
Obesity and COVID-19 in Children and Adolescents: Reciprocal Detrimental Influence—Systematic Literature Review and Meta-Analysis

 ,
,  ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
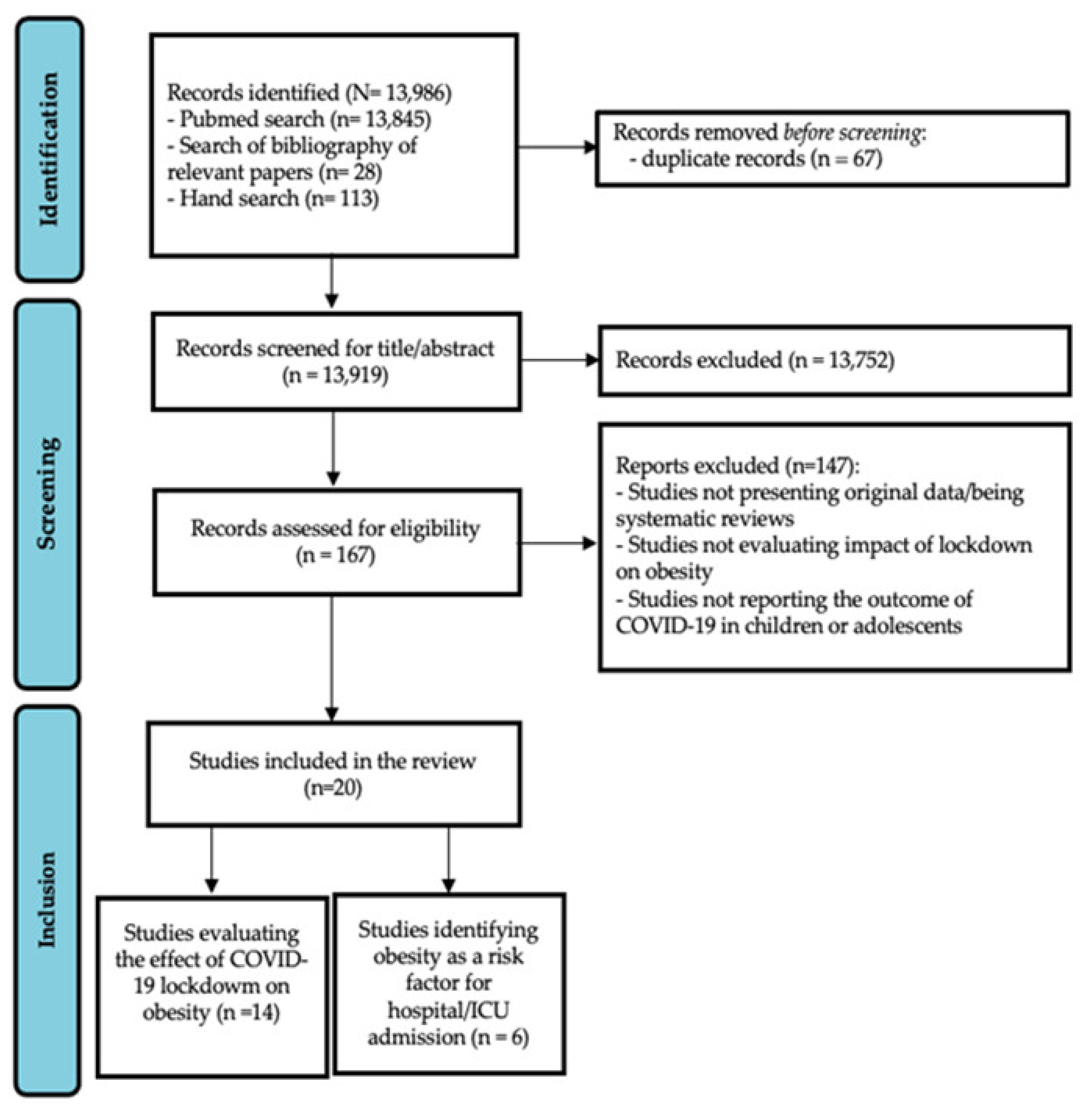
2. Materials and Methods
3. Results
3.1. Impact of COVID-19 Lockdown on Weight and Lifestyle in Children and Adolescents
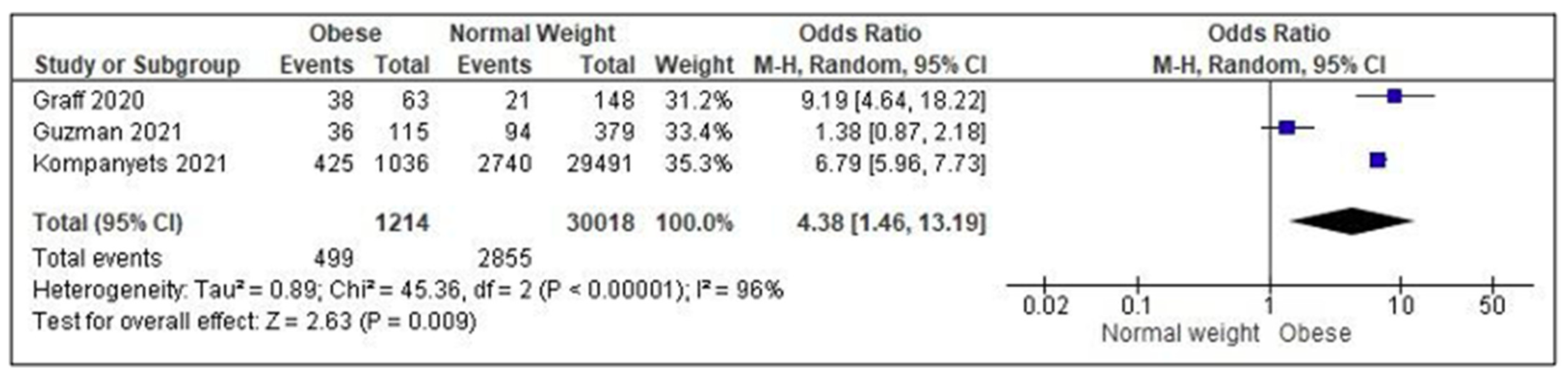
3.2. Impact of Overweight/Obesity on the Risk of Hospital/ICU Admission in Children/Adolescents with COVID-19
4. Discussion
4.1. Impact of COVID-19 Lockdown on Weight and Lifestyle Changes in Children and Adolescents
4.2. Impact of Overweight/Obesity on the Severity and Outcome of COVID-19 Disease
4.3. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Shih, T.-P.; Ko, W.-C.; Tang, H.-J.; Hsueh, P.-R. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Coronavirus Disease-2019 (COVID-19): The Epidemic and the Challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons Learnt from Easing COVID-19 Restrictions: An Analysis of Countries and Regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Chang, T.-H.; Chen, Y.-C.; Chen, W.-Y.; Chen, C.-Y.; Hsu, W.-Y.; Chou, Y.; Chang, Y.-H. Weight Gain Associated with COVID-19 Lockdown in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3668. [Google Scholar] [CrossRef]
- Bremner, J.D.; Moazzami, K.; Wittbrodt, M.T.; Nye, J.A.; Lima, B.B.; Gillespie, C.F.; Rapaport, M.H.; Pearce, B.D.; Shah, A.J.; Vaccarino, V. Diet, Stress and Mental Health. Nutrients 2020, 12, 2428. [Google Scholar] [CrossRef] [PubMed]
- Tester, J.M.; Rosas, L.G.; Leung, C.W. Food Insecurity and Pediatric Obesity: A Double Whammy in the Era of COVID-19. Curr. Obes. Rep. 2020, 9, 442–450. [Google Scholar] [CrossRef]
- Deal, B.J.; Huffman, M.D.; Binns, H.; Stone, N.J. Perspective: Childhood Obesity Requires New Strategies for Prevention. Adv. Nutr. 2020, 11, 1071–1078. [Google Scholar] [CrossRef]
- Statistics on Obesity, Physical Activity and Diet. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet (accessed on 22 March 2022).
