
Workplace Bullying and Long-Term Sickness Absence—A Five-Year Follow-Up Study of 2476 Employees Aged 31 to 60 Years in Germany





Abstract
:1. Introduction
2. Materials and Methods
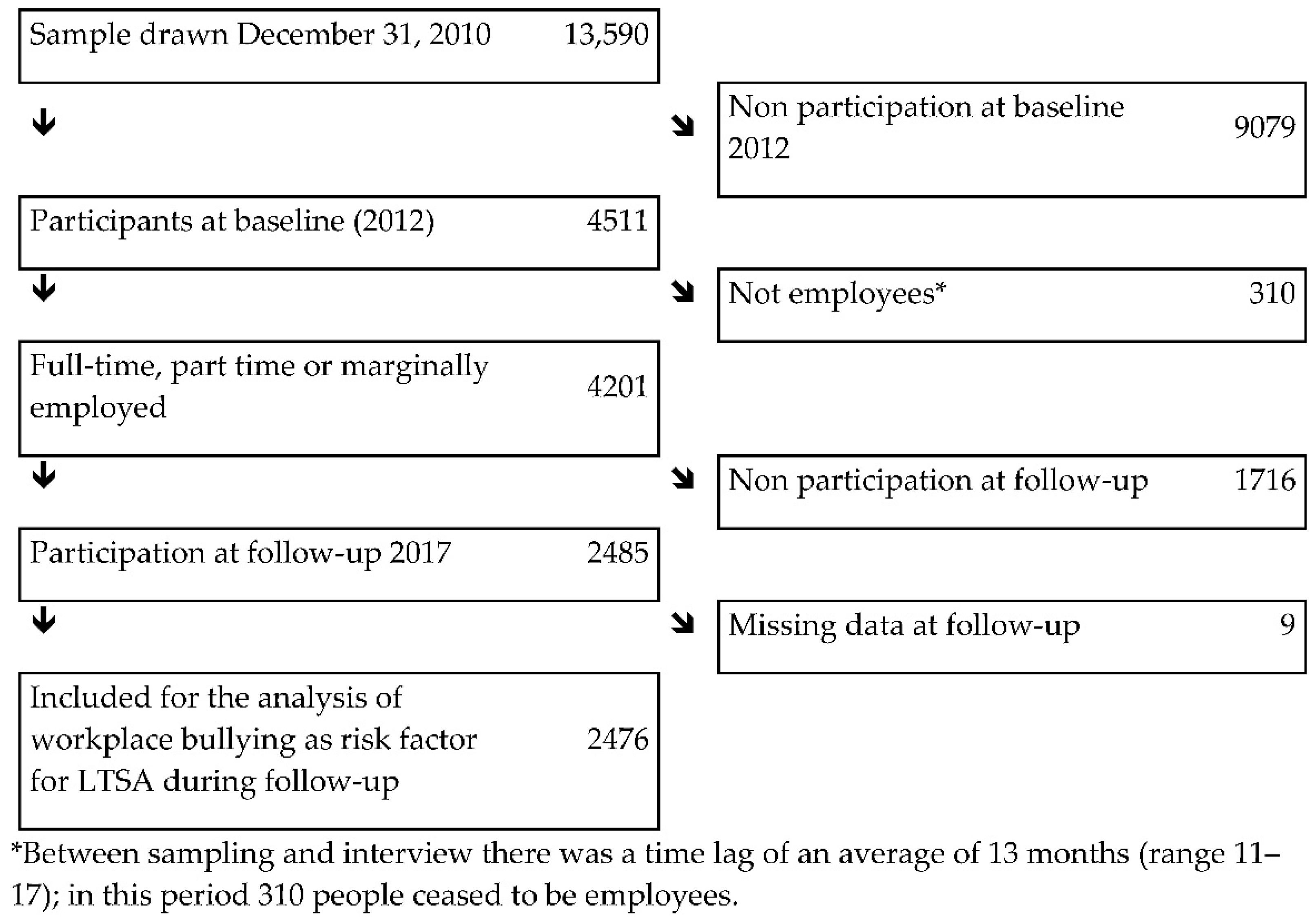
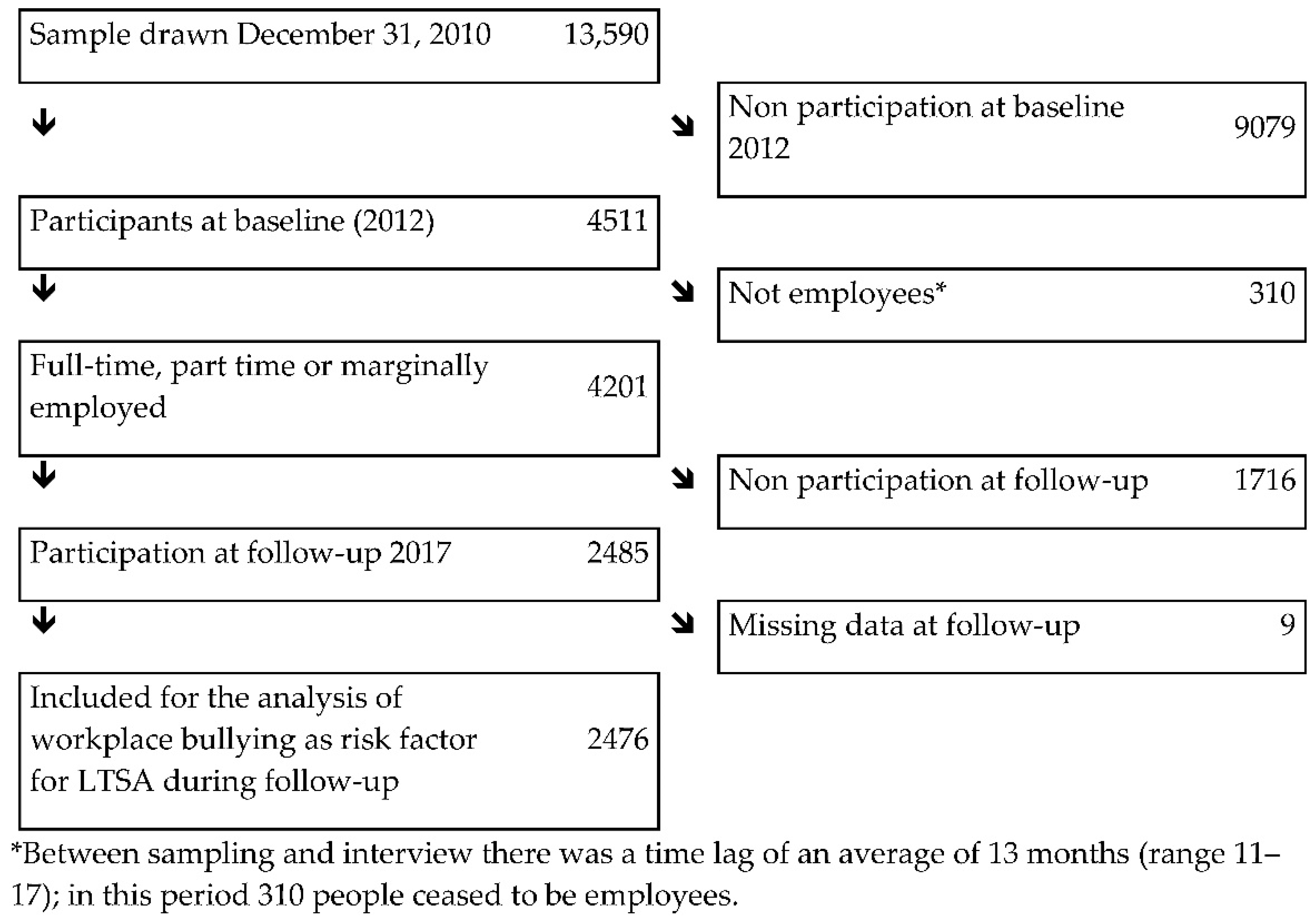
2.1. Sample
2.2. Measures
2.2.1. Long-Term Sickness Absence (LTSA)
2.2.2. Workplace Bullying
2.2.3. Covariates
2.3. Analysis
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Comparison with Earlier Studies
4.3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Einarsen, S.; Hoel, E.; Zapf, D.; Cooper, C.L. Bullying and Harassment in the Workplace: Theory, Research and Practice; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Conway, P.M.; Hogh, A.; Balducci, C.; Ebbesen, D.K. Workplace Bullying and Mental Health. In Pathways of Job-Related Negative Behaviour. Handbooks of Workpplace Bullying, Emotional Abuse and Harassment; d’Cruz, P., Noronha, E., Baillien, E., Catley, B., Harlos, K., Hogh, A., Eds.; Springer: Singapore, 2018; Volume 2. [Google Scholar]
- Mikkelsen, E.G.; Hansen, Å.M.; Persson, R.; Byrgesen, M.F.; Hogh, A. Individual consequences of being exposed to workplace bullying. In Bullying and Harassment in the Workplace: Theory, Research and Practice; Einarsen, S., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 163–208. [Google Scholar]
- Nielsen, M.B.; Indregard, A.M.; Øverland, S. Workplace bullying and sickness absence: A systematic review and meta-analysis of the research literature. Scand. J. Work. Environ. Health 2016, 42, 359–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivimaki, M.; Virtanen, M.; Vartia, M.; Elovainio, M.; Vahtera, J.; Keltikangas-Järvinen, L. Workplace bullying and the risk of cardiovascular disease and depression. Occup. Environ. Med. 2003, 60, 779–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rugulies, R.; Madsen, I.E.; Hjarsbech, P.U.; Hogh, A.; Borg, V.; Carneiro, I.G.; Aust, B. Bullying at work and onset of a major depressive episode among Danish female eldercare workers. Scand. J. Work Environ. Health 2012, 38, 218–227. [Google Scholar] [CrossRef]
- Gullander, M.; Hogh, A.; Hansen, A.M.; Persson, R.; Rugulies, R.; Kolstad, H.A.; Thomsen, J.F.; Willert, M.V.; Grynderup, M.; Mors, O.; et al. Exposure to workplace bullying and risk of depression. J. Occup. Environ. Med. 2014, 56, 1258–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einarsen, S.; Nielsen, M.B. Workplace bullying as an antecedent of mental health problems: A five-year prospective and representative study. Int. Arch. Occup. Environ. Health 2015, 88, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Bonde, J.P.; Gullander, M.; Hansen, A.M.; Grynderup, M.; Persson, R.; Hogh, A.; Willert, M.V.; Kaerlev, L.; Rugulies, R.; Kolstad, H.A. Health