein NSBP1 is highly expressed in the placenta and modulates the expression of differentiation markers in placental Rcho-1 cells. J. Cell Biochem. 2009, 106, 651–658. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, L. and W. McCully, Review: UK medicines likely to be affected by the proposed European Medicines Agency’s guidelines on phthalates. BMC Pharm. Toxicol. 2015, 16, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA CEF Panel (EFSA Panel on Food Contact Materials, Enzymes, Flavourings and Processing Aids). Scientific Opinion on the risks to public health related to the presence of bisphenol A (BPA) in foodstuffs: Executive summary. EFSA J. 2015, 13, 3978. [Google Scholar] [CrossRef]
- Calafat, A.M.; Ye, X.; Wong, L.-Y.; Reidy, J.A.; Needham, L.L. Exposure of the U.S. population to bisphenol A and 4-tertiary-octylphenol: 2003–2004. Environ. Health Perspect. 2008, 116, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Vandenberg, L.N.; Hauser, R.; Marcus, M.; Olea, N.; Welshons, W.V. Human exposure to bisphenol A (BPA). Reprod. Toxicol. 2007, 24, 139–177. [Google Scholar] [CrossRef]
- Vandenberg, L.N.; Chahoud, I.; Heindel, J.J.; Padmanabhan, V.; Paumgartten, F.J.R.; Schönfelder, G. Urinary, circulating, and tissue biomonitoring studies indicate widespread exposure to bisphenol A. Environ. Health Perspect. 2010, 118, 1055–1070. [Google Scholar] [CrossRef] [Green Version]
- Harthe, C.; Rinaldi, S.; Achaintre, D.; de Ravel, M.R.; Mappus, E.; Pugeat, M.; Dechaud, H. Bisphenol A-glucuronide measurement in urine samples. Talanta 2012, 100, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Bushnik, T.; Haines, D.; Levallois, P.; Levesque, J.; Van Oostdam, J.; Viau, C. Lead and bisphenol A concentrations in the Canadian population. Health Rep. 2010, 21, 7–18. [Google Scholar] [PubMed]
- Moors, S.; Blaszkewicz, M.; Bolt, H.M.; Degen, G.H. Simultaneous determination of daidzein, equol, genistein and bisphenol A in human urine by a fast and simple method using SPE and GC-MS. Mol. Nutr. Food Res. 2007, 51, 787–798. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Histological Classification | Molecular Classification | Stage |
|---|---|---|---|---|
| Patients with BC from Mexico City | ||||
| 1 | 60 | Ductal | Luminal | IV |
| 2 | 49 | Ductal | TN | IV |
| 3 | 42 | Canicular | HER2 | II |
| 4 | 40 | Ductal | TN | IV |
| 5 | 46 | Ductal | HER2 | III |
| 6 | 71 | Canicular | Luminal | II |
| 7 | 60 | Lobulillar | TN | II |
| 8 | 47 | Canicular | TN | II |
| 9 | 46 | Ductal | Luminal | III |
| 10 | 84 | Ductal | TN | IV |
| 11 | 37 | Ductal | HER2 | III |
| 12 | 49 | Ductal | Luminal | I |
| 13 | 57 | Ductal | TN | IV |
| 14 | 48 | Ductal | HER2 | III |
| Patients with BC from Toluca City | ||||
| A12 | 65 | Canicular | Luminal | I |
| A17 | 58 | Canicular | Luminal | 0 |
| A18 | 53 | Canicular | Luminal | I |
| A19 | 52 | Canicular | Luminal | II |
| A20 | 54 | Canicular | TN | III |
| A21 | 48 | Canicular | Luminal | III |
| A22 | 47 | Canicular | Luminal | II |
| A24 | 53 | Canicular | Luminal | II |
| A38 | 36 | Canicular | TN | II |
| A41 | 49 | Canicular | Luminal | I |
| A42 | 52 | Canicular | NI | NI |
| A43 | 58 | Canicular | TN | II |
| A44 | 64 | Canicular | TN | II |
| A45 | 50 | Canicular | Luminal | III |
| A46 | 58 | Canicular | Luminal | I |
