Abstract
Virtual communities of practice consist of individuals who use a common online platform to share professional expertise and experiences. In healthcare settings a virtual community of practice (VCoP) can optimise knowledge, skills, and the implementation of evidence-based practice. To ensure effective knowledge synthesis and translation into practice, it is essential to clarify the best methods for designing and implementing VCoPs within healthcare organisations. This scoping review aimed to identify the methods used to establish and facilitate online or digitally enabled communities of practice within healthcare organisations across the globe. Six online databases identified papers published from January 2010 to October 2020. Papers were independently screened by two reviewers using Covidence. Data were captured and analysed using a data extraction chart in Covidence. Twenty-four publications that detail methods for establishing a VCoP in healthcare were included. Few studies used a framework to establish a VCoP. It was difficult to identify details regarding methods of development and key elements such as roles, how they were coordinated, and types of technology used. Healthcare organisations can benefit from using a standardised framework for the establishment, implementation and evaluation of VCoPs to improve practice, staff engagement, and knowledge sharing.
1. Introduction
Communities of practice (CoP) are networks of individuals who interact regularly to share their interests and develop their knowledge, skills, and capabilities concerning a particular issue [1]. As internet and mobile device use has grown globally, virtual communities of practice (VCoPs) have become more prevalent in healthcare [2,3]. The COVID-19 pandemic limited physical interactions and meetings for sharing of expertise. As a consequence, the relevance and utility of VCoPs became more prominent [4]. Technology based VCoPs can provide opportunities for healthcare professionals to learn, collaborate, and share information without the limitations imposed by geography, cost, organisational boundaries, and time differences [5,6,7]. VCoPs may improve retention of healthcare professionals by reducing perceived professional isolation in rural and regional areas [8]. Health professionals who participate in a VCoP have the opportunity to share ideas, resources and knowledge, as well as access specialised knowledge [9]. VCoPs can also enhance interprofessional collaboration by reducing professional barriers and providing healthcare teams the opportunity to share and implement evidence-based practice [5]. Another benefit is the provision of a risk-free environment for members, increasing the potential for active participation [8]. While VCoPs allow health professionals to stay connected and informed, knowledge sharing in virtual communities can be limited by individual factors (such as active contributions from members), technological factors (such as access to technology and usability issues), and social factors (such as interaction within the group) [9,10,11,12].
Healthcare VCoPs have a variety of forms that allow participants to engage in either synchronous or asynchronous knowledge gain. They typically utilise a range of digital formats to establish a common virtual collaborative space [3]. These include teleconferences, webinars, videoconferences, online meeting spaces, websites, emails, the intranet, and social media [13]. Some VCoPs include blogs, online discussion forums, or file repositories [14]. Project Extension for Community Healthcare Outcomes (ECHO) is an example of a healthcare VCoP [15]. ECHO uses videoconferencing technology that allows primary care providers in rural community clinics to access a multidisciplinary team of specialists [16]. VCoPs can also be established using social media platforms, such as Facebook, Twitter and LinkedIn [8]. For example, Free Open Access Medical education (FOAM) for emergency medicine and critical care [17] communicates via Twitter [18], blogs, and podcasts [19]. Blogs and podcasts that review and present the newest evidence about a topic also allow health professionals to gain easy access to information from clinical experts [20].
The establishment of CoPs in healthcare can be enabled by employing a framework to guide development and ongoing operation [21]. Few studies report how a CoP is designed, implemented, and evaluated in alignment with user needs [3]. Wenger et al. (2002) described seven design principles for developing communities of practice in order to promote development and sustainability [22]. Probst and Borzillo (2008) proposed a CoP governance model based on 57 CoPs from leading business organisations. Their model includes setting clear objectives, sponsorship by senior executives, designation of leadership roles, establishing links beyond the community’s boundaries, ensuring a risk-free environment, and outcome measures to assess the value of CoPs [23]. Barnett et al. (2012) used Probst and Borzillo’s CoP framework to evaluate evidence for VCoPs in medical general practice training [6]. Their proposed health VCoP framework added the extra element of technology with usability, accessibility, and flexibility, of prime importance for knowledge exchange, staff empowerment and learning [6].
VCoPs are becoming increasingly popular in healthcare; however, the best methods to establish VCoPs and which frameworks ensure effective uptake and sustainability have not yet been realised. The characteristics of virtual environments help determine the successful design and management of VCoPs [24]. The aim of this scoping review was to identify the methods used to develop and sustain VCoPs and determine the essential components required to guide the establishment and facilitation of a VCoP for healthcare professionals.
2. Materials and Methods
The published protocol paper provides full details regarding the methods used to conduct this scoping review [25]. The review was conducted based on Arksey and O’Malley’s methodological framework [26] and refined using the Joanna Briggs Institute (JBI) methods for scoping reviews [27]. The PRISMA-ScR checklist [28] was followed and reviewed by the research team (LS, DJ, DK and MM) (Table S6). The PRISMA-ScR checklist has five sections: (a) identifying the research question, (b) identifying relevant studies, (c) identifying the study selection criteria, (d) charting the data, and (e) reporting the results.
