
Some Interventions to Shift Meta-Norms Are Effective for Changing Behaviors in Low- and Middle-Income Countries: A Rapid Systematic Review


Abstract
:1. Introduction
1.1. Rapid Systematic Reviews
1.2. Objectives
2. Materials and Methods
2.1. Eligibility Criteria
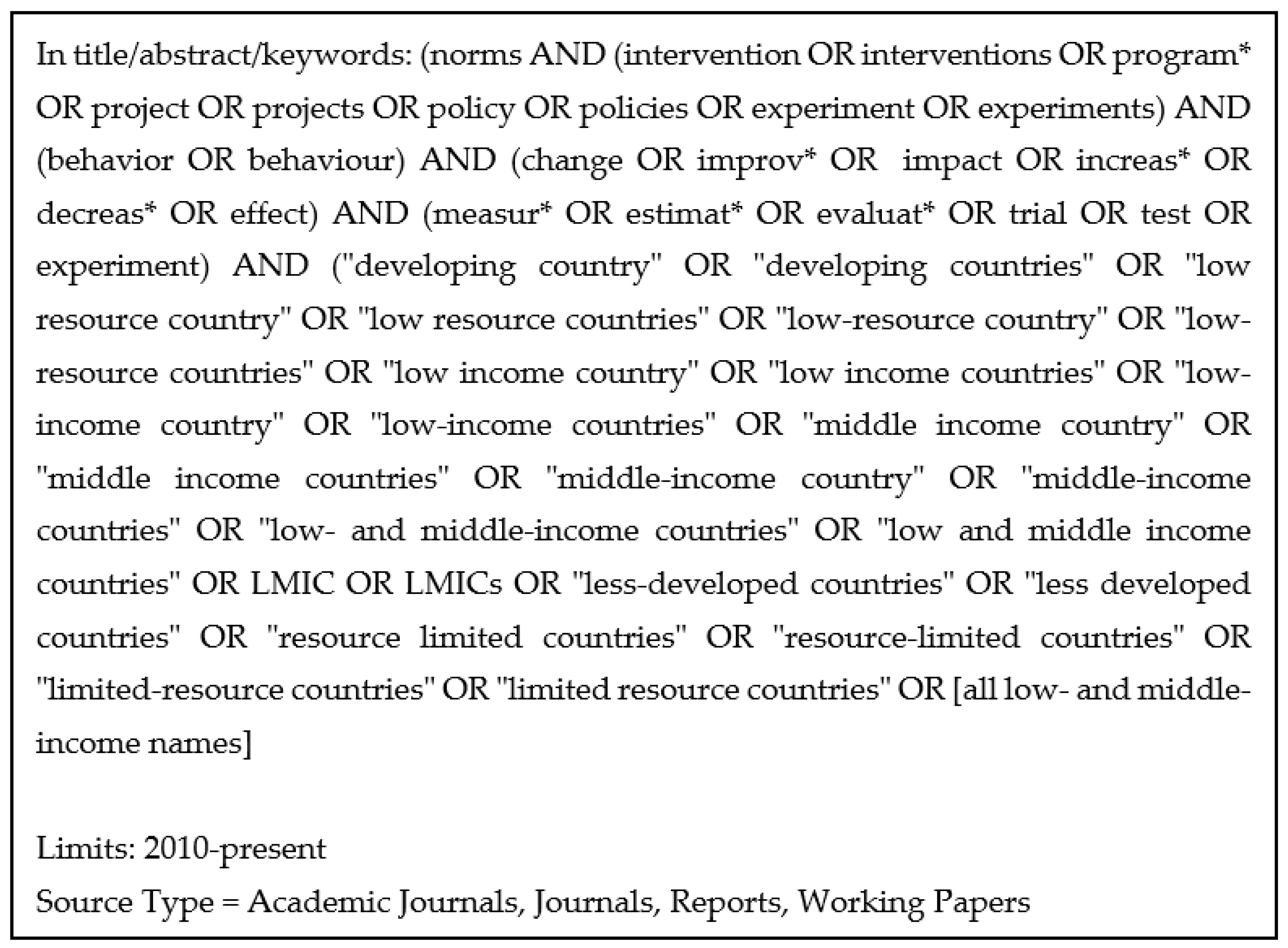
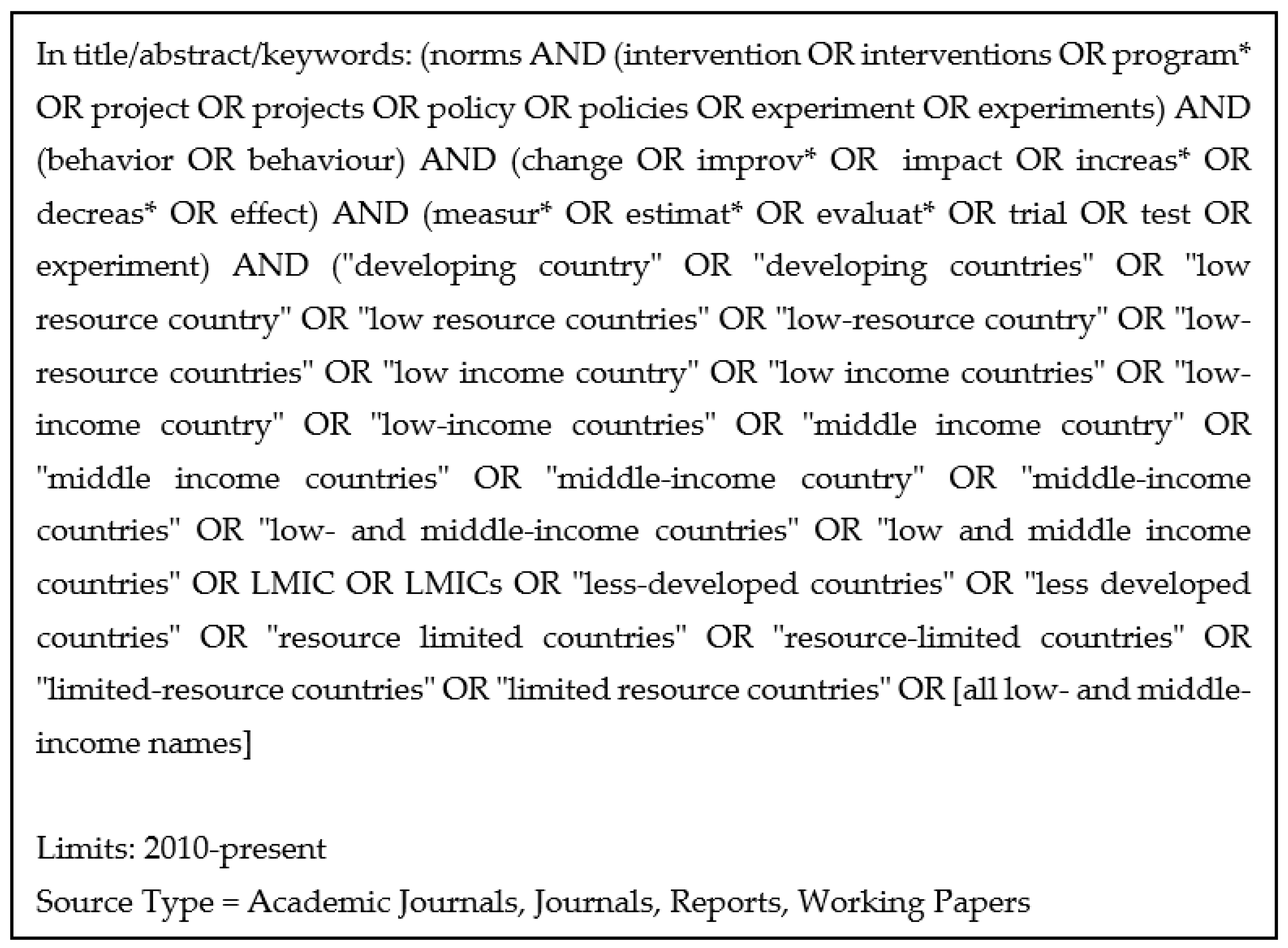
2.2. Search Strategy
2.3. Selection
2.4. Data Collection
2.5. Appraisal
2.6. Analysis
2.7. Inclusion of Systematic Reviews
2.8. Departures from the Protocol
3. Results
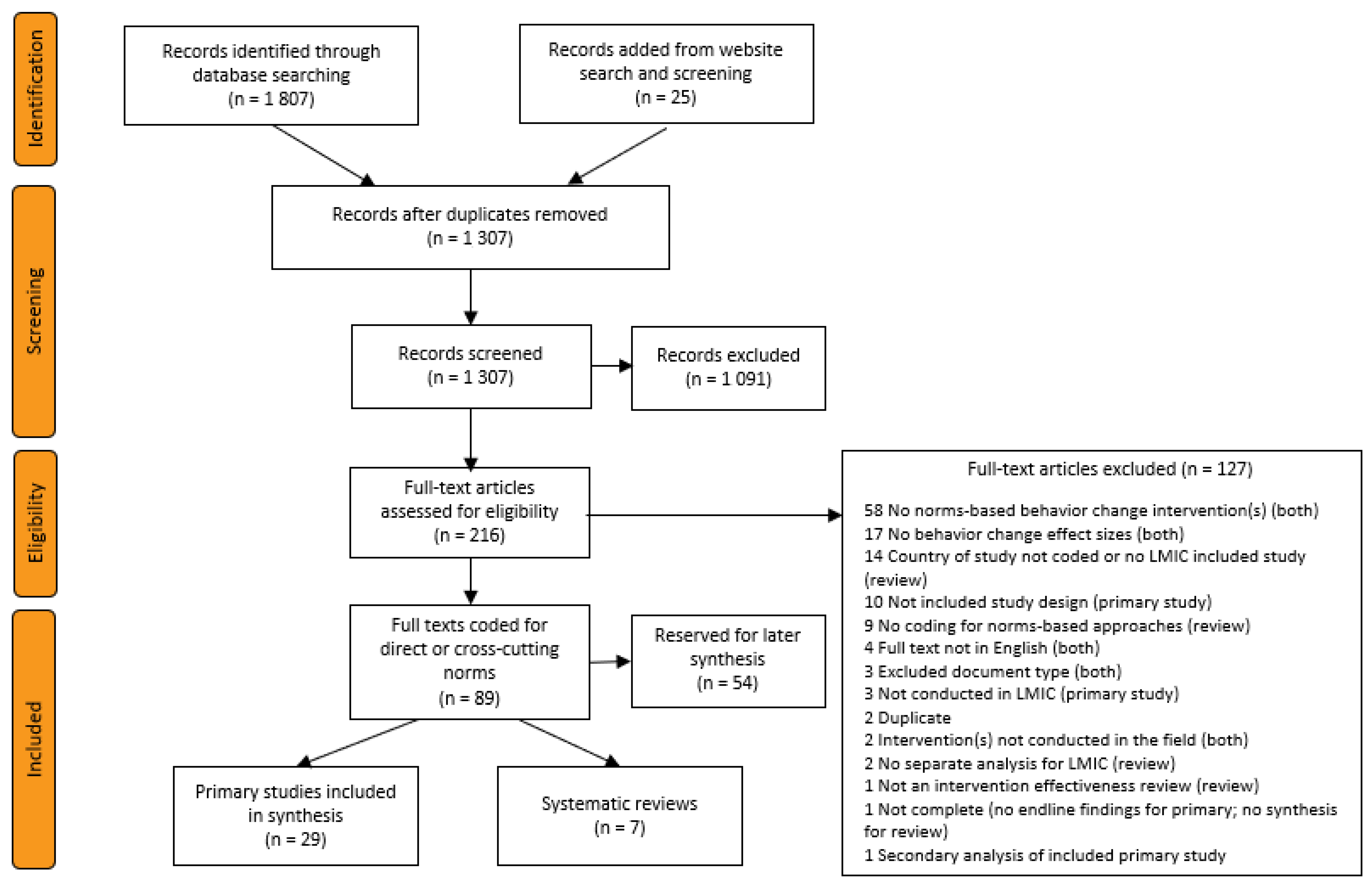
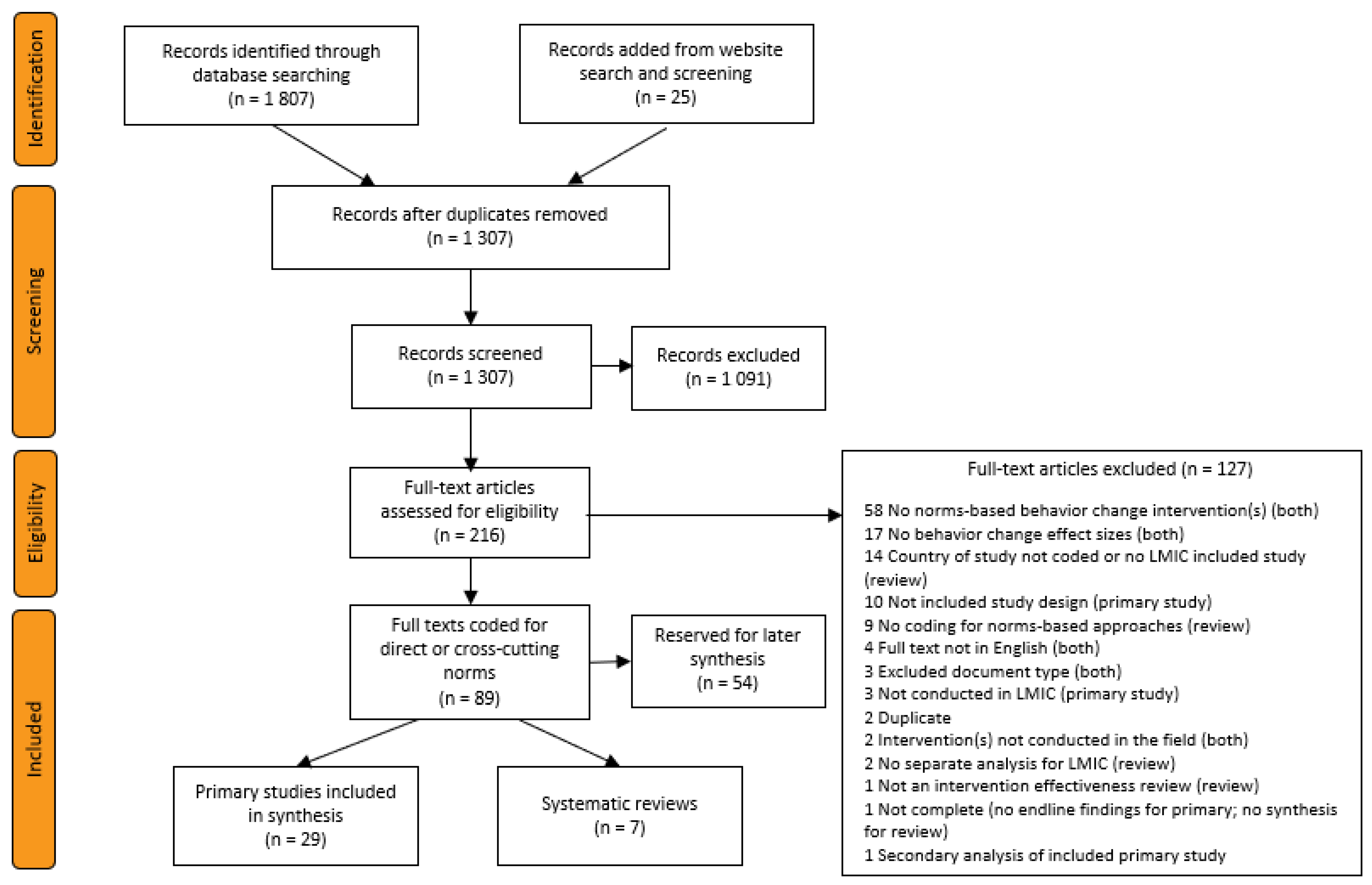
3.1. Literature Search
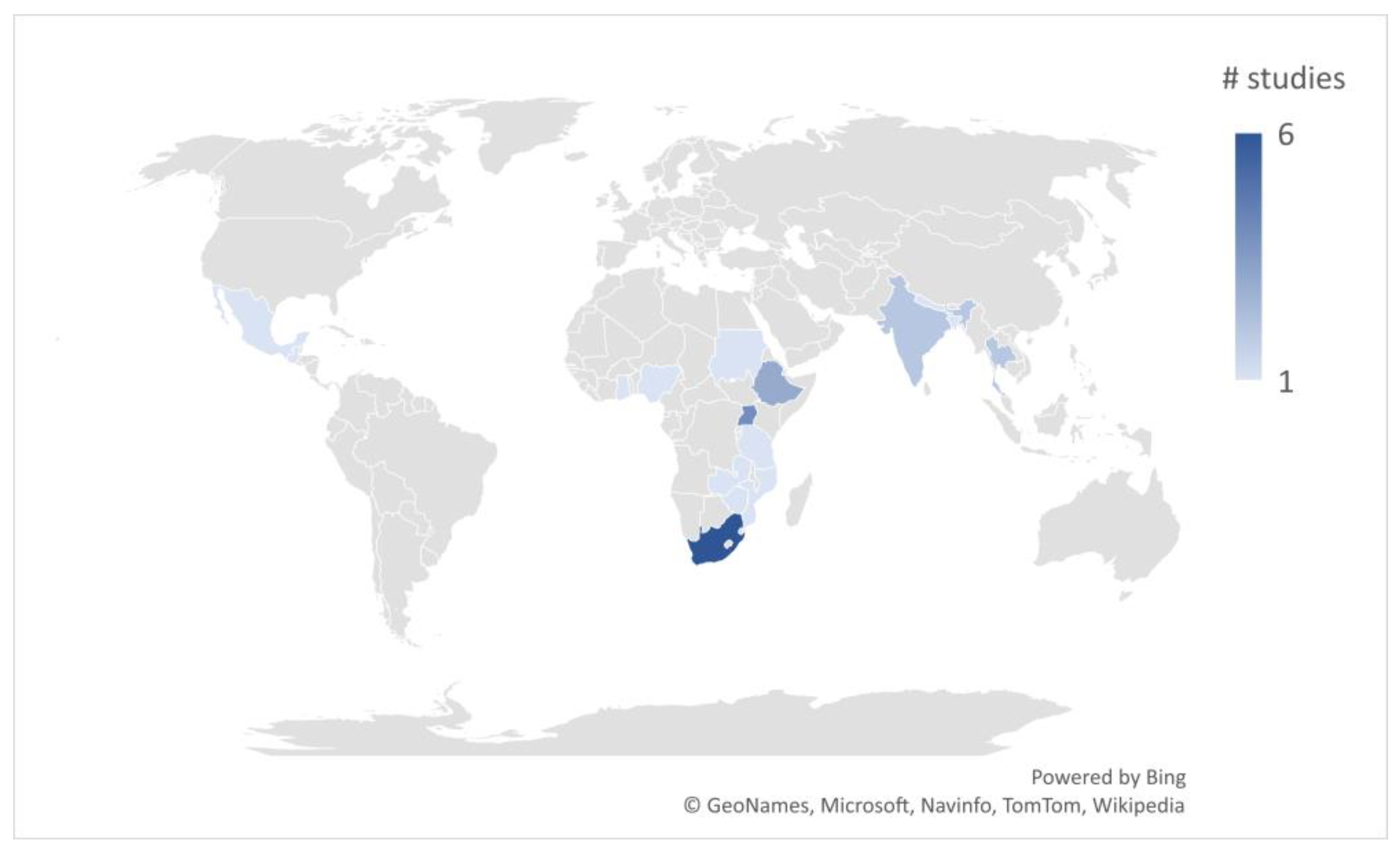
3.2. Characteristics of Included Primary Studies

{kind=link}
{kind=link}
{kind=link}
| Study ID | Title | Country | Program | Norms | Duration Months | Participant Age/Sex | Behavioral Outcome |
|---|---|---|---|---|---|---|---|
| Amin 2018 [46] | Skills-building programs to reduce child marriage in Bangladesh: A randomized controlled trial | Bangladesh | Bangladeshi Association for Life Skills, Income, and Knowledge for Adolescents (BALIKA) | Gender rights | 18 | Adolescents/Female | Personal |
| Avdeenko 2014 [47] | International interventions to build social capital: Evidence from a field experiment in Sudan | Sudan | Community Development Fund | Community pro-sociality | 50 | Adults/Together | Pro-social |
| Banerjee 2019 [32] | The entertaining way to behavioral change: Fighting HIV with MTV | Nigeria | MTV Shuga | Sexual health and HIV prevention | 1 | Youth/Together | Personal |
| Christofides 2020 [38] | Effectiveness of a multi-level intervention to reduce men’s perpetration of intimate partner violence: A cluster randomised controlled trial | South Africa | Sonke Community Health Action for Norms and Gender Equality (CHANGE) | Gender power, gender-based violence, sexuality | 18 | Adults/Male | Continuation |
| Cowan 2010 [33] | The Regai Szive Shiri project: Results of a ramonized trial of an HIV prevention intervention for youth | Zimbabwe | Regai Dzive Shiri | Sexual and reproductive health | 48 | Youth/Both | Personal |
| Dhar 2018 [48] | Reshaping adolescents’ gender attitudes: evidence from a school-based experiment in India | India | Breakthrough classes | Gender equality | 30 | Adolescents/Together | Continuation |
| Dougherty 2018 [50] | A mixed-methods evaluation of a community-based behavior-change program to improve maternal health outcomes in the upper west region of Ghana | Ghana | Community Benefits Health | Maternal health and breastfeeding | 24 | Adults/Female | Help seeking |
| Doyle 2018 [51] | Gender-transformative Bandebereho couples’ intervention to promote male engagement in reproductive and maternal health and violence prevention in Rwanda: Findings from a randomized controlled trial | Rwanda | Bandebereho | Gender equality, fatherhood, maternal health, intimate partner violence | 5 | Adults/Both | Help seeking |
| Figueroa 2016 [34] | Effectiveness of community dialogue in changing gender and sexual norms for HIV prevention: Evaluation of the Tchova Tchova program in Mozambique | Mozambique | Tchova Tchova | Gender equality, sexuality, HIV prevention | 18 | Adults/Together | Personal |
| Gottert 2020 [55] | Gaining traction: Promising shifts in gender norms and intimate partner violence in the context of a community-based HIV prevention trial in South Africa | South Africa | Tsima | Gender equality, relationship violence, sexual health | 36 | Adults/Male | Continuation |
| Kalichman 2013 [35] | Randomized community-level HIV prevention intervention trial for men who drink in South African alcohol-serving venues | South Africa | Alcohol–HIV risk reduction workshops | Safe sex, interpersonal communication | 3 | Adults/Male | Personal |