| A47 | 49 | Canicular | HER2 | IV |
| A48 | 62 | Canicular | HER2 | III |
| A49 | 43 | Canicular | Luminal | 0 |
| A50 | 47 | Canicular | Luminal | II |
| A51 | 46 | Canicular | Luminal | I |
| A52 | 52 | Canicular | NI | NI |
| A53 | 48 | Canicular | NI | NI |
| A54 | 54 | Canicular | HER2 | II |
| A55 | 45 | Lobulillar | TN | III |
| A57 | 45 | Canicular | Luminal | II |
| A58 | 34 | Canicular | Luminal | II |
| A59 | 40 | Canicular | TN | IV |
| A60 | 52 | Canicular | Luminal | 0 |
| A61 | 58 | Canicular | Luminal | II |
| A62 | 48 | Canicular | Luminal | II |
| A63 | 46 | Canicular | HER2 | III |
| A64 | 40 | Canicular | Luminal | II |
| BC survivors from Toluca City | ||||
| N24 | 44 | Canicular | Luminal | II |
| N25 | 61 | Canicular | Luminal | II |
| N26 | 46 | Canicular | Luminal | III |
| N27 | 47 | Canicular | Luminal | NI |
| N29 | 56 | Canicular | Luminal | III |
| N30 | 56 | NI | Canicular | NI |
| N31 | 43 | NI | Luminal | III |
| N32 | 43 | Canicular | Luminal | II |
| N33 | 56 | Canicular | Luminal | 0 |
| N34 | 64 | Canicular | HER2 | 0 |
| N37 | 60 | Canicular | Luminal | II |
| N40 | 49 | Canicular | TN | II |
| N42 | 52 | Canicular | Luminal | NI |
| N43 | 58 | Canicular | Luminal | NI |
| N46 | 48 | Canicular | HER2 | 0 |
| N48 | 55 | Canicular | Luminal | NI |
| N51 | 49 | Mucinous | Luminal | NI |
| N52 | 53 | Lobulillar | Luminal | NI |
| N53 | 52 | Canicular | NI | NI |
| Compound | Linear Range (pg) | Slope | Intercept | r2 | Monitored Ions |
|---|---|---|---|---|---|
| BPA-TMS | 0.1–10 | 0.0078 | 0.0375 | 0.9902 | 357, 358, 372 |
| BPS-TMS | 0.1–10 | 0.0025 | 0.004 | 0.9856 | 394, 379 |
| DEP | 10–10,000 | 0.002 | 0.2031 | 0.9948 | 149, 177, 76 |
| DBP | 10–10,000 | 0.0045 | 0.4721 | 0.9998 | 149, 205, 223 |
| BBP | 10–10,000 | 0.0019 | 0.0548 | 0.9999 | 149, 91, 206 |
| DEHP | 10–10,000 | 0.0027 | 0.2162 | 0.9995 | 149, 176, 279 |
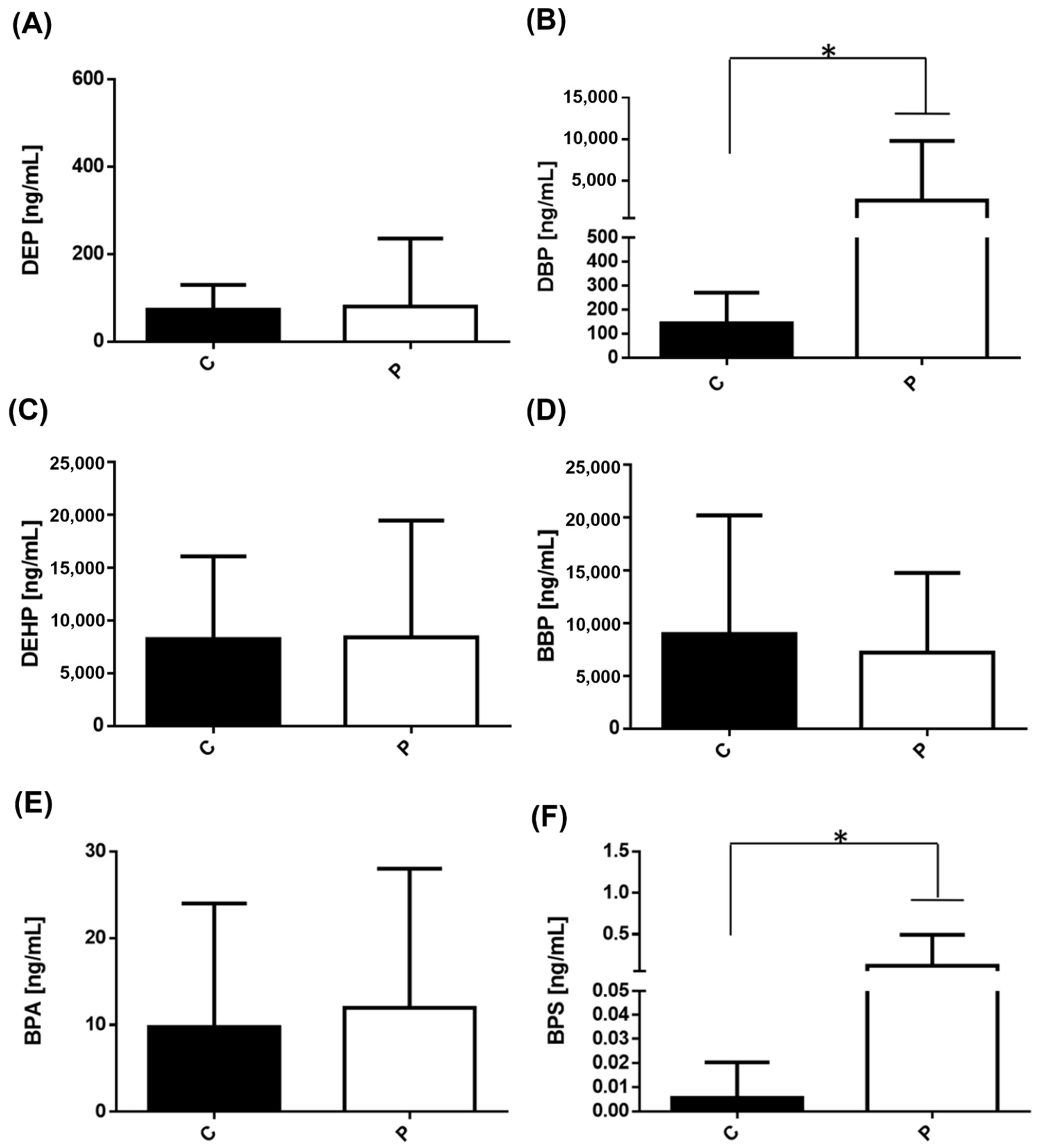
| Compound | Controls | Women with BC | Survivors of BC | p-Value |
|---|---|---|---|---|
| DEP | 72.70 ± 56.81 | 100.13 ± 179.27 | 103.77 ± 91.29 a | 0.0047 |
| DBP | 143.62 ± 126.91 | 3421.86 ± 8314.50 a | 237.55 ± 268.90 b | <0.0001 |
| DEHP | 8259.79 ± 7835.16 | 8314.61 ± 12,975.97 | 8243.22 ± 821.73 | 0.3650 |
| BBP | 9226.21 ± 12,740.50 | 6425.55 ± 8805.81 | 0 a,b | 0.0284 |
| BPA | 4.63 ± 3.10 | 13.73 ± 17.09 a | 5.37 ± 2.99 b | 0.0254 |
| BPS | 0.01 ± 0.02 | 0.12 ± 0.37 | 0 | 0.1851 |
| Study Population | Objective | Results/Conclusion | Ref. |
|---|---|---|---|
| Phthalates | |||
| Women with BC (233) residing in northern Mexico. 221 healthy women. | Phthalates were determined in urine samples by isotope dilution/high performance liquid chromatography coupled to tandem mass spectrometry. | Concentrations of mono-ethyl phthalate (MEP) were higher in cases (169.58 µg/g creatinine) than in controls (106.78 µg/g creatinine) Controls showed significantly higher concentrations of mono-n-butyl phthalate, mono(2-ethyl-5-oxohexyl) phthalate, and mono(3-carboxypropyl) phthalate (MCPP) than did the cases. The authors show for the first time that exposure to diethyl phthalate (DEP), the parent compound of MEP, may be associated with an increased risk of BC, whereas exposure to the parent phthalates of MBzP and MCPP (BBP and dioctyl phthalate, DOP, respectively) might be negatively associated with the incidence of this disease. | [20] |