- (a)
- Identifying the research question
The primary research question was (i) What is the extent of reported research on establishing VCoPs in healthcare published in the last 10 years (January 2010 to October 2020)? Additional research questions focused the review to provide guidance for setting up and conducting a VCoP in healthcare: (ii) What methods are used to establish and maintain VCoPs (including frameworks used for VCoP development, who the participants are, how it is coordinated, and methods of communication and knowledge exchange)? and (iii) What potential barriers and facilitators are identified during the implementation of VCoPs? The authorship team included researchers with clinical expertise.
- (b)
- Identifying relevant studies
Eligibility criteria: The population of interest was healthcare professionals who were part of a VCoP for the purposes of building and exchanging knowledge, developing individual capabilities, ensuring their practice is evidence-based, and enhancing interprofessional collaboration. The concept of interest was virtual communities of practice for the purpose of improving clinical outcomes. Communities of practice that described themselves as ‘virtual’, ‘on-line’ or ‘web-based’ were included. The literature included discussed the establishment and maintenance of VCoPs implemented in a healthcare setting for healthcare professionals. The context of interest was any platform used by healthcare professionals to support virtual interactions in healthcare for knowledge advancement and sharing ideas.
Included articles were accessible as full text and published between January 2010 and October 2020. They were peer-reviewed and written in English. All research methods, such as quantitative, qualitative, mixed methods, systematic reviews, meta-analyses, and guideline implementation, were included. Exclusions included grey literature, commentaries, conference proceedings, and any other opinion pieces. Studies that only evaluated VCoPs, or described VCoPs that were used only for teaching purposes (for example online learning) were also excluded.
Search strategy: The study group followed a three-step search strategy as identified by the JBI [29] in collaboration with an academic librarian, who executed the searches. The final comprehensive search was conducted across PubMed, CINAHL, CENTRAL, PsycINFO, Cochrane Library and Education Resources Information Center. Full details and an example of the search strategy, carried out in PuBMed and CINAHL, are detailed in the protocol paper [25].
- (c)
- Study selection criteria
Studies identified in the search were uploaded to Covidence. The titles and abstracts of retrieved papers were independently screened by two reviewers (LS, DJ). The same two reviewers independently screened full texts to identify studies meeting the review criteria. At each stage, any conflicts were resolved by discussion to consensus, with a third study group member (MM) consulted if necessary.
- (d)
- Charting the data
Data from eligible studies were charted independently by two researchers (LS, DJ) using a data extraction chart developed in Covidence. The tool captured relevant information about key study characteristics identified in the literature, including aims, development and size of the network, stage of development, technological infrastructure, VCoP roles, processes, participants, methods of recruitment, and evaluation. Further detail is provided in the protocol paper [25].
- (e)
- Collating, summarising, and reporting the results
Quantitative and qualitative data from the final dataset were synthesised via an iterative process with new categories and themes identified through ongoing analysis. Thematic analysis was utilised for the qualitative data, and quantitative data were summarised using frequency analysis, with the counts for each category calculated. Further details regarding data synthesis are outlined in the protocol paper [25].
3. Results
Following removal of duplicates, 2314 records were retrieved from the five databases. The results of the search strategy are shown on the PRISMA flow diagram (Figure 1). Title and abstract reviews identified 2238 records that did not meet the eligibility criteria as detailed in the methods section ‘Identifying relevant studies’. A total of 72 full text articles were assessed for eligibility, and 48 were excluded. The most common reasons for exclusion included: the study was an evaluation study only (n = 13); the intervention did not match the research question (n = 6); no full text was available (n = 5); the setting was wrong (n = 5); or the study design was incorrect (n = 5). The final review retained 24 articles.
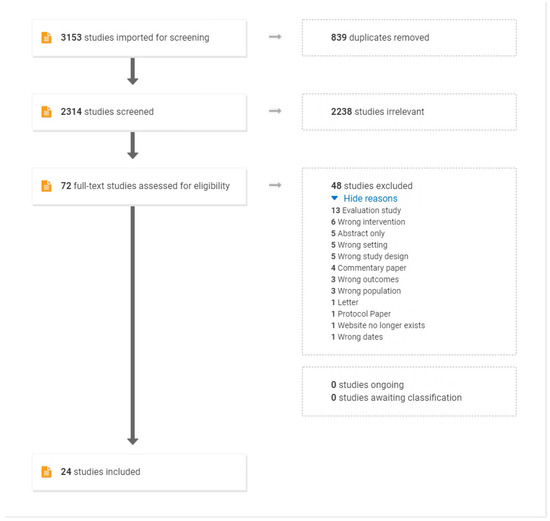
Figure 1.
PRISMA Diagram of Scoping Review Results for VCoPs in healthcare.
3.1. Study Characteristics
Tables S1–S3 outline study characteristics such as year published, study design, and the country in which the study was conducted, which demonstrates the geographic range of included studies. Most studies were conducted in the USA (n = 9), Australia (n = 4), and Canada (n = 3).
3.2. Research Methodology
Most of the VCoP studies used a case report design (n = 9). Three studies reported using mixed methods [30,31,32]. Other study design descriptions included participatory action research [33] and a discussion paper [34].
