
Research on the Relationship between Chinese Elderly Health Status, Social Security, and Depression


Abstract
:1. Introduction
2. Materials and Methods
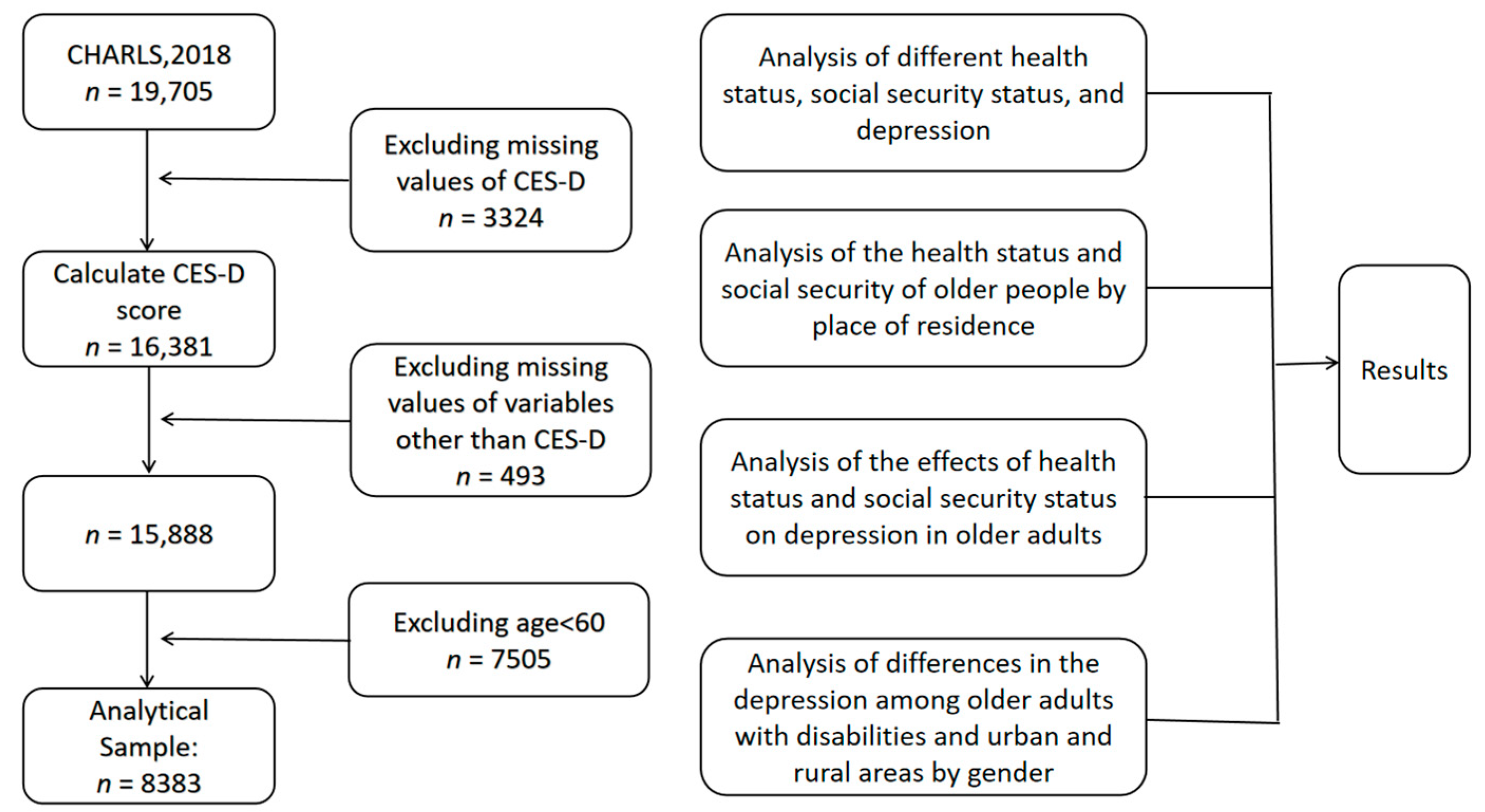
2.1. Data Source
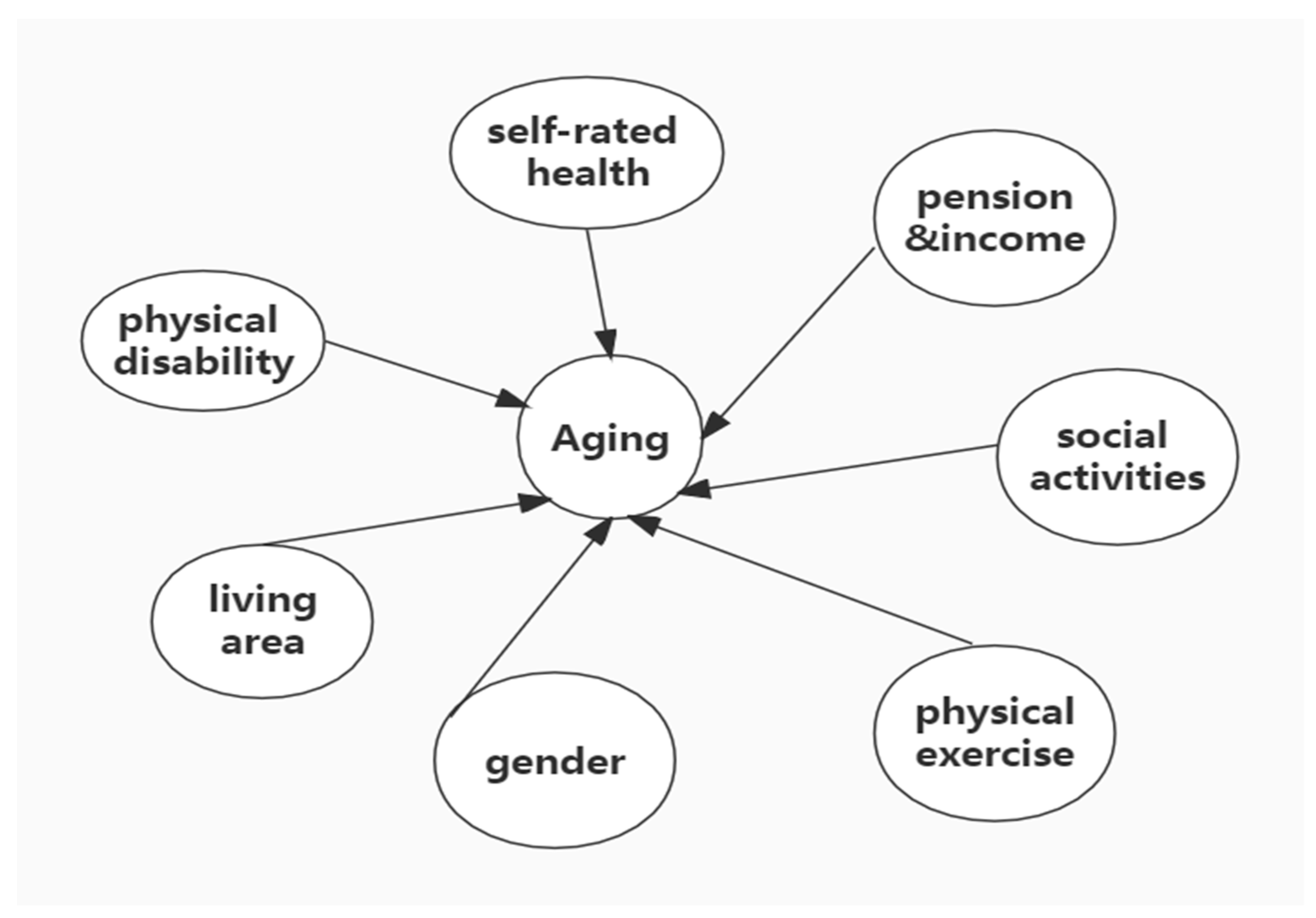
2.2. Research Content
2.3. Statistical Methods
3. Results
3.1. Analysis of the Essential Characteristics of the Elderly with Different Depression Statuses
3.2. Analysis of the Health Status and Social Security of the Elderly in Different Places of Residence
3.3. The Impact of Health Status and Social Security Status on Depression in the Elderly
3.4. Comparison of Depression among Older Persons by Gender
4. Discussion
5. Challenges
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peteet, J.R. Spirituality and mental health: Implications for ethics, medicine, and public health. Ethics Med. Public Health 2019, 9, 75–79. [Google Scholar] [CrossRef]
- Xie, L.; Shen, Y.; Wu, Y.; Yang, H. The impact of retirement on mental health. Int. J. Health Plann. Manag. 2021, 36, 1697–1713. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Q.; Chen, P.J. Population ageing challenges health care in China. Lancet 2014, 383, 870. [Google Scholar] [CrossRef]
- Feng, Z.; Liu, C.; Guan, X.; Mor, V. China’s rapidly aging population creates policy challenges in shaping a viable long-term care system. Health Aff. 2012, 31, 2764–2773. [Google Scholar] [CrossRef]
- Donohue, J.M.; Pincus, H.A. Reducing the societal burden of depression: A review of economic costs, quality of care and effects of treatment. Pharmacoeconomics 2007, 25, 7–24. [Google Scholar] [CrossRef]
- Sun, R.J. Worry about medical care, family support, and depression of the elders in urban China. Res. Aging 2004, 26, 559–585. [Google Scholar] [CrossRef] [Green Version]
- Ningling, S.; Luyan, W. The relevance of mental and physical sub-health status. Int. J. Cardiol. 2011, 152, S93–S94. [Google Scholar]
- Karam, G.E. Geriatric depression: A brief review. J. Med. Liban 2012, 60, 200–206. [Google Scholar]
- Chiao, C.; Weng, L.J.; Botticello, A.L. Social participation reduces depressive symptoms among older adults: An 18-year longitudinal analysis in taiwan. BMC Public Health 2011, 11, 292. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Xiao, Z.; Xiao, S. Suicide among the elderly in mainland china. Psychogeriatrics 2009, 9, 62–66. [Google Scholar] [CrossRef]