correlates of workplace bullying: A 3-wave prospective follow-up study. Scand. J. Work Environ. Health 2016, 42, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo-Ferraz, H.; Gil-Monte, P.R.; Grau-Alberola, E.; Llorca-Pellicer, M.; García-Juesas, J.A. Influence of Some Psychosocial Factors on Mobbing and its Consequences Among Employees Working with People with Intellectual Disabilities. J. Appl. Res. Intellect. Disabil. 2012, 25, 455–463. [Google Scholar] [CrossRef]
- Lange, S.; Burr, H.; Rose, U.; Conway, P.M. Workplace bullying and depressive symptoms among employees in Germany: Prospective associations regarding severity and the role of the perpetrator. Int. Arch. Occup. Environ. Health 2020, 93, 433–443. [Google Scholar] [CrossRef] [Green Version]
- Sterud, T.; Hanvold, T.N. Effects of adverse social behaviour at the workplace on subsequent mental distress: A 3-year prospective study of the general working population in Norway. Int. Arch. Occup. Environ. Health 2021, 94, 325–334. [Google Scholar] [CrossRef]
- Loerbroks, A.; Weigl, M.; Li, J.; Glaser, J.; Degen, C.; Angerer, P. Workplace bullying and depressive symptoms: A prospective study among junior physicians in Germany. J. Psychosom. Res. 2015, 78, 168–172. [Google Scholar] [CrossRef]
- Nielsen, M.B.; Christensen, J.O.; Finne, L.B.; Knardahl, S. Workplace bullying, mental distress, and sickness absence: The protective role of social support. Int. Arch. Occup. Environ. Health 2020, 93, 43–53. [Google Scholar] [CrossRef]
- Wooden, M.; Bubonya, M.; Cobb-Clark, D. Environment; Health, Sickness absence and mental health: Evidence from a nationally representative longitudinal survey. Scand. J. Work. Environ. Health 2016, 42, 201–208. [Google Scholar] [PubMed] [Green Version]
- Thorsen, S.V.; Rugulies, R.; Hjarsbech, P.U.; Bjorner, J.B. The predictive value of mental health for long-term sickness absence: The Major Depression Inventory (MDI) and the Mental Health Inventory (MHI-5) compared. BMC Med. Res. Methodol. 2013, 13, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorsen, S.V.; Pedersen, J.; Flyvholm, M.-A.; Kristiansen, J.; Rugulies, R.; Bültmann, U. Perceived stress and sickness absence: A prospective study of 17,795 employees in Denmark. Int. Arch. Occup. Environ. Health 2019, 92, 821–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kausto, J.; Pentti, J.; Oksanen, T.; Virta, L.J.; Virtanen, M.; Kivimäki, M.; Vahtera, J. Environment; Health, Length of sickness absence and sustained return-to-work in mental disorders and musculoskeletal diseases: A cohort study of public sector employees. Scand. J. Work. Environ. Health 2017, 43, 358–366. [Google Scholar] [CrossRef] [Green Version]