| Kraft 2012 [36] | Effects of the Gama Cuulu radio serial drama on HIV-related behavior change in Zambia | Zambia | Gama Cuulu Radio Serial Drama | Sexual health, sexual cleansing, child sexual abuse, HIV prevention | 24 | Adults/Together | Personal |
| Kyegombe 2014 [28] | The impact of SASA!, a community mobilization intervention, on reported HIV-related risk behaviours and relationship dynamics in Kampala, Uganda | Uganda | SASA! | Gender equality and power, gender-based violence | 48 | Adults/Both | Personal |
| Lundgren 2018 [49] | Does it take a village? Fostering gender equity among early adolescents in Nepal | Nepal | Choices, Voices, and Promises | Gender equity | 3 | Adolescents/Together | Personal |
| Maman 2020 [42] | Results from a cluster-randomized trial to evaluate a microfinance and peer health leadership intervention to prevent HIV and intimate partner violence among social networks of Tanzanian Men | Tanzania | Microfinance and peer health program for social networks of men | Gender-based violence and power, safe sex | 30 | Adults/Male | Continuation |
| Miller 2014 [39] | Evaluation of a gender-based violence prevention program for student athletes in Mumbai, India | India | Parivartan (Coaching Boys Into Men) | Gender equity, gender-based violence, abuse | 4 | Adolescents/Male | Personal |
| Naidoo 2016 [52] | Verbal bullying changes among students following an educational intervention using the integrated model for behavior change | South Africa | School-based education program | Gender-based violence, bullying | 5 | Adolescents/Together | Pro-social |
| Pettifor 2018 [43] | Community mobilization to modify harmful gender norms and reduce HIV risk: results from a community cluster randomized trial in South Africa | South Africa | Sonke One Man Can community mobilization | Sexual health, gender equality and power, gender-based violence, social cohesion | 24 | Youth/Together | Personal |
| Pulerwitz 2015 [40] | Changing gender norms and reducing intimate partner violence: Results from a quasi-experimental intervention study with young men in Ethiopia | Ethiopia | Male Norms Initiative | Gender equality, sexual health, intimate partner violence | 1 | Youth/Male | Continuation |
| Rijsdijk 2011 [53] | The world starts with me: A multilevel evaluation of a comprehensive sex education programme targeting adolescents in Uganda | Uganda | World Starts With Me | Sexual and reproductive health and rights | 6 | Adolescents/Together | Personal |
| Schuler 2015 [54] | Interactive workshops to promote gender equity and family planning in rural communities of Guatemala: Results of a community randomized study | Guatemala | C-Change couples workshops | Gender equality, sexual and reproductive health | 1 | Adults/Together | Continuation |
| Sharma 2020 [44] | Effectiveness of a culturally appropriate intervention to prevent intimate partner violence and HIV transmission among men, women and couples in rural Ethiopia: Findings from a cluster-randomized controlled trial | Ethiopia | Unite for a Better Life | Gender equality and power, sexuality, violence | 2 | Adults/Both | Continuation |
| Sosa-Rubi 2017 [41] | True Love: Effectiveness of a school-based program to reduce dating violence among adolescents in Mexico City | Mexico | True Love | Gender equality, dating violence, sexual rights | 4 | Adolescents/Both | Personal |
| Stark 2018 [31] | Effects of a social empowerment intervention on economic vulnerability for adolescent refugee girls in Ethiopia | Ethiopia | Creating Opportunities through Mentoring, Parental Involvement and Safe Spaces (COMPASS) | Gender power, reproductive health | 10 | Adolescents/Female | Personal |