- Khan, M.A.; Moverley Smith, J.E. “Covibesity”, a New Pandemic. Obes. Med. 2020, 19, 100282. [Google Scholar] [CrossRef]
- Frenkel, L.; Gomez, F.; Bellanti, J.A. COVID-19 in Children: Pathogenesis and Current Status. Allergy Asthma Proc. 2020, 42, 8–15. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and Diabetes as High-Risk Factors for Severe Coronavirus Disease 2019 (COVID-19). Diabetes Metab. Res. Rev. 2021, 37, e3377. [Google Scholar] [CrossRef] [PubMed]
- Caussy, C.; Wallet, F.; Laville, M.; Disse, E. Obesity Is Associated with Severe Forms of COVID-19. Obesity 2020, 28, 1175. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, S.M.; O’Rahilly, S. When Two Pandemics Meet: Why Is Obesity Associated with Increased COVID-19 Mortality? Med 2020, 1, 33–42. [Google Scholar] [CrossRef]
- Chen, Q.; Zheng, Z.; Zhang, C.; Zhang, X.; Wu, H.; Wang, J.; Wang, S.; Zheng, C. Clinical Characteristics of 145 Patients with Corona Virus Disease 2019 (COVID-19) in Taizhou, Zhejiang, China. Infection 2020, 48, 543–551. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors Associated with Hospital Admission and Critical Illness among 5279 People with Coronavirus Disease 2019 in New York City: Prospective Cohort Study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 22 March 2022).
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- RevMan 5 Download. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download (accessed on 22 March 2022).
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef]
- Azoulay, E.; Yackobovitch-Gavan, M.; Yaacov, H.; Gilboa, I.; Lopez, A.; Sheppes, T.; Waksman, Y.; Lebenthal, Y.; Brener, A. Weight Status and Body Composition Dynamics in Children and Adolescents During the COVID-19 Pandemic. Front. Pediatr. 2021, 9, 707773. [Google Scholar] [CrossRef]
- Brooks, C.G.; Spencer, J.R.; Sprafka, J.M.; Roehl, K.A.; Ma, J.; Londhe, A.A.; He, F.; Cheng, A.; Brown, C.A.; Page, J. Pediatric BMI Changes during COVID-19 Pandemic: An Electronic Health Record-Based Retrospective Cohort Study. EClinicalMedicine 2021, 38, 101026. [Google Scholar] [CrossRef]
- Cipolla, C.; Curatola, A.; Ferretti, S.; Giugno, G.; Condemi, C.; Delogu, A.B.; Birritella, L.; Lazzareschi, I. Eating Habits and Lifestyle in Children with Obesity during the COVID19 Lockdown: A Survey in an Italian Center. Acta Biomed. 2021, 92, e2021196. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Liu, J.; Wang, J.; Shen, M.; Ge, W.; Shen, H.; Zhang, T.; Yang, H.; Yin, J. Unfavorable Progression of Obesity in Children and Adolescents Due to COVID-19 Pandemic: A School-Based Survey in China. Obesity 2021, 29, 1907–1915. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Zhang, L.; Yu, W.; Yu, B.; Liu, M.; Zhang, D.; Yang, S. Impact of COVID-19 Lockdown on Activity Patterns and Weight Status among Youths in China: The COVID-19 Impact on Lifestyle Change Survey (COINLICS). Int. J. Obes. 2021, 45, 695–699. [Google Scholar] [CrossRef]
- Kang, H.M.; Jeong, D.C.; Suh, B.K.; Ahn, M.B. The Impact of the Coronavirus Disease-2019 Pandemic on Childhood Obesity and Vitamin D Status. J. Korean Med. Sci. 2021, 36, e21. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Kwon, Y.; Choe, Y.H.; Kim, M.J. COVID-19-Related School Closing Aggravate Obesity and Glucose Intolerance in Pediatric Patients with Obesity. Sci. Rep. 2021, 11, 5494. [Google Scholar] [CrossRef] [PubMed]
- Maltoni, G.; Zioutas, M.; Deiana, G.; Biserni, G.B.; Pession, A.; Zucchini, S. Gender Differences in Weight Gain during Lockdown Due to COVID-19 Pandemic in Adolescents with Obesity. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2181–2185. [Google Scholar] [CrossRef]