- Jennen, J.G.M.; Jansen, N.W.H.; van Amelsvoort, L.G.P.M.; Slangen, J.J.M.; Kant, I.J. Associations between depressive complaints and indicators of labour participation among older Dutch employees: A prospective cohort study. Int. Arch. Occup. Environ. Health 2021, 94, 391–407. [Google Scholar] [CrossRef]
- Sterud, T.; Degerud, E.; Skare, Ø.; Hanvold, T.N.; Christensen, J.O. Adverse social behaviour at the workplace and subsequent physician certified sick leave: A three-wave prospective study of the general working population in Norway. Occup. Environ. Med. 2021, 78, 576–582. [Google Scholar] [CrossRef]
- Thorsen, S.V.; Flyvholm, M.A.; Pedersen, J.; Bültmann, U.; Andersen, L.L.; Bjorner, J.B. Associations between physical and psychosocial work environment factors and sickness absence incidence depend on the lengths of the sickness absence episodes: A prospective study of 27 678 Danish employees. Occup. Environ. Med. 2021, 78, 46–53. [Google Scholar] [CrossRef]
- Aagestad, C.; Tyssen, R.; Sterud, T. Do work-related factors contribute to differences in doctor-certified sick leave? A prospective study comparing women in health and social occupations with women in the general working population. BMC Public Health 2016, 16, 235. [Google Scholar]
- Janssens, H.; Clays, E.; De Clercq, B.; Casini, A.; De Bacquer, D.; Kittel, F.; Braeckman, L. The relation between psychosocial risk factors and cause-specific long-term sickness absence. Eur. J. Public Health 2014, 24, 428–433. [Google Scholar] [CrossRef] [Green Version]
- Hinkka, K.; Kuoppala, J.; Väänänen-Tomppo, I.; Lamminpää, A. Psychosocial work factors and sick leave, occupational accident, and disability pension: A cohort study of civil servants. J. Occup. Environ. Med./Am. Coll. Occup. Environ. Med. 2013, 55, 191–197. [Google Scholar] [CrossRef]
- Clausen, T.; Hogh, A.; Borg, V. Acts of offensive behaviour and risk of long-term sickness absence in the Danish elder-care services: A prospective analysis of register-based outcomes. Int. Arch. Occup. Environ. Health 2012, 85, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Elovainio, M.; Vahtera, J. Workplace bullying and sickness absence in hospital staff. Occup. Environ. Med. 2000, 57, 656–660. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, W.; Bruusgaard, D.; Knardahl, S. Work factors as predictors of sickness absence: A three month prospective study of nurses’ aides. Occup. Environ. Med. 2003, 60, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, U.; Schiel, S.; Schroder, H.; Kleudgen, M.; Tophoven, S.; Rauch, A.; Freude, G.; Muller, G. The Study on Mental Health at Work: Design and sampling. Scand. J. Public Health 2017, 45, 584–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziebarth, N.R. Long-Term Absenteeism and Moral Hazard—Evidence from a Natural Experiment; Deutsches Institut für Wirtschaftsforschung (DIW): Berlin, Germany, 2009; Volume 888, pp. 277–292. [Google Scholar]
- Borsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S.; Team, S.C.C. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Lange, S.; Burr, H.; Conway, P.M.; Rose, U. Workplace bullying among employees in Germany: Prevalence estimates and the role of the perpetrator. Int. Arch. Occup. Environ. Health 2019, 92, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Garthus-Niegel, S.; Nubling, M.; Letzel, S.; Hegewald, J.; Wagner, M.; Wild, P.S.; Blettner, M.; Zwiener, I.; Latza, U.; Jankowiak, S.; et al. Development of a mobbing short scale in the Gutenberg Health Study. Int Arch Occup Environ. Health 2016, 89, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Leymann, H. The content and development of mobbing at work. Eur. J. Work Organ. Psychol. 1996, 5, 165–184. [Google Scholar] [CrossRef]
- Christensen, K.B.; Lund, T.; Labriola, M.; Villadsen, E.; Bultmann, U. The fraction of long-term sickness absence attributable to work environmental factors: Prospective results from the Danish Work Environment Cohort Study. Occup. Environ. Med. 2007, 64, 487–489. [Google Scholar] [CrossRef] [Green Version]
- Labriola, M. Conceptual framework of sickness absence and return to work, focusing on both the individual and the contextual level. Work 2008, 30, 377–387. [Google Scholar] [PubMed]
- Lund, T.; Labriola, M.; Christensen, K.B.; Bultmann, U.; Villadsen, E. Physical work environment risk factors for long term sickness absence: Prospective findings among a cohort of 5357 employees in Denmark. BMJ 2006, 332, 449–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagen, F. Levels of Education: Relation between ISCO Skill Level and ISCED Categories. Available online: http://www.fernunihagen.de/FTB/telemate/database/isced.htm#ISCO (accessed on 21 March 2015).
- Wirth, H.; Gresch, C.; Müller, W.; Pollak, R.; Weiss, F. Validating the ESeC-Scheme as Operationalization of Social Class the Case of Germany; Mannheimer Zentrum für Europ. Sozialforschung: Mannheim, Germany, 2009. [Google Scholar]
- Lee, P.N.; Forey, B.A.; Coombs, K.J. Systematic review with meta-analysis of the epidemiological evidence in the 1900s relating smoking to lung cancer. BMC Cancer 2012, 12, 385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, A.; Siefer, A.; Tiemann, M. BIBB/BAuA-Erwerbstätigenbefragung 2006–Arbeit und Beruf im Wandel, Erwerb und Verwertung beruflicher Qualifikationen; Bundesinstitut für Berufsbildung: Bonn, Germany, 2007. [Google Scholar]