| Thato 2013 [37] | A brief, peer-led HIV prevention program for college students in Bangkok, Thailand | Thailand | Brief, Peer-Led HIV Prevention Program | Sexual health, HIV prevention | 1 | Youth/Together | Personal |
| Vantamay 2019 [30] | “3S Project”: A community-based social marketing campaign for promoting sustainable consumption behavior among youth | Thailand | 3S Project | Sustainable consumption | 3 | Youth/Together | Continuation |
| Wagman 2015 [45] | Effectiveness of an integrated intimate partner violence and HIV prevention intervention in Rakai, Uganda: Analysis of an intervention in an existing cluster randomised cohort | Uganda | Safe Homes and Respect for Everyone Project (SHARE) | Gender rights, intimate partner violence | 4 | Adults/Both | Continuation |
| Watts 2015 [29] | The SASA! study: A cluster randomised triral to assess the impact of a violence and HIV prevention programme in Kampala, Uganda | Uganda | SASA! | Gender equality and power, gender-based violence | 32 | Adults/Together | Continuation |
| Wechsberg 2016 [26] | The male factor: Outcomes from a cluster randomized field experiment with a couples-based HIV prevention intervention in a South African township | South Africa | Couples Health Coop, Women’s/Men’s Health Coop | Gender equality, sexuality, intimate partner violence, communication | 1 | Adults/Both | Personal |
3.3. Confidence in Findings
3.4. Estimated Effects on Behavior Change
3.5. Analysis of Program Design
3.6. Systematic Reviews
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Additional Methods and Materials Details
Appendix A.1.1. Search Strategy
Appendix A.1.2. Selection
Appendix A.1.3. Data Collection
Appendix A.1.4. Appraisal
Appendix A.1.5. Departures from the Protocol
Appendix B
Appendix B.1. Systematic Reviews
Appendix B.1.1. Materials and Methods
Appendix B.1.2. Characteristics of Included Systematic Reviews
| Study ID | Title | Geography | Interventions | Participants | Behavioral Outcomes |
|---|---|---|---|---|---|
| Bourey 2015 [60] | Systematic review of structural interventions for intimate partner violence in low- and middle-income countries: organizing evidence for prevention | LMIC | Structural interventions to prevent male-perpetrated IPV including economic, social, and combined economic and social interventions | Adults | IPV incidence (or prevalence) |
| Harrison 2010 [61] | HIV prevention for South African youth: Which interventions work? A systematic review of current evidence | South Africa | In-school and out-of-school, curriculum-based HIV prevention programs for youth | Youth | Sexual and HIV risk |
| Levy 2020 [62] | Characteristics of successful programmes targeting gender inequality and restrictive gender norms for the health and wellbeing of children, adolescents, and young adults: a systematic review | Global | Community engagement and social support, economic stability, education and awareness building, physical environment | Youth | Various |
| Nikolova 2018 [63] | Review of the evidence of gender-focused interventions including men to reduce HIV risk and violence against women in sub-Saharan Africa | Sub-Saharan Africa | HIV and HIV risk programs including or focused on men that also address violence against women | Adults | HIV risk |
| Sunguya 2016 [64] | Ability of HIV advocacy to modify behavioral norms and treatment impact: A systematic review | Global | HIV advocacy interventions, e.g., media, print materials, youth outreach, social marketing | Youth and Adults | HIV risk, HIV testing |