3.3. Literature Review Papers
Five reviews were identified in the fields of social work [35], GP training [6], health and social care professionals [8], and healthcare [36,37]. These were presented as a rapid review [35], a systematic review [36], integrated reviews [8,37], and a literature review [6]. Broadly, the studies reviewed what is already in the literature regarding VCoPs for certain fields, methods of development, and usefulness. Common themes include the usefulness of VCoPs for increasing knowledge, professional development [8,37], and decreasing isolation [8], as well as the importance of privacy and trust [8,35]. Of note, and unlike other studies, Barnett et al.’s study [6] proposed a new framework for the development of VCoPs based on Probst and Borzillo’s framework, [23] as well as the findings of their review. Their proposed framework included the key themes of facilitation, champion and support, objectives and goals, a broad church, supportive environment, measurement benchmarking and feedback, technology, and community. While further research is needed, this framework may be of use in future studies. Ranmuthugala et al. (2011) sought to understand the reasons for, composition of, and intended purpose of establishing CoPs in healthcare, as well as methods of interaction and outcomes [21].
3.4. Study Aims
The study aims are summarised in Tables S1–S3. Over half (n = 14) of the studies stated that their aim was to report the guidelines or the process for developing and implementing a VCoP, which reflects the inclusion criteria for this study. Many also aimed to evaluate the implications of a VCoP on practice (n = 9). Half of the studies (n = 12) reported that the purpose of the VCoP was to support the implementation of evidence-based practice and translation of research. Another reported purpose was to conduct a literature review of the evidence supporting VCoPs in healthcare (n = 4). Two studies describe the development of an Extension for Community Healthcare Outcomes (ECHO) [16,38].
3.5. Background and Purpose of the VCoP
The majority of VCoPs were developed to support sharing professional knowledge, facilitate communication, and foster implementation of evidence-based practice amongst medical professionals and into communities that are geographically dispersed. VCoPs provided the opportunity for health professionals working in rural communities to learn from specialists in more urban areas; supporting doctors in rural practices in South Africa, for example [39]. Other VCoPs included researchers and practitioners with the intent to facilitate the dissemination of research findings into practice [40]. The ECHO system of VCoPs, such as those reported by Lewiecki et al. (2019) [16] and Lewis et al. (2018) [38], provided tele-mentoring through case presentations and didactic presentations, delivering continuing medical education (Table S4).
3.6. Dates
Where stated, almost all VCoPs commenced in the last 20 years, which likely reflects the date ranges imposed on the initial search. Six papers did not state the dates of commencement of VCoPs, or it was unclear [14,30,33,34,39,41]. The longest established VCoP reported was the Cancer Research Network, which has been supported by the National Cancer Institute since 1999 [42]. Project ECHO, the basis for two studies [16,38], was established almost 20 years ago, in 2003 [15].
3.7. Methods of Recruitment
There was wide variation in methods used to recruit members. Ten studies that were not literature reviews did not state their method of recruiting participants, or it was unclear [14,16,31,34,38,40,42,43,44,45]. VCoPs often used more than one recruitment method. The most stated method of recruitment was via email (n = 4) [32,46,47,48]. One VCoP actively promoted the establishment of the VCoP [47], while in the case of two studies, healthcare professionals volunteered as members after hearing about the study [41,49]. Other methods of recruitment include purposive sampling [39], a hospital survey [33], a face-to-face workshop [30], and recruitment via the researcher [41]. Methods of recruitment are detailed in Table 1.

Table 1.
Methods of recruitment for VCoP participants.
3.8. VCoP Membership
The types of health professionals most often included in VCoPs were allied health professionals (n = 12) and specialist physicians (n = 10). Some VCoPs were multidisciplinary; for example, Wolbrink et al. (2017) reported that their VCoP involved a physician/consultant, fellow, resident, medical student, nurse, nursing student, nurse practitioner, and respiratory therapist [44]. Other VCoPS were interdisciplinary to advance treatment in a particular area. For example, the VCoP described by Pratte et al. (2018) consisted of paediatric physiotherapists working with children with developmental coordination disorder [30]. Alary Gauvreau et al.’s (2019) VCoP involved 13 speech-language pathologists working in aphasia rehabilitation [41]. See Table 2.
Table 2.
Membership population of VCoP.
3.9. Sponsorship and Leadership Roles
Three VCoPs [30,41,47] were sponsored by the authors reporting on the VCoP. For example, Alary Gauvreau’s evaluation study for speech-language pathologists in aphasia rehabilitation was undertaken as part of her PhD [41]. Landes et al. (2019) reported on the building and implementation of a VCoP for dialectical behaviour therapy for the Department of Veterans Affairs that she created as a psychologist, researcher, and employee of Veterans Affairs [47]. Other VCoPs were joint ventures between healthcare organisations and universities; for example, a community of practice for dementia champions between Health Education England and the University of Hertfordshire [34], and a social work VCoP was a partnership between the University of Buffalo School of Social Work and the University of Buffalo Teaching and Learning Centre [45]. Other VCoPs were supported by large organisations such as Project ECHO [16,38] and the National Cancer Institute [40].
Facilitators or leaders were reported to drive the community and encourage members to participate. They may, for example, coordinate the preparation and conduction of meetings [46]. The Swedish Oral Medicine Network’s monthly meetings were led by a chairperson, but the meeting’s facilitation rotated among core members [43]. For a VCoP formed for the purpose of General Practitioners’ continuing professional development, the facilitation team comprised specialist physicians, senior GPs, a dedicated content facilitator, and an information technology administrator [48]. Additional roles included clinical experts, champions, and knowledge brokers, which are described in Table S5.