- Qiu, N.; He, H.; Qiao, L.; Ding, Y.; Ji, S.; Guo, X.; Luo, J.; Luo, Z.; Li, Y.; Pang, H.; et al. Sex Differences in Changes in BMI and Blood Pressure in Chinese School-Aged Children during the COVID-19 Quarantine. Int. J. Obes. 2021, 45, 2132–2136. [Google Scholar] [CrossRef]
- Valenzise, M.; D’Amico, F.; Cucinotta, U.; Lugarà, C.; Zirilli, G.; Zema, A.; Wasniewska, M.; Pajno, G.B. The Lockdown Effects on a Pediatric Obese Population in the COVID-19 Era. Ital. J. Pediatr. 2021, 47, 209. [Google Scholar] [CrossRef]
- Vinker-Shuster, M.; Grossman, E.S.; Yeshayahu, Y. Increased Weight Gain of Children during the COVID-19 Lockdown. Isr. Med. Assoc. J. 2021, 23, 219–222. [Google Scholar]
- Vogel, M.; Geserick, M.; Gausche, R.; Beger, C.; Poulain, T.; Meigen, C.; Körner, A.; Keller, E.; Kiess, W.; Pfäffle, R. Age- and Weight Group-Specific Weight Gain Patterns in Children and Adolescents during the 15 Years before and during the COVID-19 Pandemic. Int. J. Obes. 2022, 46, 144–152. [Google Scholar] [CrossRef]
- Woolford, S.J.; Sidell, M.; Li, X.; Else, V.; Young, D.R.; Resnicow, K.; Koebnick, C. Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic. JAMA 2021, 326, 1434–1436. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, D.M.; Oliveira, C.R.; Guerguis, S.; Eisenberg, R.; Choi, J.; Kim, M.; Abdelhemid, A.; Agha, R.; Agarwal, S.; Aschner, J.L.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 Clinical Syndromes and Predictors of Disease Severity in Hospitalized Children and Youth. J. Pediatr. 2021, 230, 23–31.e10. [Google Scholar] [CrossRef] [PubMed]
- Graff, K.; Smith, C.; Silveira, L.; Jung, S.; Curran-Hays, S.; Jarjour, J.; Carpenter, L.; Pickard, K.; Mattiucci, M.; Fresia, J.; et al. Risk Factors for Severe COVID-19 in Children. Pediatr. Infect. Dis. J. 2021, 40, e137–e145. [Google Scholar] [CrossRef] [PubMed]
- Guzman, B.V.; Elbel, B.; Jay, M.; Messito, M.J.; Curado, S. Age-Dependent Association of Obesity with COVID-19 Severity in Paediatric Patients. Pediatr. Obes. 2022, 17, e12856. [Google Scholar] [CrossRef]
- Kompaniyets, L.; Agathis, N.T.; Nelson, J.M.; Preston, L.E.; Ko, J.Y.; Belay, B.; Pennington, A.F.; Danielson, M.L.; DeSisto, C.L.; Chevinsky, J.R.; et al. Underlying Medical Conditions Associated With Severe COVID-19 Illness Among Children. JAMA Netw. Open 2021, 4, e2111182. [Google Scholar] [CrossRef]
- Swann, O.V.; Holden, K.A.; Turtle, L.; Pollock, L.; Fairfield, C.J.; Drake, T.M.; Seth, S.; Egan, C.; Hardwick, H.E.; Halpin, S.; et al. Clinical Characteristics of Children and Young People Admitted to Hospital with COVID-19 in United Kingdom: Prospective Multicentre Observational Cohort Study. BMJ 2020, 370, m3249. [Google Scholar] [CrossRef]
- Verma, S.; Lumba, R.; Dapul, H.M.; Gold-von Simson, G.; Phoon, C.K.; Lighter, J.L.; Farkas, J.S.; Vinci, A.; Noor, A.; Raabe, V.N.; et al. Characteristics of Hospitalized Children With SARS-CoV-2 in the New York City Metropolitan Area. Hosp. Pediatr. 2021, 11, 71–78. [Google Scholar] [CrossRef]
- Singer, M.; Bulled, N.; Ostrach, B.; Mendenhall, E. Syndemics and the Biosocial Conception of Health. Lancet 2017, 389, 941–950. [Google Scholar] [CrossRef]
- Horton, R. Offline: COVID-19 Is Not a Pandemic. Lancet 2020, 396, 874. [Google Scholar] [CrossRef]
- CDC. BMI for Children and Teens. Available online: https://www.cdc.gov/obesity/basics/childhood-defining.html (accessed on 11 May 2022).