| Temin 2020 [65] | Close to home: Evidence on the impact of community-based girl groups | LMIC | Community-based girl group programs, also known as safe spaces | Adolescents | Various |
| Wamoyi 2014 [66] | A review of interventions addressing structural drivers of adolescents’ sexual and reproductive health vulnerability in sub-Saharan Africa: implications for sexual health programming | Sub-Saharan Africa | Economic empowerment, economic empowerment plus school attendance, safe spaces, behavior-change communication | Adolescents | Various |
| Study ID | Eligibility Criteria | Identification and Selection | Data Collection and Appraisal | Synthesis and Findings | Overall Risk of Bias | Notes | Number of Included Studies |
|---|---|---|---|---|---|---|---|
| Bourey 2015 [60] | Low | Unclear | Unclear | Unclear | Unclear | Only two indexes searched and no web search; extracted same outcomes from multiple articles of same study; risk of bias not addressed in results synthesis; emphasis of results based on statistical significance | 20 articles covering 16 programs |
| Harrison 2010 [61] | Unclear | Unclear | Unclear | High | High | Some of the exclusion criteria seem arbitrarily applied; no details about screening process; no risk-of-bias assessment | 13 articles covering 8 programs |
| Levy 2020 [62] | Low | Unclear | Unclear | High | High | Limited information on search terms and selection procedures; no risk-of-bias assessment other than methods parameters; synthesis methods not clear but emphasis on statistical significance | 61 documents covering 59 programs |
| Nikolova 2018 [63] | Low | Low | Unclear | Unclear | Unclear | Extracted same outcomes from multiple articles of same study; quality-rating methodology not clear; rating addressed in results synthesis; vote counting | 17 articles covering 13 programs |
| Sunguya 2016 [64] | Low | Low | Low | Unclear | Unclear | No summary measure risk of bias, risk of bias not addressed in results synthesis | 25 |
| Temin 2020 [65] | Low | High | High | High | High | Limited search terms produced very few initial hits; no risk-of-bias assessment; extracted large number of outcomes from each study; vote counting | 30 programs |
| Wamoyi 2014 [66] | Low | High | High | Unclear | High | Almost all screening at title level; no study design criteria; extracted large number of outcomes for each program; no risk-of-bias assessment | 21 documents covering 15 programs |
Appendix B.1.3. Systematic Review Findings
References
- Heise, L.; Manji, K. Social norms. In GSDRC Professional Development Reading Pack; Department for International Development: London, UK, 2016. [Google Scholar]
- Perkins, H.W.; Berkowitz, A.D. Perceiving the Community Norms of Alcohol Use among Students: Some Research Implications for Campus Alcohol Education Programming. Int. J. Addict. 1986, 21, 961–976. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, R.C.; McAlaney, J.; Bewick, B.M. A Critical Appraisal of the Social Norms Approach as an Interventional Strategy for Health-Related Behavior and Attitude Change. Front. Psychol. 2018, 9, 2180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allcott, H. Social norms and energy conservation. J. Public Econ. 2011, 95, 1082–1095. [Google Scholar] [CrossRef] [Green Version]
- Cislaghi, B.; Shakya, H. Social Norms and Adolescents’ Sexual Health: An Introduction for Practitioners Working in Low and Mid-income African countries. Afr. J. Reprod. Health 2018, 22, 38–46. [Google Scholar] [CrossRef]
- Ashburn, K.; Costenbader, B.; Igras, S.; Pirzadeh, M.; Homan, R. Social Norms Background Reader; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2016; Available online: https://www.alignplatform.org/resources/social-norms-background-reader-0 (accessed on 11 March 2021).