- Li, M.Z.; Katikireddi, S.V. Urban-rural inequalities in suicide among elderly people in china: A systematic review and meta-analysis. Int. J. Equity Health 2019, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Romero, R.; Herranz-Rodriguez, C.; Kostov, B.; Gene-Badia, J.; Siso-Almirall, A. Intervention to reduce perceived loneliness in community-dwelling older people. Scand. J. Caring Sci. 2021, 35, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.X.; Zhang, Q.; Li, C.X.; Lin, J.T. Prevalence of and risk factors for asthma among people aged 45 and older in china: A cross-sectional study. BMC Pulm. Med. 2021, 21, 407–418. [Google Scholar] [CrossRef]
- Su, D.; Chen, Z.; Chang, J.; Gong, G.; Guo, D.; Tan, M.; Zhang, Y.; Liu, Y.; Chen, X.; Chen, X.; et al. Effect of social participation on the physical functioning and depression of empty-nest elderly in China: Evidence from the china health and retirement longitudinal survey (charls). Int. J. Environ. Res. Public Health 2020, 17, 9438. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Gong, L.; Chen, F.; Sun, D.; Dong, Y.; Wang, X.; Kang, Q.; Chen, J. Logistic regression analysis of self-evaluated health status of rural residents in gaoyou. Chongqing Med. 2013, 42, 54–56. [Google Scholar]
- Cislaghi, B.; Cislaghi, C. Self-rated health as a valid indicator for health-equity analyses: Evidence from the italian health interview survey. BMC Public Heath 2019, 19, 533. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, P.; Nunez, A.; Merz, E.; Brintz, C.; Weitzman, O.; Navas, E.L.; Camacho, A.; Buelna, C.; Penedo, F.J.; Wassertheil-Smoller, S.; et al. Measurement properties of the center for epidemiologic studies depression scale (ces-d 10): Findings from hchs/sol. Psychol. Assess. 2017, 29, 372–381. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y. Intergenerational differences in age-friendly environments and health outcomes: Social support as a mediator. J. Intergener. Relatsh. 2021, 19, 124–143. [Google Scholar] [CrossRef]
- Peng, R. Impact of medical and pension insurance on the long-term care expenses for the chinese disabled elderly: An empirical analysis based on clhls data. Chin. J. Health Policy 2017, 10, 46–51. [Google Scholar]
- Battaglia, G.; Bellafiore, M.; Alesi, M.; Paoli, A.; Bianco, A.; Palma, A. Effects of an adapted physical activity program on psychophysical health in elderly women. Clin. Interv. Aging 2016, 11, 1009–1015. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.; Polman, E. Is it me or her? How gender composition evokes interpersonally sensitive behavior on collaborative cross-boundary projects. Organ. Sci. 2015, 26, 334–355. [Google Scholar] [CrossRef] [Green Version]