- Djalalinia, S.; Qorbani, M.; Peykari, N.; Kelishadi, R. Health Impacts of Obesity. Pak. J. Med. Sci. 2015, 31, 239–242. [Google Scholar] [CrossRef]
- Scott, K.M.; Bruffaerts, R.; Simon, G.E.; Alonso, J.; Angermeyer, M.; de Girolamo, G.; Demyttenaere, K.; Gasquet, I.; Haro, J.M.; Karam, E.; et al. Obesity and Mental Disorders in the General Population: Results from the World Mental Health Surveys. Int. J. Obes. 2008, 32, 192–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey-López, J.P.; Vicente-Rodríguez, G.; Biosca, M.; Moreno, L.A. Sedentary Behaviour and Obesity Development in Children and Adolescents. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, R. Childhood Overweight, Obesity, and the Metabolic Syndrome in Developing Countries. Epidemiol. Rev. 2007, 29, 62–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leproult, R.; Van Cauter, E. Role of Sleep and Sleep Loss in Hormonal Release and Metabolism. Endocr. Dev. 2010, 17, 11–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancuso, P. Obesity and Respiratory Infections: Does Excess Adiposity Weigh down Host Defense? Pulm. Pharm. 2013, 26, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B.; Burke, P.J.; Lewandowski, L. When Pandemics Collide: The Impact of COVID-19 on Childhood Obesity. J. Pediatr. Nurs. 2021, 56, 90–98. [Google Scholar] [CrossRef]
- Doom, J.R.; Lumeng, J.C.; Sturza, J.; Kaciroti, N.; Vazquez, D.M.; Miller, A.L. Longitudinal Associations between Overweight/Obesity and Stress Biology in Low-Income Children. Int. J. Obes. 2020, 44, 646–655. [Google Scholar] [CrossRef]
- de Figueiredo, C.S.; Sandre, P.C.; Portugal, L.C.L.; Mázala-de-Oliveira, T.; da Silva Chagas, L.; Raony, Í.; Ferreira, E.S.; Giestal-de-Araujo, E.; Dos Santos, A.A.; Bomfim, P.O.-S. COVID-19 Pandemic Impact on Children and Adolescents’ Mental Health: Biological, Environmental, and Social Factors. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 106, 110171. [Google Scholar] [CrossRef]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and Lockdown on Mental Health of Children and Adolescents: A Narrative Review with Recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Annunziata, G.; Di Somma, C.; Laudisio, D.; Colao, A.; Savastano, S. Obesity and Sleep Disturbance: The Chicken or the Egg? Crit. Rev. Food Sci. Nutr. 2019, 59, 2158–2165. [Google Scholar] [CrossRef]
- Moreno, J.P.; Johnston, C.A.; Chen, T.-A.; O’Connor, T.A.; Hughes, S.O.; Baranowski, J.; Woehler, D.; Baranowski, T. Seasonal Variability in Weight Change during Elementary School. Obesity 2015, 23, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19-Related School Closings and Risk of Weight Gain Among Children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Irfan, O.; Muttalib, F.; Tang, K.; Jiang, L.; Lassi, Z.S.; Bhutta, Z. Clinical Characteristics, Treatment and Outcomes of Paediatric COVID-19: A Systematic Review and Meta-Analysis. Arch. Dis. Child. 2021, 106, 440–448. [Google Scholar] [CrossRef]
- Harman, K.; Verma, A.; Cook, J.; Radia, T.; Zuckerman, M.; Deep, A.; Dhawan, A.; Gupta, A. Ethnicity and COVID-19 in Children with Comorbidities. Lancet Child. Adolesc. Health 2020, 4, e24–e25. [Google Scholar] [CrossRef]