3.10. Technology and Infrastructure
A wide variety of web and internet tools were used to facilitate VCoPs; this allowed members to access VCoPs from anywhere, promoting active participation and interaction for health professionals who are isolated or have time limitations. Many VCoPs utilised more than one type of technological infrastructure. Over half (n = 14) of the studies reported using a web-based or digital platform (e.g., Web 2.0 or Microsoft SharePointWeb). The remainder used videoconferencing (e.g., Adobe Connect, Zoom) (n = 3), social network sites (n = 1), and podcasts (n = 1). Table 3 details the technological infrastructure of the reviewed VCoPs.
Table 3.
Technological infrastructure of VCoPs.
3.11. VCoP Development
The extensive variety of presentations of VCoPs revealed considerable variability in how networks were developed (see Table S4). For some VCoPs, development was planned and organised. For example, Lewis et al. (2010) described the development of a VCoP for the University of Buffalo’s School of Social Work using Wenger’s developmental stages of a CoP [45]. Lewis et al. (2010) outlined how project goals and aims were developed and how these were matched to the VCoP technology platform [45]. TeleECHO networks were developed with the support of a dedicated team from Project ECHO which conducted training for those committed to starting and developing this method of VCoP [15]. Conversely, other VCoPs developed less purposefully, and possibly evolved from pre-existing conference meetings; for example, Friberger (2013) reported that in the early 1990s, four hospital clinics discussed cases via telephone conferencing, which evolved into the Swedish Oral Medicine Network (SOMNet) [43].
3.12. Size of the Network
The size of the network for the VCoPs was not always reported in the papers. Where it was reported, size varied greatly and was reported in multiple ways, including the number of individual members or participants, hospitals, and research centres, as well as the number and range of countries included in the network. For example, one VCoP included 13 speech and language pathologists across a city [41], compared to an online platform such as OPENPedatrics, which engaged a global community of critical care clinicians [44]. The VCoP model ‘Project ECHO’, which was discussed in two papers [16,38], reported participants in more than 9000 cities and 180 countries since launching [15]. Other papers where the VCoP included a website also reported the number of page views and site visits in a particular time period; for example, Ting (2018) stated that the CanadiEM website (at the time of reporting) had more than 2.5 million page views from 217 countries [49]. The size of the networks is detailed in Tables S2 and S3.
3.13. VCoP Forms of Interaction
A wide range of formats for VCoP interactions were reported, although not all papers provided detailed descriptions of the activities that were included (Table 4). Several VCoPs (n = 8) offered a learning hub platform (e.g., [30,48]) with resources available on a website and asynchronous learning occurring via an online discussion forum, for example. Others offered live discussions (for example, case studies, clinical questions, and hot topics), online meetings, and live presentations by a guest speaker or clinical expert. An online discussion platform via forum posts was the most reported activity (n = 9), followed by online live discussions (for example, case-based presentations, clinical questions, and hot topics) (n = 7). Other activities included periodic emails with news, updates, or notifications of forum posts (n = 5). Some VCoPs reported providing recordings of live meetings (n = 3), online-live presentations (n = 3), YouTube videos, or webinars (n = 2). Less commonly reported activities were blogs, tele-mentoring, and podcasts.
Table 4.
VCoP forms of interaction.
3.14. Theoretical Frameworks Supporting Development of the VCoPs
Six VCoPs did not report using a specific framework [8,14,30,34,43,48]. The most reported framework for the development of VCoPs was Wenger’s CoP theoretical framework (n = 4) [31,40,45,49]. Two VCoPs were part of an overarching model, such as Project ECHO. The ECHO model learning framework involved a virtual community of participants who presented anonymized cases to specialists and their peers for discussion and recommendations [15], such as Bone Health TeleECHO [16] and Dermatology ECHO [38]. Probst and Borzillo’s (2008) framework of successful factors for VCoPs [23] formed the basis of one of the reviewed VCoPs, which was a web based VCoP for primary health workers in the Basque Health System [46]. Following a literature review of General Practice training and VCoPs, Barnett et al. (2012) developed a health VCoP framework [6] that was also based on Probst and Borzillo’s business CoP framework [23]. Two reviewed papers reported using Barnett’s health VCoP framework [35,47]. Theoretical frameworks employed for each VCoP are detailed in Table S4. The number and types of frameworks used are noted in Table 5.
Table 5.
Theoretical framework for development of VCoP.
3.15. Outcome Measures
Although ‘evaluation only’ studies were excluded in this scoping review, many included studies had an evaluation component. The methods employed for outcome measurement also varied; quantitative outcomes such as level of participant engagement and web analytics being common evaluation tools. Landes et al. (2019), for example, used web analytics to measure usage trends, including the number of unique users each month, user locations, visits, and average number of requests [47]. Qualitative outcomes included member surveys, semi-structured interviews, and focus groups regarding members’ views on enablers, challenges, processes and outcomes.