- Nolen-Hoeksema, S. Emotion regulation and psychopathology: The role of gender. Annu. Rev. Clin. Psychol. 2012, 8, 161–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Dauwan, M.; Begemann, M.J.H.; Slot, M.I.E.; Lee, E.H.M.; Scheltens, P.; Sommer, I.E.C. Physical exercise improves quality of life, depressive symptoms, and cognition across chronic brain disorders: A transdiagnostic systematic review and meta-analysis of randomized controlled trials. J. Neurol. 2021, 268, 1222–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohrnberger, J.; Fichera, E.; Sutton, M. The relationship between physical and mental health: A mediation analysis. Soc. Sci. Med. 2017, 195, 42–49. [Google Scholar] [CrossRef]
- Bayliss, M.; Rendas-Baum, R.; White, M.K.; Maruish, M.; Bjorner, J.; Tunis, S.L. Health-related quality of life (hrql) for individuals with self-reported chronic physical and/or mental health conditions: Panel survey of an adult sample in the united states. Health Qual. Life Out. 2012, 10, 154. [Google Scholar] [CrossRef] [Green Version]
- Lenze, E.J.; Rogers, J.C.; Martire, L.M.; Mulsant, B.H.; Rollman, B.L.; Dew, M.A.; Schulz, R.; Reynolds, C.F., 3rd. The association of late-life depression and anxiety with physical disability: A review of the literature and prospectus for future research. Am. J. Geriatr. Psychiatry 2001, 9, 113–135. [Google Scholar] [CrossRef]
- Han, E.J.; Lee, J.; Cho, E.; Kim, H. Socioeconomic costs of dementia based on utilization of health care and long-term-care services: A retrospective cohort study. Int. J. Environ. Res. Public Health 2021, 18, 376. [Google Scholar] [CrossRef]
- Chen, X.; Wang, T.; Busch, S.H. Does money relieve depression? Evidence from social pension expansions in China. Soc. Sci. Med. 2019, 220, 411–420. [Google Scholar] [CrossRef]
- Walker, A.K.; Kavelaars, A.; Heijnen, C.J.; Dantzer, R. Neuroinflammation and comorbidity of pain and depression. Pharmacol. Rev. 2014, 66, 80–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarbrink, K.; Ni, G.; Sonnergren, H.; Schmidtchen, A.; Pang, C.; Bajpai, R.; Car, J. The humanistic and economic burden of chronic wounds: A protocol for a systematic review. Syst. Rev. 2017, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The meaning of “aging in place” to older people. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, J.; Pybis, J.; Bacon, J. Counselling in the third sector: To what extent are older adults accessing these services and how complete are the data third sector services collect measuring client psychological distress? Couns. Psychother. Res. 2021, 21, 382–392. [Google Scholar] [CrossRef]