- Tsankov, B.K.; Allaire, J.M.; Irvine, M.A.; Lopez, A.A.; Sauvé, L.J.; Vallance, B.A.; Jacobson, K. Severe COVID-19 Infection and Pediatric Comorbidities: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 103, 246–256. [Google Scholar] [CrossRef]
- Nogueira-de-Almeida, C.A.; Del Ciampo, L.A.; Ferraz, I.S.; Del Ciampo, I.R.L.; Contini, A.A.; Ued, F.D.V. COVID-19 and Obesity in Childhood and Adolescence: A Clinical Review. J. Pediatr. 2020, 96, 546–558. [Google Scholar] [CrossRef]
- Cena, H.; Fiechtner, L.; Vincenti, A.; Magenes, V.C.; De Giuseppe, R.; Manuelli, M.; Zuccotti, G.V.; Calcaterra, V. COVID-19 Pandemic as Risk Factors for Excessive Weight Gain in Pediatrics: The Role of Changes in Nutrition Behavior. A Narrative Review. Nutrients 2021, 13, 4255. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author, Year | Country | Study Period (Months) | Study Design | N | Males (N, %) | Population | Age (Mean ± SD; Range) | Setting | Weight Measure | Weight Status Before Lockdown | Weight Status After Lockdown | Change in Weight Status | Change in Eating Habits | Decrease in Physical Activity (PA) | Sleep Changes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Androutsos O. et al., 2021 [21] | Greece | 2 | CSS | 397 | 228 (57.4) | C, A | 7.8 ± 4.1 * | O | BW | 32.3 ± 16.9 * | n.a. | stable BW: N = 214 (58.9%); BW increase: N = 127 (35%); BW decrease: N = 22 (6.1%) | Increase in fresh fruit juices, vegetables, dairy products, pasta, sweets, snacks and breakfast | N = 261 (66.9%) | Increased sleep time (h/d). BL: >10 h/d = 13.3%, <8 h/d = 15.4% vs. AL: >10 h/d = 24.2%, <8 h/d = 4.8% |
| Azoulay E. et al., 2021 [22] | Israel | 7 | LS | 220 | 109 (49.5) | C, A | 10.8 ± 3.2 * | H | BMI-SDS | BMI-SDS: 1.74 (1.40, 2.03) ** | BMI-SDS: 1.70 (1.36, 1.97) ** | MFR increase in underweight (p = 0.05) and normal weight (p = 0.008), but not in overweight/obese patients. Associations in BMI z-scores (r = 0.961, p < 0.001) and MFR z-scores (r = 0.854, p < 0.001) before and during the pandemic. A multivariate linear regression model identified socioeconomic position, pre-pandemic BMI and MFR z-scores, and physical activity levels during the pandemic as predictors for delta MFR z-scores (F = 12.267, p < 0.001) | n.a. | n.a. | n.a. |
| Brooks C.G. et al., 2021 [23] | USA | 12 | HC | 96,501 | n.a. | C, A | 6–17 | H | BMI-SDS | 0.31 (0.29, 0.32) ** | 0.62 (0.59, 0.64) ** | Overall increased BMI-SDS: 0.30 (0.27–0.33) *. (In obese C AL: 1.16 (1.07–1.24) ** vs. BL: 0.56 (0.52–0.61) **; Hispanic C AL: 0.93 (0.84–1.02) ** vs. BL: 0.41 (0.36–0.46) **; C lacking commercial insurance AL: 0.88 (0.81, 0.95) ** vs.BL: 0.43 (0.39, 0.47) **; DBMI higher in boys vs. girls (0.36 vs. 0.24) | n.a. | n.a. | n.a. |
| Cipolla C. et al., 2021 [24] | Italy | 1 | CSS | 64 | 26 (40.6) | C, A | 13.9 ± 2.4 * | H | BMI | 27.7 ± 4.8 * | 27.6 ± 4.0 * | BMI increase: N = 31 (48.4%); BMI decrease: N = 33 (51.6%) | Increase in bread/pasta/pizza (N = 43; 67.2%); desserts (N = 3; 4.7%), meat (N = 8; 12.5); vegetables/fruit (N = 10; 15.6%); sugar drinks (N = 20; 31.2%) | Higher BMI increase in sedentary patients (p = 0.024) and in those spending longer time at videogaming (p = 0.005) | n.a. |