- Tankard, M.E.; Paluck, E.L. Norm perception as a vehicle for social change. Soc. Issues Policy Rev. 2016, 10, 181–211. [Google Scholar] [CrossRef]
- Lundgren, R.; Uysal, J.; Barker, K.; McLarnon-Silk, C.; Shaw, B.; Greenberg, J.; Kohli, A. Social Norms Lexicon; Institute for Reproductive Health, Georgetown University for the U.S. Agency for International Development; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2021. [Google Scholar]
- Nguyen, G.; Costenbader, E.; Plourde, K.F.; Kerner, B.; Igras, S. Scaling-up Normative Change Interventions for Adolescent and Youth Reproductive Health: An Examination of the Evidence. J. Adolesc. Health 2019, 64, S16–S30. [Google Scholar] [CrossRef] [Green Version]
- Learning Collaborative to Advance Normative Change. Identifying and Describing Approaches and Attributes of Norms-Shifting Interventions; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2017. [Google Scholar]
- Yamin, P.; Fei, M.; Lahlou, S.; Levy, S. Using Social Norms to Change Behavior and Increase Sustainability in the Real World: A Systematic Review of the Literature. Sustainability 2019, 11, 5847. [Google Scholar] [CrossRef] [Green Version]
- Brown, A.N. An approach to rapid evidence review and what we learned when we piloted it. R&E Search for Evidence, 30 September 2020. [Google Scholar]
- Brown, A.N.; Shieh, J. What evidence in there for interventions to address the dual burden of malnutrition? A rapid review. R&E Search for Evidence, 13 October 2020. [Google Scholar]
- Brown, A.N.; Shieh, J. School-based physical activity and diet interventions can be effective for addressing obesity in children in LMICs: Evidence from systematic reviews. R&E Search for Evidence, 13 November 2020. [Google Scholar]
- Affengruber, L.; Wagner, G.; Waffenschmidt, S.; Lhachimi, S.K.; Nussbaumer-Streit, B.; Thaler, K.; Griebler, U.; Klerings, I.; Gartlehner, G. Combining abbreviated literature searches with single-reviewer screening: Three case studies of rapid reviews. Syst. Rev. 2020, 9, 162. [Google Scholar] [CrossRef]
- Featherstone, R.M.; Dryden, D.M.; Foisy, M.; Guise, J.-M.; Mitchell, M.D.; Paynter, R.A.; Robinson, K.A.; Umscheid, C.A.; Hartling, L. Advancing knowledge of rapid reviews: An analysis of results, conclusions and recommendations from published review articles examining rapid reviews. Syst. Rev. 2015, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E. A scoping review of rapid review methods. BMC Med. 2015, 13, 224. [Google Scholar] [CrossRef] [Green Version]
- Khangura, S.; Konnyu, K.; Cushman, R.; Grimshaw, J.; Moher, D. Evidence summaries: The evolution of a rapid review approach. Syst. Rev. 2012, 1, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Langlois, E.V.; Straus, S.E. (Eds.) Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide; World Health Organization: Geneva, Switzerland, 2017; p. 119.
- Brown, A.N. Rapid Evidence Review of The Effectiveness of Behavior Change Interventions That Incorporate Social Norms Approaches in Low- And Middle-Income Countries. 2020. Available online: https://osf.io/3fpnq (accessed on 28 April 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blattman, C.; Hartman, A.C.; Blair, R.A. How to promote order and property rights under weak rule of Law? An experiment in changing dispute resolution behavior through Community Education. Am. Political Sci. Rev. 2014, 108, 100–120. [Google Scholar] [CrossRef]
- Brown, A.N. Public health vs. social science: Do publication lags matter? R&E Search for Evidence, 18 December 2019. [Google Scholar]
- Shelton, J.D. The 6 domains of behavior change: The missing health system building block. Glob. Health Sci. Pract. 2013, 1, 137–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waddington, H.; Aloe, A.M.; Becker, B.J.; Djimeu, E.W.; Hombrados, J.G.; Tugwell, P.; Wells, G.; Reeves, B. Quasi-experimental study designs series-paper 6: Risk of bias assessment. J. Clin. Epidemiol. 2017, 89, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wechsberg, W.M.; Zule, W.A.; El-Bassel, N.; Doherty, I.A.; Minnis, A.M.; Novak, S.D.; Myers, B.; Carney, T. The male factor: Outcomes from a cluster randomized field experiment with a couples-based HIV prevention intervention in a South African township. Drug Alcohol Depend. 2016, 161, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speizer, I.S.; Zule, W.A.; Carney, T.; Browne, F.A.; Ndirangu, J.; Wechsberg, W.M. Changing sex risk behaviors, gender norms, and relationship dynamics among couples in Cape Town, South Africa: Efficacy of an intervention on the dyad. Soc. Sci. Med. 2018, 209, 95–103. [Google Scholar] [CrossRef]
- Kyegombe, N.; Abramsky, T.; Devries, K.M.; Starmann, E.; Michau, L.; Nakuti, J.; Musuya, T.; Heise, L.; Watts, C. The impact of SASA!, a community mobilization intervention, on reported HIV-related risk behaviours and relationship dynamics in Kampala, Uganda. J. Int. AIDS Soc. 2014, 17, 19232. [Google Scholar] [CrossRef]
- Watts, C.; Devries, K.; Kiss, L.; Abramsky, T.; Kyegombe, N.; Michau, L. The SASA! Study: A Cluster Randomised Trial to Assess the Impact of a Violence and HIV Prevention Programme in Kampala, Uganda; International Initiative for Impact Evaluation: New Delhi, India, 2015; pp. 1–34. [Google Scholar]
- Vantamay, N. “3S project”: A community-based social marketing campaign for promoting sustainable consumption behavior among youth. J. Komun. Malays. J. Commun. 2019, 35, 32–49. [Google Scholar] [CrossRef]
- Stark, L.; Seff, I.; Assezenew, A.; Eoomkham, J.; Falb, K.; Ssewamala, F.M. Effects of a Social Empowerment Intervention on Economic Vulnerability for Adolescent Refugee Girls in Ethiopia. J. Adolesc. Health 2018, 62, S15–S20. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, A.; Ferrara, E.L.; Orozco-Olvera, V.H. The Entertaining Way to Behavioral Change: Fighting HIV with MTV. 2019. Available online: http://www.nber.org/papers/w26096.pdf (accessed on 13 November 2020).