- Wang, G.Y.; Zhang, X.J.; Wang, K.; Li, Y.H.; Shen, Q.; Ge, X.J.; Hang, W. Loneliness among the rural older people in anhui, china: Prevalence and associated factors. Int. J. Geriatr. Psych. 2011, 26, 1162–1168. [Google Scholar] [CrossRef]
- Sarla, E.; Lambrinou, E.; Galanis, P.; Kalokairinou, A.; Sourtzi, P. Factors that influence the relationship between social support and health-related quality of life of older people living in the community. Gerontol. Geriatr. Med. 2020, 6, 2333721420911474. [Google Scholar] [CrossRef] [Green Version]
- Quinn, K.M.; Laidlaw, K.; Murray, L.K. Older peoples’ attitudes to mental illness. Clin. Psychol. Psychother. 2009, 16, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Xie, H.; Wang, G.; Hu, Q.; Jia, J.; Ji, X.; Jiang, W. The effects of family-centered collaborative care on family burden and social support for caregivers of patients with depression. Chin. J. Nurs. 2018, 53, 662–667. [Google Scholar]
- Chou, K.L.; Chi, I. Social support exchange among elderly chinese people and their family members in hong kong: A longitudinal study. Int. J. Aging. Hum. Dev. 2001, 53, 329–346. [Google Scholar] [CrossRef]
- Sun, J.; Hao, X.; Bo, T. Analysis of the status quo and needs of community care for disabled elderly in beijing. Chin. J. Health Policy 2016, 9, 57–64. [Google Scholar]
- Chin, C.W.W.; Phua, K.-H. Long-term care policy: Singapore’s experience. J. Aging Soc. Policy 2016, 28, 113–129. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Total | Healthy | Depressive | p | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Age | 3.363 | 0.186 | |||
| 60–70 | 5435 (64.83) | 3588 (66.02) | 1847 (33.98) | ||
| 70–80 | 2536 (30.25) | 1637 (64.55) | 899 (35.45) | ||
| >80 | 412 (4.92) | 283 (68.69) | 129 (31.31) | ||
| Sex | 186.165 | <0.001 | |||
| Female | 4110 (49.03) | 2404 (58.49) | 1706 (41.51) | ||
| Male | 4273 (50.97) | 3104 (72.64) | 1169 (27.36) | ||
| Marriage | 71.705 | <0.001 | |||
| NO | 1562 (18.63) | 883 (56.53) | 679 (43.47) | ||
| YES | 6821 (81.37) | 4625 (67.81) | 2196 (32.19) | ||
| Self-rated health | 904.043 | <0.001 | |||
| Very bad | 880 (10.50) | 758 (86.10) | 122 (13.90) | ||
| Bad | 957 (11.40) | 775 (81.00) | 182 (19.00) | ||
| Fair | 4137 (49.30) | 2939 (71.00) | 1198 (29.00) | ||
| Good | 1853 (22.10) | 858 (46.30) | 995 (53.70) | ||
| Very good | 556 (6.60) | 178 (32.00) | 378 (68.00) | ||
| Physical disability | 40.121 | <0.001 | |||
| NO | 8132 (97.00) | 5390 (66.30) | 2742 (33.70) | ||
| YES | 251 (3.00) | 118 (47.00) | 133 (53.00) | ||