- Tynes, T.; Aagestad, C.; Thorsen, S.V.; Andersen, L.L.; Perkio-Makela, M.; Garcia, F.J.P.; Blanco, L.G.; Vermeylen, G.; Parent-Thirion, A.; Hooftman, W.; et al. Physical working conditions as covered in European monitoring questionnaires. BMC Public Health 2017, 17, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skov, T.; Deddens, J.; Petersen, M.R.; Endahl, L. Prevalence proportion ratios: Estimation and hypothesis testing. Int. J. Epidemiol. 1998, 27, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Kivimaki, M.; Nyberg, S.T.; Batty, G.D.; Fransson, E.I.; Heikkila, K.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; et al. Job strain as a risk factor for coronary heart disease: A collaborative meta-analysis of individual participant data. Lancet 2012, 380, 1491–1497. [Google Scholar] [CrossRef] [Green Version]
- Rothman, K.J.; Greenland, S. Causation and causal inference in epidemiology. Am. J. Public Health 2005, 95 (Suppl. S1), S144–S150. [Google Scholar] [CrossRef] [Green Version]
- Einarsen, S. Harassment and bullying at work: A review of the scandinavian approach. Aggress. Violent Behav. 2000, 5, 379–401. [Google Scholar] [CrossRef]
- Zapf, D.; Gross, C. Conflict escalation and coping with workplace bullying: A replication and extension. Eur. J. Work Organ. Psychol. 2001, 10, 497–522. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, A.; Moreno-Jiménez, B.; Sanz-Vergel, A.I. Reciprocal relations between workplace bullying, anxiety, and vigor: A two-wave longitudinal study. Anxiety Stress Coping 2015, 28, 514–530. [Google Scholar] [CrossRef] [Green Version]
- Nabe-Nielsen, K.; Grynderup, M.B.; Conway, P.M.; Clausen, T.; Bonde, J.P.; Garde, A.H.; Hogh, A.; Kaerlev, L.; Török, E.; Hansen, Å.M. The Role of Psychological Stress Reactions in the Longitudinal Relation Between Workplace Bullying and Turnover. J. Occup. Environ. Med./Am. Coll. Occup. Environ. Med. 2017, 59, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.B.; Harris, A.; Pallesen, S.; Einarsen, S.V. Workplace bullying and sleep—A systematic review and meta-analysis of the research literature. Sleep Med. Rev. 2020, 51, 101289. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Magnusson Hanson, L.L.; Lange, T.; Starkopf, L.; Westerlund, H.; Madsen, I.E.H.; Rugulies, R.; Pentti, J.; Stenholm, S.; Vahtera, J.; et al. Workplace bullying and workplace violence as risk factors for cardiovascular disease: A multi-cohort study. Eur. Heart J. 2019, 40, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Dehue, F.; Bolman, C.; Völlink, T.; Pouwelse, M. Coping with bullying at work and health related problems. Int. J. Stress Manag. 2012, 19, 175–197. [Google Scholar] [CrossRef]