- Cowan, F.M.; Pascoe, S.J.; Langhaug, L.F.; Mavhu, W.; Chidiya, S.; Jaffar, S.; Mbizvo, M.T.; Stephenson, J.M.; Johnson, A.M.; Power, R.M.; et al. The Regai Dzive Shiri project: Results of a randomized trial of an HIV prevention intervention for youth. Aids 2010, 24, 2541–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueroa, M.E.; Poppe, P.; Carrasco, M.; Pinho, M.D.; Massingue, F.; Tanque, M.; Kwizera, A. Effectiveness of Community Dialogue in Changing Gender and Sexual Norms for HIV Prevention: Evaluation of the Tchova Tchova Program in Mozambique. J. Health Commun. 2016, 21, 554–563. [Google Scholar] [CrossRef] [Green Version]
- Kalichman, S.C.; Simbayi, L.C.; Cain, D.; Carey, K.B.; Carey, M.P.; Eaton, L.; Harel, O.; Mehlomakhulu, V.; Mwaba, K. Randomized community-level HIV prevention intervention trial for men who drink in South African alcohol-serving venues. Eur. J. Public Health 2013, 24, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraft, J.; Hill, Z.; Membe, I.; Zhang, Y.; Meassick, E.; Monsour, M.; Maumbi, M.; Ndubani, P.; Manengu, J.; Mwinga, A. Effects of the Gama Cuulu Radio Serial Drama on HIV-Related Behavior Change in Zambia. J. Health Commun. 2012, 17, 929–945. [Google Scholar] [CrossRef] [PubMed]
- Thato, R.; Penrose, J. A Brief, Peer-Led HIV Prevention Program for College Students in Bangkok, Thailand. J. Pediatr. Adolesc. Gynecol. 2013, 26, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Christofides, N.J.; Hatcher, A.M.; Rebombo, D.; McBride, R.S.; Munshi, S.; Pino, A.; Abdelatif, N.; Peacock, D.; Levin, J.; Jewkes, R.K. Effectiveness of a multi-level intervention to reduce men’s perpetration of intimate partner violence: A cluster randomised controlled trial. Trials 2020, 21, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, E.; Das, M.; Tancredi, D.J.; McCauley, H.L.; Virata, M.C.; Nettiksimmons, J.; O’Connor, B.; Ghosh, S.; Verma, R. Evaluation of a gender-based violence prevention program for student athletes in Mumbai, India. J. Interpers Violence 2014, 29, 758–778. [Google Scholar] [CrossRef]
- Pulerwitz, J.; Hughes, L.; Mehta, M.; Kidanu, A.; Verani, F.; Tewolde, S. Changing Gender Norms and Reducing Intimate Partner Violence: Results from a Quasi-Experimental Intervention Study with Young Men in Ethiopia. Am. J. Public Health 2015, 105, 132–137. [Google Scholar] [CrossRef]
- Sosa-Rubi, S.; Saavedra-Avendano, B.; Piras, C.; Van Buren, S.; Bautista-Arredondo, S.; Sosa-Rubi, S.G.; Van Buren, S.J. True Love: Effectiveness of a School-Based Program to Reduce Dating Violence among Adolescents in Mexico City. Prev. Sci. 2017, 18, 804–817. [Google Scholar] [CrossRef]
- Maman, S.; Mulawa, M.I.; Balvanz, P.; Luz McNaughton Reyes, H.; Kilonzo, M.N.; Yamanis, T.J.; Singh, B.; Kajula, L.J. Results from a cluster-randomized trial to evaluate a microfinance and peer health leadership intervention to prevent HIV and intimate partner violence among social networks of Tanzanian men. PLoS ONE 2020, 15, e0230371. [Google Scholar] [CrossRef] [Green Version]
- Pettifor, A.; Lippman, S.A.; Gottert, A.; Suchindran, C.M.; Selin, A.; Peacock, D.; Maman, S.; Rebombo, D.; Twine, R.; Gómez-Olivé, F.X.; et al. Community mobilization to modify harmful gender norms and reduce HIV risk: Results from a community cluster randomized trial in South Africa. J. Int. AIDS Soc. 2018, 21, e25134. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Leight, J.; Verani, F.; Tewolde, S.; Deyessa, N. Effectiveness of a culturally appropriate intervention to prevent intimate partner violence and HIV transmission among men, women, and couples in rural Ethiopia: Findings from a cluster-randomized controlled trial. PLoS Med. 2020, 17, e1003274. [Google Scholar] [CrossRef] [PubMed]
- Wagman, J.A.; Gray, R.H.; Campbell, J.C.; Thoma, M.; Ndyanabo, A.; Ssekasanvu, J.; Nalugoda, F.; Kagaayi, J.; Nakigozi, G.; Serwadda, D.; et al. Effectiveness of an integrated intimate partner violence and HIV prevention intervention in Rakai, Uganda: Analysis of an intervention in an existing cluster randomised cohort. Lancet Glob. Health 2015, 3, e23–e33. [Google Scholar] [CrossRef] [Green Version]
- Amin, S.; Saha, J.S.; Ahmed, J.A. Skills-Building Programs to Reduce Child Marriage in Bangladesh: A Randomized Controlled Trial. J. Adolesc. Health 2018, 63, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Avdeenko, A.; Gilligan, M.J. International Interventions to Build Social Capital: Evidence from a Field Experiment in Sudan. Am. Political Sci. Rev. 2015, 109, 427–449. [Google Scholar] [CrossRef] [Green Version]
- Dhar, D.; Jain, T.; Jayachandran, S. Reshaping Adolescents’ Gender Attitudes: Evidence from a School-Based Experiment in India. 2018. Available online: http://www.nber.org/papers/w25331.pdf (accessed on 13 November 2020).
- Lundgren, R.; Gibbs, S.; Kerner, B. Does it take a village? Fostering gender equity among early adolescents in Nepal. Int. J. Adolesc. Med. Health 2018, 32, 20170164. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, L.; Stammer, E.; Derbile, E.; Dery, M.; Yahaya, W.; Gle, D.B.; Otieno, J.; Fotso, J.C. A Mixed-Methods Evaluation of a Community-Based Behavior Change Program to Improve Maternal Health Outcomes in the Upper West Region of Ghana. J. Health Commun. 2018, 23, 80–90. [Google Scholar] [CrossRef]
- Doyle, K.; Levtov, R.G.; Barker, G.; Bastian, G.G.; Bingenheimer, J.B.; Kazimbaya, S.; Nzabonimpa, A.; Pulerwitz, J.; Sayinzoga, F.; Sharma, V.; et al. Gender-transformative bandebereho couples’ intervention to promote male engagement in reproductive and maternal health and violence prevention in Rwanda: Findings from a randomized controlled trial. PLoS ONE 2018, 13, e0192756. [Google Scholar] [CrossRef] [Green Version]
- Naidoo, S.; Satorius, B.K.; de Vries, H.; Taylor, M. Verbal Bullying Changes Among Students Following an Educational Intervention Using the Integrated Model for Behavior Change. J. Sch. Health 2016, 86, 813–822. [Google Scholar] [CrossRef]
- Rijsdijk, L.E.; Bos, A.E.; Ruiter, R.A.; Leerlooijer, J.N.; De Haas, B. The World Starts with Me: A multilevel evaluation of a comprehensive sex education programme targeting adolescents in Uganda. BMC Public Health 2011, 11, 334. [Google Scholar] [CrossRef]
- Schuler, S.R.; Nanda, G.; Ramírez, L.F.; Chen, M. Interactive workshops to promote gender equity and family planning in rural communities of Guatemala: Results of a community randomized study. J. Biosoc. Sci. 2015, 47, 667–686. [Google Scholar] [CrossRef] [PubMed]
- Gottert, A.; Pulerwitz, J.; Haberland, N.; Mathebula, R.; Rebombo, D.; Spielman, K.; West, R.; Julien, A.; Twine, R.; Peacock, D.; et al. Gaining traction: Promising shifts in gender norms and intimate partner violence in the context of a community-based HIV prevention trial in South Africa. PLoS ONE 2020, 15, e0237084. [Google Scholar] [CrossRef] [PubMed]
- Homan, R. Costing of Norms-Shifting Interventions: A Primer from the Passages Project; Institute for Reproductive Health, Georgetown University for the U.S. Agency for International Development; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2020. [Google Scholar]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS Group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Brown, A.N.; Skelly, H.J. How much evidence is there really? Mapping the evidence base for ICTD interventions. Inf. Technol. Int. Dev. 2019, 15, 16–33. [Google Scholar]
- Bourey, C.; Williams, W.; Bernstein, E.E.; Stephenson, R. Systematic review of structural interventions for intimate partner violence in low- and middle-income countries: Organizing evidence for prevention. BMC Public Health 2015, 15, 1165. [Google Scholar] [CrossRef] [Green Version]
- Harrison, A.; Newell, M.L.; Imrie, J.; Hoddinott, G. HIV prevention for South African youth: Which interventions work? A systematic review of current evidence. BMC Public Health 2010, 10, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.K.; Darmstadt, G.L.; Ashby, C.; Quandt, M.; Halsey, E.; Nagar, A.; Greene, M.E. Characteristics of successful programmes targeting gender inequality and restrictive gender norms for the health and wellbeing of children, adolescents, and young adults: A systematic review. Lancet Glob. Health 2020, 8, e225–e236. [Google Scholar] [CrossRef] [Green Version]