| Hypertension | 9.031 | 0.003 | |||
| NO | 7417 (88.50) | 4915 (66.30) | 2502 (33.70) | ||
| YES | 966 (11.20) | 593 (61.40) | 373 (38.60) | ||
| Dyslipidemia | 16.978 | <0.001 | |||
| NO | 7548 (90.00) | 5013 (66.40) | 2535 (33.60) | ||
| YES | 835 (10.00) | 495 (59.20) | 340 (40.70) | ||
| Diabetes | 9.3789 | 0.002 | |||
| NO | 7883 (94.00) | 5211 (66.10) | 2672 (33.90) | ||
| YES | 500 (6.00) | 297 (59.40) | 203 (40.60) | ||
| Medical insurance | 5.971 | 0.015 | |||
| NO | 211 (2.50) | 122 (57.80) | 89 (42.20) | ||
| YES | 8172 (97.50) | 5386 (65.90) | 2786 (34.10) | ||
| Pension | 193.5306 | <0.001 | |||
| NO | 6488 (77.40) | 4010 (61.80) | 2478 (38.20) | ||
| YES | 1895 (22.60) | 1498 (79.10) | 397 (20.90) |
| Variables | Urban Area n (%) | Urban–Rural Area n (%) | Rural Area n (%) | p | |
|---|---|---|---|---|---|
| Depressive | 112.481 | <0.001 | |||
| NO | 1253 (76.03) | 396 (70.71) | 3859 (62.49) | ||
| YES | 395 (23.97) | 164 (29.29) | 2316 (37.51) | ||
| Self-rated health | 77.115 | <0.001 | |||
| Very bad | 174 (10.56) | 52 (9.29) | 654 (10.59) | ||
| Bad | 235 (14.26) | 76 (13.57) | 646 (10.46) | ||
| Fair | 887 (53.82) | 292 (52.14) | 2958 (47.90) | ||
| Good | 269 (16.32) | 101 (10.04) | 1483 (24.02) | ||
| Very good | 83 (5.04) | 39 (6.96) | 434 (7.03) | ||
| Medical insurance | 15.580 | <0.001 | |||
| NO | 21 (1.27) | 10 (1.79) | 180 (1.91) | ||
| YES | 1627 (98.73) | 550 (98.21) | 5995 (97.09) | ||
| Pension | 10.883 | <0.001 | |||
| NO | 521 (31.61) | 286 (51.07) | 5681 (92.00) | ||
| YES | 1127 (68.39) | 274 (48.93) | 494 (8.00) |
| Variables | B | S.E. | Wald | p | OR | 95% CI |
|---|---|---|---|---|---|---|
| Self-rated health | ||||||
| Very bad | −2.497 | 0.137 | 331.029 | <0.001 | 0.082 | 0.063–0.108 |
| Bad | −2.088 | 0.127 | 270.396 | <0.001 | 0.124 | 0.097–0.159 |
| Fair | −1.590 | 0.101 | 248.784 | <0.001 | 0.204 | 0.167–0.249 |
| Good | −0.638 | 0.105 | 36.808 | <0.001 | 0.528 | 0.430–0.655 |
| Physical disability | ||||||
| YES | 0.479 | 0.140 | 11.723 | 0.001 | 1.615 | 1.227–2.125 |
| Hypertension | ||||||
| YES | 0.111 | 0.077 | 2.045 | 0.153 | 1.117 | 0.960–1.300 |
| Dyslipidemia | ||||||
| YES | 0.136 | 0.083 | 2.668 | 0.102 | 1.146 | 0.973–1.350 |
| Diabetes | ||||||
| YES | 0.030 | 0.105 | 0.079 | 0.778 | 1.030 | 0.838–1.266 |
| Medical insurance | ||||||
| YES | −0.177 | 0.154 | 1.335 | 0.248 | 0.837 | 0.620–1.132 |
| Pension | ||||||
| YES | −0.497 | 0.071 | 48.607 | <0.001 | 0.608 | 0.529–0.699 |
| Age | ||||||
| 70–80 | 0.211 | 0.124 | 2.882 | 0.090 | 1.234 | 0.968–1.574 |