Many studies used mixed methods to assess the level of impact of the VCoP. Farrell et al. (2014) claimed that web analytics alone would not capture the full extent of the growth and member engagement of the CoP; in addition to page views and membership data, they collected the level of response to different discussion postings and regular member surveys [40]. Wolbrink et al. (2017) combined web-based member surveys with site analytics to evaluate their online paediatric critical care CoP [44]. SOMNet evaluation methods included an online questionnaire, interviews with participants, and observations of teleconference meetings [43]. Lewis et al. (2018) presented findings from a case study using photographs to demonstrate how the ECHO VCoP worked to improve both provider knowledge and patient outcomes [38]. Outcome measures employed are detailed in Tables S1 and S2.
4. Discussion
This scoping review showed rapid progress in the development of virtual communities of practice across the globe to improve evidence-based practice and clinical outcomes in healthcare. Several methods were used to develop and maintain VCoPs, such as webinars, online discussions, blogs, live case discussions, and use of social media. There was, however, little consensus regarding the best way to approach VCoP design and implementation in healthcare settings. Extensive variability was observed in the types of participants, how they were coordinated and facilitated, methods of access, communication approaches, and digital support. Dube et al. noted that VCoPs in organisations share some common characteristics, yet they all have ‘unique personalities’ [13].
The evidence synthesis also highlighted wide variations in the quality of reporting in the literature reviewed. Thirteen full text articles were rejected as they only evaluated the VCoP and did not provide details about methodology. The process of establishing, developing, and maintaining VCoPs was also inadequately reported. A lack of description of the key elements of the development of a VCoP makes it difficult for others to replicate interventions and identify best practices for how additional CoPs can be best designed to facilitate sharing information and knowledge [36].
Wenger et al. advised that for CoPs, it is important to know the best methods of development and implementation to benefit participants as well as the host organisation [22]. Our findings highlighted that healthcare VCoPs are diverse in nature and not always implemented in a systematic manner. A small number of studies used a framework to design and develop their VCoP. Four reviewed papers [31,40,45,49] utilised Wenger’s principles for the development of a CoP [22], which suggests that these principles could be successfully applied. The additional elements of mode of interaction and technology employed could also be considered. Two studies [35,47] employed Barnett et al.’s framework [6] for the development of their VCoPs. Barnett et al.’s proposed health VCoP framework [6], developed from Probst and Borzillo’s ten commandments for VCoPs gleaned from the business literature [23], added the elements of technology and community [6]. These two elements may ensure ease of use and access, with options for both synchronous and asynchronous communication [6]. Further evaluation is warranted to determine whether this framework could be applied to the development of future international healthcare VCoPs. An action research framework was suggested in one paper, with the development of the CoP recorded by facilitators, in addition to community projects that were devised and implemented [50]. The use of a standardised framework may assist a quality assurance process to ensure all key elements are considered in the design and reporting of the establishment of VCoPs for healthcare.
Important factors in the growth of VCoPs for healthcare professionals in a 7-year longitudinal study was the presence of a centralised leadership structure and the frequent rotation of leadership over time [9]. Few papers in this scoping review detailed the key organisation or sponsor of the VCoP. A VCoP pre-implementation survey for general practice training revealed that potential members perceived a VCoP’s sponsor to be important as an initial stakeholder champion [2]. Other roles described in the reviewed papers included leaders, facilitators, subject matter experts, and content editors; however, who performed each of these roles was seldom indicated. Sometimes, the researchers reporting on the VCoP, Galheigo et al. (2019) [33] and Alary Gauvreau et al. (2019) [41], for example, also held VCoP roles such as facilitators or leaders.
An extensive range of technologies and formats for VCoP interactions were reported. VCoPs depend on active participation by all members to develop and share content. All members need to be encouraged to contribute to discussions that enable the VCoP to be successful and sustainable [8]. However, methods of interaction within VCoPs are likely to influence members’ experiences [3]. Online live discussion forums were popular, suggesting that their social nature helped to create a sense of community among members [8]. A key factor in VCoPs’ success is members’ perceived trust and commitment to both each other and the organisation, which may be assisted by live discussion [20,42]. Member engagement can also be facilitated by ensuring active facilitation, a stimulating environment [51], and employing technologies that allow for a range of communications and ease of use [8]. Healthcare professionals’ access to digital technologies, their technical capability, and the usability of VCoP platforms also need to be considered when developing a healthcare VCoP [9]. Digital healthcare capability frameworks that could facilitate the implementation of practice into real-world settings, have recently been published [52,53,54,55]. These frameworks highlight that health professionals benefit from an understanding of digital health technologies that enable secure connection, collaboration, and information sharing with other medical and health professionals; the potential benefits of engaging in online networks; and the technologies that support collaborative relationships [52].
This review has several limitations. Only literature published in English was reviewed; there may be other global examples of VCoPs in non-English speaking cultures. We did not analyse the digital technologies used to support VCoP, such as sensors, webcams, or robotics. The lived experience of VCoP users was beyond the scope of this evaluation. We did not evaluate how participation in VCoPs facilitated work-based learning, work satisfaction, staff retention, or career pathways. We also excluded non-empirical studies and reports that were purely qualitative in nature. Finally, the outcomes of VCoPs on common health services problems, such as hospital falls [56], awaits confirmation with controlled trials.