- Nikolova, S.P.; Small, E. Review of the evidence of gender-focused interventions including men to reduce HIV risk and violence against women in sub-Saharan Africa. J. HIV/AIDS Soc. Serv. 2018, 17, 87–117. [Google Scholar] [CrossRef]
- Sunguya, B.F.; Munisamy, M.; Pongpanich, S.; Junko, Y.; Jimba, M. Ability of HIV Advocacy to Modify Behavioral Norms and Treatment Impact: A Systematic Review. Am. J. Public Health 2016, 106, e1–e8. [Google Scholar] [CrossRef]
- Temin, M.; Heck, C.J. Close to home: Evidence on the impact of community-based girl groups. Glob. Health Sci. Pract. 2020, 8, 300–324. [Google Scholar] [CrossRef]
- Wamoyi, J.; Mshana, G.; Mongi, A.; Neke, N.; Kapiga, S.; Changalucha, J. A review of interventions addressing structural drivers of adolescents’ sexual and reproductive health vulnerability in sub-Saharan Africa: Implications for sexual health programming. Reprod. Health 2014, 11, 131–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jewkes, R.; Gibbs, A.; Jama-Shai, N.; Willan, S.; Misselhorn, A.; Mushinga, M.; Washington, L.; Mbatha, N.; Skiweyiya, Y. Stepping Stones and Creating Futures intervention: Shortened interrupted time series evaluation of a behavioural and structural health promotion and violence prevention intervention for young people in informal settlements in Durban, South Africa. BMC Public Health 2014, 14, 1325. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Watts, C.H.; Hargreaves, J.R.; Ndhlovu, L.X.; Phetla, G.; Morison, L.A.; Busza, J.; Porter, J.D.H.; Pronyk, P. Understanding the impact of a microfinance-based intervention on women’s empowerment and the reduction of intimate partner violence in South Africa. Am. J. Public Health 2007, 97, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Ferrari, G.; Abramsky, T.; Watts, C.; Hargreaves, J.; Morison, L.; Phetla, G.; Porter, J.; Pronyk, P. Assessing the incremental effects of combining economic and health interventions: The IMAGE study in South Africa. Bull World Health Organ 2009, 87, 824–832. [Google Scholar] [CrossRef]
- Pronyk, P.M.; Hargreaves, J.R.; Kim, J.C.; Morison, L.A.; Phetla, G.; Watts, C.; Busza, J.; Porter, J.D. Effect of a structural intervention for the prevention of intimate-partner violence and HIV in rural South Africa: A cluster randomised trial. Lancet 2006, 368, 1973–1983. [Google Scholar] [CrossRef]
- Gupta, J.; Falb, K.L.; Lehmann, H.; Kpebo, D.; Xuan, Z.; Hossain, M.; Zimmerman, C.; Watts, C.; Annan, J. Gender norms and economic empowerment intervention to reduce intimate partner violence against women in rural Côte d’Ivoire: A randomized controlled pilot study. BMC Int. Health Hum. Rights 2013, 13, 46. [Google Scholar] [CrossRef] [Green Version]
| Study ID | Identification Strategy | Number of Concerns | Concern Notes | Sample Size |
|---|---|---|---|---|
| Strong confidence | ||||
| Amin 2018 [46] | CRCT | 0 | None | 5309 |
| Avdeenko (2015) [47] | CRCT | 0 | None | 576 |
| Banerjee 2019 [32] | CRCT | 1 | Working paper | 3070 |
| Christofides 2020 [38] | CRCT | 0 | None | 1508 |
| Cowan 2010 [33] | CRCT | 1 | High attrition from outmigration | 2079 |
| Dhar 2018 [48] | CRCT | 1 | Working paper | 13,987 |
| Doyle 2018 [51] | RCT | 1 | Multiple comparisons | 1123 |
| Gottert 2020 [55] | CRCT | 0 | None | 915 |
| Kalichman 2013 [35] | CRCT | 1 | Multiple comparisons | 984 |
| Maman 2020 [42] | CRCT | 0 | None | 1029 |
| Pettifor 2018 [43] | CRCT | 1 | Repeated cross-section used to measure individual changes | 2356 |
| Schuler 2015 [54] | CRCT | 1 | High lost to follow-up | 294 |
| Sharma 2020 [44] | CRCT | 0 | None | 5125 |
| Stark 2018 [31] | CRCT | 0 | None | 881 |
| Wechsberg 2016 [26] | CRCT | 0 | None | 533 |
| Good confidence | ||||
| Kyegombe 2014 [28] | CRCT | 2 | Challenges to implementation, social desirability bias related to intervention, multiple comparisons | 2530 |
| Naidoo 2016 [52] | CRCT | 2 | High attrition, behavioral metric unclear, no correction for clusters | 434 |
| Pulerwitz 2015 [40] | DD | 0 | None | 483 |
| Sosa-Rubi 2017 [41] | DD | 0 | None | 885 |
| Thato 2013 [37] | DD | 0 | None | 30 |
| Vantamay 2019 [30] | DD | 0 | None | 80 |
| Watts 2015 [29] | CRCT | 2 | Institutional report, challenges to implementation | 1459 |
| Weak confidence | ||||
| Dougherty 2018 [50] | SD | 3 | Confusion over the implementation of the intervention incentives, evidence of spillover, no correction for clusters | 1050 |
| Figueroa 2016 [34] | SD | 1 | Multiple comparisons, weak indexes, social desirability bias related to intervention | 915 |
| Kraft 2012 [36] | SD | 1 | Implementation challenges | 3624 |
| Lundgren 2018 [49] | DD | 2 | Shortened intervention period, multiple comparisons, no true control | 1200 |
| Miller 2014 [39] | DD | 2 | Evidence of implementation fidelity problems, high lost to follow-up | 309 |
| Rijsdijk 2011 [53] | DD | 2 | Intervention not implemented with fidelity in all sites, multiple outcomes | 1519 |
| Wagman 2015 [45] | DD | 2 | Attrition, multiple comparisons | 2953 |
| Study ID and Program | Intervention Level | Intervention Activities | Key Findings on Behavioral Outcomes |
|---|---|---|---|
| Amin 2018 [46] BALIKA | Individual | Training centers for girls offering education assistance, gender rights awareness training, or livelihoods skills; mentors | “The average program effect in the community was significant with adjusted hazard ratio…0.72…for gender…relative to those living in control arm villages.” p. 29 |
| Avdeenko 2015 [47] Community Development Fund | Community | Community construction projects, capacity building for project management and community participation, social mobilizers, community scorecards | “Respondents in treated communities self-report greater civic participation than do respondents in control communities.” p. 441 However, “Subjects in treated communities did not behave more prosocially in any of the laboratory activities than did subjects from control communities.” p. 438 |
| Banerjee 2019 [32] MTV Shuga | Community | Edutainment, television serial drama | The study estimates that MTV Shuga led to reduction in risky sexual behavior as measured by an index, but the effect is not statistically significant. p. 23 |
| Christofides 2020 [38] Sonke CHANGE | Both | Door-to-door discussions, community action teams, workshops | “We found that the intervention did not significantly affect any of the primary or secondary outcomes. There was no effect on men’s past year use of physical or sexual IPV or a reduction in severe IPV.” p. 10 |
| Cowan 2010 [33] Regai Dzive Shiri | Both | Youth program delivered by professional peer educators, community-based program for knowledge and support, training for clinic workers | “There was no effect of the intervention on reported sexual behavior, reported clinic use or reported use of pregnancy prevention in men or women in intervention communities.” p. 2549 |
| Dhar 2018 [48] Breakthrough classes | Individual | School-based classroom discussions | “...self-reported behaviors influenced by gender attitudes...became more aligned with gender-progressive norms...” p. 15 |
| Doyle 2018 [51] Bandebereho | Individual | Small group sessions with curricula for couples and men and women separately | “The Bendebereho intervention led to substantial improvements in multiple reported outcomes, including … women’s ANC attendance, men’s accompaniment at ANC, modern contraceptive use, and partner support during pregnancy.” p. 12 |
| Gottert 2020 [55] Tsima (by Sonke) | Both | Workshops for men and women, street theater and community activities, support groups, local leadership engagement | “Younger men in both intervention and control communities reported reductions in IPV perpetration, leading to a null intervention effect.” p. 14 |
| Kalichman 2013 [35] Alcohol-HIV risk reduction workshops | Both | Individual-level workshops, role playing, community-level activation | “However, there was a significant effect of the intervention on proportion of intercourse occasions protected by condoms; the experimental HIV prevention groups demonstrated significantly greater use of condoms over the follow-up period. Also, men in the intervention condition engaged in more conversations within their communities about HIV/AIDS…” p. 836 |