- Zapf, D.; Dormann, C.; Frese, M. Longitudinal studies in organizational stress research: A review of the literature with reference to methodological issues. J. Occup. Health Psychol. 1996, 1, 145–169. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, J.; Bjorner, J.B.; Burr, H.; Christensen, K.B. Transitions between sickness absence, work, unemployment, and disability in Denmark 2004–2008. Scand. J. Work Environ. Health 2012, 38, 516–526. [Google Scholar] [CrossRef] [Green Version]
- d’Errico, A.; Burr, H.; Pattloch, D.; Kersten, N.; Rose, U. Working conditions as risk factors for early exit from work-in a cohort of 2351 employees in Germany. Int. Arch. Occup. Environ. Health 2021, 94, 117–138. [Google Scholar] [CrossRef]
- Taris, T.W.; Kompier, M.A.J. Cause and effect: Optimizing the designs of longitudinal studies in occupational health psychology. Work Stress 2014, 28, 1–8. [Google Scholar] [CrossRef]
- Baillien, E.; De Cuyper, N.; De Witte, H. Job autonomy and workload as antecedents of workplace bullying: A two-wave test of Karasek’s Job Demand Control Model for targets and perpetrators. J. Occup. Organ. Psychol. 2011, 84, 191–208. [Google Scholar] [CrossRef]
- Baillien, E.; Rodriguez-Muñoz, A.; Van den Broeck, A.; De Witte, H. Do demands and resources affect target’s and perpetrators’ reports of workplace bullying? A two-wave cross-lagged study. Work Stress 2011, 25, 128–146. [Google Scholar]
- Conway, P.M.; Burr, H.; Rose, U.; Clausen, T.; Balducci, C. Antecedents of Workplace Bullying among Employees in Germany: Five-Year Lagged Effects of Job Demands and Job Resources. Int. J. Environ. Res. Public Health 2021, 18, 10805. [Google Scholar] [CrossRef] [PubMed]
- Law, R.; Dollard, M.F.; Tuckey, M.R.; Dormann, C. Psychosocial safety climate as a lead indicator of workplace bullying and harassment, job resources, psychological health and employee engagement. Accid. Anal. Prev. 2011, 43, 1782–1793. [Google Scholar] [CrossRef] [PubMed]
- Bond, S.A.; Tuckey, M.R.; Dollard, M.F. Psychosocial safety climate, workplace bullying, and symptoms of posttraumatic stress. Organ. Dev. J. 2010, 28, 37. [Google Scholar]
- Attell, B.K.; Kummerow Brown, K.; Treiber, L.A. Workplace bullying, perceived job stressors, and psychological distress: Gender and race differences in the stress process. Soc. Sci. Res. 2017, 65, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Gardner, D.; Bentley, T.A.; Catley, B.; Cooper-Thomas, H.; O’Driscoll, M.P.; Trenberth, L. Ethnicity, workplace bullying, social support and psychological strain in Aotearoa/New Zealand. N. Z. J. Psychol. 2013, 42, 84–91. [Google Scholar]

{kind=link}
| n | % | Mean | Std. Dev. | |
|---|---|---|---|---|