| Association of phthalate exposures and breast cancer risk in a Danish nationwide cohort (1,122,042 women), using redeemed prescriptions for phthalate-containing drug products to measure exposure. | Drugs containing phthalates that were marketed in Denmark were registered in an internal Danish Medicines Agency database. The authors enrolled a Danish nationwide cohort of 1.12 million women at risk for a first cancer diagnosis on 1 January 2005. The authors calculated the annual cumulative phthalate exposure content of each filled prescription by multiplying the mass of phthalate per capsule by the fill amount. They calculated the cumulative milligrams of cellulose acetate (CAP) phthalate or polyvinyl acetate phthalate contained in all prescriptions filled by a patient during each year of follow-up. Finally, they made a multivariable Cox regression to estimate the associations between phthalate exposure and the incidence of invasive breast carcinoma according to the ER status of tumors. | High-level dibutyl phthalate (DBP) exposure (>10,000 cumulative mg) was associated with an approximately two-fold increase in the incidence rate of ER+ breast cancer. Cumulative exposures to DBP, cellulose acetate phthalate (CAP), and hydroxypropyl methylcellulose phthalate (HPMCP) were categorized as no exposure, 1 to 249 mg, 250 to 999 mg, 1000 to 9999 mg, and 10,000 mg or more. Cumulative exposure to DEP was categorized as unexposed, 1 to 9 mg, 10 to 99 mg, and 100 mg or more. Polyvinyl acetate phthalate (PVAP) exposure was rare and therefore modeled as a dichotomous variable (unexposed to any exposure [range, 1.3 to 682 cumulative grams]). | [21] |
| Case-control study within the Women’s Health Initiative (WHI) prospective cohort (419 invasive cases and 838 controls) | Quantification of 13 phthalate metabolites and creatinine in two or three urine samples per participant over one to three years | The urinary concentration of phthalates did not result in an increased risk of developing invasive BC in postmenopausal women. However, not entirely consistent, but the authors observed some positive effects between phthalate biomarker concentrations and BC diagnosed within three years. In addition, the majority of the positive association was significant for ER+/PR+ disease. It is worth noting that the positive effects estimated were closer to null and not statistically significant when analyses were extended to include case subjects diagnosed within five years or among the full study population. The above suggests that urine phthalate biomarker concentrations predict short-term, but not long-term BC risk. The authors grouped phthalate biomarkers by their parent phthalates by dividing the concentrations of each metabolite of a single parent by its molecular weight and then summing the concentrations across metabolites were corrected for creatinine concentration. The authors did not report a range of concentrations of phthalates, they reported the odds ratios established for each phthalate. | [22] |