5. Conclusions
A variety of methods are available to establish and maintain VCoPs in healthcare. However, as a result of poor reporting on the development and key elements of VCoPs, the overall data quality was limited and difficult to extract for analysis. It was often difficult to determine if VCoPs were CoPs with a technology component. Many identified studies focused on evaluating VCoPs, members’ experiences, and user analytics, rather than detailing the methods and any theoretical frameworks used to establish the VCoP. Methods adopted depend on needs, the personal preference of participants, access to digital technologies, access to multi-media platforms to develop education and training resources within the VCoP ‘toolkits’, the time available, and support from organisational leaders. Healthcare organisations may benefit from using a standardised framework for the establishment, implementation and review of VCoPs to improve clinical practice, staff engagement, and knowledge sharing.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph19137994/s1, Table S1: Table of characteristics for review papers; Table S2: Table of study characteristics case reports; Table S3: Table of study characteristics: Other types of study; Table S4: Table of VCoP processes; Table S5: Table of VCoP roles; Table S6: PRISMA-ScR checklist.
Author Contributions
Conceptualization, L.S., D.J., D.K. and M.E.M.; methodology, L.S., D.J. and D.K.; formal analysis, L.S. and D.J.; investigation, L.S. and D.J.; resources, L.S., D.J., D.K. and M.E.M.; validation L.S., D.J., D.K. and M.E.M.; data curation, L.S. and D.J.; writing—original draft preparation, L.S.; writing—review and editing, L.S., D.J., D.K. and M.E.M.; supervision, M.E.M. and D.K.; project administration, M.E.M.; funding acquisition, M.E.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Australian National Health and Medical Research Council Project Grant, grant number Morris et al., GNT1152853.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors thank Yvonne Hamey, Holmesglen Institute librarian, for her assistance in the literature search.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wenger, E. Communities of Practice: A Brief Introduction. 2004. Available online: https://wenger-trayner.com/introduction-to-communities-of-practice/ (accessed on 26 May 2022).
- Barnett, S.; Jones, S.C.; Bennett, S.; Iverson, D.; Robinson, L.; Paton, C.; Boudry, C. A virtual community of practice for general practice training: A preimplementation survey. JMIR Med. Educ. 2016, 2, e13. [Google Scholar] [CrossRef] [PubMed]
- Fragou, O. A Design Framework for Building a Virtual Community of Practice. In The Challenges of the Digital Transformation in Education, Proceedings of the 21st International Conference on Interactive Collaborative Learning (ICL2018), Kos Island, Greece, 25–28 September 2018; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Mills, J.; Li, C.; Fullerton, S.; Chapman, M.; Jap, J.; Sinclair, C.; Collins, A.; Campbell, E. Staying connected and informed: Online resources and virtual communities of practice supporting palliative care during the novel coronavirus pandemic. Prog. Palliat. Care 2020, 28, 251–253. [Google Scholar] [CrossRef]
- Ikioda, F.; Kendall, S.; Brooks, F.; Reidy, C. Developing an online community of practice to empower health visitors: Findings from a pilot study. J. Health Visit. 2014, 2, 436–440. [Google Scholar] [CrossRef]
- Barnett, S.; Jones, S.C.; Bennett, S.; Iverson, D.; Bonney, A. General practice training and virtual communities of practice-a review of the literature. BMC Fam. Pract. 2012, 13, 87. [Google Scholar] [CrossRef]
- Dieleman, C.; Duncan, E.A. Investigating the purpose of an online discussion group for health professionals: A case example from forensic occupational therapy. BMC Health Serv. Res. 2013, 13, 253. [Google Scholar] [CrossRef]
- McLoughlin, C.; Patel, K.D.; O’Callaghan, T.; Reeves, S. The use of virtual communities of practice to improve interprofessional collaboration and education: Findings from an integrated review. J. Interprof. Care 2017, 32, 136–142. [Google Scholar] [CrossRef]
- Antonacci, G.; Colladon, A.F.; Stefanini, A.; Gloor, P. It is rotating leaders who build the swarm: Social network determinants of growth for healthcare virtual communities of practice. J. Knowl. Manag. 2017, 21, 1218–1239. [Google Scholar] [CrossRef]
- Malinen, S. Understanding user participation in online communities: A systematic literature review of empirical studies. Comput. Hum. Behav. 2015, 46, 228–238. [Google Scholar] [CrossRef]
- Amichai-Hamburger, Y.; Gazit, T.; Bar-Ilan, J.; Perez, O.; Aharony, N.; Bronstein, J.; Dyne, T.S. Psychological factors behind the lack of participation in online discussions. Comput. Hum. Behav. 2016, 55, 268–277. [Google Scholar] [CrossRef]
- Nistor, N.; Baltes, B.; Dascălu, M.; Mihăilă, D.; Smeaton, G.; Trăuşan-Matu, Ş. Participation in virtual academic communities of practice under the influence of technology acceptance and community factors. A learning analytics application. Comput. Hum. Behav. 2014, 34, 339–344. [Google Scholar] [CrossRef]
- Dubé, L.; Bourhis, A.; Jacob, R. Towards a typology of virtual communities of practice. Interdiscip. J. Inf. Knowl. Manag. 2006, 1, 69–93. [Google Scholar] [CrossRef]
- Sims, J.M. Communities of practice: Telemedicine and online medical communities. Technol. Forecast. Soc. Chang. 2018, 126, 53–63. [Google Scholar] [CrossRef]
- University of New Mexico, H.S. Project ECHO 2022. Available online: https://hsc.unm.edu/echo/ (accessed on 26 May 2022).