| Hu J. et al., 2021 [25] | China | 12 | HC | 207,536 | n.a | C, A | 6–17 | H | zBMI | 0.29 ± 0.01 * | 0.45 ± 0.01 * | Increase of zBMI and OB in 2020 vs. 2014–2019 in all age groups, but significant only for ages 6–11 and 15–16. zBMI increase in boys (0.18) higher than in girls (0.13, p = 0.014). Similar rise in urban and rural areas | n.a. | n.a. | n.a. |
| Jia P. et al., 2020 [26] | China | 1 | CSS | 2824 | 678 (24.0) | A | 17.5 ± 1.2 * | S | BW; BMI | BW: 58.6 ± 17.1 * BMI: 22.7 ± 6.7 * | BW: 60.2 ± 22.9 *; BMI: 23.6 ± 8.6 * | Increase in mean BMI and BW | n.a. | Decrease in moderate-/vigorous-intensity PA: 0.5 ± 1.7 * vs. 0.4 ± 1.7 * d/w | Increase in sleeping time: sleep (h/d): 7.5 ± 3.2 * vs. 7.7 ± 4.7 * (workdays); 8.0 ± 3.4 * vs. 8.2 ± 5.4 * (weekends) |
| Kang H.M. et al., 2021 [27] | South Korea | 6 | HC | 226 | 96 (42.5) | C, A | 10.5 (8.7–12.4) ** | H | zBMI | 0.4 ± 1.3 * | 0.2 ± 1.3 * | OW/OB: 31.4 vs. 23.9 % (p = 0.074); increase from NW to OW/OB: 9.5%. Mean zBMI 0.42 ± 1.25 vs. 0.2 ± 1.25 (p < 0.001) Days after school closure (p = 0.004) and normoweight (p = 0.017) pre-COVID were negative predictors | n.a. | n.a. | n.a. |
| Kim E.S. et al., 2021 [28] | South Korea | 6 | HC | 90 | 70 (77.8) | C, A | 12.2 ± 3.4 * | H | BW; zBW; BMI; zBMI | BW: 67.2 ± 23.8 *; zBW: 2.0 ± 0.8 *; BMI: 26.7 ± 4.6 *; zBMI: 1.9 ± 0.5 * | BW: 71.1 ± 24.2 *; zBW: 2.2 ± 0.7 *; BMI: 27.7 ± 4.6 *; zBMI: 2.0 ± 0.4 * | △zBW: 0.18 (0.1–0.29) **; △zBMI 0.06 (0–0.12) ** | n.a. | yes | n.a. |
| Maltoni G. et al., 2021 [29] | Italy | 3 | LS | 51 | 31 (60.8) | C, A | 14.7 ± 2.1 * | H | BW; BMI; BMI SDS; WC; W/H-r | BMI: 32.6 ± 4.0 *; BMI SDS: 2.4 ± 0.5 *; WC: 102.1 ± 12.6 *; W/H-r: 0.6 ± 0.1 * | n.a. | △BW: 2.8 ± 3.7 *; Δ-BMI: 0.5 ± 1.3 *; Δ-BMI SDS: 0.1 ± 0.2 *; ΔWC.: 4.4 ± 7.8 *; ΔW/H-r: 0.02 ± 0.005 * △BW: M 3.8 ± 3.4 vs. F 1.2 ± 3.7 (p = 0.02) Δsedentary behavior: M3.8 ± 2.7 vs. F 1.5 ± 2.5 (p = 0.003) | Δ-intake of vegetables/fruit: −0.1 ± 0.5 * (portions/w) | yes | n.a. |
| Qiu N. et al., 2021 [30] | China | 7 | LS | 446 | 260 (58.2) | C | 7–12 | S | Median BMI | 20.9 kg/m2 | 22.4 kg/m2 | Increase from NW to OW/OB in 28.1%; from OW to OB in 42.42%. Boys at significantly higher risk | Increased number of meals, higher in parents with primary school vs. high school diploma (6 ± 0.7 vs. 4.4 ± 1.3, p = 0.02) | n.a. | n.a. |
| Valenzise M. et al., 2021 [31] | Italy | 12 | HC | 40 | 23 (57.5) | C, A | 11.6 ± 3.3 * | O | Δ-BMI | 30.2 ± 4.0 * | 32.0 ± 5.5 * | BMI increase (32 ± 5.5 vs. 30.2 ± 4) not significant | n.a. | N = 38 (95%) | n.a. |
| Vinker-Shuster M. et al., 2021 [32] | Israel | 1 | HC | 229 | 117 (51.1) | C, A | 0–6 y: N = 60 6–18 y: N = 169 | H | aaBWp | 38.8 ± 33.7 * | 40.4 ± 34.4 * | Overall increase of weight percentile (40.4 vs. 38.8, p = 0.03) higher in boys (37.7 vs. 34.4, p = 0.01) vs girls (no significant changes), and in patients < 6 yo (39.2 vs. 33.6, p = 0.02) | n.a. | n.a. | n.a. |
| Vogel M. et al., 2021 [33] | Germany | 12 | HC | 274,456 | n.a | C, A | 6–18 | H | ΔBMI-SDS | 0.001 (0.001, 0.002) ** | 0.048 (0.039, 0.056) ** | BMI-SDS increase over 3-month AL 1.38 (95% CI 1.30–1.47; p < 0.001), >30 times as high as for years 2005–2019. Highest effects in OB group (OR 1.85; 95% CI 1.45–2.35; p < 0.001), in all ages | n.a. | n.a. | n.a. |