| >80 | 0.167 | 0.125 | 1.786 | 0.181 | 1.182 | 0.925–1.511 |
| Sex | ||||||
| Male | 0.516 | 0.053 | 96.172 | <0.001 | 0.597 | 0.539–0.662 |
| Marriage | ||||||
| YES | −0.358 | 0.065 | 30.103 | <0.001 | 0.699 | 0.615–0.795 |
| Education level | ||||||
| Medium level | 0.481 | 0.376 | 1.633 | 0.201 | 1.617 | 0.774–3.381 |
| High level | 0.181 | 0.383 | 0.222 | 0.637 | 1.198 | 0.565–2.539 |
| Income | ||||||
| YES | −0.253 | 0.079 | 10.150 | 0.001 | 0.777 | 0.665–0.907 |
| Social activities | ||||||
| YES | −0.162 | 0.051 | 9.993 | 0.002 | 0.851 | 0.769–0.940 |
| Strenuous exercise | ||||||
| YES | 0.302 | 0.058 | 26.893 | <0.001 | 1.352 | 1.206–1.515 |
| Moderate exercise | ||||||
| YES | 0.014 | 0.052 | 0.071 | 0.789 | 1.014 | 0.915–1.124 |
| Light exercise | ||||||
| YES | −0.072 | 0.066 | 1.170 | 0.279 | 0.931 | 0.818–1.060 |
| Variables | Female (n = 4110) | Male (n = 4273) | ||||
|---|---|---|---|---|---|---|
| n | n | Rate (%) | n | n | Rate (%) | |
| Disability | ||||||
| NO | 3995 | 1633 | 40.88 | 4137 | 1109 | 26.81 |
| YES | 115 | 73 | 63.48 | 136 | 60 | 44.12 |
| 23.52 | 19.85 | |||||
| p | <0.001 | <0.001 | ||||
| Variables | Female (n = 4110) | Male (n = 4273) | ||||
|---|---|---|---|---|---|---|
| n | n | Rate (%) | n | n | Rate (%) | |
| Area | ||||||
| Urban area | 859 | 248 | 28.87 | 789 | 147 | 18.63 |
| Urban–rural area | 278 | 96 | 34.53 | 282 | 68 | 24.11 |
| Rural area | 2973 | 1362 | 45.81 | 3202 | 954 | 29.79 |
| 84.76 | 41.29 | |||||
| p | <0.001 | <0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, M.; Chen, J.; Ma, C. Research on the Relationship between Chinese Elderly Health Status, Social Security, and Depression. Int. J. Environ. Res. Public Health 2022, 19, 7496. https://doi.org/10.3390/ijerph19127496
Shao M, Chen J, Ma C. Research on the Relationship between Chinese Elderly Health Status, Social Security, and Depression. International Journal of Environmental Research and Public Health. 2022; 19(12):7496. https://doi.org/10.3390/ijerph19127496
Chicago/Turabian StyleShao, Min, Jianwei Chen, and Chao Ma. 2022. "Research on the Relationship between Chinese Elderly Health Status, Social Security, and Depression" International Journal of Environmental Research and Public Health 19, no. 12: 7496. https://doi.org/10.3390/ijerph19127496
APA StyleShao, M., Chen, J., & Ma, C. (2022). Research on the Relationship between Chinese Elderly Health Status, Social Security, and Depression. International Journal of Environmental Research and Public Health, 19(12), 7496. https://doi.org/10.3390/ijerph19127496