- Lewiecki, E.M.; Jackson, A.; Lake, A.F.; Carey, J.J.; Belaya, Z.; Melnichenko, G.A.; Rochelle, R. Bone health TeleECHO: A force multiplier to improve the care of skeletal diseases in underserved communities. Curr. Osteoporos. Rep. 2019, 17, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Nickson, C.P.; Cadogan, M.D. Free Open Access Medical education (FOAM) for the emergency physician. Emerg. Med. Australas. 2014, 26, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Roland, D.; Spurr, J.; Cabrera, D. Preliminary evidence for the emergence of a health care online community of practice: Using a netnographic framework for Twitter hashtag analytics. J. Med. Internet Res. 2017, 19, e7072. [Google Scholar] [CrossRef]
- Cadogan, M.; Thoma, B.; Chan, T.M.; Lin, M. Free Open Access Meducation (FOAM): The rise of emergency medicine and critical care blogs and podcasts (2002–2013). Emerg. Med. J. 2014, 31, e76–e77. [Google Scholar] [CrossRef]
- Thoma, B.; Brazil, V.; Spurr, J.; Palaganas, J.; Eppich, W.; Grant, V.; Cheng, A. Establishing a Virtual Community of Practice in Simulation: The Value of Social Media. Simul. Healthc. 2018, 13, 124–130. [Google Scholar] [CrossRef]
- Ranmuthugala, G.; Plumb, J.J.; Cunningham, F.C.; Georgiou, A.; Westbrook, J.I.; Braithwaite, J. How and why are communities of practice established in the healthcare sector? A systematic review of the literature. BMC Health Serv. Res. 2011, 11, 273. [Google Scholar] [CrossRef]
- Wenger, E.; McDermott, R.A.; Snyder, W. Cultivating Communities of Practice: A Guide to Managing Knowledge; Harvard Business Press: Brighton, MA, USA, 2002. [Google Scholar]
- Probst, G.; Borzillo, S. Why communities of practice succeed and why they fail. Eur. Manag. J. 2008, 26, 335–347. [Google Scholar] [CrossRef]
- Li, L.C.; Grimshaw, J.M.; Nielsen, C.; Judd, M.; Coyte, P.C.; Graham, I.D. Use of communities of practice in business and health care sectors: A systematic review. Implement. Sci. 2009, 4, 27. [Google Scholar] [CrossRef]
- Shaw, L.; Jazayeri, D.; Kiegaldie, D.; Morris, M. Virtual communities of practice to improve clinical outcomes in healthcare: Protocol for a 10-year scoping review. BMJ Open 2021, 11, e046998. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Pratte, G.; Hurtubise, K.; Rivard, L.; Berbari, J.; Camden, C. Developing a web platform to support a community of practice: A mixed methods study in pediatric physiotherapy. J. Contin. Educ. Health Prof. 2018, 38, 19–24. [Google Scholar] [CrossRef]
- Rolls, K.D.; Hansen, M.M.; Jackson, D.; Elliott, D. Intensive care nurses on social media: An exploration of knowledge exchange on an intensive care virtual community of practice. J. Clin. Nurs. 2020, 29, 1381–1397. [Google Scholar] [CrossRef]
- Vinson, C.A. Using concept mapping to develop a conceptual framework for creating virtual communities of practice to translate cancer research into practice. Prev. Chronic Dis. 2014, 11, E68. [Google Scholar] [CrossRef][Green Version]
- Galheigo, S.M.; Braga, C.P.; Magalhães, L.; Kinsella, E.A. An occupational therapy community of practice within pediatric acute care: Fostering professional, social and cultural capital in resource challenged settings. Cad. Bras. Ter. Ocup. 2019, 27, 776–791. [Google Scholar] [CrossRef]
- Mayrhofer, A.; Goodman, C.; Holman, C. Establishing a community of practice for dementia champions (innovative practice). Dementia 2015, 14, 259–266. [Google Scholar] [CrossRef]
- Adedoyin, A.C.A. Deploying virtual communities of practice as a digital tool in social work: A rapid review and critique of the literature. Soc. Work Educ. 2016, 35, 357–370. [Google Scholar] [CrossRef]
- Ranmuthugala, G.; Cunningham, F.C.; Plumb, J.J.; Long, J.; Georgiou, A.; Westbrook, J.I.; Braithwaite, J. A realist evaluation of the role of communities of practice in changing healthcare practice. Implement. Sci. 2011, 6, 49. [Google Scholar] [CrossRef] [PubMed]
- Rolls, K.; Hansen, M.; Jackson, D.; Elliott, D. How health care professionals use social media to create virtual communities: An integrative review. J. Med. Internet Res. 2016, 18, e5312. [Google Scholar] [CrossRef] [PubMed]
- Lewis, H.; Becevic, M.; Myers, D.; Helming, D.; Mutrux, R.; Fleming, D.A.; Edison, K. Dermatology ECHO-an innovative solution to address limited access to dermatology expertise. Rural Remote Health 2018, 18, 4415. [Google Scholar] [CrossRef] [PubMed]