| Case-control study of Alaskan native women 170 women (75 cases, 95 controls) | To measure the association between exposure to environmental chemicals and breast cancer. Seven to ten phthalate metabolites were measured in urine samples. | The authors found a potential association for DEHP exposure, which results in high levels of monoethylhexyl phthalate (MEHP) metabolites and the progression of breast cancer. The concentrations of phthalate metabolites were creatinine corrected (3.5 µg/g creatinine in controls and 5.3 µg/g creatinine in cases). Although urinary concentrations for most of the 7 phthalates metabolites were higher among cases than controls, these differences were not statistically significant. 40 of the 62 women who had invasive tumors had BC with an ER+/PR+ phenotype; the rest of them were negative for hormone markers. Urine concentrations were higher in 3 of 7 phthalate metabolites among women with ER-/PR-tumors. The differences were not statistically significant | [23] |
| Women resident of northern Mexico with histologically confirmed BC (233 individuals) and healthy controls (221 individuals) | To evaluate if phthalate exposure interacts with a flavonoid diet to promote the risk of BC. Urinary metabolites concentrations of nine phthalates were made and corrected to creatinine concentration. | A higher intake of anthocyanidins and flavan-3-ols (from vegetables), synergistically increased the a negative association between monobenzyl phthalate (MBzP), a metabolite of BBP, and the risk of BC. The consumption of some flavonoids may interact with exposure to phthalates with the risk of BC. Concentrations of urine metabolites of phthalates were found in a range of (5–139 μg/g creatinine). | [24] |
| U.S women with BC (cases = 43, controls = 1964 individuals) | Examination the relationship between the exposure to different endocrine disruptor compounds such as polychlorinated biphenyls (PCBs), BPA or phthalates; and risk of BC in U.S. women. The authors measured the urinary levels (ng/g) of BPA and ten metabolites of phthalates. Urinary levels were corrected to the creatinine concentration. | There were no significant associations between phthalates or BPA and BC. | [25] |
| Meta-analysis Search in the literature with different databases were performed in PubMed, Embase, and Cochrane library (2288 articles were included) | Assessment of the association between urinary phthalate metabolites and risk of BC and uterine leiomyoma. | DEHP metabolites were associated with an increased risk of BC as well as uterine leiomyoma. Important considerations for the authors: The ranges of cut-off levels of urinary phthalate metabolites were not consistent among the studies, which affect the general conclusions. Most of the studies reviewed analyzed the exposure of phthalates at a specific point in the disease, but it was impossible to calculate exactly the cumulative exposure dose, which might lead to limited conclusions. It is necessary to extend the study to different geographic regions or ethnic populations | [26] |
| Bisphenols | |||
| Polish women with or without BC in post-menopause. (1962) BC cases (1338 postmenopausal) and 2241 controls (1529 postmenopausal) | To evaluate the association between urinary unconjugated BPA and a metabolite of BPA, the BPA-glucuronide (BPA-G) and risk of BC in postmenopausal women from Poland. Urinary levels of BPA-G were calculated and creatinine-adjusted (ng-BPa-G/mg creatinine). The range of BPA concentrations for BC cases was around 2.29–4.78 ng/mg; and in controls was 2.76 ng/mg | There was no association between BPA-G and women with BC in the postmenopausal stage. | [27] |