| Woolford S. et al. [34] | USA | 1 | HC | 191,509 | n.a | C, A | 5–17 | H | ΔBMI-SD | 5–11 y: 0.15 (0.11–0.18) **; 12–15 y: −0.03 (−0.07–0.00) **; 16–17 y: −0.25 (−0.30–−0.21) ** | 5–11 y: 1.72 (1.67–1.76) **; 12–15 y: 0.87 (0.83– 0.91) **; 16–17 y: 0.23 (0.18–0.28) ** | Increase in ΔBMI-SD especially for age 5–11 yo (1.57) vs. 12–15 yo (0.91) vs. 16–17 yo (0.48). OW/OB increase 8.7% (45.7 vs. 36.2%) for age 5–11 yo vs. 5.2% for age 12–15 yo vs. 3.1% for age 16–17 yo | n.a. | n.a. | n.a. |
| Author | Country | Study Design | Age * (Mean; Range; yr) | N | Males (N, %) | Population | N Obese (%) | Obese Hospitalized/Admitted to ICU (N, %) | Normal Weight Hospitalized/Admitted to ICU (N, %) | Risk Factor and Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Fernandes D.M. et al., 2020 [35] | US | HC; LS | 10 (1–17) | 250 * | 170 (60.5) | C, A | 85 (34.0) | 85 (100) | 165 (100) | Obesity (aOR 3.39, 95% CI 1.26–9.10) severe disease |
| Graff K. et al., 2021 [36] | US | HC | 11 (0–23) | 211 * | 262 (57.7) | C, A | 63 (29.9) | 38 (60.3) | 21 (14.2) | Obesity (OR 2.48; 95% CI 1.2–5.1), and severe obesity (OR 4.8; CI 1.9–12.1) hospital admission |
| Guzman et al., 2021 [37] | US | HC | 0–21 | 494 | 203 (45.6) | C, A | 115 (23.3) | 36 (31.3) | 94 (24.8) | Obesity (ARR 2.02, 95% CI 1.17–3.48) critical illness. Higher risk for age 13–21 yo [ARR 3.09, 95% CI 1.48–6.47] |
| Kompanyets et al., 2021 [38] | US | CSS | 6–18 | 30,527 * | 15.974 (50.2) | C, A | 1036 (29.4) | 425 (41.0) | 2740 (9.3) | Type 1 diabetes (aRR 4.60, 95% CI, 3.91–5.42) and obesity (aRR 3.07, 95% CI, 2.66–3.54) hospitalization |
| Swann O.V. et al., 2020 [39] | UK | LS | 4.6 (0.3–13.7) | 602 * | 367 (56.0) | C, A | 17 (2.8) | 17 (100) | 585 (100) | age < 1 m (OR 3.21, 95% CI 1.36–7.66), age 10–14 yo (OR 3.23, 95% CI 1.55–6.99), and black ethnicity (OR 2.82, 95% CI 1.41–5.57) admission to critical care |
| Verma S. et al., 2021 [40] | US | CSS | 5 (0.2–15.2) | 48 * | 52 (63.0) | C, A | 19 (39.6) | 19 (100) | 29 (100) | Obesity ICU admission (63 vs. 28% normal weight, p = 0.02) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Fauci, G.; Montalti, M.; Di Valerio, Z.; Gori, D.; Salomoni, M.G.; Salussolia, A.; Soldà, G.; Guaraldi, F. Obesity and COVID-19 in Children and Adolescents: Reciprocal Detrimental Influence—Systematic Literature Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 7603. https://doi.org/10.3390/ijerph19137603
La Fauci G, Montalti M, Di Valerio Z, Gori D, Salomoni MG, Salussolia A, Soldà G, Guaraldi F. Obesity and COVID-19 in Children and Adolescents: Reciprocal Detrimental Influence—Systematic Literature Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(13):7603. https://doi.org/10.3390/ijerph19137603
Chicago/Turabian StyleLa Fauci, Giusy, Marco Montalti, Zeno Di Valerio, Davide Gori, Maria Giulia Salomoni, Aurelia Salussolia, Giorgia Soldà, and Federica Guaraldi. 2022. "Obesity and COVID-19 in Children and Adolescents: Reciprocal Detrimental Influence—Systematic Literature Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 13: 7603. https://doi.org/10.3390/ijerph19137603
APA StyleLa Fauci, G., Montalti, M., Di Valerio, Z., Gori, D., Salomoni, M. G., Salussolia, A., Soldà, G., & Guaraldi, F. (2022). Obesity and COVID-19 in Children and Adolescents: Reciprocal Detrimental Influence—Systematic Literature Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(13), 7603. https://doi.org/10.3390/ijerph19137603