- Coleman, A. A virtual community of practice framework to support doctors’ practices in national health insurance (NHI) in South Africa. Stud. Ethno Med. 2012, 6, 155–160. [Google Scholar] [CrossRef][Green Version]
- Farrell, M.M.; La Porta, M.; Gallagher, A.; Vinson, C.; Bernal, S.B. Peer Reviewed: Research to Reality: Moving Evidence Into Practice Through an Online Community of Practice. Prev. Chronic Dis. 2014, 11, E78. [Google Scholar] [CrossRef]
- Alary Gauvreau, C.A.; Le Dorze, G.; Kairy, D.; Croteau, C. Evaluation of a community of practice for speech-language pathologists in aphasia rehabilitation: A logic analysis. BMC Health Serv. Res. 2019, 19, 530. [Google Scholar] [CrossRef]
- Dearing, J.W.; Greene, S.M.; Stewart, W.F.; Williams, A.E. If we only knew what we know: Principles for knowledge sharing across people, practices, and platforms. Transl. Behav. Med. 2011, 1, 15–25. [Google Scholar] [CrossRef]
- Friberger, M.G.; Falkman, G. Collaboration processes, outcomes, challenges and enablers of distributed clinical communities of practice. Behav. Inf. Technol. 2013, 32, 519–531. [Google Scholar] [CrossRef]
- Wolbrink, T.A.; Kissoon, N.; Mirza, N.; Burns, J.P. Building a global, online community of practice: The OPENPediatrics World Shared Practices Video Series. Acad. Med. 2017, 92, 676–679. [Google Scholar] [CrossRef]
- Lewis, L.A.; Koston, Z.; Quartley, M.; Adsit, J. Virtual communities of practice: Bridging research and practice using Web 2.0. J. Educ. Technol. Syst. 2010, 39, 155–161. [Google Scholar] [CrossRef]
- Abos Mendizabal, G.; Nuño Solinís, R.; Zaballa González, I. HOBE+, a case study: A virtual community of practice to support innovation in primary care in Basque Public Health Service. BMC Fam. Pract. 2013, 14, 168. [Google Scholar] [CrossRef]
- Landes, S.J.; Smith, B.N.; Weingardt, K.R. Supporting grass roots implementation of an evidence-based psychotherapy through a virtual community of practice: A case example in the Department of Veterans Affairs. Cogn. Behav. Pract. 2019, 26, 453–465. [Google Scholar] [CrossRef]
- Murad, A.; Hyde, N.; Chang, S.; Lederman, R.; Bosua, R.; Pirotta, M.; Audehm, R.; Yates, C.J.; Briggs, A.M.; Gorelik, A.; et al. Quantifying Use of a Health Virtual Community of Practice for General Practitioners’ Continuing Professional Development: A Novel Methodology and Pilot Evaluation. J. Med. Internet Res. 2019, 21, e14545. [Google Scholar] [CrossRef] [PubMed]
- Ting, D.K.; Thoma, B.; Luckett-Gatopoulos, S.; Thomas, A.; Syed, S.; Bravo, M.; Zaver, F.; Purdy, E.; Kwok, E.S.; Chan, T.M. Canadi EM: Accessing a virtual community of practice to create a canadian national medical education institution. AEM Educ. Train. 2019, 3, 86–91. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho-Filho, M.A.; Tio, R.A.; Steinert, Y. Twelve tips for implementing a community of practice for faculty development. Med. Teach. 2020, 42, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.; Korjonen, H.; Keswani, A.; Hughes, E. Virtual communities of practice: Can they support the prevention agenda in public health? Online J. Public Health Inform. 2015, 7, e222. [Google Scholar] [CrossRef]
- Littlewood, N.; Gordon, B.; Department of Health. Digital Health Capability Framework for Health Professionals; 1 Treasury Place: Melbourne, VIC, Australia, 2021. [Google Scholar]
- Australian Digital Health Agency. Australia’s National Digital Health Strategy. Available online: https://www.digitalhealth.gov.au/sites/default/files/2020-11/Australia%27s%20National%20Digital%20Health%20Strategy%20-%20Safe%2C%20seamless%20and%20secure.pdf (accessed on 26 May 2022).
- Australian Digital Health Agency. National Nursing and Midwifery Digital Health Capability Framework. 2020. Available online: https://www.digitalhealth.gov.au/sites/default/files/2020-11/National_Nursing_and_Midwifery_Digital_Health_Capability_Framework_publication.pdf (accessed on 26 May 2022).
- National Health Service. A Health and Digital Care Capabilities Framework. 2018. Available online: https://www.hee.nhs.uk/sites/default/files/documents/Digital%20Literacy%20Capability%20Framework%202018.pdf (accessed on 26 May 2022).
- Morris, M.E.; Webster, K.; Jones, C.; Hill, A.-M.; Haines, T.; McPhail, S.; Kiegaldie, D.; Slade, S.; Jazayeri, D.; Heng, H.; et al. Interventions to reduce falls in hospitals: A systematic review and meta-analysis. Age Ageing 2022, 51, afac077. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).