| GENDER 2012 | ||||
| Men | 1206 | 49% | ||
| Women | 1270 | 51% | ||
| AGE 2012 | 46.9 | 7.6 | ||
| OCCUPATIONAL LEVEL 2012 | ||||
| Unskilled workers | 144 | 6% | ||
| Skilled workers | 1039 | 42% | ||
| Semi-professionals | 683 | 28% | ||
| Academics/managers | 610 | 25% | ||
| SMOKING STATUS 2012 | ||||
| Never | 1009 | 41% | ||
| Former | 765 | 31% | ||
| Current | 702 | 28% | ||
| PHYSICAL DEMANDS 2012 (min 0, max 4) | 1.09 | 1.02 | ||
| WORKPLACE BULLYING 2012 | ||||
| No | 2069 | 84% | ||
| Occasional | 244 | 10% | ||
| Severe | 163 | 7% | ||
| LTSA EPISODE 2012–2017 | ||||
| No | 1863 | 75% | ||
| Yes | 613 | 25% |
| N | LTSA during Follow-Up 2012–2017 | |||||
|---|---|---|---|---|---|---|
| Cases, n | Cases (%) | Adjusted for Gender, Age, Age Squared, Occupational Level, Smoking and Physical Demands at Work | ||||
| p-Value * | RR | 95% CI | ||||
| Workplace bullying 2012 | 0.072 | |||||
| no | 2069 | 489 | 24 | 1 | ||
| occasional | 244 | 68 | 28 | 1.15 | 0.85; 1.55 | |
| severe | 163 | 56 | 34 | 1.48 | 1.05; 2.19 | |
| N | LTSA during Follow-Up 2014–2017 * | |||||
|---|---|---|---|---|---|---|
| Cases, n | Cases (%) | Adjusted for Gender, Age, Age Squared, Occupational Level, Smoking and Physical Demands at Work | ||||
| p-Value † | RR | 95% CI | ||||
| Workplace bullying 2012 | 0.005 | |||||
| no | 2069 | 317 | 15 | 1 | ||
| occasional | 244 | 47 | 19 | 1.21 | 0.86; 1.71 | |
| severe | 163 | 41 | 25 | 1.69 | 1.10; 2.36 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burr, H.; Balducci, C.; Conway, P.M.; Rose, U. Workplace Bullying and Long-Term Sickness Absence—A Five-Year Follow-Up Study of 2476 Employees Aged 31 to 60 Years in Germany. Int. J. Environ. Res. Public Health 2022, 19, 7193. https://doi.org/10.3390/ijerph19127193
Burr H, Balducci C, Conway PM, Rose U. Workplace Bullying and Long-Term Sickness Absence—A Five-Year Follow-Up Study of 2476 Employees Aged 31 to 60 Years in Germany. International Journal of Environmental Research and Public Health. 2022; 19(12):7193. https://doi.org/10.3390/ijerph19127193
Chicago/Turabian StyleBurr, Hermann, Cristian Balducci, Paul Maurice Conway, and Uwe Rose. 2022. "Workplace Bullying and Long-Term Sickness Absence—A Five-Year Follow-Up Study of 2476 Employees Aged 31 to 60 Years in Germany" International Journal of Environmental Research and Public Health 19, no. 12: 7193. https://doi.org/10.3390/ijerph19127193
APA StyleBurr, H., Balducci, C., Conway, P. M., & Rose, U. (2022). Workplace Bullying and Long-Term Sickness Absence—A Five-Year Follow-Up Study of 2476 Employees Aged 31 to 60 Years in Germany. International Journal of Environmental Research and Public Health, 19(12), 7193. https://doi.org/10.3390/ijerph19127193