| Maman 2020 [42] Microfinance and peer health program | Individual | Business and entrepreneurship training, microfinance loans, investment groups, peer health leader training, peer health discussions | For men, “there were no differences in condition in STI prevalence, IPV perpetration, or sexual risk behaviors at the 30-month follow-up.” p. 1 |
| Pettifor 2018 [43] Sonke One Man Can | Community | Community workshops, community action teams, community theater and discussion, leader engagement | “When examining secondary endpoints for the trial, we did not observe significant differences among men in intervention versus control communities over time regarding multiple sex partners in the past 12 months, condom use at last sex, perpetration or experience of intimate partner violence or hazardous drinking.” p. 6 |
| Schuler 2015 [54] C-Change couples workshops | Individual | Interactive workshops for couples (together and separate), games, role playing | “Findings regarding contraceptive use were suggestive but not significant.” |
| Sharma 2020 [44] Unite for a Better Life | Individual | Participatory and skills-building sessions delivered as part of coffee ceremonies | “For the secondary outcomes, only the men’s UBL intervention significantly reduced male perpetration of past-year sexual IPV...and no intervention reduced perpetration of past-year physical IPV.” |
| Stark 2018 [31] COMPASS | Individual | Weekly sessions for girl groups with mentors in traditional huts, parental engagement | “...girls in the treatment arm had approximately equal odds compared to girls in the control arm of working for pay at the end line... We observe moderate trends in the hypothesized directions for schooling and transactional sexual exploitation...” p. S17 |
| Wechsberg 2016 [26] Couples’, Women’s and Men’s Health Coops | Individual | Peer-led workshops with groups in community libraries, including role playing and action planning | “Men in the CHC arm were half as likely to report heavy drinking at 6-month follow-up as men in the comparison arm…The proportion of men reporting consistent condom use in the past 30 days increase in each intervention arm.” p. 313 |
| Study ID | Intervention Level | Intervention Activities | Key Findings on Behavioral Outcomes |
|---|---|---|---|
| Kyegombe 2014 [28] SASA! | Community | Community activists, training of professionals, door-to-door visits, community dramas and films, community conversations | “Among men, effect estimates in the hypothesized direction were observed for all HIV-risk behaviours and indicators of relationship dynamics, with results statistically significant at the 5% level for all but two outcomes.” p. 4 |
| Naidoo 2016 [52] School-based education program | Individual | Weekly lessons in school with group discussion, role playing, video watching, and drawing | “Comparing the verbal bullying of other people in the intervention group versus control, from baseline to postintervention (p = 0.047) was significantly reduced.” p. 817 |
| Pulerwitz 2015 [40] Male Norms Initiative | Both | Interactive group education, community mobilization and engagement, Engaging Boys and Men in Gender Transformation manual | “In our multivariate IPV analyses, however, only the finding of lower reported violence from the community engagement (CE-only) intervention remained marginally significant...” p. 136 |
| Sosa-Rubi 2017 [41] True Love | Both | Training of school staff, schoolyard activities, classroom-based workshops, community engagement | “We found a 58% (p < 0.05) and 55% (p < 0.05) reduction in the prevalence of perpetrated and experienced psychological violence, respectively, among SCC, IL-1 males compared to males exposed only to the SCC component.” p. 804 |
| Thato 2013 [37] Brief, Peer-led HIV Prevention Program | Individual | Group sessions taught by peer leader using video and discussion | The program “did not significantly increase AIDS/STIs preventative behaviors” p. 58 |
| Vantamay 2019 [30] 3S Project | Individual | Social marketing campaign through classroom activities and projects | “The mean scores of the experimental group were higher than the mean scores of the control group significantly in all of the five indicators... including the sustainable consumption behavior.” p. 42 |
| Watts 2015 [29] SASA! | Community | Community activists, training of professionals, door-to-door visits, community dramas and films, community conversations | “The findings also suggest that SASA! impacted significantly on the reported levels of sexual concurrency, with 27 per cent of partnered men in intervention communities reporting having had other sexual partners in the past year, compared to 45 per cent of men in the control communities…” p. ii |
| Study ID | Intervention Level | Intervention Activities | Key Findings on Behavioral Outcomes |
|---|---|---|---|
| Dougherty 2018 [50] Community Benefits Health | Community | Community-based incentives, health messaging through various media, peer educators and community health officers | “Across three of the six study outcomes, we found that women who were exposed to the intervention activities were significantly more likely to have practiced improved health outcomes.” p. 88 |
| Figueroa 2016 [34] Tchova Tchova | Community | Facilitated community dialogues, radio magazine, HIV/AIDS prevention gender tool | “88% of intervention and 72% of control respondents in the sample said they talked with their partner about HIV and/or sexual behavior in the past 3 months.” p. 559 |
| Kraft 2012 [36] Gama Cuulu Radio Serial Drama | Both | Radio serial drama, community drama, one-on-one education sessions, small-group discussions | “There were few statistically significant differences over time between the two provinces, and only one statistically significant difference on a behavioral outcome (i.e., condom use, last sex).” p. 941 |
| Lundgren 2018 [49] Choices, Voices, and Promises | Both | Video series for families, group discussion, public poster display, community discussion | In the Choices, Voices, Promises sample, respondents were more likely to answer they have told their parents (guardian) that it is important for sisters/you to continue studying than in the Choices only sample. |
| Miller 2014 [39] Parivartan (Coaching Boys into Men) | Individual | Training of coaches, coach role models, coach-led discussions with players | “Fewer negative intervention behaviors (i.e., laughing and going along with peers’ abusive behaviors) were reported by intervention athletes at follow-up compared with comparison athletes, but this difference was only marginally significant.” p. 771 |
| Rijsdijk 2011 [53] World Starts with Me | Individual | Computer-based lessons in schools with peer educators, games, assignments | “No significant effects were found for past performance behaviour [of condom use].” “No significant effects were found for past performance behaviour regarding avoiding and escaping risky situations…” p. 8 |
| Wagman 2015 [45] SHARE | Both | Community-based mobilization through advocacy, training, learning materials, and special events plus one-on-one intervention with women seeking HCT | “SHARE has no effect on male-reported IPV perpetration.” p. e23 “SHARE was also associated with significant increases in disclosure of HIV status in men and women.” p. e30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, A.N. Some Interventions to Shift Meta-Norms Are Effective for Changing Behaviors in Low- and Middle-Income Countries: A Rapid Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 7312. https://doi.org/10.3390/ijerph19127312
Brown AN. Some Interventions to Shift Meta-Norms Are Effective for Changing Behaviors in Low- and Middle-Income Countries: A Rapid Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(12):7312. https://doi.org/10.3390/ijerph19127312
Chicago/Turabian StyleBrown, Annette N. 2022. "Some Interventions to Shift Meta-Norms Are Effective for Changing Behaviors in Low- and Middle-Income Countries: A Rapid Systematic Review" International Journal of Environmental Research and Public Health 19, no. 12: 7312. https://doi.org/10.3390/ijerph19127312
APA StyleBrown, A. N. (2022). Some Interventions to Shift Meta-Norms Are Effective for Changing Behaviors in Low- and Middle-Income Countries: A Rapid Systematic Review. International Journal of Environmental Research and Public Health, 19(12), 7312. https://doi.org/10.3390/ijerph19127312