| 711 women with BC and 598 women without BC belonged to Nassau and Suffolk Counties on Long Island, NY | To evaluate the association of seven urinary phenol biomarkers and BC incidence with subsequent mortality. The authors also examined the effect measure modification by body mass index (BMI). The measurements were made in urine samples and corrected for concentrations of creatinine | The concentrations of BPA found in the control group were around 1.2 μg/g creatinine and 1.3 in women with BC. There was no association between BPA levels and BC incidence. Mortality associations were more pronounced among women with high body mass index. BC incidences were strongly related to urinary concentrations of parabens | [28] |
| Korean women with or without BC (N = 167) | Potential associations between BPA exposure and risk of BC in Korean women among patients with BC and controls (N = 167). The levels of BPA were monitored in serum samples (μg/L) | There were no significant differences in the serum levels of BPA (conjugated + free form) between the cases and controls. The range of conjugated BPA levels was 0–13.87 μg/L, and the levels of free BPA were 0.012–0.04 μg/L. | [29] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segovia-Mendoza, M.; Palacios-Arreola, M.I.; Monroy-Escamilla, L.M.; Soto-Piña, A.E.; Nava-Castro, K.E.; Becerril-Alarcón, Y.; Camacho-Beiza, R.; Aguirre-Quezada, D.E.; Cardoso-Peña, E.; Amador-Muñoz, O.; et al. Association of Serum Levels of Plasticizers Compounds, Phthalates and Bisphenols, in Patients and Survivors of Breast Cancer: A Real Connection? Int. J. Environ. Res. Public Health 2022, 19, 8040. https://doi.org/10.3390/ijerph19138040
Segovia-Mendoza M, Palacios-Arreola MI, Monroy-Escamilla LM, Soto-Piña AE, Nava-Castro KE, Becerril-Alarcón Y, Camacho-Beiza R, Aguirre-Quezada DE, Cardoso-Peña E, Amador-Muñoz O, et al. Association of Serum Levels of Plasticizers Compounds, Phthalates and Bisphenols, in Patients and Survivors of Breast Cancer: A Real Connection? International Journal of Environmental Research and Public Health. 2022; 19(13):8040. https://doi.org/10.3390/ijerph19138040
Chicago/Turabian StyleSegovia-Mendoza, Mariana, Margarita Isabel Palacios-Arreola, Luz María Monroy-Escamilla, Alexandra Estela Soto-Piña, Karen Elizabeth Nava-Castro, Yizel Becerril-Alarcón, Roberto Camacho-Beiza, David Eduardo Aguirre-Quezada, Elías Cardoso-Peña, Omar Amador-Muñoz, and et al. 2022. "Association of Serum Levels of Plasticizers Compounds, Phthalates and Bisphenols, in Patients and Survivors of Breast Cancer: A Real Connection?" International Journal of Environmental Research and Public Health 19, no. 13: 8040. https://doi.org/10.3390/ijerph19138040
APA StyleSegovia-Mendoza, M., Palacios-Arreola, M. I., Monroy-Escamilla, L. M., Soto-Piña, A. E., Nava-Castro, K. E., Becerril-Alarcón, Y., Camacho-Beiza, R., Aguirre-Quezada, D. E., Cardoso-Peña, E., Amador-Muñoz, O., Garduño-García, J. d. J., & Morales-Montor, J. (2022). Association of Serum Levels of Plasticizers Compounds, Phthalates and Bisphenols, in Patients and Survivors of Breast Cancer: A Real Connection? International Journal of Environmental Research and Public Health, 19(13), 8040. https://doi.org/10.3390/ijerph19138040